
Abstract
Background:
Topical antibiotic agents are not generally indicated for preventing of surgical site infections (SSIs) in clean incisions, and the drug concentrations that should be delivered to local incision sites remain uncertain. The aim of this study was to critically assess the efficacy of topical antibiotic agents in comparison with non-antibiotic agents for preventing SSIs in clean incisions by performing a systematic review and meta-analysis.
Methods:
We conducted a search of literature in PubMed, Embase, and Cochrane Databases and included randomized controlled trials (RCTs) on topical antibiotic use for patients with clean post-surgical incisions. The primary outcome was the incidence of SSI, presented as the event rate. Eleven RCTs were included.
Results:
Using random-effects modeling, the pooled risk ratio (RR) of developing a post-surgical incisions infection was 0.83 (95% confidence interval [CI], 0.61–1.16; I2, 0%). In subgroup analyses, no reductions in SSI were observed when topical antibiotic agents were used to treat incisions due to spinal (RR, 0.75; 95% CI, 0.40–1.38; I2, 0%), orthopedic (RR, 0.69; 95% CI, 0.37–1.29; I2, 0%), dermatologic (RR, 0.77; 95% CI, 0.39–1.55; I2, 65%), or cardiothoracic surgeries (RR, 1.31; 95% CI, 0.83–2.06; I2: 0%). The incidence of SSI across different operative phases did not differ for the application of topical antibiotic agents compared with non-antibiotic agents (RR, 0.80; 95% CI, 0.56–1.14; I2, 0%).
Conclusions:
The results of this meta-analysis show that topical antibiotic agents provide no clinical benefit for preventing SSI in clean incisions.
More than a decade ago, the World Health Organization issued guidelines for the prevention of surgical site infections (SSIs), which do not recommend the use of antibiotic agents to irrigate surgical incisions prior to closure. However, prophylactic antibiotic agents continue to be subjectively applied by physicians in clinical practice. 1 Guidelines from the U.S. Centers for Disease Control and Prevention (CDC) also advise against the application of ointments, solutions, or powders to surgical incision sites, although no guidelines are provided for the use or avoidance of specific antibiotic agents. 2 Although topical antibiotic agents are not indicated for post-surgical incision infection prophylaxis after clean surgeries, many dermatologists continue to prescribe them. 3 The use of local antibiotic agents at the surgical site has received very limited approval across all surgical prophylaxis consensus guidelines that we are aware of. Nonetheless, the selective use of topical antibiotic agents for surgical prophylaxis has been found to be beneficial after certain procedures, including joint arthroplasty, cataract surgery, and breast augmentation. Outside of these specific indications, conclusive evidence supporting the use of topical antibiotic agents at surgical incision sites derived from randomized controlled trials (RCTs) remains limited. 4
Topical antibiotic therapy affords many potential advantages, but clinically infected wounds typically require systemic antibiotic therapy, whereas clinically uninfected wounds that are healing as expected do not require antimicrobial agents. 5 In addition, topical therapies can result in the development of local hypersensitivity or contact dermatitis reactions that may interfere with local wound healing. 4 A meta-analysis demonstrated that the routine application of topical antibiotic agents to surgical incision did not reduce the incidence of SSIs for clean or clean-contaminated surgeries, and additional trials remain necessary to assess the effectiveness of topical antibiotic use after high-risk surgeries or for selected patient groups. 6 Therefore, we conducted a meta-analysis of RCTs to identify evidence for the efficacy and safety of topical antibiotic agents compared with non-antibiotic agents when used for the prevention of SSI after clean surgery.
Methods
This study has been conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses for Protocols (PRISMA) statement. 7
Literature search
Our literature search was performed to identify pertinent English-language scholarly journal articles indexed in the PubMed, Embase, and Cochrane Databases from 1980 to 2022 (Fig. 1). We used the terms “antibiotics,” “antimicrobials,” “antibacterial,” “antibacterial agents,” “antibiotic prophylaxis,” “anti-infective,” “topical,” and “topical antiinfective agent” combining with “surgical wound,” “surgical wound infection,” and “wound infection” as key words for the search.
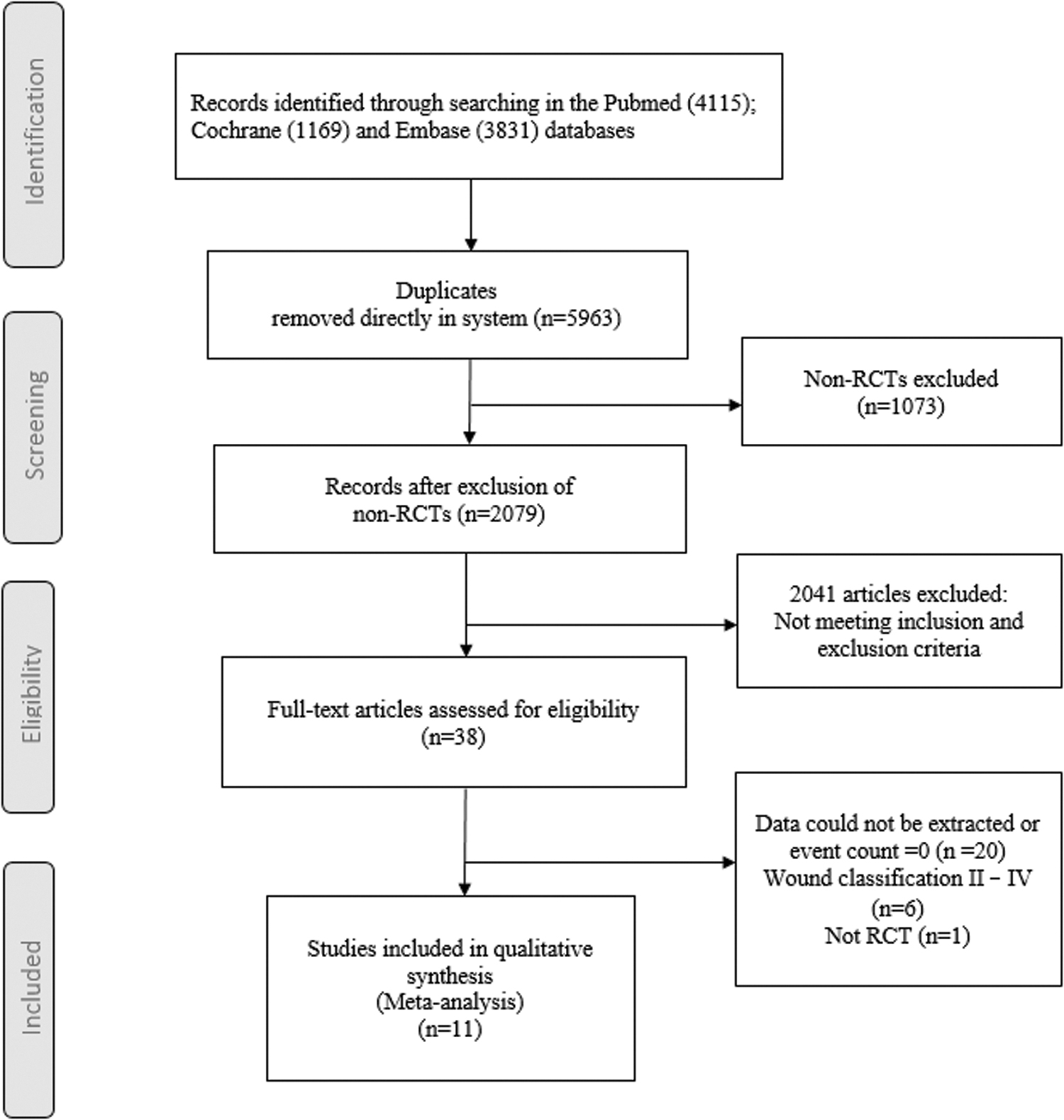
Preferred Reporting Items for Systematic reviews and Meta-Analyses for Protocols (PRISMA) flow diagram of the literature search.
Inclusion and exclusion criteria
We included RCTs evaluating the efficacy of prophylactic topical antibiotic use in patients undergoing surgeries that were specifically classified as clean (I). 2 Trials that described other wound classes were included if data from class (I) could be extracted. Different forms of topical antibiotic agents were included, including ointments, creams, lotions, and powders. Studies examining the use of irrigation solutions during surgery, the use of antibiotic dressings for incisions, and other forms of antibiotic delivery were excluded.
Quality appraisal
We adapted the Cochrane Collaboration recommendations to evaluate the quality of studies, and this standard is widely used in evidence-based reviews and meta-analyses. Two reviewers (W.-L.L. and C.-Y.H.) independently assessed the methodologic quality of each trial using the risk of bias method recommended by the Cochrane Collaboration. All domains were independently scored by the two co-authors for each study. Consensus was reached after classification by the individual researchers. Heterogeneity among studies was assessed using I2 statistics. The reference lists for all retrieved studies were cross-checked for additional reports.
Meta-analysis
Overall mean effect sizes were estimated using random-effects or fixed-effects models according to the heterogeneity among studies, with I2 values of 25%, 25%–50%, and more than 50% corresponding to small, moderate, and high heterogeneity, respectively. Fixed-effects models were used when I2 ≤ 50%.7,8 All statistical analyses were performed using RStudio Version 1.3.1093 (Posit PBC, Boston, MA, USA). The “metafor” package was applied to conduct the meta-analysis. Statistical significance was defined as a two-tailed p value <0.05.
Results
After removing 5,963 duplicates, we excluded 1,073 studies that were not identified as RCT during title and abstract screening. After further exclusions, the full-text of 38 studies were retrieved, and 12 trials with complete data were included in the meta-analysis (Fig. 1, Table 1). Figure 2 presents the pooled risk ratio (RR) and SSI incidence for groups treated with topical antibiotic agents or placebo for each type of surgery across 11 studies,9–19 after excluding one study that had an SSI event count of 0 and thus could not provide an estimate of incidence rate. 20 The combined total SSI event count of the 11 RCTs was 149 (of 3,687 participants) in the topical antibiotic group and 159 (of 3,820 participants) in the non-antibiotic group. Using random-effects modeling, the pooled RR for developing a post-surgical incision infection was 0.83 (95% confidence interval [CI], 0.61–1.16; I2, 0%). The quality appraisal results are shown in Table 2.

Meta-analysis of surgical site infections.
Summary of Included Studies (n = 11)
RCT = randomized controlled trial.
Quality Appraisal Using the Cochrane Collaboration Method
RCT = randomized controlled trial.
Seven trials9,12,13,17,19,20 had adequate randomization and sequence descriptions, and six trials utilized allocation concealment.11,13–15,17,19 In the blinding domains, five of the 11 trials had a high potential of bias due to the lack of participant blinding, and the practice of assessor blinding was unclear in four trials.11,12,16,18 One trial had a high potential of bias due to selective reporting. 8 Two trials14,17 in the topical antibiotic group administered nasal antibiotic agents, and four trials administered antibiotic agents.14,17,18,20
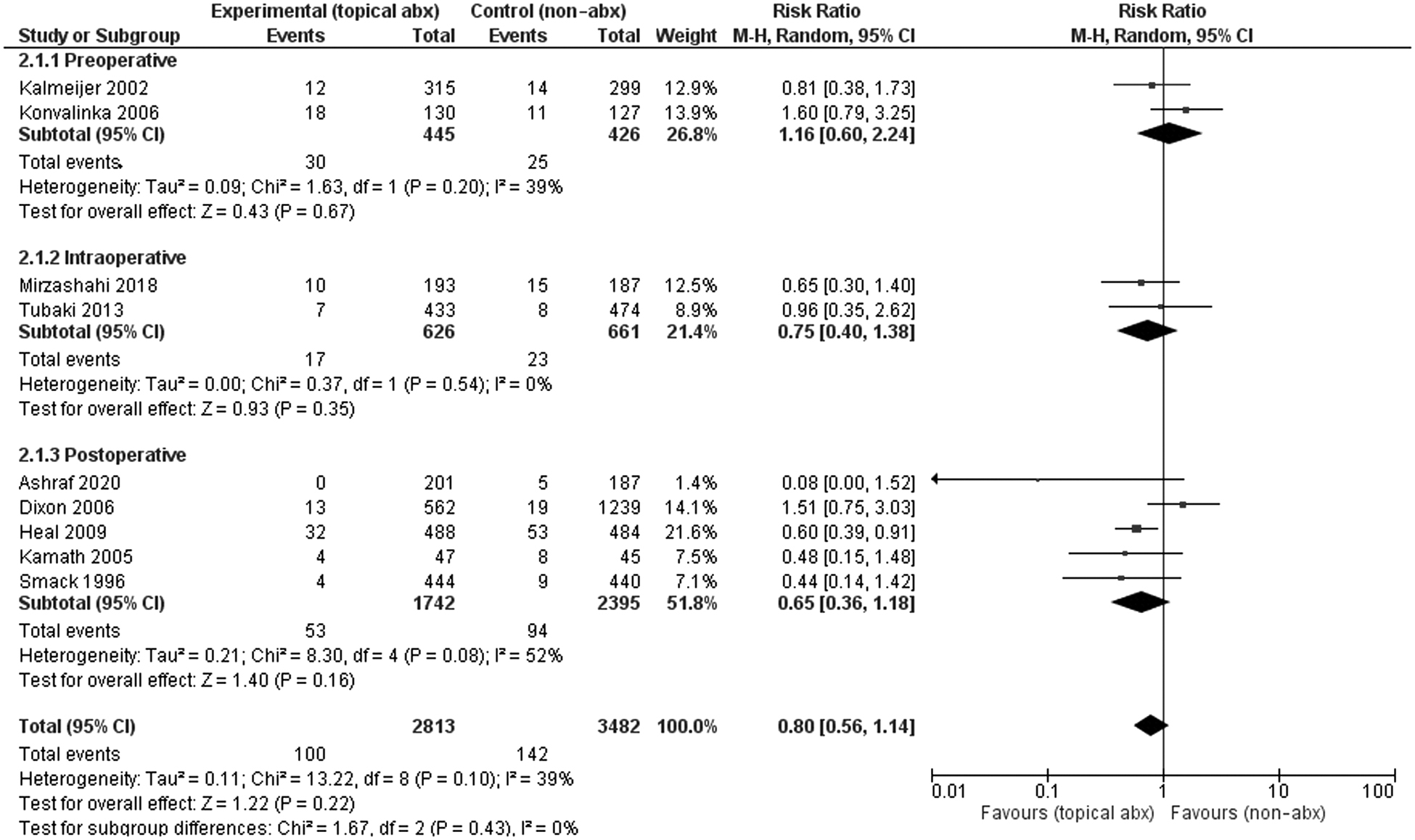
In the subgroup analyses, no reduction in SSI was observed in response to topical antibiotic use for spinal (RR, 0.75; 95% CI, 0.40–1.38; I2, 0%), orthopedic (RR, 0.69; 95% CI, 0.37–1.29; I2, 0%), dermatological (RR, 0.77; 95% CI, 0.39–1.55; I2, 65%), or cardiothoracic surgeries (RR, 1.31; 95% CI, 0.83–2.06; I2, 0%; Fig. 2). Furthermore, no significant difference in SSI incidence rates was observed according to the timing of antibiotic administration between topical antibiotic agents and non-antibiotic agents (RR, 0.80; 95% CI, 0.56–1.14; I2, 0%; Fig. 3).
Forest plot examining the incidence of contact dermatitis.
Five trials collected data on contact dermatitis, and two studies10,20 could not be included in the meta-analysis due to an event count of 0 (Fig. 4). No significant difference in the incidence rate of contact dermatitis was observed between the use of topical antibiotic agents and non-antibiotic agents (RR, 1.13; 95% CI, 0.36–3.58; I2, 37%).

Forest plot examining differences associated with antibiotic administration at various operative phases.
Discussion
Surgical site infection can delay incision healing, impair cosmetic outcomes, and increase healthcare costs. Topical antibiotic agents are sometimes used to reduce microbial contaminant exposure after surgical procedures, with the aim of reducing SSI occurrence. 12 Chen et al. 6 suggested that the results of studies examining the efficacy of prophylactic topical antibiotic use should be examined specifically for patients with clean (class 1) wounds. 13 The primary aim of this meta-analysis was to summarize and interpret all existing evidence from RTCs regarding the effects of topical antibiotic agents applied to clean surgical incisions on SSI rates. Our study was specifically targeted to examine RCTs comparing topical antibiotic and non-antibiotic agent use in patients with clean post-surgical incisions. Subgroup and sensitivity analyses were performed to assess heterogeneity and efficacy under specific conditions.
Eleven RCTs met the eligibility criteria for inclusion in the current review. The findings of our systematic review and meta-analysis indicate that topical antibiotic agents have no effect on reducing the occurrence of SSIs compared with non-antibiotic agents. Topical antibiotic agents do not need to be applied to surgical sites for the prevention of infection, with no beneficial effects identified for dermatologic, spinal, orthopedic, or cardiothoracic surgery. Our study findings are compatible with those reported in the meta-analysis conducted by Chen et al., 6 which showed that topical antibiotic agents could not reduce the risk of SSI compared with placebo (RR, 0.89; 95% CI, 0.59–1.32). Additionally, our analysis found no difference in the incidence of SSI between topical antibiotic agents and non-antibiotic agents across the operative phases of administration.
We found that the risk of contact dermatitis did not increase with the use of topical antibiotic agents after spinal, orthopedic, dermatological, or cardiothoracic surgeries. Under clean surgery conditions (class 1 wounds), for which the baseline infection rate is already low, the absolute risk reduction of SSI occurrence is likely smaller, and the case for using topical antibiotic agents is weaker than for other wound types. 13 Our review has contributed additional evidence, but clinical practice must be guided by clinical risks and benefits.
Limitations
Our meta-analysis study had some limitations that should be addressed. The inclusion of studies with high potential of bias is the primary weakness. In addition, this meta-analysis was limited to clean post-operative incisions, and the results might not be applicable to other types of incisions under other conditions. Nonetheless, the risk estimates observed in our study was very close to that obtained by the meta-analysis by Chen et al. 6 (0.83 vs. 0.89), which included both clean and clean-contaminated post-surgical incisions. However, some studies except for the RCT appear to favor topical treatment as the prevention post-operative incision infection. The favorable outcomes observed in non-randomized studies suggest the presence of a potential difference between the groups.
Conclusions
Although non-randomized studies may include potential biases and confounding factors that could influence the observed outcomes, we believe that this discrepancy highlights the need for further investigation and careful interpretation of the results.
Footnotes
Funding Information
This study was supported by a grant from the Chi Mei Medical Center and Kaohsiung Medical University Research Foundation (112CM-KMU-01(X112001)).
Author Disclosure Statement
The authors declare that they have no potential conflicts of interest.