
Abstract
Background:
Surgical site infection remains a significant cause of morbidity and mortality. Traditionally, the causation has been inferred from the organism(s) detected in the post-operative setting. However, the intra-operative surgical site and the bacteria it harbors have been scarcely studied. Compared with culture-dependent methods, the development of genomic technology provides a new sensitive tool that could aid in characterizing the bacteria within the surgical site. The purpose of this literature review is to establish if there is a predictive role of sampling the intra-operative surgical site.
Methods:
A systematic literature review was conducted identifying relevant literature reporting on studies that sampled the intra-operative surgical site of any specialty, using either traditional culture or a culture-independent genomic sequencing-based technique and correlation with infection was attempted. The review identified studies between 1959 and 2021 in MEDLINE, EMBASE and Cochrane.
Results:
The initial search identified 7,835 articles; 36 remained after screening. Thirty-one articles focused on culture-dependent techniques, five on culture-independent. Subgroup meta-analysis demonstrates that a positive intra-operative culture carries a risk of downstream infection with an odds ratio of 8.6, however limited by a high false-positive and inability to correlate the intra-operative culture with the post-operative infection. In contrast, culture-independent studies through genomic sequencing are not predictive but suggest that the surgical incision is a complex microbial community with a shift toward dysbiosis in certain patients.
Conclusion:
The intra-operative surgical site clearly harbors bacteria. Both techniques give rise to separate explanations underpinning the role of bacteria in surgical site infection. It is possible there is a more complex dynamic community within the incision that makes a patient susceptible to infection. Characterizing this microbial community in large scale studies, including patients with infections may enhance our ability to predict and prevent incisional surgical site infections in patients undergoing surgical procedures.
Surgical site infection (SSI) is a complex process with multiple variables. Surgery involves creating an incision and entering a plane that is usually offered protection from invading microbes by the skin. This exposed plane is now vulnerable to contamination from multiple sources including the patient's own skin flora, the environment (staff and equipment), and microbes from deeper layers/organs depending on the type of operation being performed. The current surgical dogma is that the bacteria that invades the surgical incision will be responsible for the eventual downstream infection, yet clinical sampling of the intra-operative surgical site is not standard practice in modern surgery to confirm this. Traditional microbial isolation studies have used culture-based methods to identify bacteria in the pre-operative setting (to risk stratify) and in the post-operative setting when the infection has already developed. As rates of SSIs continue to stagnate in all forms of surgery, it is clear the intra-operative site must be investigated for its diagnostic potential.
Historically, cultures were once taken from the intra-operative setting as a surrogate for contamination, but their use was limited given the inability to cultivate major pathogenic organisms. This may directly be related to the inherent bias present in culture-dependent methods, given that predetermined conditions are not suited for cultivation of all bacteria. Hence results perceived as negative or sterile may be reflective of a technique lacking sensitivity. In the twenty-first century, culture-independent techniques are now challenging culture-based methods given its superior ability to identify microbes. Irrespective of the technique used, the ability to identify the bacterial profile of the intra-operative surgical incision correctly will enhance our understanding of SSIs.
At present, preventative strategies to mitigate the risk of SSIs are empirical without clear microbiologic targets. Identifying the bacteria within the surgical incision during the intra-operative period may allow us to predict those at risk and, therefore, initiate early targeted treatment. The evidence in this field is deficient. The focus of this literature review is to identify and evaluate the literature on intra-operative surgical site sampling and the role it plays in predicting infection.
Methods
Study screening
This literature review was performed adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). The review was registered with PROSPERO (CRD42022314647) prior to commencement.
The following Population, Intervention, Comparison, Outcomes and Study (PICOS) criteria was used to shape study selection:
Patient population: Patients undergoing an elective or emergency surgical procedure of any specialty. Intervention/exposure: The surgical incision was sampled intra-operatively using a culture-dependent technique. Comparator: The surgical incision was sampled intra-operatively using a culture-independent technique with focus on genomic amplification through a genomic sequencing platform. Outcome: SSI. Setting: Hospitalized patients.
All studies, excluding case reports, case series, and conference abstracts, were considered. Animal-based or non-English studies were excluded. Clinical studies reporting on SSI were screened. All surgical specialties were included if an incision of the skin was performed. Studies were selected if the surgical site was sampled intra-operatively, using either a culture-dependent or culture-independent technique and correlation was attempted with subsequent SSI. Any study in which a clinical intervention was tested (for example, randomized control trial investigating the impact of saline or betadine irrigation on the intra-operative microbiology and subsequent SSI) was excluded. An electronic search was performed between March 4, 2022 and March 11, 2022 using EMBASE, MEDLINE and The Cochrane Library. The search list was imported into EndNote 7 and Covidence.
Data extraction
With aid from a standardized form, data were extracted from included articles by the primary author (V.V.) and reviewed by a secondary author (T.M.). Any disagreements were resolved by discussion. The data extracted includes:
Basic information from the study: year of publication, authors.
Details about the type of operation: clean, clean-contaminated, contaminated, dirty, and surgical specialty.
Sampling method: culture-independent or culture-dependent technique.
Outcomes: comparison of intra-operative and post-operative findings including organisms present, matching, negative predictive value (NPV), positive predictive value (PPV), sensitivity (SN), specificity (SP), and odds ratio (OR) (if available).
Assessment of methodological quality
Articles that met full-text eligibility were assessed for quality and bias using Newcastle-Ottawa quality control tool for observational case/cohort-controlled studies. This was performed independently by V.V. and T.M. Any disagreements were resolved by discussion. The scores are displayed in the tabulated results of the studies in Supplementary Tables S1 and S2.
Statistical analysis
A hybrid approach was adopted in the synthesis of the results of this literature review. All studies included were prospective observational investigations. The studies using culture-dependent methods used quantitative methods in such a manner that facilitated a subgroup meta-analysis in this review. Given the likely heterogeneity between these observational studies, a random effects meta-analysis model was used, implementing the DerSimonian-Laird method.
Results
Study selection
The preliminary search identified 7,835 articles; after removal of duplicates 7,379 remained. Eleven additional papers were identified through reference screening. Eighty-one articles met the criteria for full-text screening, of which 36 papers were identified and included in this systematic review (Fig. 1).
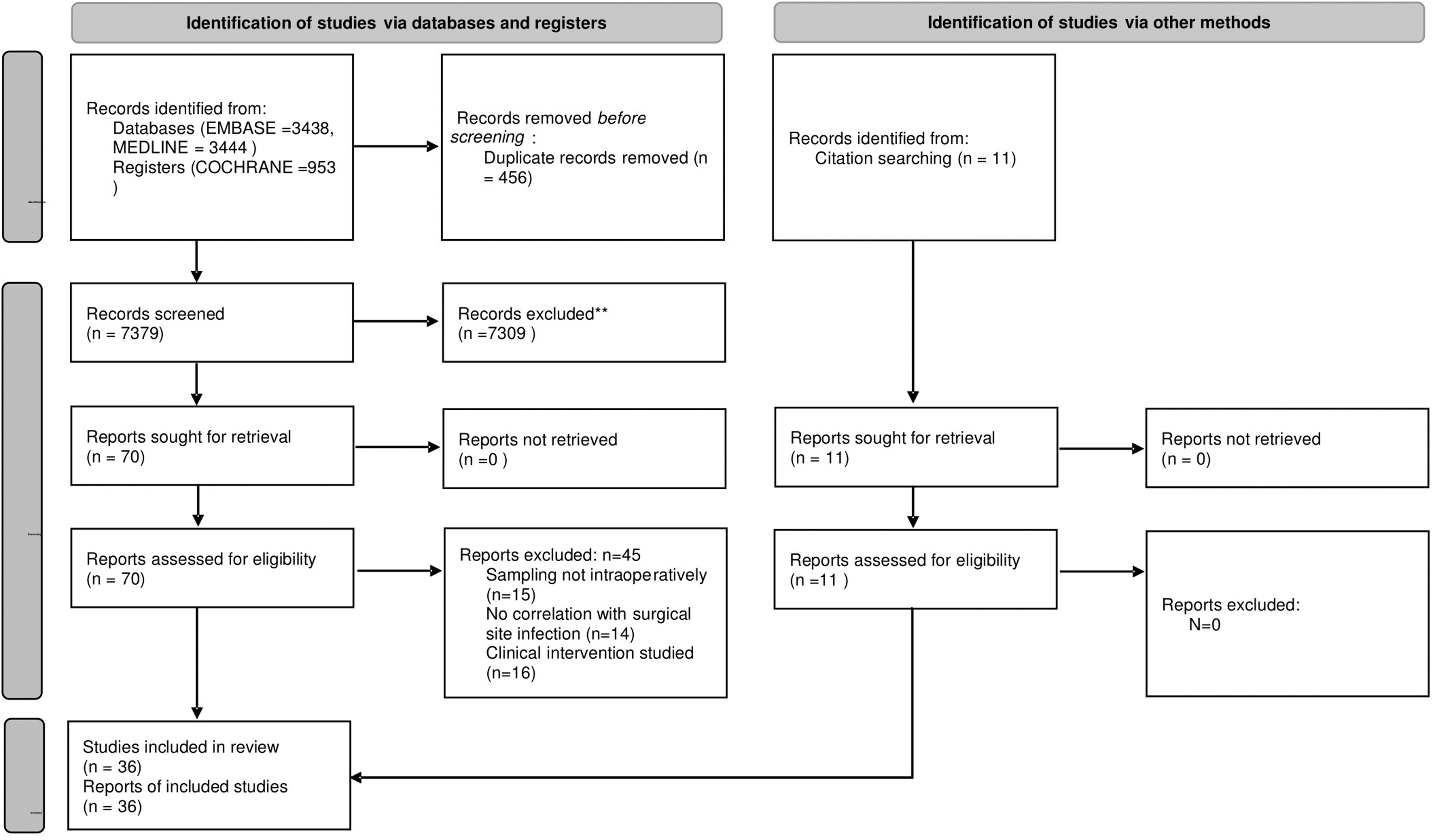
Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) flow chart.
Study characteristics
A total of 36 studies with more than 10,000 participants were included in the review. All studies were of prospective observational study design and conducted between 1959 and 2021. Of the 36 studies, 31 studies focused on culture-dependent techniques; five studies focused on culture-independent techniques for sampling. The results have been summarized in Supplementary Tables S1 and S2.
Risk of bias
Most of the investigations included in this review were of high quality with a score above seven using the Newcastle-Ottawa quality control tool. Several studies scored high on the risk of bias assessment with a score of four or below. These studies were older and scored poorly in the domains of outcome (poor follow-up) and comparability (details in Supplementary Tables S1 and S2).
Intra-operative sampling using culture-dependent methods (n = 31)
The studies involved patients in general surgery (colorectal, upper gastrointestinal, hepatobiliary), head and neck, obstetrics, orthopedics, neurosurgery, and urology. Overall, culture techniques were heterogenous, however, the primary end point of using intra-operative cultures was similar. Most studies sampled the surgical incision at the end of the case, after fascial closure prior to closure of the skin. The location of incision varied from abdominal, head, neck, and limbs, depending on the specialty. The definition of an SSI was homogenous in all the articles; no significant variation was noted. The overarching premise in these investigations was that the intra-operative bacteria was responsible for the downstream infection, hence, culture-based methods were used to identify, diagnose, and stratify the risk of subsequent incisional SSIs in these patients. The results, however, were conveyed in three ways, which has shaped the flow of this review.
First, most of the observational studies qualitatively described the organisms cultured intra-operatively and the relevance of the pathogens identified, essentially characterizing the intra-operative microbiology. Second, some studies used a quantitative approach, attempting to use the result of a positive or negative intra-operative culture to arbitrarily diagnose a downstream SSI (practically speaking, using culture as a surrogate for contamination). These studies clearly documented the rates of positive/negative culture and SSIs. The majority also provided the diagnostic statistics with SN, SP, PPV, NPV, and OR. In this subgroup, the studies that did not calculate the diagnostic statistics, this information was extrapolated and calculated for the purposes of this review. Overall, this enabled us to perform a subgroup meta-analysis in which the diagnostic utility of an intra-operative culture could be assessed. Last, another quantitative approach was used as a subset of studies further attempted to correlate the results from the intra-operative culture with the culture of the post-operative SSI.
Intra-operative microbiology
To elicit the differences in the microbiology, the studies were categorized into clean and clean-contaminated. The definition of this was consistent throughout the studies with clean involving procedures that are uninfected with no exposure from respiratory, alimentary, or genitourinary tract, whereas the latter involved elective breach of these tracts. Clean operations, as expected, cultured skin flora intra-operatively, such as Staphylococcus epidermidis, Corynebacterium, and Propionibacterium acnes. Rarely, organisms such as gram-negative anaerobes were cultured intra-operatively. To highlight the relevance of the intra-operative culture further, a minority of studies provided the result of the post-operative infection culture and intra-operative culture in individual patients. In these patients, the intra-operative cultures were predominantly monomicrobial and represented common skin commensals such as Staphylococcus epidermidis. However, the organisms in the infections were often polymicrobial and included known pathogenic organisms such as Staphylococcus aureus, Escherichia coli, and Pseudomonas aeruginosa.
In this review, clean-contaminated procedures had a higher rate of SSI. This is reflected through the intra-operative microbiology, which is completely different from clean operations. Although common skin organisms were cultured, pathogenic organisms classically associated with the gastrointestinal, urologic, and reproductive tract were more common. In comparison with the clean group, the rate of matching intra-operative and post-operative infection cultures is higher. There was also a trend toward polymicrobial growth (intra-operatively) and presence of common pathogens such as Escherichai coli, Klebsiella pneumoniae, Pseudomonas aeruginosa being more accurately identified intra-operatively as the SSI pathogens in the post-operative culture.
Risk of an SSI with a positive intra-operative culture (n = 21)
Twenty-one observational cohort-controlled trials were identified in this subgroup. These studies clearly documented the number of patients, rates of positive and negative culture, and surgical site infection (results summarized in Table 1). Fourteen studies demonstrated a positive association with an OR of 1, 13 of which had statistical significance. On an individual study level, the results suggest that a positive intra-operative culture can be used as a risk factor but not as a diagnostic test, because of the high false-positive rate. To test the overall diagnostic potential, a receiver operating characteristic curve (ROC) was produced based on the individual study sensitivity/specificity levels (Fig. 2). The area under the curve is 0.86, which favors a positive culture in diagnosing an SSI. A pooled diagnostic odds ratio was calculated using DerSimonian-Laird random effects weighted model for observational studies. Overall, a positive intra-operative culture and SSI has an odds ratio of 8.6, however, with a moderate heterogeneity score, suggesting large variation between studies (Fig. 3).
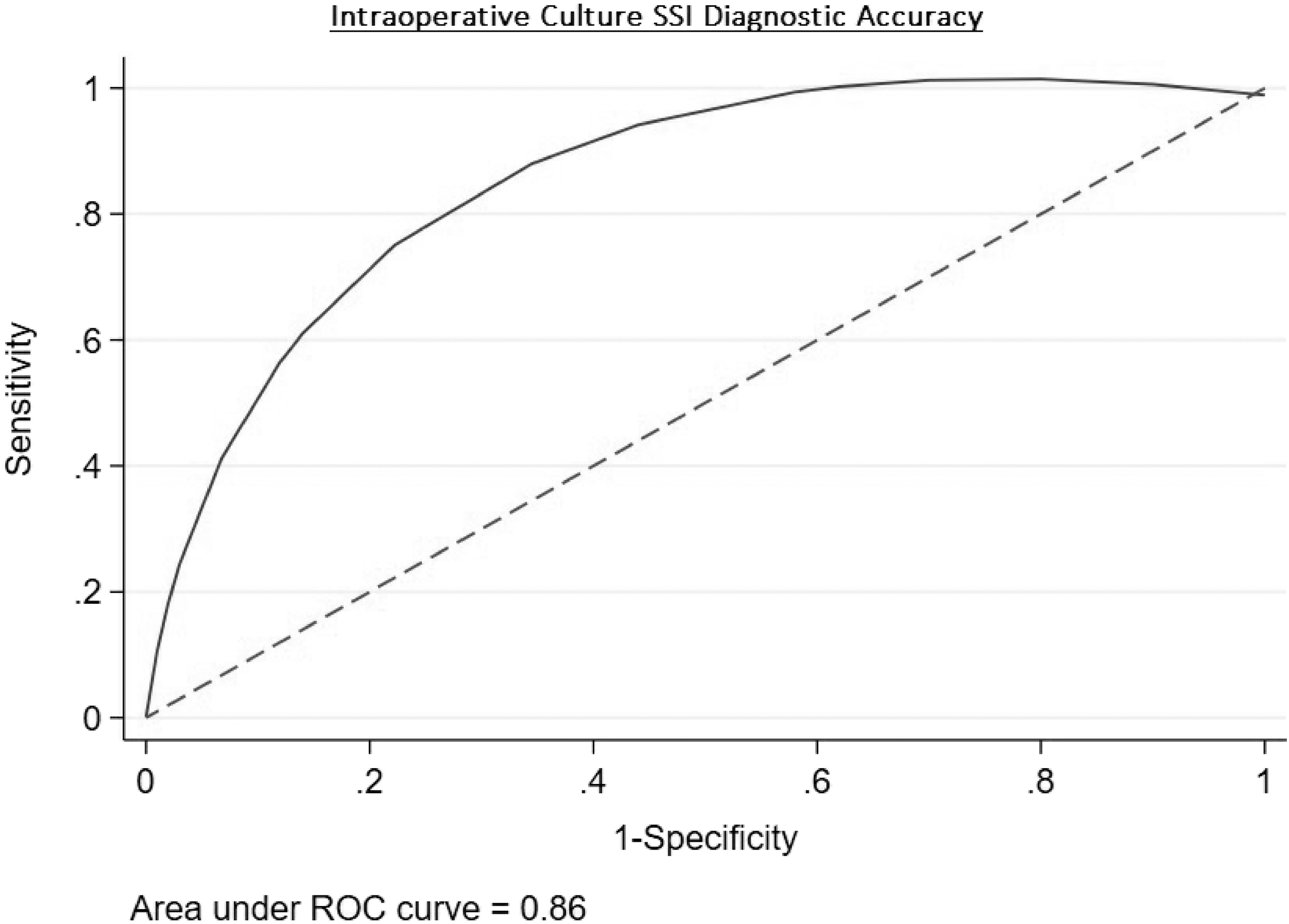
Receiver operating characteristic curve (ROC) demonstrating potential of intra-operative culture. SSI = surgical site infection.
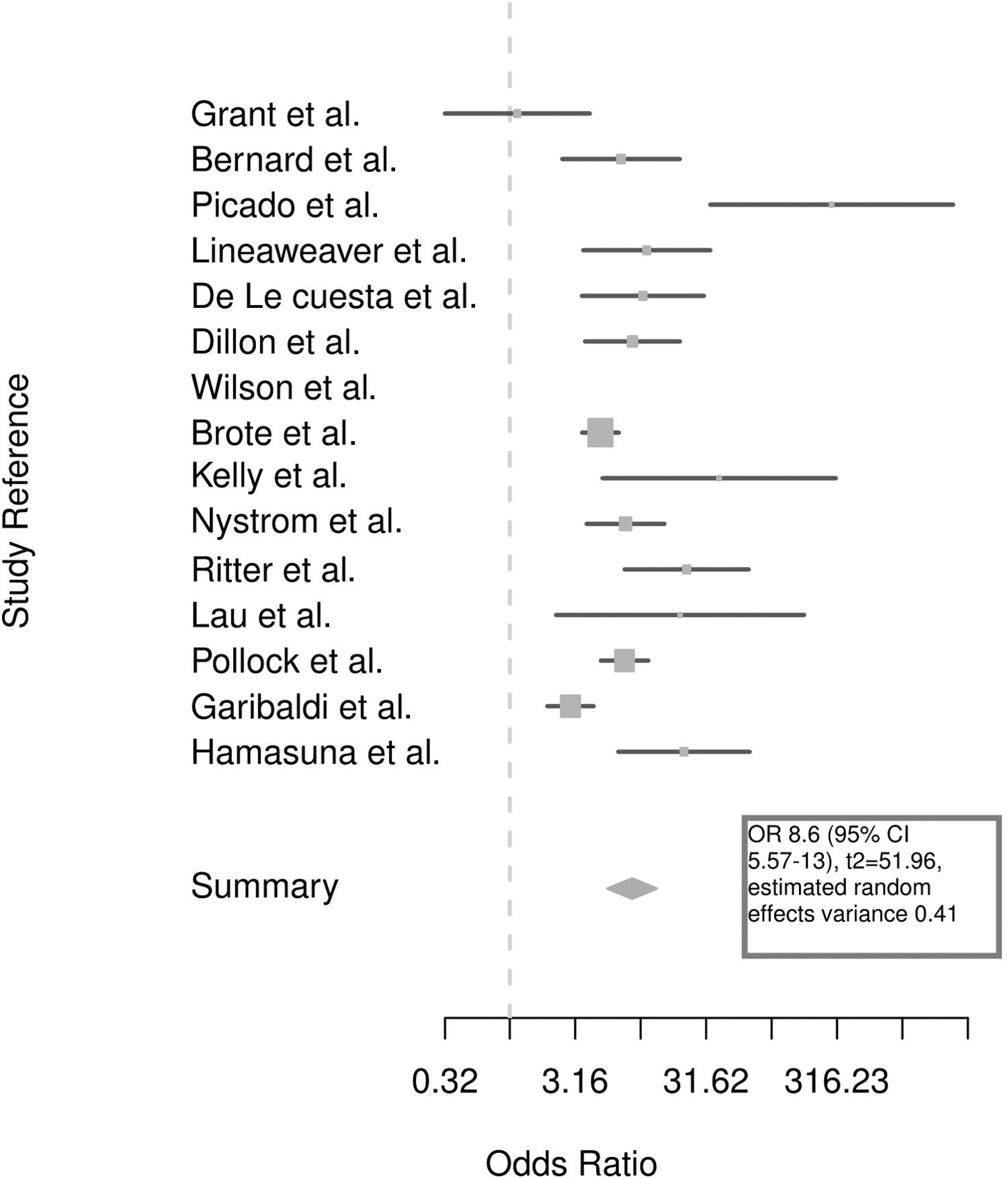
Pooled observational studies (n = 21) Forrest plot of risk of surgical site infection (SSI) with a positive intra-operative culture using DerSimonian-Laird estimator. OR = odds ratio; CI = confidence interval.
Summarized Results from Twenty-One Studies Allowing for Quantitative Analysis
B = both; C = clean; CC = clean-contaminated. + = positive intra-operative culture; − = negative intra-operative culture; OR = odds ratio; CI = confidence interval; N/A = not applicable.
Correlation of intra-operative and post-operative cultures
Twenty studies attempted to correlate intra-operative cultures with post-operative SSI cultures. These studies reported the percentage of matching intra- and post-operative cultures in individual patients. On an individual study level, nine demonstrated a negative correlation (<50%); the remainder were positive. As a collective, in 64% of cases the correct pathogen was identified intra-operatively. However, in a subgroup analysis, clean-contaminated studies (n = 14 correctly identified the offending pathogen intra-operatively 71% of the time. In comparison, clean operations (n = 6), matched only in 44% of cases (Tables 2 and 3).
Studies That Commented on Correlation Rates Between Intra-Operative and Post-Operative Culture
C = clean; CC = clean-contaminated/contaminated/dirty; SSI = surgical site infection.
Pooled Correlation Rates Between Intra-Operative and Post-Operative Culture in Clean and Clean-Contaminated Surgery With Weighted Average Calculated
SSI = surgical site infection.
Intra-operative sampling using culture-independent techniques with genomic sequencing (n = 5)
Five studies met the inclusion criteria in the fields of colorectal, orthopedic, vascular, obstetric, and cardiothoracic surgery. The results of all the studies have been summarized and presented within the Supplementary Tables S1 and S2. The common themes for analysis in this review include the inability to predict SSIs, the dynamic changes in the surgical incision, and the microbial diversity within the surgical incision across different forms of surgery.
Natoli et al. 1 prospectively investigated 111 patients undergoing orthopedic intervention for closed fractures, non-unions, and removal of metalwork (for non-infectious reasons). Specimens were taken intra-operatively from all patients for standard qualitative, aerobic, and anaerobic culture. This was compared with DNA extraction for 16S rRNA amplification via next-generation sequencing (NGS). The authors have not disclosed the specific techniques and primer selection but have stated they performed quantitative polymerase chain reaction (PCR) and NGS. Nine of 111 patients had a positive culture, compared to 27 of 111 in the NGS group. Both culture and NGS identified common skin commensals, such as Staphylococcus epidermidis and Corynebacterium intra-operatively. Culture mostly identified a single pathogen whereas NGS identified multiple. With respect to predictive capabilities, in the culture positive group, two patients developed an infection; the organisms post-operatively did not correlate. In the NGS group, one patient developed an infection; the organism post-operatively did not correlate. The key finding from this article was that neither culture or NGS was predictive of infection, however NGS was more sensitive in microbial isolation.
Vierhout et al. 2 and Holder-Murray et al. 3 also attempted to correlate culture-independent techniques with subsequent infection. Vierhout et al. 2 investigated 10 patients undergoing endovascular aneurysmal repair via groin cutdowns. They sampled the intended groin incision after disinfection with biopsies and subsequently submitted the samples for NGS. This was a pilot study part of a larger trial, from which they selected two patients who had developed an SSI and matched them with eight controls. Next-generation sequencing in all patients demonstrated the presence of skin commensals. Pathogens, such as Staphylococcus aureus and gram-negative anaerobes, were not detected in those with infections or without. No difference was noted in the microbiome in either group. In one patient who developed an infection, a higher relative abundance of Staphylococcus haemolyticus was detected, but the causative organisms for the post-operative infection was polymicrobial with Escherichia coli, Enterococus faecalis, and Staphylococcus aureus. These organisms were not identified intra-operatively by NGS.
Holder-Murray et al. 3 investigated 60 patients undergoing elective bowel resections. Only one patient in this cohort developed an infection. With respect to predictive capabilities, the causative organism for this infection was Enterococcus faecalis, which was confirmed on culture in the post-operative infection. This study involved dynamic sampling (discussed below) and, in this patient, Enterococcus faecalis was not detected pre-operatively, intra-operatively or on days one and two immediately post-operatively. However, on day four, this organism was seen in the ileostomy effluent from the patient and in low relative abundance on samples taken from the superficial skin of the day four incision. Hence, the offending pathogen was detected using NGS prior to an infection developing, however, in the post-operative period, not intra-operatively.
Dynamic changes within the surgical site
Holder-Murray et al., 3 Rood et al., 4 and Romano et al. 5 attempted to establish the changes that occur in the surgical incision from the pre-operative to post-operative period. The common hypothesis was an aberrant microbiome is present in the immediate peri-, intra-, or post-operative period, which may contribute to the development of an infection. Holder-Murray et al. 3 investigated patients undergoing elective colorectal resections for malignant and benign pathology. The abdominal skin (overlying intended laparotomy wound or bowel extraction site in laparoscopic procedures) was sampled in the pre-operative clinic, prior to antiseptic disinfection, after disinfection, daily post-operatively, and finally in the post-operative clinic visit. The subcutaneous wound was sampled on peritoneal opening and peritoneal closure. The patient's intestinal tract was also sampled with rectal and luminal swabs. The subcutaneous wound on opening showed minimal microbial presence, however, the closing sample demonstrated an increased relative abundance of Bacteroidacaea, Lachnosparchiea, and Enterobacteriaceae, bacteria which were seen in the lumen of the bowel of the same patients, suggesting endogenous contamination.
The impact of this endogenous contamination on the incision is clear through sampling of the abdominal skin. The pre-operative and post-operative clinic samples were comparable, however, in the immediate days after the operation, the alpha (microbial richness) diversity was significantly lower. Additionally, common skin commensals at a genus level, such as Corynebacterium and Propniobacterium, were depleted and replaced by Enterobacteriaceae and other gram-negative anaerobes, suggesting a dysbiosis. The overall impact this has on infection is unclear given that only one patient developed an SSI in this study.
Rood et al. 4 characterized the microbiome in women undergoing caesarean section. In their cohort, obese women had a higher percentage of clinical SSIs. The authors dynamically sampled the patients, at multiple locations (and timepoints) however the most relevant for this review was the surgical incision (Pfannenstiel) before skin preparation and after skin closure, representing the native skin microbiome and the disruption caused by surgery. Overall, non-obese women at a phylum level demonstrated stability with consistent presence of Actinobacteria and Firmicutes and limited Proteobacteria and Bacteroides between the pre- and post-operative period. In comparison, obese women demonstrated instability with a reduction in Actinobacteria and increase in Firmicutes, Protobacteria, and Bacteroidetes at the end of the case. The authors further characterized by describing the relative abundance of the phylotypes present. In obese women, the start of the case was characterized by Corynebacterium, Staphylococci, and Clostridiales with a stark change at the end. Corynebacterium was reduced substantially, Staphylococci was relatively stable, and there were large increase in Clostridiales. Additionally, Bacteroidetes and Proteobacteria both appeared (not seen in non-obese women). The authors quantified this aberrance with a dysbiosis ratio, comparing Proteobacteria and Bacteroides over skin commensals Propionibacterium and Staphylococcus. Only in obese women was this ratio increased.
Romano et al. 5 characterized the dynamic microbiome in patients undergoing coronary artery bypass grafts. The authors intended to correlate differences in patients with an infection, but no patients developed an SSI in their small cohort, however, the temporal changes in the microbial community were unique. The sternotomy site was sampled extensively from the skin, subcutaneous wound, mediastinum, and scar. The skin, subcutaneous wound, and mediastinum were sampled from the opening and closure of each site respectively. The authors characterized the bacteria at a genus and phylum level. At a genus level on the skin pre-operatively, Propionibacterium, Corynebacterium, and Staphylococcus dominated. The skin at the end of the case showed an increase in Propionibacterium and decrease in Corynebacterium. At the level of phylum there is a steady increase in Proteobacteria with the highest levels at the end of the case. Bacteroidetes also increased throughout the wound with highest relative abundance in the mediastinum samples.
Discussion
To predict an outcome, we must understand the primary problem. Surgical site infection is a multifactorial process. There is a range of clinical factors that makes a person susceptible to infection, including age, gender, immunosuppression, procedure, location, and contamination. It is the combination of these features that either protects or predisposes a patient to infection. Contamination refers to microbial presence in an environment foreign to its own such as the surgical site, which is a neo-environment created by the surgeon. It is unfamiliar to the body and all its constituents. It is clear from this literature review, when the surgical site harbors bacteria, there is a predisposition to infection. However, the role of the organism(s) intra-operatively is not clear. The collective information from culture based and independent studies raises two possibilities.
First, a positive intra-operative culture (irrespective of the organism) is a risk factor for infection. It has a diagnostic odds ratio of 8.6. Furthermore, when mixed anaerobes or certain specific pathogens are detected (e.g., Escherichia coli), there is a higher risk of subsequent infection. We must now address whether the organism(s) at the end of the case is responsible for the subsequent infection. If this is the case, then we would expect the post-operative infection culture to match the intra-operative result. This was not supported by the culture-dependent studies, with only 64% of the cases reporting a culture match. In clean procedures, this was worse at 44%. If we believe that it is the intra-operative bacteria that is ultimately responsible for the post-operative infection, then culture-dependent techniques are promising, but ultimately inadequate due to the inability to culture the offending pathogen. This creates a gap in the literature which may be addressed by a culture-independent technique, which is more sensitive in detecting microbes.
However, an alternative pathologic process is possible if we consider the information from the culture-independent studies. Two key findings were drawn from this review. First, genomic sequencing through amplification of the 16S rRNA gene is far more sensitive than culture in detection of bacteria, and second, there is a dynamic microbial community within the surgical incision, which demonstrates a path towards dysbiosis (displacement of skin commensals with replacement of anaerobic bacteria). This concept of dysbiosis was quantified by Rood et al., 6 who were able to generate a ratio based on skin commensals and anaerobic bacteria. Although this information does not presently allow us to predict infection, it shows a clear aberrance in patients across multiple forms of surgery, including clean and clean-contaminated operations.
Considering this, the bacteria within the wound at the end of the case represents a complex microbial community. It is the profile of this community that may determine whether a patient develops an infection or not. If we consider the information from NGS to be true, i.e., the bacteria detected is present, not just noise, then we must think about the dynamics. At the end of an operation, all bacteria within the incision are in a new environment, relatively foreign to its own. The bacteria now must contend with a proinflammatory state, with variable levels of oxygen and carbon dioxide, and must compete with other organisms for survival. In this state, the patient's own clinical variables will also influence bacterial survival. The eventual outcome in the days after the patient's operation will be either the growth of a certain pathogenic bacteria (which may not have been dominant at the end of the operation) resulting in infection, or persistence of skin commensals and host bacteria, resulting in healing. Although this draws on the information from the culture-independent studies, we could argue that the culture-based studies also showed this. A positive culture demonstrated a propensity for infection irrespective of the organism cultured. The lack of correlation between intra- and post-operative cultures may be because of the changing microbial community. The organisms detected by culture intra-operatively are simply a snapshot of the larger bacterial community, which changes throughout the surgical pathway and the resultant pathogen causing the SSI is selected in the days after the sample was taken.
The two theories discussed are fundamentally different. Intra-operatively, if the organism cultured is responsible for the subsequent infection, the solution is straightforward. We must identify the organisms correctly and initiate early treatment; culture has demonstrated this. However, NGS could enhance our ability to detect and predict. On the contrary, a complex microbial community is far more difficult to interpret. Microbial community assembly and, therefore, function are influenced by factors that are deterministic and stochastic. Stochastic factors include chance colonization and random extinction while, in contrast, deterministic factors would include environment factors and interspecies interaction. This concept is not fully understood in biology or in other scientific fields. The interplay between these factors remains a debate. With respect to the surgical site, it would seem logical that the deterministic factors shape the microbial community. 7 The resultant community will either lead to infection or to healing. Therefore, characterizing this community intra-operatively may be of clinical benefit. However, at present, the paucity of data limits this potential. This presents another gap in the literature. Large-scale observational studies characterizing the microbial community of the surgical site in patients with and without infections is required to determine if there is a detectable aberrant community at the end of the case.
The results of this literature review have raised plausible explanations that require further investigation. However, we must accept some limitations. For culture-dependent studies, articles were included from as early as 1959 and practice has since changed. The techniques used in culture vary from study to study which can be misleading, an issue shared by culture-independent studies. Variations existed regarding patient selection, sample collection, and processing. Furthermore, the use of different primers for 16S rRNA makes it difficult to compare results. Although NGS offers an extensive insight into the microbial community, it does not distinguish between living and dead organisms, therefore it is difficult to differentiate between functional bacteria and noise.
In conclusion, sampling of the surgical site using culture-based techniques can identify an at-risk patient, but its clinical application is limited because of its inability to identify the potential pathogen involved. Although culture-independent techniques are not predictive, they have, however, offered a unique insight into a potentially more complex microbial environment within the surgical incision. Irrespective of the technique used, it is clear that intra-operative bacteria play a key role in the development of a subsequent infection. At present, the use of NGS has been limited to small datasets in patients without infection. Implementing large-scale studies that use NGS to allow for comparison of patients with infections may provide critical information about the type and role of the bacteria intra-operatively. This has potential to identify high-risk patients correctly and implement clinical change.
Footnotes
Authors' Contributions
V.V. conceived and designed the review, performed the search, performed the analysis, and wrote the paper. T.M. was the second reviewer in the search and quality assessment and assisted in editing of the paper. S.S. assisted in design of the review and supervised the writing of the paper. E.H., P.P., and S.K. supervised the writing of the paper.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author Disclosure Statement
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.