
Abstract
Background:
Post-operative organ/space infection (OSI) is associated with prolonged hospital stay or re-admission. Here, we explore the predictors for OSI in pediatric patients after appendectomy.
Patients and Methods:
Among post-appendectomy pateints, the OSI was reviewed. A multicenter case control study was conducted to explore the risk factors for OSI among pediatric patients with appendicitis after appendectomy between January 2009 and December 2019. The potential risk factors associated with OSI were explored using multivariable logistic regression methods.
Results:
In the current cohort, 723 patients fulfilled the OSI criteria. According to multivariable logistic regression analysis, the occurrence of OSI was associated with complicated appendicitis (odds ratio [OR], 1.82; 95% confidence interval [CI], 1.03–3.686; p = 0.016), the lower the level of pre-operative lymphocyte-C-reactive protein (LCR; OR, 14.42; 95% CI, 1.57–73.26; p < 0.001), pan-peritonitis (OR, 4.36; 95% CI, 1.34–21.66; p = 0.006), systemic inflammatory response syndrome (SIRS; OR, 8.22; 95% CI, 1.84–49.63; p < 0.001), and abscess presentation (OR, 11.32; 95% CI, 2.03–61.86; p < 0.001). The receiver operating characteristic (ROC) curve evaluation further confirmed the relatively high accuracy of the above factors to predict OSI.
Conclusions:
The identified potential risk factors in the current research can be used for OSI identification in patients after appendectomy. Recognition of the risk factors may allow the choice of the treatment process more reasonably.
The most common abdominal emergency in the pediatric population is acute appendicitis,1,2 complications of which can include perforated appendicitis and gangrenous appendicitis, accounting for approximately one-third of the whole appendicitis population.3,4 Post-operative organ/space infection (OSI) developed in approximately 5% of pediatric patients after appendectomy, and in the cohort of complicated appendicitis, the rate of post-operative OSI may be as high as 25%.5,6 Organ/space infection cannot be completely avoided, although various improvement s have been widely adopted. Usually, post-operative OSI requires intravenous antibiotic agents and drainage, and accounts for the most frequent cause of a prolonged hospital stay or re-admission.7,8
The identification of potential post-operative OSI patients is critical to increase vigilance and achieve timely and accurate intervention. 9 The disease severity and operative approach had been implicated for the occurrence of OSI in several recent studies.9–12 However, a broader scope of variables regarding the surgical features need to be further elucidated, especially in specific pediatric conditions. In this study, we investigated the incidence of OSI in patients who underwent appendectomy, and we also explored the predictors of OSI to improve patient outcomes.
Materials and Methods
Patient population
A cohort of post-appendectomy patients was collected and reviewed from a collaborative program at three tertiary pediatric general surgical departments between April 2008 and December 2020 at Chongqing Children's Hospital, Chongqing Health Center for Women and Children, Chongqing Three Gorges Central Hospital. A case control analysis was conducted to investigate the risk factor for OSI. The Institutional Review Board of each site approved the current protocol with protection of personal information. The need for patient consent was waived because of the retrospective routine care review without interventions. A study flow chart is presented in Figure 1, describing patient inclusion and exclusion.
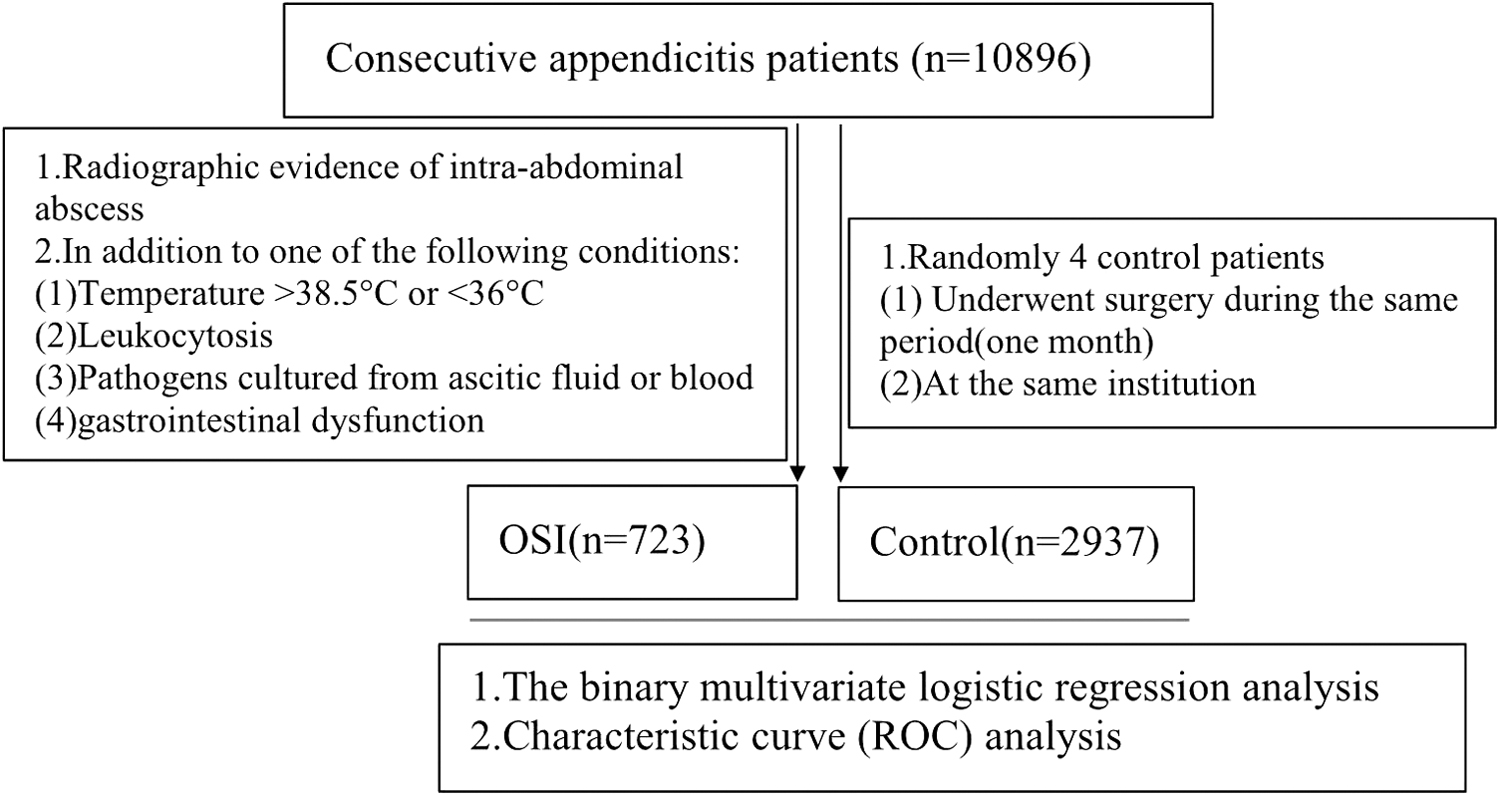
Flow chart of patient inclusion, and analysis. ROC = receiver operating characteristic curve.
At the involved institutes, the diagnosis of appendicitis is evaluated comprehensively at initial presentation, including physical examination, laboratory results, and abdominal imaging findings. The surgical decision and the surgical approaches (laparoscopic or open procedures) were made depending on patient selection, disease involvement, and surgical team preference.
After emergency operation, the antibiotic usage and management were identical for all patients, including antibiotic doses and dose intervals. The first dose of broad-spectrum antibiotic therapy was administered one hour pre-operatively.
The standard protocol of post-operative antibiotic agents after appendectomy comprised patients receiving an intravenous fluid bolus of broad-spectrum antibiotic therapy with either piperacillin/tazobactam (100–150 mg/kg/d in two divided doses) or cefoperazone sodium and sulbactam (100–150 mg/kg per dose in two divided doses) as well as metronidazole (30 mg/kg per dose in two divided doses). The antibiotic agents should be adjusted according to the results for bacterial culture at four to five days post-operatively. The protocol continued until the serum C-reactive protein (CRP) level is below 1.0 mg/dL as well as the leukocyte count and temperature had returned to normal, or a minimum of five days. At least two assessments were performed on all patients every morning and afternoon to determine whether they met discharge criteria.
Systemic inflammatory response syndrome (SIRS) is defined following the International Pediatric Sepsis Consensus Conference guidelines, including at least two of the following four criteria upon initial presentation: temperature >38.5°C or <36°C; respiratory rate greater than two standard deviations for the patient's age; heart rate greater than two standard deviations for the patient's age; leukocytosis elevated or depressed from normal value for the patient's age. The post-operative OSI was defined with the following criteria within 30 days after the operative procedure: intra-abdominal abscess under imaging evaluation, as well as one of the following four criteria: temperature >38.5°C or <36°C and leukocytosis elevated or depressed from normal value for the patient's age; pathogens positive in blood or ascitic fluid; and gastrointestinal symptoms, including vomiting, abdominal pain, and distention. An episode of blood stream infections was defined according to the presence of clinical sepsis and the identification of pathogens, which included any bacteria isolated from at least one blood culture. 13
For the case group, the patients included in the analysis were those identified with post-operative OSI after appendectomy. Controls were five randomly selected cases for a given OSI case among patients operated on for emergency appendicitis at the same institution during the same period (approximately one month). The inclusion criteria were as follows: age >0.5 years and <16 years; no steroid or immunosuppressive medication administration. The exclusion criteria were a history of laparotomy; the patients managed with interval appendectomy; antibiotic allergy. All the electronic clinical data for the case and control samples were collected and independently reviewed by two investigators with specific training.
Statistical analysis
The data manipulation and statistical analysis were then conducted using SPSS Statistics, version 26, (IBM Corp, Armonk, NY). The data distribution was initially assessed utilizing Kolmogorov-Smirnov test. The continuous data were expresssed as the means ± standard deviations and the medians (interquartile ranges) for normally and non-normally distributed variables, respectively, and processed using the independent Student t-test and the Mann-Whitney U test, respectively. The categorical data were presented as frequencies (percentages) and conducted using the χ 2 test or Fisher exact test, with the relative risk estimation. Univariable analysis was performed to identify the association of all predictor variables with the primary dichotomous outcome (post-operative OSI vs. control). The binary multivariable unconditional logistic regression analysis was further performed with the variables in univariable analysis (p < 0.2). Receiver operative characteristic (ROC) curve analysis was further performed to evaluate the area under the curve (AUC) to determine the ideal predictive value of the specific measurements(best sensitivity and best specificity simultaneously). The significant difference was considered as p < 0.05.
Results
During the study period, a total of 10,896 consecutive appendicitis patients underwent appendectomy between April 2008 and December 2020. Overall, OSI was diagnosed in 723 (6.9%) patients, who were reviewed in the present research. Among them, 93 patients were subjected to percutaneous or transrectal drainage because of a huge abscess and persistent fever.
The detailed description of baseline clinical characteristics between the OSI and control groups is presented in Table 1. Regarding the age of patients, it was somewhat younger for the OSI group than that of the control group (p = 0.038). Furthermore, there was a severe pre-operative comorbidity presented in the patients with OSI, such as pan-peritonitis (p < 0.001), pre-operative abscess (p < 0.001), and SIRS (p = 0.004), suggesting its potential as the risk factors. Among the pre-operative laboratory parameters, white blood cell (WBC) count (p = 0.021), CRP (p < 0.001), and lymphocyte-C-reactive protein (LCR; p < 0.001) were presented as more severe in those patients with OSI compared with those without OSI, suggesting the severe intra-abdominal inflammation. Moreover, microbiologic positive was more common in the OSI group (p = 0.001), along with a longer antibody utilization (data not shown). Interestingly, the laparoscopic operation presented as a protective factor for the OSI (p = 0.007). No differences were presented in terms of intra-operative parameters, such as operative blood loss and surgical duration (Table 1). Multivariable regression further determined the OSI associated independent risk factors utilizing a hierarchical forward stepwise approach with the variables introduction that were determined in the univariable analysis.
Baseline Demographics and the Initial Operative Characteristics of Patients
Recurrence: intussusception occurred before admission.
ALB = Albumin; ASA = American Society of Anesthesiologists; CAR = C-reactive protein to albumin ratio; CRP = C-reactive protein; EBL = Estimated blood loss; Hb = hemoglobin; IQR = interquartile range; LCR = lymphocyte-C-reactive protien ratio; NLR = neutrophil-lymphocyte ratio; OSI = organ/space infection; PLR = platelet-lymphocyte ratio; SD = standard deviation; SIRS = systemic inflammatory response syndrome; WBC = white blood cell count.
As shown in Table 2, five independent risk factors related to OSI were confirmed, including complicated appendicitis (OR, 1.82; 95% CI, 1.03–3.686; p = 0.016), the pre-operative LCR level (OR, 14.42; 95% CI, 1.57–73.26; p < 0.001), the worse symptoms (pan-peritonitis) (OR, 4.36; 95% CI, 1.34–21.66; p = 0.006), SIRS (OR, 8.22; 95% CI, 1.84–49.63; p < 0.001), and pre-operative abscess 2 cm or more (OR, 11.32; 95% CI, 2.03–61.86; p < 0.001), which were independent predictors of OSI. The ROC analysis for the AUC is presented in Table 3. The above predictors, including elevated CRP, pan-peritonitis, abscess 2 cm or more, SIRS, and LCR could predict OSI with a relatively high accuracy (Table 3).
Multivariable Regression Analysis of Factors Associated With Bile Leakage
OR = odds ratio; CI = confidence interval; SIRS = systemic inflammatory response syndrome; LCR = lymphocyte-C-reactive protein ratio.
Receiver Operating Characteristic Curve Results and Sensitivity, Specificity Values
CRP = C-reactive protein; SIRS = systemic inflammatory response syndrome; LCR = lymphocyte-C-reactive protein ratio; CI = confidence interval; NPV = negative predictive value; PPV = positive predictive value.
Discussion
In the present research, we explored the various variables associated with post-operative OSIs among pediatric patients, a common post-operative complication after appendectomy. We explored the incidence of post-operative OSI involved in the current cohort. We further identified five variables as independent risk factors for post-operative OSI. To our knowledge, the current results are the first to report an accurate benchmark to definitively predict post-operative OSI, which is required for prompt management after appendectomy among pediatric patients.
Post-operative OSI continues to be a common and serious complication with a high impact on length of stay and total cost, although the management experience for different forms of appendicitis is more and more rich. 14 The incidence for OSI varied substantially (1.6%–14.4%), especially in the most likely conditions for abscess formation, complicated appendicitis, such as gangrenous and perforated appendicitis.15–17 We explored the incidence of post-operative OSI and blood stream infection after appendectomy and investigated the associated risk factors. Consistent with previous reports for a relatively higher post-operative OSI rate, we detected a 6.9% incidence after appendectomy. An additional secondary blood stream infection with OSI was detected in 4.9% of our patients. In our routine clinical practice, the blood cultures were not taken routinely, and the diagnosis criteria of OSI do not need blood microbiologic data. In our patients, OSI was diagnosed after signs of infection followed by radiologic evidence and are not always verified with microbiologic data. Furthermore, the total incidence of OSI may be obscured because of early aggressive antibiotic agent treatment, which may confuse the diagnosis.
In the current cohort, follow-up has been of relatively long duration. Approximately 11% of the patients developed an intra-abdominal abscess. The source of infection was an intra-abdominal abscess in 68% within seven days after appendectomy. If these are lacking, the patient may be temporarily discharged from the hospital, only to be re-admitted later (32%). The primary infection or the secondary blood stream infection were presented late in a substantial number of patients and the OSI may be diagnosed late.18,19 This is supported by the findings of Jen et al., 20 in which 12.3% of the patients developed post-operative intra-abdominal abscess within 30 days after appendectomy, and approximately 5% of the re-admissions were because of persistent abscess. 21 Unfortunately, the blood stream infection was not evaluated for every case with OSI identification.
Consistent with this, in the current cohort, approximately 20% of all the intra-abdominal infections were diagnosed late and led to re-admission within one month, which constitutes the common reason for re-admission. Under appropriate management, such as percutaneous or transrectal drainage, the persistent abscess and the severity of inflammation can achieve improvement.
Effective post-operative OSI prevention requires risk recognition for the involved clinical condition. Many predictors have been suggested to be associated with the development of OSI.9,14 Until now, no associated clinical factors have been identified among pediatric patients with appendicitis. In the present research, we detected several risk factors as independent risk factors for OSI, including severe symptoms such as pan-peritonitis, representing the presence of acute inflammation and the poor performance status. Severe complicated disease, such as severe appendicitis, gangrenous and perforated appendicitis, and low levels of pre-operative albumin (ALB) have been associated with increased OSI incidence. In the previous report, post-operative need for the intensive care unit reflects the comorbidities. 22 This association may be well explained by the overall status of the patients.
C-reactive protein alone is a good factor as an inflammatory marker, whereas peripheral lymphocytes represents the host's cytotoxic immune response to intestinal microflora. The LCR value is the combination of the inflammatory and immunologic response. In various clinical settings, the rapid response indicator for systemic inflammatory responses during the pre-operative period is found to be the LCR value.23–25 We further found that LCR was strongly related with the occurrence of post-operative OSI. We suggested in the current patients with appendicitis that low LCR value means the high risk of OSI, with an enhancement of SIRS. To our knowledge, the LCR was first used in the prediction of OSI here in the present research.
Previous research has suggested that the disease severity drives the occurrence of post-operative OSI after pediatric appendectomy. In this study, we further detected that pan-peritonitis, abscess on admission, and SIRS reflecting aspects of disease severity were additional independent risk factors for OSI after appendectomy. Furthermore, pre-operative sepsis and longer operative times were also the significant predictors of OSI in previous research. 13 As suggested, there were 4.9 occurrences of OSI in patients with complicated appendicitis compared with that of uncomplicated appendicitis. 9 The inflammation and edema may indeed develop to fluid exudation and deposition within the abdominal cavity, which have been suggested to be related to OSI occurrence.26,27 However, in the current research, the peritoneal drain placement in the abdominal cavity did not show difference between the two groups from the current cohort, which should be confirmed in the future research.
Laparoscopic surgical procedures continue to increase in recent years, and the utilization of laparoscopic operations was striking, nearly as high as 90% overall. 28 As suggested, laparoscopic operation is relative difficult and should be monitored carefully as well as performed skillfully. Interestingly, in the present research, use of minimally invasive techniques seem to confer a prophylactic effect. The selection of operative approach was decided by the individual surgeon, which is non-random; the concern exists that there may be integral differences. Open surgery may be more likely performed on a child who appears acutely ill. Surgeons may generally favor a particular operative procedure due to years of experience and have different outcomes compared with those still learning. 29
The present study has potential weaknesses that need to be considered when seeking generalization. The first limitation is the retrospective research covering a long time period in which an inherent risk of selection bias may exist for the data. Second, the protocol in patient management and care was only decided by each surgeon's experience, which was not randomly determined. Because of the data limitation, many cases of OSI are identified late or not included in the current cohort. Hence, the current data should not be arbitrarily interpreted as a conclusion that any surgical intervention should be performed aggressively.
Conclusions
In conclusion, the present study highlights several clinical variables for post-operative OSI after appendectomy. Future multicenter prospective clinical studies in the future with identical criteria and robust evidence for OSI should be performed to confirm the conclusions of the present research.
Footnotes
Authors' Contributions
Xia, Chen, Liu, and Guo designed the study and analyzed the data. Chen and Yan evaluated the manuscript. Liu, Ghen, and Yan performed the statistical measurements and analyzed the data. Guo and Yan analyzed the data, and Guo wrote the manuscript. All authors read and approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding Information
This study was supported by grants from the Key Project of the Chongqing Natural Science Foundation (CSTC, 2008BA0021, cstc2012jjA0155) for collection, analysis, and interpretation of data and Chongqing Health Planning Commission of Research Fund (No: 2016MSXM044) in writing the manuscript. The funding agency paid for the scholarships of the students involved in the research.
Author Disclosure Statement
The authors declare that they have no competing interests. All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.