
Abstract
Background:
With the recent increase of minor lumbar spine surgeries being performed in the outpatient setting, there is a need for information on factors that contribute to post-operative complications for these surgeries.
Patients and Methods:
This was a prospective observational study examining risk factors for self-reported post-operative drainage in patients who underwent lumbar spine surgery. Patient surveys and the hospital's electronic medical records were used to collect data on patient demographic, patient lifestyle, and surgical variables. Univariable and multivariable analyses in addition to a random forest classifier were performed.
Results:
A total of 146 patients were enrolled in the study with 111 patients included in the final analysis. The average age and body mass index (BMI) of these patients was 66 and 27.8, respectively. None of the 146 patients in this study developed surgical site infection. Older age, no steroid use, no pet ownership, and spine surgery involving two or more levels were all found to be risk factors for wound drainage.
Conclusions:
This study evaluated lifestyle, environmental, and traditional risk factors for surgical site drainage that have not been explored cohesively related to outpatient orthopedic surgery. Consistent with the existing literature, outpatient spine surgery involving two or more levels was most strongly associated with surgical site drainage after surgery.
In recent years, minor lumbar spine procedures have become increasingly performed in the outpatient setting. This shift toward outpatient surgeries has been seen across multiple surgical specialties. Despite this, there is a paucity of literature that exists on risk factors for adverse events in the outpatient orthopedic setting. 1 Most of the current literature supports ambulatory spine surgery as a safe option with favorable clinical outcomes, however, it is important to consider the implications of selection bias towards younger, healthier patients regarding those findings. 2 Thus, the frequency of post-operative surgical site complications after lumbar spine surgery and what factors contribute to surgical site complications has not been described in the setting of outpatient spine surgery. As a result, the normal post-operative surgical site healing process for outpatient surgery is not well understood.
Surgical site complications can have devastating consequences including prolonged patient discomfort, increased patient mortality, and increased risk for infection or revision.3,4 Understanding factors involved in surgical site complications will allow surgeons to counsel patients more appropriately and develop preventative measures to mitigate risk.
Traditional patient-related risk factors for surgical site complications after spine surgery include obesity, smoking, and diabetes mellitus.3,5–8 Furthermore, intra-operative risk factors have been identified including longer operation time, implant usage, and surgical approach.3,4,9 Additionally, seasonal variation in overall infection rates, specifically higher infection during the summer months, has been observed and described for laminectomy. 10 Surgical site infections (SSIs) are known to be one of the most common post-operative complications after spinal surgery.5,8,11 Our hospital's SSI rates for laminectomy and fusion, although relatively low at 0.76% (compared to reported ranges of 0.5–2.0%), are higher for outpatient spine procedures than they are for similar inpatient spine procedures, despite the outpatient population being generally healthier and having lower risk.12–15
In this study, we used patient surveys to capture the status of a patient's surgical site complication, how they cared for the complication, and information on other daily routines that may affect surgical site healing. These data allow us to identify factors associated with surgical site complications in outpatient lumbar spine procedures, including differences in complications related to patient environment. We hypothesized that factors in the patient's environment may impact the likelihood of surgical site complications in the outpatient lumbar spine surgery population.
Patients and Methods
Study population and data collection
After Institutional Review Board (IRB) approval was obtained, patients undergoing planned outpatient spine surgery from August 2018 to December 2019 were recruited for this study through mail and e-mail invitations. Participants filled out an initial survey at the time of consent about their diet, housing, pet ownership status, and caretakers. Follow-up surveys were conducted through mail or e-mail to ascertain the outcome of interest, self-reported drainage from the surgical site, as well as additional medical care, and participant environment at post-operative weeks one and two.
Demographic and surgical data were collected for these participants using the hospital's electronic medical records. Surgical site infection was measured by the hospital's infection control department, according to definitions set by National Healthcare Safety Network/U.S. Centers for Diseases Control and Prevention (NHSN/CDC). 16
Univariable and multivariable analysis
Univariable analyses were conducted in SAS 9.4 (SAS Institute Inc, Cary, NC) for all variables to determine association with the primary outcome of self-reported drainage from the surgical site. Logistic regression was performed for continuous variables and χ 2 tests were performed as appropriate for categorical variables. A multivariable analysis was also performed to adjust for statistically significant variables. Significance was determined at the p < 0.05 level.
Random forest
A random forest classifier was created in R-Studio using tidyverse, caret, and randomForest packages with self-reported drainage at post-operative week one as the outcome. 17 Features were excluded if they had little variability, duplicated the same information as another feature, or more than 20% of the observations were missing. Where possible, features with low variability were included by re-coding. For example, survey responses for type of housing were listed as house, apartment, condo, or other. For analysis, these were re-coded as house and apartment/condo to explore a difference between less and more densely populated living conditions. This left 35 variables for inclusion in the random forest classifier.
Continuous features were re-coded as binary categorical variables such that the random forest algorithm would not prioritize continuous over categorical variables. All variables were one-hot encoded to ensure that features with more levels were not prioritized over features with less. The dataset contained four missing values across three features, all of which were categorical. The value of each feature with the highest frequency was imputed to the missing data.
The data were split into 70% training and 30% test sets to ensure a large enough test set for the small sample size (n = 111). Training and test sets were compared to ensure similar makeup. Baseline probability of choosing the correct outcome at random was calculated by randomly sampling from a vector containing the values of our outcome (0 = no drainage, 1 = drainage) for the number of observations in the test set with replacement. The performance of the final model was evaluated by its sensitivity, specificity, negative predictive value (NPV), positive predictive value (PPV), receiver operating characteristic (ROC) curve, and area under the curve (AUC).
Results
A total of 146 patients were enrolled in the study, comprising 23.4% of the total outpatient surgical population in this timeframe. After surveys were distributed and completed; 111 of these patients had at least one survey that could be included in the final analysis. The average age and body mass index (BMI) of these patients was 66 and 27.8, respectively. Most of these patients had an American Society of Anesthesiologists (ASA) score of one or two (87/111; 78.3%) and 93.6% of the patients reported not being an active smoker. None of the 146 patients in this study developed an SSI.
Univariable analysis
The univariable analysis showed age (p = 0.045), number of spinal levels (p ≤ 0.001) the number of times the patient's dressing was changed during the first week after surgery (p < 0.001), pet ownership (p = 0.041), steroid use (p = 0.049), and number of days after surgery before shower or bath (p = 0.007) as significantly associated with incision drainage at week one or two (Table 1 and Table 2). The number of times the patient's dressing was changed, although associated with the primary outcome, was excluded from further analysis because patients with drainage are likely changing their dressings more frequently, and the variable is therefore not a risk factor.
Univariable Analysis of Patient and Surgical Factors
BMI = body mass index; ASA = American Society of Anesthesiology; MRSA/MSSA = methicillin-resistant Staphylococcus aureus/methicillin-susceptible Staphylococcus aureus.
Performed as logistic regression.
Univariable Analysis of Patient Survey Questions
Performed as logistic regression.
Methicillin-resistant Staphylococcus aureus/methicillin-susceptible Staphylococcus aureus (MRSA/MSSA) colonization status data were collected as MRSA/MSSA positive, MRSA/MSSA negative, or not tested. Hospital protocols dictate MRSA/MSSA testing for planned inpatient orthopedic procedures, and often correlate with in-person pre-screening visits for higher-risk patients. Additionally, high-risk patients undergoing outpatient procedures also have in-person pre-screening visits and follow protocol for MRSA/MSSA testing. Patients who were not tested are in general healthier patients with planned outpatient procedures, who undergo pre-operative telephone interviews instead of in-person pre-operative screening.
Multivariable analysis
A multivariable analysis was performed on variables with univariate p < 0.05, except as noted above (Table 3). After adjusting for age, steroid use, pet ownership and levels of spine surgery, spine surgery involving two or more levels was the only variable that remained significant and had increased odds of wound drainage (odds ratio [OR], 6.17; 95% confidence interval [CI], 2.23–17.02). Steroid use and no pet ownership continued to show a trend toward less drainage although not statistically significant.
Multivariable Analysis
OR = odds ratio; CI = confidence interval.
Random forest
The probability of correctly guessing the drainage at random was 44%. The final model predicted the outcome with 66% accuracy on the training set and 62% accuracy on the test set and the AUC was 0.63. Accuracy was determined by the percentage of correctly predicted outcomes in each set. The model performed much better at predicting cases without drainage than with drainage (sensitivity = 0.09; specificity = 0.87,;PPV = 0.25; NPV = 0.67). The most important variables used by the algorithm were number of spinal levels and whether or not a patient was ultimately discharged on the day of surgery (Fig. 1).
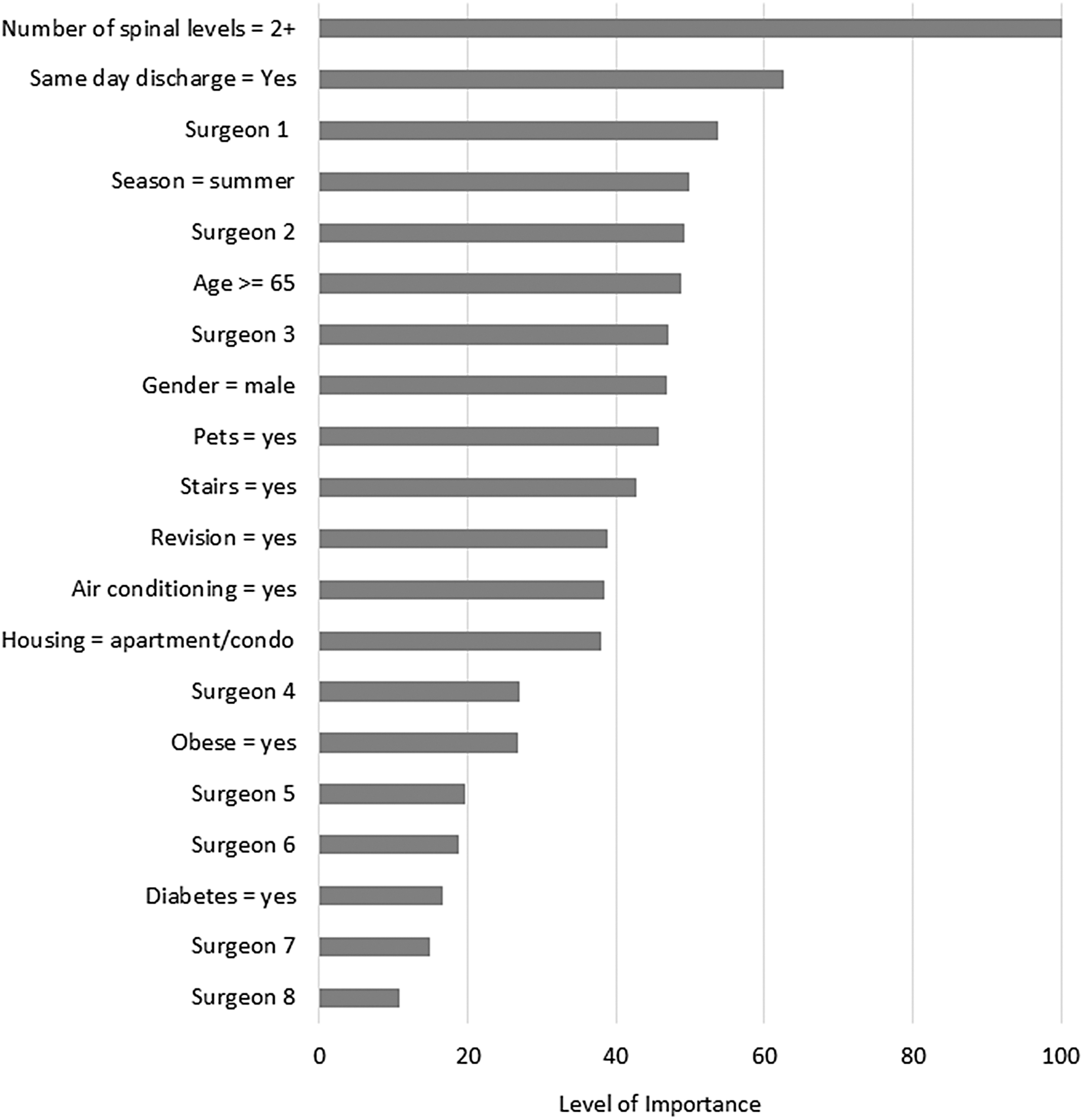
Graph of variable importance for wound drainage using the random forest classifier. Importance noted on a scale of 0–100, with 0 being least important.
Discussion
This study analyzed a cohort of 111 people who underwent an outpatient lumbar spinal surgery and found number of spinal levels was the most predictive factor associated with post-operative wound drainage. We assessed a number of non-traditional lifestyle and environmental variables in this study. Although some of these factors, such as pet ownership, post-operative bathing, and seasonality showed signals of importance, they were ultimately less impactful than traditional risk factors. Both steroid use and pet ownership, although significant in the univariate analysis, did not show any effect on drainage after adjusting for other variables in the multivariable analysis. This was likely the result of multiplicity of testing, and the low impact of these variables compared with other factors that were measured.
A study by Klein et al. 18 looked at pre-operative nutrition in spinal surgery patients and found that it was highly predictive of postoperative complications. Factors including number of days after surgery until taking a shower or bath and number of times the dressing was changed were both statistically significant but may be confounded by the amount of surgical site drainage. Because of this chicken-and-egg effect, we did not include these variables in multivariable analysis. These kinds of patient lifestyle factors may give insight to personal challenges that would increase the likelihood of postoperative complications.
Other known risk factors for SSI including smoking, revision surgery, diabetes mellitus, total procedure time, and BMI were not seen to increase surgical site drainage.6–8 This may be accounted for by the process our hospital's surgeons have in place for patient selection and reduction of certain risk factors prior to surgery. In addition, although surgical site drainage may contribute to SSI risk, it is not necessarily driven by the same risk factors that increase likelihood of SSI. Two or more levels operated on during spine surgery was the most predictive of surgical site drainage, which is likely due to the complicated nature of larger surgeries and increased surgical time. This has been noted in prior studies assessing risk for a variety of outcomes after spine surgery. 19
We observed clear surgeon variability in regards to surgical site drainage as seen in the univariable and random forest classifier. This may be the result of surgeon acceptance/tolerance for drainage or the variation in the surgeon's patient population. Although surgeon 3 was shown to have lower rates of drainage, there were no major differences between surgeons in their preparatory, surgical, or closure processes that stood out. One study by Brook et al. 20 found that 47.2% of the variation in hospital complication rates could be explained by surgeon factors. This provides evidence that the surgeon's individualized technique for a given procedure should be considered when looking at patient outcomes because of the variability seen among each surgeon's approaches during more complex spinal surgeries.
The random forest classifier illustrated greater than two levels of spine surgery, same day discharge, summer weather, older age, and surgeon variability as the top five most important variables that affect wound drainage. This was overall consistent with the univariate analysis. Patients who were not discharged on the same day were likely more complicated cases with additional risk factors not recorded. Despite summer season not being significant in the univariable analysis, it was important in the random forest classifier. This is consistent with prior observation of increased in infections during the summer months.21,22 Drainage is frequently a precursor to infection, and thus the increased infection risk in the summer may also be an increased risk for surgical site drainage.
Both of the models used, namely the multivariable logistic regression and the random forest classifier, showed that the number of levels operated on was clearly the biggest predictor of surgical site drainage. Although the random forest classifier had a 62% accuracy, it allowed us to factor in many more variables and determine the importance of these variables granularly while maintaining power and statistical significance. However, the random forest classifier does not describe directionality of importance (increasing or decreasing wound drainage) and is therefore best interpreted together with traditional univariable analysis. The multivariable analysis on the other hand specifically indicates a positive or negative effect on surgical site drainage but does not allow us to adjust for as many variables, limiting the model's equivalence to real-world situations. Studies have been done to compare the use of a random forest versus a logistic regression and both have been shown to be superior in different cases.23,24 Using both of these complementary models gives a more comprehensive, well-rounded view of the risk factors contributing to wound drainage. Reassuringly, the most important factor in both models was the same.
Limitations
This study is limited in its generalizability because data were collected from a single orthopedic specialty hospital. The study was performed during a period of low infection, which limited ability to use SSI as an outcome.
Conclusions
This study evaluated lifestyle, environmental, and traditional risk factors for surgical site drainage that have not been explored cohesively related to outpatient orthopedic surgery. Consistent with existing literature, outpatient spine surgery involving two or more levels was most strongly associated with surgical site drainage after surgery.
Footnotes
Authors' Contributions
Conceptualization (supporting): Hoffman. Conceptualization (lead): Hollenbeck. Methodology (supporting): Hoffman. Methodology (lead): Hollenbeck. Investigation (lead): Hoffman, Lanza. Formal analysis (lead): Hoffman, Lanza. Formal analysis (supporting): Simon. Writing—original draft (lead): Simon. Writing—review and editing (equal): Schoeller, Fang, Coden, Hollenbeck. Supervision (lead): Hollenbeck.
Funding Information
No funding was received.
Author Disclosure Statement
All authors report no conflicts of interest.