
Abstract
Background:
Procalcitonin (PCT) is a biomarker for sepsis, but its utility has not been investigated in necrotizing enterocolitis (NEC). Necrotizing enterocolitis is a devastating multisystem disease of infants that in severe cases requires surgical intervention. We hypothesize that an elevated PCT will be associated with surgical NEC.
Patients and Methods:
After obtaining Institutional Review Board (IRB) approval (#12655), we performed a single institution retrospective case control study between 2010 and 2021 of infants up to three months of age. Inclusion criteria was PCT drawn within 72 hours of NEC or sepsis diagnosis. Control infants had a PCT drawn in the absence of infectious symptoms. Recursive partitioning (RP) identified PCT cutoffs. Categorical variable associations were tested using Fisher exact or χ2 tests. Continuous variables were tested using Wilcoxon rank sum test, Student t-test, and Kruskal-Wallis test. Adjusted associations of PCT and other covariables with NEC or sepsis versus controls were obtained via multinomial logistic regression analysis.
Results:
We identified 49 patients with NEC, 71 with sepsis, and 523 control patients. Based on RP, we selected two PCT cutoffs: 1.4 ng/mL and 3.19 ng/ml. A PCT of ≥1.4 ng/mL was associated with surgical (n = 16) compared with medical (n = 33) NEC (87.5% vs. 39.4%; p = 0.0015). A PCT of ≥1.4 ng/mL was associated with NEC versus control (p < 0.0001) even when adjusting for prematurity and excluding stage IA/IB NEC (odds ratio [OR], 28.46; 95% confidence interval [CI], 11.27–71.88). A PCT of 1.4–3.19 ng/mL was associated with both NEC (adjusted odds ratio [aOR], 11.43; 95% CI, 2.57–50.78) and sepsis (aOR, 6.63; 95% CI, 2.66–16.55) compared with controls.
Conclusions:
A PCT of ≥1.4 ng/mL is associated with surgical NEC and may be a potential indicator for risk of disease progression.
Procalcitonin (PCT) has been identified as a biomarker for the diagnosis of sepsis in both adult and pediatric populations.1–3 Although it plays a primary role in calcium homeostasis, PCT has been shown to increase in systemic inflammatory reactions. 4 Increasing within three to four hours of the initial insult, it can be used as an early predictor of illness and has been proposed as a potential biomarker for necrotizing enterocolitis (NEC).5,6
Although predominantly an intestinal disorder, NEC is also associated with systemic disease and can present with or without concomitant sepsis. 7 Common risk factors for NEC include low birth weight and prematurity, although normal-weight term infants up to three months old can also be affected.8,9 Necrotizing enterocolitis affects 5% of all infants admitted to neonatal intensive care units (NICUs) and up to 9% of infants between 22 and 29 weeks' gestational age. 7 The incidence has been reported to be as high as 20% at individual institutions. 7 Early diagnosis of NEC remains challenging given the subtle clinical picture. Often initially presenting as progressive feeding intolerance, NEC symptoms are frequently non-specific and can be attributed to a wide variety of other pathologies. 10
Once diagnosed, the severity of NEC must be stratified to patients who can be medically managed versus those who progress to requiring surgical intervention. Clinical and radiographic diagnostic features are the mainstay of defining the severity of NEC. 11 An updated version of the modified Bell's criteria, used to define NEC, is still in clinical use today. Surgical NEC, Bell's stage IIIB, is characterized by intestinal necrosis and perforation that requires prompt operative intervention. 12 Between 27% and 52% of infants diagnosed with NEC will ultimately require surgical intervention.12–14 Appropriate timing of operative treatment remains paramount to increasing survival but identifying the ideal timing of intervention remains difficult. Many infants with NEC who need surgical intervention may not display definitive signs that can delay operative care.
Once operative intervention is decided on, mortality rates remain as high as 50% even after intervention. 15 Up to 20% of infants with NEC die prior to receiving surgery. 15 Early operative intervention has been associated with reduction of morbidity and mortality associated with surgical NEC. 15 The addition of early biomarkers to the modified Bell's criteria has the potential to facilitate timely diagnosis and identify infants at high risk of progression to surgical NEC, providing benefit to both clinicians and patients.
This pilot study has three aims: to define the association between elevated PCT and NEC; to define the association between elevated PCT and surgical versus medical NEC; and finally, to determine if elevated PCT would differentiate infants with NEC from those with proven sepsis. We hypothesized that an elevated PCT would be associated with NEC as well as with surgical versus medical NEC.
Patients and Methods
Study design and setting
After obtaining Institutional Review Board (IRB) approval (#12655), we identified infants up to three months old who were admitted to Oklahoma Children's Hospital (Oklahoma City, OK) and had a PCT level drawn during admission between January 1, 2010, and January 1, 2021. Patients who were evaluated in the emergency department with a PCT level, but were ultimately discharged, were excluded (Fig. 1). This study was designed as a single-institution, retrospective case control analysis. Cases were defined as patients diagnosed with either NEC or sepsis. Controls included patients who were admitted without signs of infection. A retrospective chart review was conducted, and data were collected regarding demographics, date of diagnosis of NEC or sepsis, PCT level, whether surgery was performed, risk factors of developing NEC, symptoms, radiologic findings, and laboratory findings. Chart review for patients with NEC was continued for six months after diagnosis to evaluate for complications from NEC such as death, short bowel syndrome (SBS), and stricture formation.
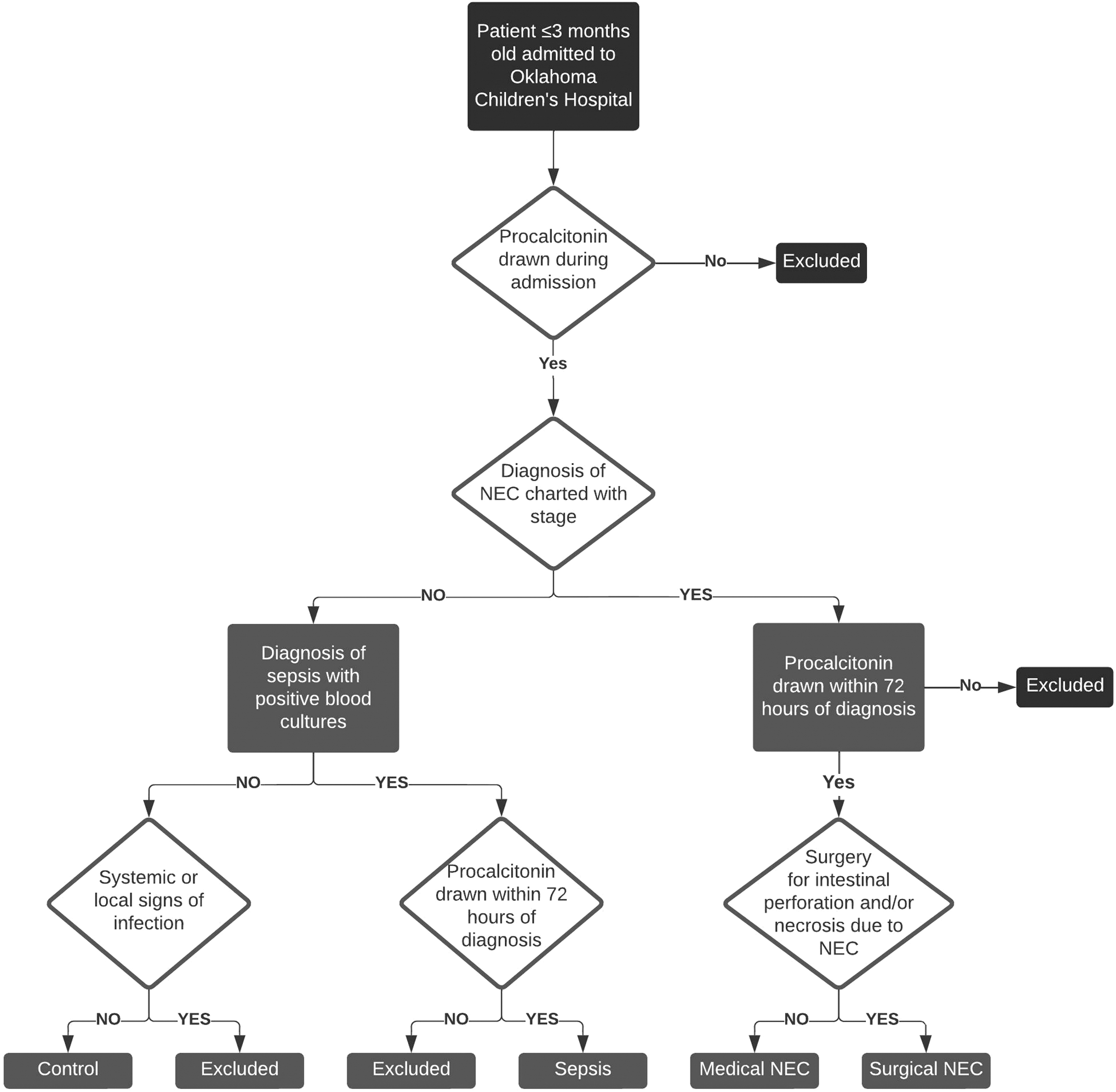
Flow diagram of patient inclusion for control, necrotizing enterocolitis (NEC), and sepsis groups.
Participants
Necrotizing enterocolitis
Patients with NEC had to have a diagnosis of NEC documented in the medical record along with the appropriate stage according to modified Bell's criteria. All stages of NEC were included. PCT had to be drawn within 72 hours before or after the diagnosis of NEC. Patients with recurrent NEC were included although a PCT had to be drawn within 72 hours of diagnosis of recurrence. Surgical NEC was defined as any patient who had intestinal perforation or necrosis secondary to NEC that required operative intervention regardless of initial staging (Fig. 1). Surgical pathology or documentation in the operative note had to confirm the diagnosis of surgical NEC. Patients were included in the surgical NEC group regardless of if the operative intervention was peritoneal drain placement or exploratory laparotomy. Only infants who required surgery in the acute phase of NEC were defined as surgical NEC. Infants who developed strictures several weeks after resolution of NEC were categorized as a subset of medical NEC. Patients with isolated, spontaneous intestinal perforation without additional signs of necrosis were excluded. Charts were reviewed to exclude those patients who had symptom improvement with dietary changes and had a diagnosis of food protein-induced enterocolitis syndrome (FPIES) or milk protein allergy. 16
Sepsis
The definition of sepsis in infants is variable. 17 Given that PCT is most frequently associated with bacteremia-associated sepsis, this article narrows the definition of sepsis accordingly. 17 Inclusion criteria for sepsis was at least one systemic symptom defined as hypotension, temperature instability, apnea, or bradycardia in addition to blood cultures positive for bacteria. A diagnosis of sepsis also had to be noted in the patient's chart (Fig. 1). Procalcitonin had to be drawn within 72 hours before or after the diagnosis of sepsis to be included. Patients who presented with isolated bacteremia or systemic symptoms in the absence of bacteremia were excluded.
Controls
Control patients were infants up to three months of age who were admitted to Oklahoma Children's Hospital and had a PCT level drawn during admission in the absence of infectious signs or symptoms. Patients with positive blood cultures or viral screens, history of systemic symptoms such as temperature instability, hypotension, apnea, and bradycardia were excluded. Patients with local signs of infection, such as erythematous and purulent wound drainage or urinary tract infections, were also excluded (Fig. 1). Examples of reasons for admission in control patients included seizures, feeding intolerance, and history of syncopal episodes at home. Control patients had PCT levels drawn in primarily two settings: the NICU/pediatric intensive care unit (PICU) or the emergency department. Both groups had PCT levels drawn as a part of a septic workup either because of concerning maternal or neonatal features. For patients in the NICU/PICU, most premature infants had a PCT value drawn as a part of routine septic workup regardless of symptoms. In addition, any infant whose mother had prolonged rupture of membranes, concerns for chorioamnitis, or had a history of drug use also had a PCT drawn as a part of the septic workup. In the emergency department, PCT was routinely drawn as a part of the septic workup for patients who presented with seizures reported by the parents at home, hypoglycemia, feeding intolerance, weakness, and failure to thrive. All patients whose workup revealed concerns for systemic or localized infection outside of an elevated PCT were excluded from the control group.
Data collection
Data were collected from electronic medical records and entered in a Research Electronic Data Capture (REDCap) database. Data included demographics, weight, date of admission, date of diagnosis of NEC or sepsis, PCT level (ng/mL), comorbidities, history of prematurity, radiologic findings, abdominal physical examination findings, systemic symptoms, modified Bell's staging (for patients with NEC), cause of sepsis (for sepsis patients), blood culture growth (for patients with bacteremia in both the NEC and sepsis groups), and PCT values. Comorbidities were grouped into neurologic, cardiac, pulmonary, gastrointestinal, renal, chromosomal, or other. They included both congenital and acquired medical conditions. Outcome data collected included surgery and long-term complications from NEC. Complications were defined as death, stricture, or SBS.
Variables
Primary outcomes of interest were PCT elevation and the development of surgical versus medical NEC or complications due to NEC. Secondary outcomes were PCT elevation in NEC versus control patients and NEC versus sepsis patients.
Potential confounders included patients with a concomitant diagnosis of NEC and sepsis that were included within the NEC group. Patients with NEC were staged using the modified Bell's criteria. 18
Statistical methods
Categorical variables were summarized using frequencies and proportions. Bivariable associations were assessed using Fisher exact, Monte-Carlos Exact, or χ 2 tests. Mean and standard deviation (SD) or median and interquartile range (IQR) were used to summarize continuous variables. Wilcoxon rank sum test, analysis of variance (ANOVA), Student t-test, and Kruskal-Wallis test were used to assess differences in continuous variables as appropriate. Recursive partitioning was used to find an optimal PCT cutoff to categorize PCT levels. Model discrimination and fit were assessed using the area under the curve (AUC) and Hosmer-Lemeshow goodness-of-fit statistics, respectively. Multinomial logistic regression was used to assess elevated PCT and associations with NEC, sepsis, and control groups adjusting for other covariates. Subgroup analysis was performed on patients with NEC excluding stage IA/IB because these stages are classified as suspected NEC. Statistical significance was assigned if p < 0.05. SAS 9.4 (SAS Institute, Cary, NC) or JMP Pro version 15.2.0 (SAS Institute) software was used for all data analytics.
Results
Participants
A total of 523 controls, 71 patients with sepsis, and 49 patients with NEC met inclusion criteria for their respective groups during the 11-year review period. The average PCT values for the control, NEC, and sepsis groups were 1.7, 17, and 28.1, respectively.
Descriptive data
Controls
Among the 523 controls, 50.2% were female, 49.8% were male (Table 1). Most patients were white (66.1%) without comorbidities (64.2%; Table 1). Fourteen control patients (2.7%) were missing data regarding ethnicity. Premature infants comprised 29.1% of the control group with the majority of these defined as moderate to late preterm (32–37 weeks' gestational age; n = 101; 66.4%). Median estimated gestational age (EGA) at birth was 38.4 weeks.
Sociodemographic and Clinical Characteristics of Control, Patients With NEC, and Patients With Sepsis
NEC = necrotizing enterocolitis; IQR = interquartile range; EGA = estimated gestational age; cGA = corrected gestational age; SD = standard deviation.
NEC
There were 49 patients diagnosed with NEC who met the inclusion criteria of whom 33 were diagnosed with medical NEC and 16 were diagnosed with surgical NEC. Most patients were white (58.3%) males (55.1%) with a history of prematurity at birth (79.6%) and had one or more comorbidities (69.4%; Table 1). There was a difference in gender (75% male in the surgical NEC versus 45.5% in the medical NEC group; p = 0.05) and race (p = 0.02) between the medical and surgical NEC groups (Table 2). The median EGA was 30.9 weeks at birth and 35.0 weeks at date of diagnosis. There were no patients with recurrent NEC in the medical group. There were two patients with recurrent NEC in the surgical NEC group. Both patients underwent successful treatment for medical NEC with complete resolution of symptoms before recurrence. Three patients in the surgical NEC group were initially staged with medical NEC but progressed to requiring acute operative intervention. Two patients in the surgical NEC group underwent peritoneal drain placement alone whereas the remaining 14 underwent exploratory laparotomy.
Sociodemographic and Clinical Characteristics of Medical Versus Surgical Patients With NEC
NEC = necrotizing enterocolitis; IQR = interquartile range; EGA = estimated gestational age; cGA = corrected gestational age; SD = standard deviation.
There were six patients who had concomitant bacteremia at the time of diagnosis of NEC. Among these patients, one grew Escherichia coli, two grew Klebsiella oxytoca, one grew methicillin-resistant Staphylococcus epidermidis, one grew coagulase-negative staphylococci, and the final patient grew methicillin-sensitive Staphylococcus aureus. Five of these patients progressed to surgical NEC. The mortality was 50% among patients who had both bacteremia and NEC. Most patients within the medical NEC group were stage IIA (30.3%). This was followed by IB (27.3%), IA (21.2%), IIB (15.2%), and IIIA (6.1%).
Sepsis
There were 71 patients diagnosed with sepsis who met the inclusion criteria. Most of these patients were also male (57.8%), white (57.1%), and had one or more comorbidities (52.9%; Table 1). However, only 39.4% of these patients had a history of prematurity, which was significantly lower when compared with the NEC group (p < 0.0001). The median EGA was 37.3 weeks at birth and 40.8 weeks at the date of diagnosis, which was older compared with to the NEC group (p < 0.0001; Table 1). Most blood cultures in this patient population were Escherichia coli (23%), Staphylococcus aureus (16%), group B Streptococcus (16%) or Staphylococcus epidermidis (16%). The most common causes of sepsis were unknown (positive blood cultures without an identified source, 35%), urinary tract infections (25%), upper respiratory infections (11%), and meningitis (10%).
Main results
Procalcitonin ≥1.4 ng/mL is associated with NEC compared with controls
Logistic regression identified a statistically significant association between PCT ≥1.4 ng/mL and NEC compared with controls (p < 0.0001). This association held when adjusting for prematurity (odds ratio [OR], 28.46; 95% confidence interval [CI], 11.27–71.88) and excluding stage IA/IB (p < 0.0001). The receiver operating characteristics (ROC) model showed an area under the curve (AUC) of 0.84 when stage IA/IB were included and 0.89 when stage IA/IB were excluded.
Procalcitonin ≥1.4 ng/mL is associated with surgical NEC compared with medical NEC
There was no difference in the EGA at birth, corrected gestational age at diagnosis, distribution of prematurity or comorbidities between medical and surgical NEC (p > 0.05; Table 2). This remained true when excluding stage IA and IB (p > 0.05).
There was also no statistically significant difference between the two groups regarding timing between PCT collection and diagnosis of NEC (p > 0.05). The majority of medical (78.8%) and surgical (87.5%) patients with NEC had a PCT drawn either before or the day of being diagnosed with NEC (Table 2).
A PCT value ≥1.4 ng/mL was associated with surgical compared with medical NEC (87.5% vs. 39.4%; p = 0.002; Fig. 2). This remained significant after controlling for prematurity with 10.71 higher odds of a patient with PCT ≥1.4 ng/mL having surgical compared with medical NEC (adjusted odds ratio [aOR], 10.71; 95% CI, 2.08– 55.23). This significance was lost when excluding stage IA and IB NEC (p = 0.06; aOR, 5.87; 95% CI, 0.995–34.58).
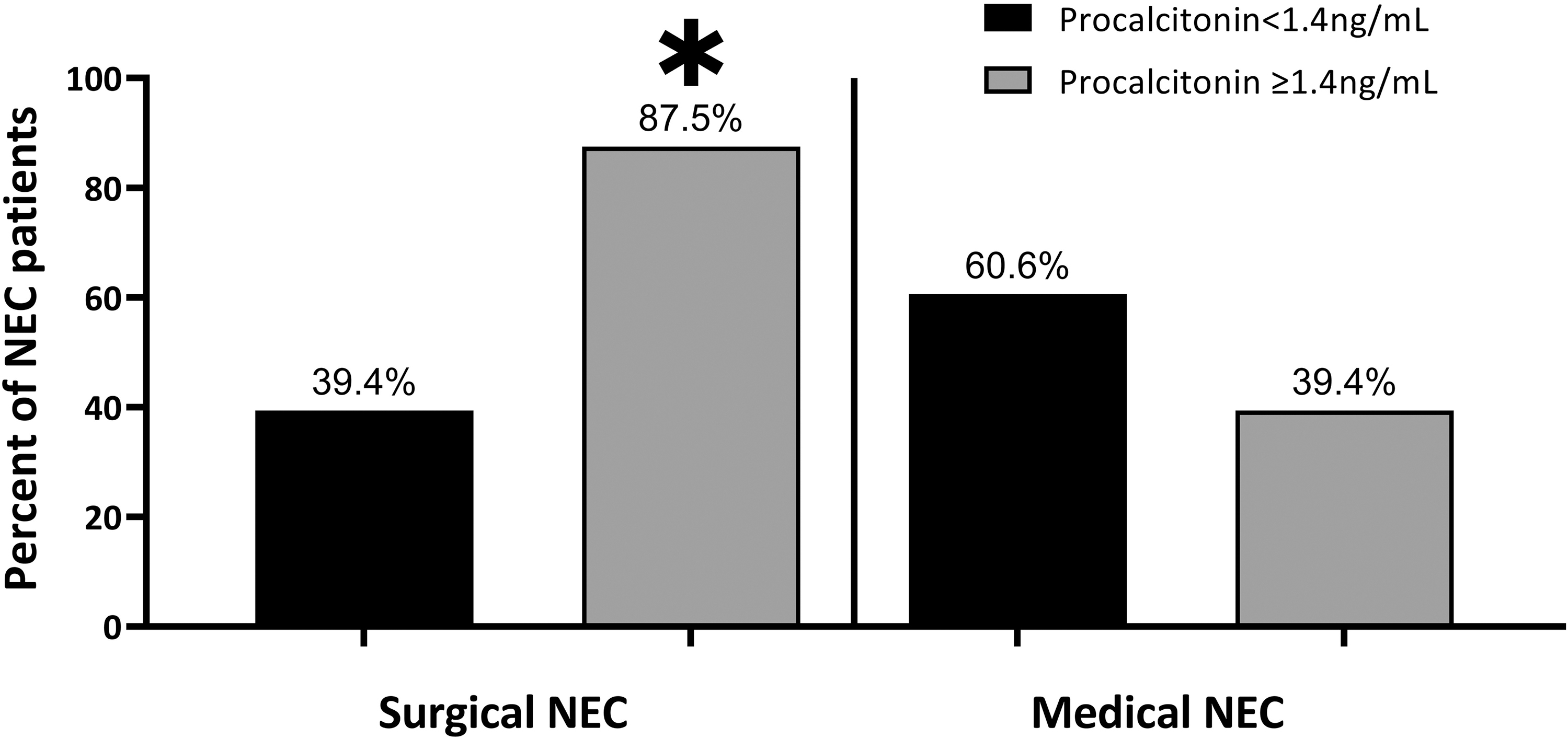
Percent of patients with necrotizing enterocolitis (NEC) who required surgery because of intestinal perforation or necrosis versus those who were underwent medical management alone (p = 0.002; adjusted odds ratio [aOR], 10.71 for surgical NEC, 95% confidence interval [CI], 2.08–55.23).
Procalcitonin cannot differentiate between sepsis and NEC
There was an association between elevated PCT and both sepsis and NEC (medical and surgical) compared with controls. When considering sepsis, additional PCT cutoff values were identified by recursive partitioning. These values were <1.4 ng/mL, 1.4–3.19 ng/mL, and >3.19 ng/mL. After controlling for prematurity, a PCT between 1.4 ng/mL and 3.19 ng/mL was associated with both NEC (aOR, 11.43; 95% CI, 2.57–50.78) and sepsis (aOR, 6.63; 95% CI, 2.66–16.55). When using a PCT cutoff value of 3.19 ng/mL, they both remained significantly associated but, the odds ratio of having sepsis increased over NEC (aOR, 19.55; 95% CI, 10.46–36.51 vs. aOR, 10.77; 95% CI, 3.23–35.89).
Compared with controls, patients with abdominal distention had 48.46 times higher odds of having a diagnosis of NEC (95% CI, 16.36–143.47). In contrast, abdominal distention was not associated with sepsis (aOR, 1.2; 95% CI, 0.40–3.60).
Subgroup analysis
Elevated PCT is not associated with complications related to NEC
There was a statistically significant association between PCT ≥1.4 ng/mL and the presence of any complications related to NEC (73.7% of patients with complications had a PCT ≥1.4 ng/mL compared with 43.3% of patients without complications, p = 0.04; Fig. 3). However, subanalysis did not demonstrate an association between PCT ≥1.4 ng/mL and stricture (p = 0.36), SBS (p = 1), or death (p = 0.18). Similarly, the association between elevated PCT and any complication became insignificant when stage IA and IB NEC were excluded (p = 0.28).
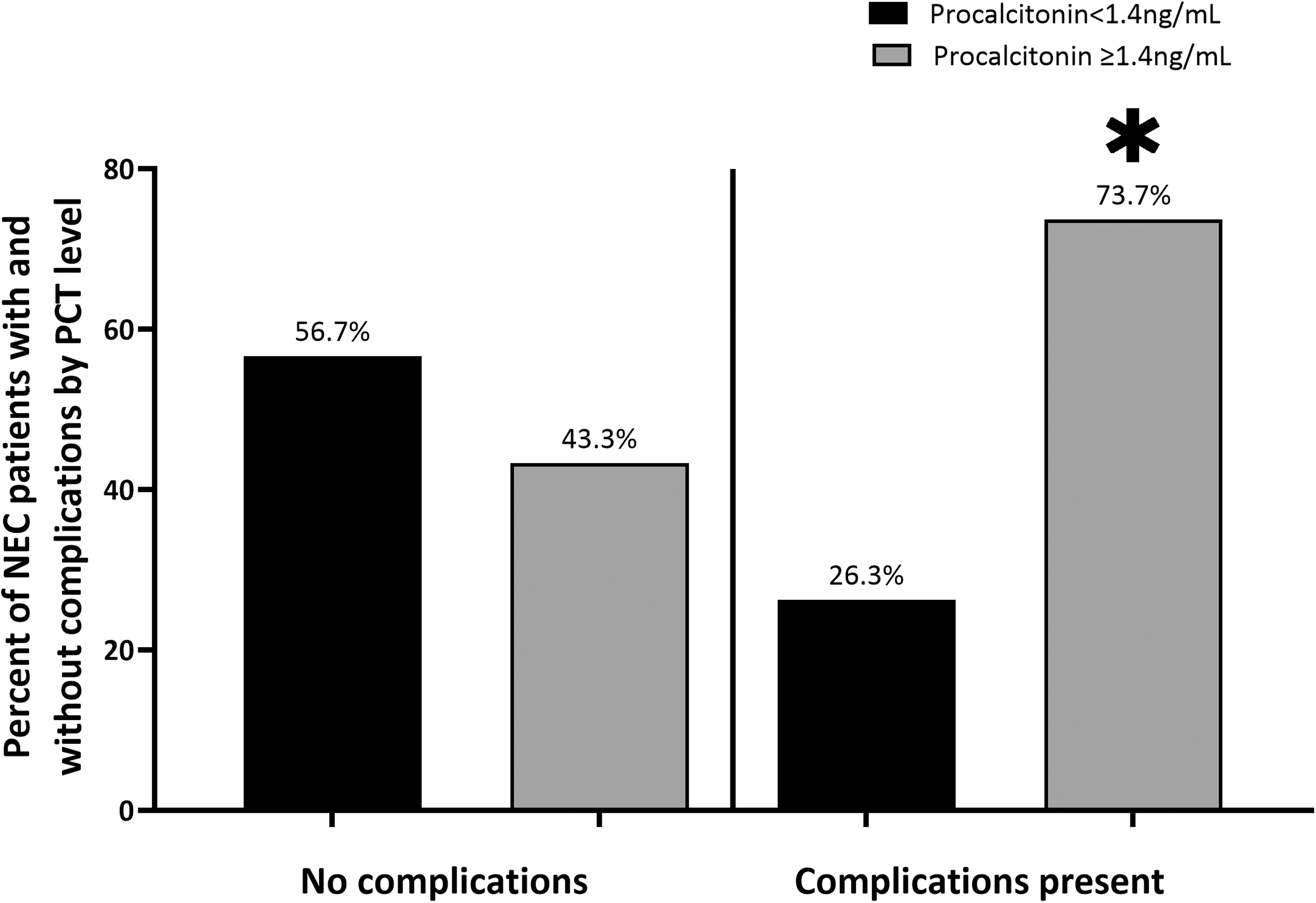
Percent of patients with necrotizing enterocolitis (NEC; medical and surgical) who developed complications related to NEC versus those who did not stratified by procalcitonin (PCT) level greater or less than 1.4 ng/mL (73.7% of patients with NEC with complications had a PCT ≥1.4 ng/mL compared with 43.3% of patients with NEC without complications;
Discussion
Key results
This study demonstrates that a PCT ≥1.4 ng/mL is associated with surgical versus medical NEC. It is also associated with NEC compared with controls. Elevated PCT is associated with both sepsis and NEC but in the presence of abdominal distention, is associated with NEC compared with sepsis. Procalcitonin elevation is not associated with complications secondary to NEC.
Limitations
This study cannot be used to infer risk of developing NEC based on PCT values because of its retrospective nature. There is also selection bias because not all patients diagnosed with NEC have a PCT drawn. Given that PCT is most often drawn as a marker for systemic inflammation and sepsis, patients who had a PCT drawn and were subsequently diagnosed with NEC may have had more clinical similarities to sepsis. The timing of PCT collection is another limitation in that they were drawn either 72 hours before or after the diagnosis, with the majority of PCTs drawn the day of diagnosis. This limits our ability to determine the relation between timing of the PCT draw and development of NEC.
Furthermore, the time to peak PCT value and resultant decrease to normal is unknown in patients with NEC. Understanding the trend of PCT in NEC is necessary to give better insight into the management of NEC. Further studies are needed to understand the relation between the trend of PCT values and NEC. The sample size of the NEC and sepsis groups are also low, leading to larger confidence intervals and cutoff values that may change with additional data. Finally, this study was unable to age match control patients with patients with NEC, which may introduce confounding bias.
Interpretations
Various biomarkers such as C-reactive protein (CRP), calprotectin, intestinal fatty acid-binding protein, serum amyloid-A protein, and others have been suggested as potential biomarkers in the diagnosis of NEC. 19 Although promising, no biomarker for NEC has been validated successfully. Varying reports of both elevated and decreased levels of PCT have been reported in patients with NEC with no consensus in the literature.5,6,19–22 Currently, only one study has examined PCT as a predictor of surgical NEC but no difference in PCT was found between the medical and surgical groups. 22
Identification of a biomarker that can differentiate between patients with NEC who will resolve with medical management alone versus those who will progress to requiring operative intervention is important. 23 Necrotizing enterocolitis is often a diagnostic challenge because the signs and symptoms can be variable and the disease may progress quickly and without warning. 23 Enhancing our ability to identify those at-risk of requiring an operation before they develop definitive signs and symptoms would be invaluable. At our institution, PCT is a readily available in-house test that takes approximately 20 to 30 minutes to result after it is drawn. It is relatively expensive for patients without insurance, costing $100 at our institution. However, the cost is lower to patients with insurance and financial assistance is available for low-income patients making the test more financially feasible. This study demonstrates that in patients with NEC, PCT ≥1.4 ng/mL is associated with an increased need for surgical intervention. Because PCT can increase within three hours of initial insult, using it as a biomarker may improve morbidity and mortality by helping the clinician initiate earlier operative intervention versus continuing with medical management alone. 24
This study also demonstrates that elevated PCT is associated with NEC compared with controls. The diagnosis of NEC can be challenging and may mimic many other diseases such as sepsis, cow's milk protein allergy, spontaneous intestinal perforation, congenital abnormalities (such as intestinal stenosis or meconium plug syndrome), and feeding intolerance of prematurity, among others.25–27 Given the association of PCT with NEC and because it increases as a part of the inflammatory response, an elevated PCT may help the clinician narrow the differential diagnosis of a patient ultimately diagnosed with NEC.
Although it may help narrow the differential diagnosis to exclude non-inflammatory diseases that mimic NEC, when used alone, an elevated PCT is unable to differentiate reliably between NEC and sepsis. This study shows that this association changes when put in the context of physical examination and degree of PCT elevation. These findings indicate that in the setting of abdominal distention and a moderately elevated PCT, there is a higher likelihood of a diagnosis of NEC versus sepsis. This study also demonstrates that a benign abdominal examination and elevated PCT increases the likelihood for a diagnosis of sepsis although further studies with higher patient numbers are needed to better elucidate these findings.
This work lays the groundwork for future prospective studies to determine if PCT can be used as a predictor for early surgical NEC. Prospective studies collecting serial PCT measurements are needed to determine a temporal association between rise in PCT and development of NEC. Further studies are also needed to determine if earlier operative intervention based on these values leads to improved clinical outcomes.
Generalizability
The generalizability of this study is limited by its retrospective nature coming from a single institution. A multicenter study is needed to better determine if the findings of this study can be more broadly applied.
Conclusions
A PCT of ≥1.4 ng/mL is associated with surgical NEC and may be a potential indicator for risk of disease progression.
Footnotes
Acknowledgments
We would like to thank the Departments of Pediatric Surgery and Neonatology for their partnership in helping bring this work to completion. We would also like to thank Dr. Erynn Bergner (Oklahoma Children's Hospital, Neonatal-Perinatal Medicine) for her assistance in study design.
Authors' Contributions
Conceptualization: Liebe, Lewis, Hunter. Methodology: Liebe, Lewis, Stewart, Hunter. Investigation: Liebe, Lewis, Loerke, Golubkova, Leiva. Writing–original draft: Liebe. Writing–review and editing: Lewis, Loerke, Golubkova, Leiva, Stewart, Gin, Porter, Chaaban, Hunter. Visualization: Liebe. Project administration: Liebe, Hunter. Data curation: Loerke, Golubkova, Leiva, Sarwar, Gin, Porter. Formal analysis: Stewart, Sarwar. Resources: Stewart, Hunter. Software: Sarwar. Validation: Hunter. Supervision: Hunter.
Funding Information
No funding was used for this project.
Author Disclosure Statement
The authors have nothing to disclose and no conflicts of interest.