
Abstract
Anastomotic leak after colorectal surgery is a devastating complication that may require re-operation, diverting stoma creation, and prolonged wound healing. Anastomotic leak is associated with a mortality of 4% to 20%. Despite intense research and novel approaches, the anastomotic leak rate has failed to substantially improve over the past decade. Adequate anastomotic healing requires collagen deposition and remodeling through post-translational modification. The human gut microbiome has been previously implicated as a key driver of wound and anastomotic complications. Specific microbes function in a pathogenic fashion by propagating anastomotic leak and poor wound healing. The two most studied organisms, Enterococcus faecalis and Pseudomonas aeruginosa, can be collagenolytic and may activate additional enzymatic pathways that lyse connective tissue. Furthermore, these microbes are enriched in post-operative anastomotic tissue as identified using 16S rRNA sequencing. Commonly encountered stressors including antibiotic administration, a Western (i.e., high-fat, low-fiber) diet, and concomitant infection can trigger dysbiosis and induce a pathobiome phenotype. Therefore, personalized microbiome modulation to maintain homeostasis may be the next step in improving the anastomotic leak rate. Oral phosphate analogs, tranexamic acid, and pre-operative diet rehabilitation have shown promise in in vitro and in vivo studies as ways to address the pathogenic microbiome. However, further translational human studies are required to validate findings. Accordingly, this article reviews the gut microbiome as it pertains to post-operative anastomotic leak, explores microbial impact on anastomotic healing, describes the shift from the commensal microbiome to a pathobiome, and introduces potential therapies to mitigate anastomotic leak risk.
Anastomotic leak after colorectal surgery (CRS) is a complication associated with substantial morbidity, mortality, and cost. Management of anastomotic leak frequently requires re-operation, diverting stoma creation, and a period of prolonged wound healing. Mortality following anastomotic leak spans 4% to 20%.1,2 Post-operative leak rates vary in frequency by anastomotic location.3–5 Even with recent technologic developments, including fluorescence angiography to confirm adequate perfusion, increased use of robotic and minimally invasive techniques, and research to identify and manage anastomotic leak risk factors (i.e., stapled versus handsewn and timing of resection after neoadjuvant chemoradiation), anastomotic leak rates have remained constant over the previous decade.4–6
The initiation of the Integrative Human Microbiome Project (phase 2 of the initial Human Microbiome Project) has led to renewed interest in characterizing and understanding the role of gastrointestinal flora in many clinical conditions. Studies have implicated microbiome imbalance, or dysbiosis, as a possible mechanism for many conditions including post-operative complications and sepsis. 7 Liu et al. 8 demonstrated that patients with sepsis have microbiomes with significant Fusobacteriia and Gammaproteobacteria enrichment. This dysbiosis was associated with a decrease in physiologic metabolic pathway activity and an increase in inflammatory pathway activity leading to an increased susceptibility to end organ damage. Van Praagh et al. 9 performed Illumina MiSeq using end-to-end anastomotic “donut” samples to study microbial community composition at the time of surgery. Principal component analysis demonstrated that microbiome diversity was negatively correlated with developing an anastomotic leak (e.g., diversity supports healing) and that patients who developed leaks had microbiomes with increases in Lachnospiraceae and Bacteroidaceae populations. Such a shift in the commensal microbiome that leads to untoward host impacts has been termed the pathobiome.
Both non-modifiable and modifiable factors influence an individual's microbiome, including age, gender, genetics, body mass index, and diet. Of these influences, diet presents itself as a seemingly readily modifiable factor with potential benefits extending to peri-operative microbiome optimization. 10 It is imperative for surgeons to have an understanding and an appreciation for the role of the microbiome throughout their patient's peri-operative course. Herein, we review the gut microbiome as it pertains to post-operative anastomotic leak, explore microbial impact on anastomotic healing, describe the shift from the commensal microbiome to a pathobiome, and introduce potential therapies to mitigate anastomotic leak risk.
Importance of the Human Gut Microbiome in Pathologic States
The human microbiome houses a combination of both protective and pathogenic bacteria. Health is dependent upon maintaining a homeostatic balance between both microbial populations. A balanced gastrointestinal microbiome is essential for immune system development as a result of exposure to gut bacteria, nutrient breakdown and absorption, and epithelial mucosal barrier function. Both acute and chronic alterations in the microbiome exert deleterious influences on the gut in a local fashion, but also the host in a remote fashion. Microbiome imbalance (dysbiosis) has is associated with a number of diseases including inflammatory bowel disease, diabetes mellitus, obesity, and colon cancer. 11 In patients with colorectal cancer, a generalized dysbiosis pattern has been discovered. This pattern includes a decrease in butyrate-producing bacteria and an increase in bacteria associated with strong local inflammatory responses (Firmicutes, Bacteroidetes, Fusobacteria, Enterobacteriacea), potentially contributing to tumorigenesis. 11
The adult human gastrointestinal tract is colonized by approximately 100 trillion microbes, with the largest population residing in the colon. 12 For scale, the genomic content of the microbiome is estimated to be more than 100 times that of the human genome with the ratio of human to bacterial cell approximately 1:1. 12 Advancements and cost decreases in high throughput sequencing over the last two decades have greatly improved our knowledge of the microbiome. The Human Microbiome Project was a 10-year, two-phase program that began by first characterizing a reference set of more than 3,000 microbial genome sequences, completed using a combination of 16S rRNA marker gene (present across all bacteria) and metagenome shotgun sequencing. The second phase, Integrative Human Microbiome Project, greatly expanded our knowledge of host–microbiome interactions by analyzing a number of dynamic characteristics (i.e., epigenetics, cytokine profiles, antibody profiles, proteomics) in longitudinal cohorts of known microbiome-associated conditions including pre-term birth, inflammatory bowel disease, and pre-diabetes mellitus. 13
A key clinical condition for understanding the interplay between disease state, microbiome, and other organs is sepsis. The microbiome of a patient with sepsis is subject to many stressors including antibiotic agents, nutrition support, immune system activation, and organ injury or failure. A common cause for acute iatrogenic microbiome imbalance is empiric or therapeutic antibiotic therapy. Even a short course of antibiotic agents may exert a long-term effect. Lofmark et al. 14 evaluated microbiome effects for two years after a seven-day course of clindamycin and found a substantial decline in native species diversity in general, and Bacteroides species in particular. Patients with sepsis often require nutritional support in the form of parenteral or enteral nutrition. Total parenteral nutrition decreases overall microbiome diversity and predisposes to expansion of pathologic, proinflammatory bacteria species.15,16 Even patients receiving enteral nutrition demonstrate changes in their gut microbiome that are dependent on the specific formula concentrations of short chain fatty acids, fiber fat and secondary bile acids. 17 Thus, enteral alimentation may exert different formula-specific influences while providing goal nutritional support; such influences remain unmonitored and largely unanticipated in clinical practice. Routine post-operative changes of gut flora occur and are characterized by decreases in healthy Lactobacilli and Bifidobacteria species and increases in maladaptive Pseudomonas, Staphylococcus, and Enterococcus. 18 The dysbiosis induced by these stressors in patients with sepsis are associated with higher rates of bacteremia, organ failure, and mortality, offering a potential avenue for microbiome-targeted therapeutic intervention. 19
Anastomotic Healing and the Impact of the Microbiome
The modern notion of a bowel anastomosis originated in the late nineteenth century. A combination of aseptic protocols introduced by Lister 20 in the 1860s launched a germ-theory informed period of surgical care. Recognition of the importance of serosal apposition and submucosal collagen formation for successful anastomotic healing by both Lembert 21 and Halsted 22 transformed a previously life-threatening procedure into a relatively safe and common one. 23 Similar to cutaneous wound repair, anastomotic healing occurs in three main phases: inflammatory, proliferative, and remodeling (Fig. 1). The critical biologic step in the pathophysiology of wound healing is the synthesis and remodeling of collagen. 24 Collagen undergoes post-translational modification with hydroxylation of proline residues that permits it to crosslink and provide anastomotic strength. Early investigations of the bursting pressure of ileocolic anastomoses demonstrated that anastomoses reach approximately 60% of their maximum tensile strength at three to four days, and approximately 100% at seven days, a strength approximately 50% of native colon bursting strength. 25 Factors impeding collagen synthesis and augmenting lysis degrade healing substantially. Anastomoses are particularly sensitive to ischemia as adequate oxygen delivery is a prerequisite for proline hydroxylation. 27 Normally, collagenase and other proteolytic enzymes are inhibited to facilitate collagen formation and enable wound repair. 28 Increased collagenase activity is associated with an enhanced risk of anastomotic failure. Unrelieved intra-abdominal infection (failure of source control, iatrogenic injury, technical error) may derail anastomotic healing because of decreased collagen synthesis and increased lysis in response to certain bacteria.
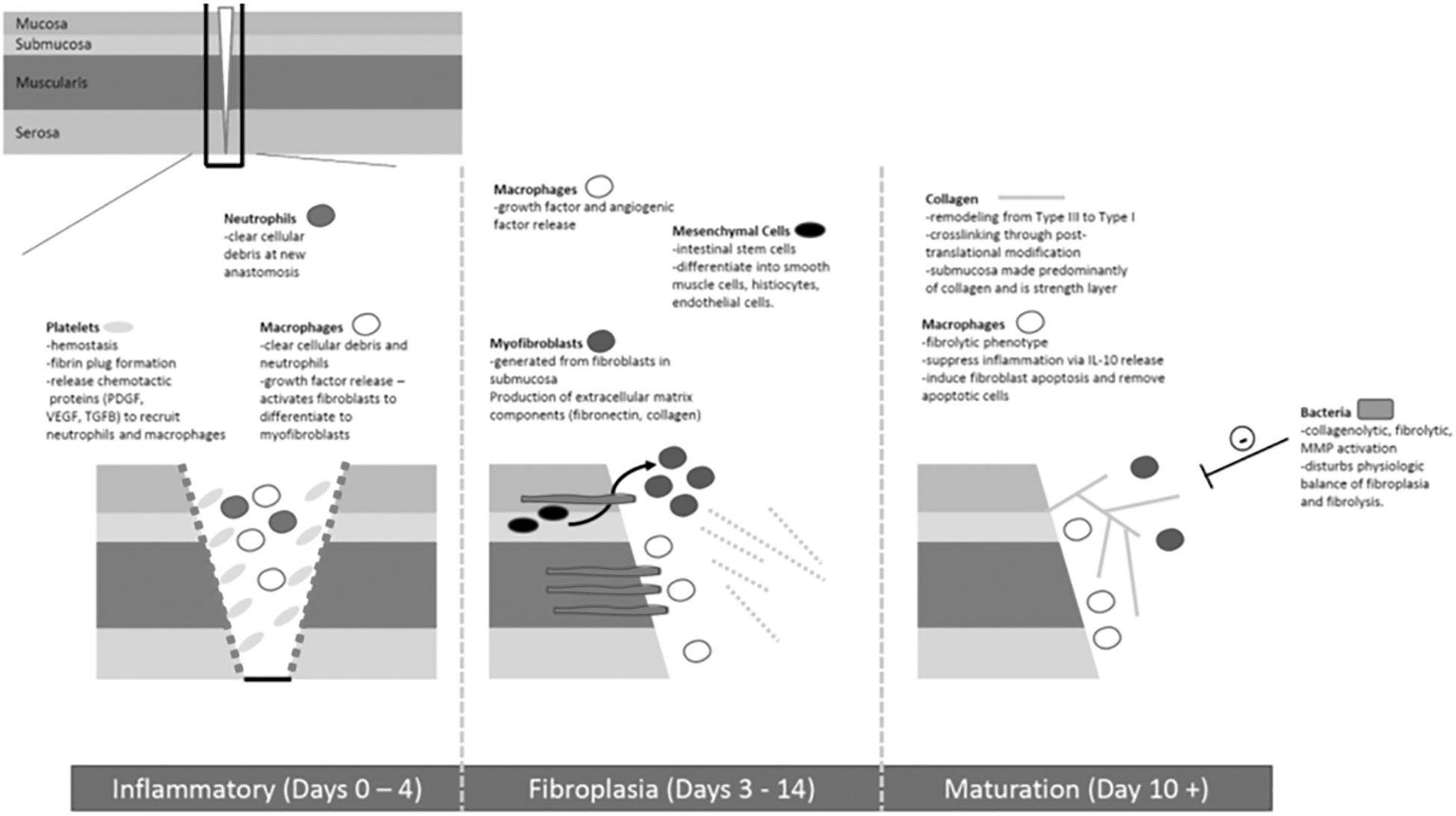
This figure depicts three distinct phases of anastomotic wound healing and the key elements that occur during those time frames.
The notion that microbes influence anastomotic healing is not novel as it dates to the 1950s. Using an in vivo canine model of colon anastomosis, Cohn and Rives 29 demonstrated that intra-luminal antibiotic administration protected anastomoses despite partial ischemia induced by mesenteric vessel ligation, a finding that has been replicated by others.30,31 Pseudomonas aeruginosa was one of the first microbes to be investigated as a driver of anastomotic leak. Shardey et al. 32 found that oral Pseudomonas aeruginosa inoculation led to 95% increased risk of post-gastrectomy anastomotic failure in rats. The virulence of Pseudomonas aeruginosa has been further characterized to include virulence factors such as PA-I lectin/adhesin, which facilitates bacterial adhesion to the gut mucosa and degrades the epithelial barrier to exotoxin A. 33 Surgical and catabolic stress may each trigger the elaboration of such virulence factors and appear to underpin the notion of gut-derived sepsis. An in vivo assessment of Pseudomonas aeruginosa discovered that such bacteria at the site of an anastomosis may undergo a genetic mutation, a single nucleotide polymorphism, in the mexT gene. 34 This mutation alters the Pseudomonas aeruginosa phenotype to one that is capable of inducing epithelial disruption as a result of increased collagenase activity. 34 Therefore, induced pathogenesis of certain bacteria may plausibly threaten anastomotic integrity during the early phase of healing.
Unsurprisingly, sites of anastomotic leak are readily characterized by altered flora. A study compared rat colon anastomotic tissue on post-operative day six to control tissue obtained on post-operative day zero to evaluate tissue microbes. This comparison identified that anastomosis leads to changes in the composition of tissue-based microbes, including a 500-fold increase in Enterococcus, without altering the composition of endoluminal flora. 35 Enterococcus is another microbe implicated in the pathogenesis of anastomotic leak through multiple mechanisms. In vivo studies note that Enterococcus faecalis elaborates collagenase, degrades type-I collagen, and activates matrix metalloproteinase 9 (MMP9) which then degrades type-IV collagen. 36 Additionally, Enterococcus faecalis binds to and activates human fibrinolytic protease plasminogen (PLG) inducing supraphysiologic collagen degradation. 37 Such observations do not exist in isolation as a variety of microbes have been implicated in the pathogenesis of anastomotic leak principally on the basis of native or acquired collagen degradation capability (Table 1). Clearly, the ability to avoid inducing a phenotype that enable collagen degradation would support anastomotic healing.
Microbes Implicated in Pathophysiology of Anastomotic Leak
SNP = single nucleotide polymorphism.
A Paradigm Shift to a Pathobiome is Associated with Anastomotic Leak and Surgical Site Infection
The post-operative gastrointestinal microbiome undergoes dysbiosis and demonstrates augmented inflammation as a result. 38 Enriched Enterobacteriaceae, Enterococcus, Staphylococcus, and Pseudomonas was noted when comparing pre- and post-operative stool samples from patients undergoing surgery for colorectal malignancy; many of these species are implicated in untoward outcomes. 39 Decreases in bacteria species including healthy commensals such as Lactobacilli and Bifidobacteria sp. have been noted in dysbiotic colonic microbiomes and reflect decreased beneficial bacteria and reduced diversity as well. 18 A number of potentially modifiable aspects of care may induce dysbiosis including pre-operative intestinal preparation, administration of peri-operative antibiotic agents, and pre-operative dietary composition. Less modifiable elements include the proinflammatory consequences of tissue manipulation, the pre-operative chronic organ failure, and autophagy failure, each of which may impact outcome. 40
In the dysbiomic post-operative gastrointestinal tract, Enterococcus faecalis and Pseudomonas aeruginosa routinely emerge as dominant species when diversity is reduced. There appears to be a genomic shift in these bacteria post-operatively whereby they adopt a pathologic phenotype associated with increased collagenase activity. 34 Worse, Enterococcus faecalis isolates cultured from post-operative colorectal surgery patients evidenced higher collagenolytic activity than pre-operative isolates indicating virulence induction. The putative mechanism is upregulation of phage-related and hydrolytic enzyme encoding genes in post-operative isolates; virulence is clearly inducible. 41 A preliminary survey performed on 64 bacterial strains isolated from human anastomotic tissues demonstrated that only Enterococcus faecalis and Pseudomonas aeruginosa express this specific phenotype. 36 Relatedly, Bacillus subtilis as well as Serratia marcescens also express collagenolytic activity that may contribute to anastomotic leak. These data identify that maladaptive pressures trigger a progression from a balanced microbiome to a dysbiome and ultimately, a pathobiome. Specific bacteria seem more responsible for pathobiome-induced anastomotic failure and therefore offer potential targets for either trigger remediation, microbiome re-balancing, or virulence factor denial strategies.
Microbiome-Based Strategies to Improve Surgical Outcomes
Strategies to eliminate triggers that induce pathobiome transformation may be promising therapies to deploy around surgical interventions that require anastomoses. Because luminal phosphate depletion serves as a stress trigger for bacteria—and a trigger for the elaboration of virulence factors to support bacterial survival—one potential therapy is the administration of oral phosphate. In vitro and in vivo studies document that oral phosphate supplementation decreased the collagenase activities of Serratia marcescens and Pseudomonas aeruginosa, decreased microbial colonization of anastomotic tissues, and enabled healing compared with a tap water control. 42
Repurposing other existing therapies such as tranexamic acid (TXA) may be useful in supporting anastomotic integrity as TXA inhibits PLG. Accordingly, TXA administered via rectal enema appeared to prevent Enterococcus faecalis-driven anastomotic in a murine model. 37 Currently, TXA is principally administered as an adjunct for hemorrhage control in patients with post-injury fibrinolysis. Tranexamic acid kinetics demonstrate minimal transrectal absorption, and high doses have been delivered without adverse event. 43 A 2021 in vivo murine pathogen-induced anastomotic leak study specifically evaluated TXA for anastomotic leak prevention. 44 After laparotomy and colorectal anastomosis, suspensions of Enterococcus faecalis and Pseudomonas aeruginosa were administered via enema. Rectal TXA administration decreased plasminogen activity, prevented anastomotic leak, and decreased enrichment of collagenolytic microbes in anastomotic tissues as well as luminal flora. 44 Human trials investigating the role of TXA in prevention of anastomotic leak remain on the horizon.
A topic of renewed interest in peri-operative management of colorectal surgery patients is the use of mechanical and antibiotic intestinal preparation. From the 1950s to the 1980s, mechanical intestinal preparation coupled with non-absorbed oral antibiotic agents served as the standard of care. In the 1990s, peri-operative intravenous antibiotic administration began to supplant oral antibiotic preparation and was driven, at least in part, by increased utilization of minimally invasive techniques and smaller access incisions. A meta-analysis of six randomized controlled trials including 1,159 patients compared mechanical intestinal preparation to no intestinal preparation and found no differences in the rates of anastomotic leak, infection, mortality, or re-operation. 45 Nonetheless, there remains controversy regarding the efficacy—or lack thereof—of pre-operative oral neomycin and metronidazole as some studies note decreased rates of surgical site infection, anastomotic leak, and post-operative sepsis. 46 This controversy may be fueled by the observation that pathogenic collagen-degrading Enterococcus faecalis remain unimpacted by common peri-operative intravenous antibiotic agents such as cefoxitin, but may be effectively addressed by luminal antibiotic therapy. 36 Because each patient harbors a unique microbiome, it is reasonable to consider that an intestinal preparation regimen should be personalized; prior antibiotic exposure and the presence of resistant organisms could inform antibiotic agent selection. 47 Screening for high-risk collagenolytic and drug-resistant microbes could lead to a tailored pre-operative intestinal preparation regimen that targets specific elements of a given patient's microbiome. Such efforts dovetail with approaches that impede the development of a pathobiome.3,47
Finally, there has been great interest in investigating dietary modulation to prepare patients for surgery. Weight reduction to improve outcomes from a variety of surgical procedures including ventral hernia repair and total knee arthroplasy is well chronicled.48,49 With regard to colorectal surgery, obesity positively correlates with an increased risk of anastomotic leak and is a potentially modifiable risk factor for those with non-malignant conditions. 50 For patients with malignancies for whom surgical management is time sensitive, planned weight reduction is generally not feasible. Instead, dietary composition modification may be a reasonable approach to altering the anastomotic microenvironment. A murine model demonstrated that a Western-type high-fat, low-fiber, and decreased minerals and water diet increases the proportion of colonic collagenolytic microbes compared with a standard chow (high-fiber, low-fat) diet. 51 Murine microbiome changes induced by long-term ingestion of a Western-type diet can be partially mitigated by a short course (four weeks) of a standard chow diet. 52 These data suggest that deliberate dietary modification may beneficially improve the host microbiome and potentially support anastomotic healing. Similar positive results were obtained in mice habituated to a Western-type diet with a shorter (seven days) course of pre-operative dietary rehabilitation with changes in colonic microbiome that may be tracked using fecal analysis and assessed as a potential pre-operative marker of surgical readiness. 53 Although these pre-clinical results are promising, deploying such techniques awaits human trials.
Conclusions
Anastomotic leak is a potentially life-threatening complication after colorectal surgery. Surgical intervention induces maladaptive changes in the adult gastrointestinal tract microbiome that leads dysbiosis that may progress to pathobiosis. Transformation to a pathobiome is marked by decreased diversity and an increased proportion of specific bacteria that elaborate virulence factors including those that increase collagen lysis and threaten anastomotic integrity. Strategies that mitigate against dysbiosis or pathobiosis are developing and may target specific microbes in a precision fashion to personalize the approach to pre-operative preparation to improve anastomotic healing and surgical outcomes.
Footnotes
Authors' Contributions
Conceptualization: Guyton. Data curation: both authors. Formal analysis: both authors. Writing–original draft: both authors. Writing–review and editing: Guyton. Both authors approved the final version.
Funding Information
No funding was received.
Author Disclosure Statement
No competing financial interests exist.