
Abstract
Background:
Necrotizing fasciitis (NF) is a potentially fatal soft tissue infection. Four types of pathogens can be distinguished in the pathogen spectrum, although there are strong regional differences with regard to the most common pathogens.
Patients and Methods:
All cases of NF between 2003 and 2021 with an identified causative agent were analyzed retrospectively. The cases were divided into three groups: polymicrobial, gram-positive and gram-negative. Demographic factors, localization of infection, inflammatory parameters, and clinical outcome were compared between the three groups.
Results:
A total of 95 cases were analyzed, 41% of which were caused by multiple pathogens. A gram-positive pathogen was reported in 40% of cases and a gram-negative pathogen in 19%. There were significant differences between the three groups with respect to age (with patients in the gram-negative group being on average the oldest) and intensive care unit admissions (which was most frequent in the polymicrobial group).
Conclusions:
The pathogen spectrum of NF has rarely been studied in a large patient population. Gram-positive pathogens account for the majority of monomicrobial infections in our study. Nevertheless, we recommend calculated broad-spectrum antibiotic therapy given the high number of polymicrobial infections and gram-negative infections. Gram-negative infections may be associated with increased mortality, elevated procalcitonin levels, and are relatively frequent in NF of the lower extremities.
Necrotizing fasciitis (NF) is an urgent condition with high morbidity and mortality presenting a major challenge regarding diagnosis and treatment. Although NF is relatively rare, it must be considered as a differential diagnosis in many situations, especially soft tissue infections of the extremities. In the study by Kaul et al. 1 the incidence of NF caused by group A streptococci was determined. 2 This was 0.09 in the first year and 0.40 per 100.00 in the last year of the study. Because the incidence also depends on the reporting practices, the geographical localization and is influenced by time-related factors, exact values for the general incidence are difficult to determine. 3
According to Morgan et al., 4 four different types of NF can be distinguished. Type 1 constitutes polymicrobial infections and represents the majority of infections (70%–80%). Type 2 concerns monomicrobial infections, which are mainly caused by group A streptococci. Type 3 constitutes infections caused by gram-negative pathogens and type 4 infections caused by fungi. Streptococcus species are considered the most frequent monomicrobial pathogens, followed by Staphylococcus aureus. 5 There are regional differences in the spectrum of causative micro-organisms, with gram-positive pathogens predominating in Europe and the United States, whereas gram-negative pathogens are more common in Asia. 6 In addition, relations exist between various predisposing factors and causative micro-organisms. For example, saltwater lacerations are typically associated with Vibrio vulnificus infection and mucosal breaches with polymicrobial infections. 7
Several comorbidities associated with NF have been reported in the literature. For instance, diabetes mellitus, obesity, and liver cirrhosis are considered risk factors for the occurrence of NF.8,9 Liver cirrhosis, end-stage renal disease, age (>60 years), and soft tissue emphysema, among others, are considered independent predictors of mortality in NF. 10 In 2018, the U.S. Food and Drug Administration (FDA) issued a safety warning on sodium-glucose cotransporter-2 inhibitors (SGLT2i), which were associated with an increased incidence of Fournier gangrene, although a study by Yang et al. 11 found no increased risk for Fournier gangrene associated with SGLT2i compared with dipeptidyl peptidase-4 inhibitors.
Clinical factors, laboratory data, and imaging techniques are well-established elements in the diagnostic process. Redness, swelling, disproportionate pain characteristically outside the margins of the apparent skin involvement, and fever can characterize the clinical appearance in the beginning stages. 12 In later stages, ecchymoses, bullae, skin necrosis, skin anesthesia and crepitus can become evident, signifying progressing tissue destruction.7,13 In the earliest stages systemic symptoms such as malaise, diarrhea, and anorexia with disproportionate limb pain can be present without any apparent skin involvement. 7 The most widely known laboratory-based scoring system for the diagnosis of NF is the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC), which includes parameters such as hemoglobin and sodium, as well as inflammatory parameters (C-reactive protein and leukocytes). 14 Recent studies also show a diagnostic value of procalcitonin.15,16 Among the imaging methods, computed tomography has a significantly higher diagnostic value than radiographic examinations, 17 although broad application in forms of soft tissue infections must be discussed because of the radiation exposure.
The diagnosis of NF is frequently associated with a poor prognosis. For example, Al-Qurayshi et al. 18 found a mortality rate of 12.6% in their study. The identification of patients with an increased mortality risk is therefore an important step for the initiation of early intensive care measures. In a randomized controlled trial, Khamnuan et al. 19 presented a risk scoring model for cases of necrotizing fasciitis. The Mortality in Necrotizing Fasciitis (MNF) scoring system presented in the study can be used to identify at-risk patients.
The aim of the study was to present the pathogen spectrum based on a relatively large NF patient population for central Europe and to demonstrate possible correlations between the individual pathogen groups and various clinical parameters. This might contribute to an improved calculated antibiotic therapy, which is given immediately on suspicion of NF, in the absence of an identified pathogen.
Patients and Methods
We performed a retrospective analysis of NF cases treated in our Department of Plastic, Reconstructive and Hand Surgery, Center for Severe Burn Injuries between 2003 and 2021. A database analysis was performed, identifying all cases of NF by using International Classification of Diseases (ICD) codes. In addition, the diagnosis of NF had to be confirmed in the discharge letter, which in our clinic only occurs after it is confirmed in the histopathologic examination. Microbiologic culture results were obtained from intra-operative specimens. Another inclusion criterion was a microbial finding with at least one cultured pathogen. A flowchart for the inclusion and exclusion process in this study is presented in Figure 1. This study was conducted in accordance with the Declaration of Helsinki. An ethics vote was waived because of the retrospective and anonymous study protocol.
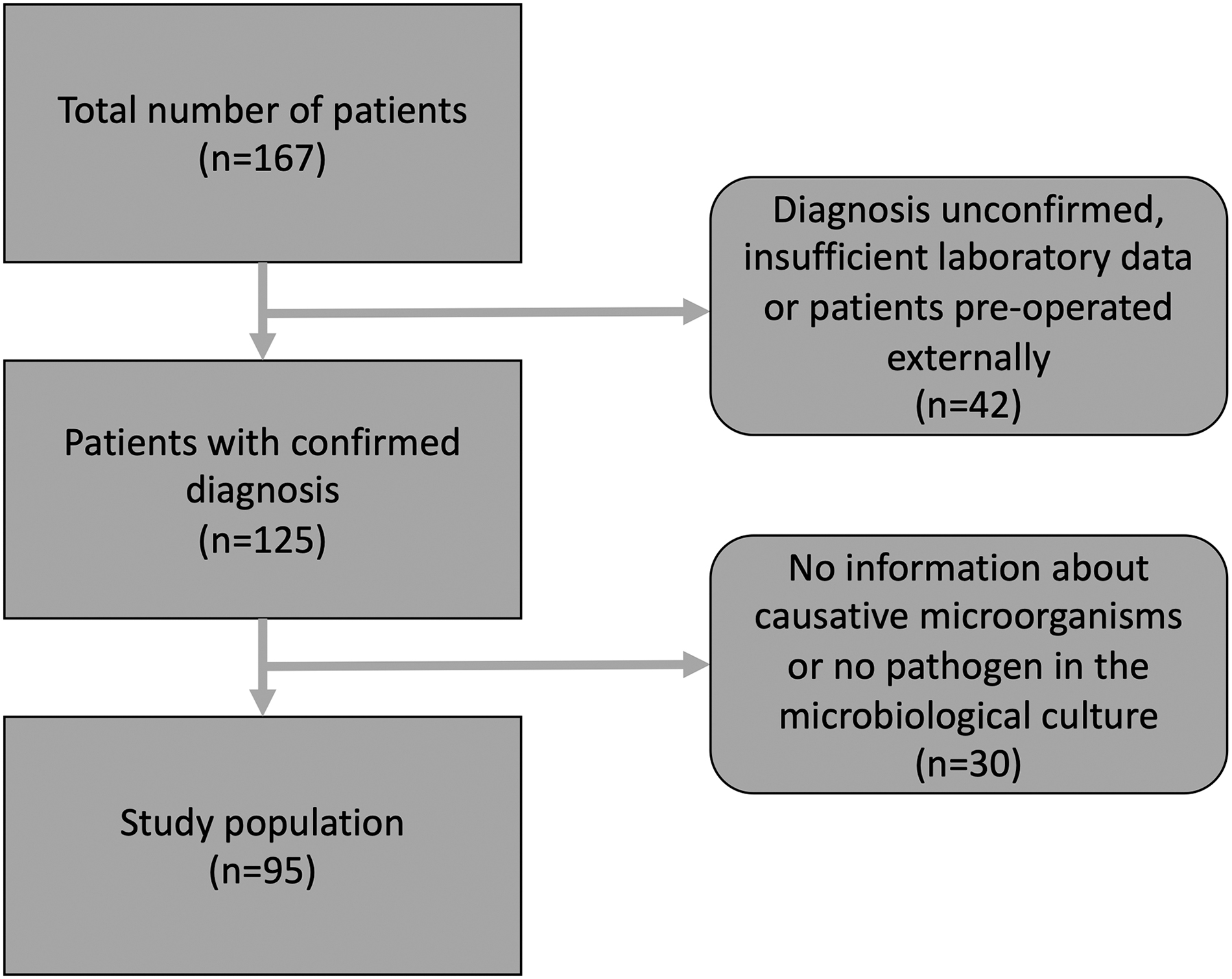
Flowchart of patient inclusion.
Demographic, laboratory, and outcome data were collected from the included patients. The localization of infection was also documented. Data were collected in Microsoft® Excel (Microsoft Corporation, Redmond, WA) and analyzed in Microsoft® Excel and IBM SPSS Statistics (IBM Corp, Armonk, NY). After a verification of normal distribution, the statistical evaluation was performed by analysis of variance (ANOVA) under post-hoc Bonferroni correction and χ 2 testing. The p values after Bonferroni correction were reported in the adjusted form. The significance level was set to a two-sided p < 0.05. Bar charts were used for graphical presentation.
Results
A total of 95 cases of NF were included in the study. The group with polymicrobial infections consisted of 39 cases (41%), the group with gram-positive infections consisted of 38 cases (40%), and the group with gram-negative infections consisted of 18 cases (19%). Data on demographics, NF localization, laboratory parameters, and clinical course can be found in Table 1. The mean age in the study was 57.1 ± 14.3 years. Comparing the three groups, the mean age was highest in the gram-negative group (p = 0.004).
Demographic Data, Site of Infection, Inflammatory Parameters, and Clinical Outcome in Polymicrobial, Gram-Positive, and Gram-Negative Infections with NF
Values in bold indicate statistically significant results.
NF = necrotizing fasciitis; ICU = intensive care unit.
The difference between polymicrobial infections and gram-negative infections was statistically significant with respect to age (p = 0.009). The age difference between gram-positive and gram-negative infections was also statistically significant (p = 0.006). A total of 65, or 68%, of patients with NF were males. There was no statistically significant difference between the three groups in this regard. The upper extremity was the site of infection 18 times (19%) in the study. The lower extremity was most commonly affected, with 40 cases (42%), followed by the perineal/genital area in 23 cases (24%) and the upper extremity in 18 cases (19%). There were no cases of cervical NF and three cases (3%) involved the trunk. More than one region was affected by NF in 11 patients (12%). No significant difference in localization was noted among the three groups. The mean leukocyte count was highest in the gram-positive group (20.0/mm3). Mean C-reactive protein (CRP) was highest in polymicrobial infections (22.6 mg/dL). The mean procalcitonin was highest in gram-negative infections (27.7 ng/mL).
The average length of hospitalization in this study was 38.8 ± 32.0 days and was highest in polymicrobial infections (p = 0.54). A total of 68 patients (72%) required transfer to an intensive care unit (ICU) during their in-patient stay. Intensive care treatment was most common for polymicrobial infections (p = 0.034). Of the 95 patients included in the study, 13 patients (14%) subsequently died. The length of hospital stay and rate of ICU admission were not significantly different between the three groups.
Most upper extremity infections were caused by pathogens from the gram-positive spectrum (61%). Lower extremity infections were also most frequently caused by gram-positive pathogens (40%). This was followed by polymicrobial (33%) and gram-negative infections (28%). Infections of the perineum or genital region were most commonly caused by polymicrobial pathogens (52%). A graphical representation of the data can be found in Figure 2.

Relative frequencies of pathogen groups in different localizations of necrotizing fasciitis (NF). Because of the limited number of cases in these regions, we did not report the frequency of pathogens in the cervical area, trunk area, or at multiple sites.
Most cases of NF were caused by multiple pathogens (41%; Table 2). The most common causative bacteria in monomicrobial infections were of the Staphylococcus or Streptococcus strain (33%). This was followed by Escherichia coli (9%), Pseudomonas aeruginosa (6%), Enterococcus faecium (4%) and Klebsiella pneumoniae (2%). Actinomyces, Propionibacterium, Clostridium perfringens, and Serratia marcescens were all cultured once each.
Causative Micro-Organisms
Discussion
In this study, the pathogen spectrum of NF was presented based on a retrospective analysis of 95 cases from a single center. Of the infections, 41% were caused by a polymicrobial bacterial spectrum. A gram-positive pathogen was the etiologic agent in 40% of cases and a gram-negative pathogen in 19% of cases. Streptococci or staphylococci as monomicrobial pathogens were cultured from 33% of the collected samples. Statistically significant differences were found between the three groups with respect to age and the proportion of patients who required intensive care. The mean age was highest in the gram-negative infection group, whereas the rate of ICU admission was highest in the polymicrobial infection group.
Microbiologic spectrum
Polymicrobial infections accounted for 41% of cases, whereas gram-positive infections were detected in 40% of cases. Gram-negative pathogens caused 19% of the cases of NF. The perineum is classically described as a site for polymicrobial infections whereas cases of NF of the extremities are more likely to be caused by monomicrobial infections. 5 This is in accordance with the results of our study in which gram-positive pathogens were cultivated most frequently in infections of the upper and lower extremities and polymicrobial infections were most frequent in the area of the perineum. In a study by Nawijn et al. 20 that included patients from the Netherlands, between 34% and 42% of cases of NF were caused by group A streptococci. In our study, 40% of infections were caused by gram-positive pathogens, whereby also other gram-positive pathogens contributed in addition to group A streptococci. Friederichs et al. 21 found 42% polymicrobial infections in their study from Germany, which is consistent with the results of our study (41%). Here, the majority of monomicrobial infections were also gram-positive pathogens. However, it should be noted that only patients who developed sepsis were included in the study. The overall trend indicates that gram-positive pathogens account for the majority of monomicrobial infections in central Europe.
Inflammatory parameters
The mean procalcitonin was 28 ng/dL in cases of NF from the gram-negative spectrum, 13 in gram-positive infections, and 11 in polymicrobial infections. Although the difference was not statistically significant, the values indicate that a correlation between the pathogen spectrum and procalcitonin should not be ruled out and could potentially represent a significant difference in a larger sample size. Koizumi et al. 22 found in their study that bacteremia caused by gram-negative pathogens resulted in higher serum procalcitonin levels on average. Leli et al. 23 also came to the same conclusion regarding elevated procalcitonin levels in bacteremia caused by gram-negative pathogens. This was also confirmed by Liu et al. 24 in their study, in which CRP values were also compared between gram-positive and gram-negative bacteremia and no significant differences could be demonstrated in this regard. The elevated procalcitonin levels in gram-negative infections may be relevant for potential decision support tools based on procalcitonin. These might be more effective in regions with more gram-negative pathogens than in regions where cases of NF are more likely to be caused by gram-positive pathogens. However, a future research project should assess whether the association between procalcitonin and gram-negative infections can also be generalized to cases of NF. Regarding leukocytes and CRP, no trend could be detected in our study.
Clinical outcome
The average length of hospitalization was relatively long at 38.8 days, although no differences were found between the different groups in this respect. In the study by Leiblein et al., 12 the average length of hospital stay was 32 days for comparison. The prolonged hospital stay for NF can be justified by the multiple surgical procedures, the ICU stays often required, and the prolonged intravenous antibiotic therapy that is frequently necessary. The review by Goh et al. 9 indicates that an average of 3.2 debridements are required. Subsequently, further reconstructive procedures are usually indicated. A difference was found between the three groups with regard to the rate of admission to the ICU, but not for mortality. This was highest for polymicrobial pathogens in this study. Here, the mortality rate was highest for gram-negative infections (28%). Age was also highest in the gram-negative infection group and may have acted as a confounding factor here.
Data not collected in this study, such as dietary habits or gut microbiome factors, may also have had an impact on immune functions and thus on the clinical outcome of patients. 25 In comparison, the retrospective study by Anaya et al. 26 demonstrated that clostridial infections were associated with increased mortality. Hsiao et al. 27 demonstrated an increased mortality rate in NF caused by Vibrio or Aeromonas infections in their study. In general, however, there are relatively few studies illustrating differences in clinical outcomes between groups of NF. Gelbard et al. 28 presented a meta-analysis examining the timing of initial surgical debridement. In the early group (first debridement less than 12 hours after arrival), the average mortality was 14%, whereas in the late group (first debridement after 12 hours), it was 26%. In our study, the mortality rate was 14%, which is within the previously reported range.
Anti-infective therapy
Antibiotic therapy is the mainstay of treatment along with surgical debridement. The heterogeneity in terms of causative organisms as well as the severity of NF with its associated morbidity and mortality justify an empirical therapy with broad-spectrum antibiotic agents addressing gram-positive as well as gram-negative bacteria. This is also consistent with the results of our study, in which 41% polymicrobial and 19% gram-negative infections were reported in addition to the increased frequency of cases of NF caused by gram-positive pathogens in Europe that has already been reported in the literature. 6 If NF is suspected, empiric antibiotic therapy with for example piperacillin-tazobactam as well as vancomycin should be started immediately, provided there are no intolerances to the antibiotic agents. 29 After pathogen identification, antibiotic therapy should be modified according to the antibiotic sensitivity testing. For instance, in cases due to Streptococcus pyogenes, therapy with penicillin and clindamycin may be considered.29,30 Antibiotic therapy is usually administered for an average period of four to six weeks, with continuation of antibiotic therapy for five days after signs of NF have resolved. 31
Strengths and limitations
The retrospective and non-randomized study protocol is a potential weakness of the study. Factors such as the average age of the patients may have acted as confounders when statistically testing for an association between the pathogen spectrum and inflammatory parameters and clinical outcome. Another limitation of the retrospective study protocol is a possible imperfect standard bias because the initial emergency department examinations and patient data collected were performed by many different physicians who do not have the same level of experience about NF.
A strength of this study is the inclusion of a relatively large number of patients (for NF). Attention was also paid to post hoc correction to avoid falsely significant results. However, it should be noted that the results of this study should not be generalized because of regional differences in the pathogen spectrum. Few studies to date have reviewed associations with different pathogen groups in cases of NF. Our study therefore provides a useful resource for the diagnosis and treatment of NF.
Conclusions
The pathogen spectrum of NF has rarely been described based on a large number of cases. Gram-positive pathogens account for the majority of monomicrobial infections in our study. Nevertheless, we recommend calculated broad-spectrum antibiotic therapy given the high number of polymicrobial infections and gram-negative infections. Gram-negative infections may be associated with increased mortality, elevated procalcitonin levels and are relatively frequent in NF of the lower extremities.
Footnotes
Authors' Contributions
Conceptualization: Breidung, Megas. Methodology: Megas, Breidung, Aurnhammer, Billner. Validation: Megas, Reichert, Billner. Formal analysis: Breidung, Megas, Malsagova. Investigation: Breidung, Malsagova. Resources: Reichert. Surgical procedures: Reichert, Billner, Malsagova, Megas. Data curation: Breidung, Aurnhammer, Megas. Writing—original draft preparation: Breidung, Megas. Writing—review and editing: Megas, Aurnhammer, Loukas, Billner, Breidung, Reichert. Visualization: Breidung, Loukas, Megas. Supervision: Megas, Reichert. Project administration: Megas. All authors have read and agreed to the published version of the manuscript.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors declare no conflict of interest.