
Abstract
Background:
Surgical antimicrobial prophylaxis (SAP) is the peri-operative administration of antimicrobial agents. Compliance rates vary worldwide from 15% to 84.3%, with studies in Turkey not exceeding 35%. The aim of this multicenter study was to determine the rate of appropriate antibiotic class, timing, and duration as well as discharge prescriptions in Turkey. Thus, we aimed to determine the rate of full compliance with SAP procedures in our country
Patients and Methods:
This multicenter, prospective, observational, descriptive study was conducted in 47 hospitals from 28 provinces in seven different regions of Turkey. Patients over 18 years of age in all surgical units between June 6, 2022, and June 10, 2022, were included in the study.
Results:
Of the 7,978 patients included in the study, 332 were excluded from further analyses because of pre-existing infection, and SAP compliance analyses were performed on the remaining 7,646 cases. The antibiotic most commonly used for SAP was cefazolin (n = 4,701; 61.5%), followed by third-generation cephalosporins (n = 596; 7.8%). The most common time to start SAP was within 30 minutes before surgery (n = 2,252; 32.5%), followed by 30 to 60 minutes before surgery (n = 1,638; 23.6%). Surgical antimicrobial prophylaxis duration was <24 hours in 3,516 (50.7%) patients and prolonged until discharge in 1,505 (21.7%) patients. Finally, the actual proportion of patients compliant with SAP was 19% (n = 1,452) after omitting 4,458 (58.3%) patients who were prescribed oral antibiotic agents at discharge as part of a prolonged SAP.
Conclusions:
Surgical antimicrobial prophylaxis compliance rates are still very low in Turkey. Prolonged duration of SAP and especially high rate of antibiotic prescription at discharge are the main reasons for non-compliance with SAP.
Surgical antimicrobial prophylaxis (SAP) is the peri-operative administration of antimicrobial agents to prevent surgical site infections (SSIs), which account for 14% to 17% of health-care–associated infections. 1 SSIs are primarily related to factors such as patient comorbidities, type of operation, and wound class, which is categorized as clean, clean-contaminated, contaminated, and dirty/infected. Surgical site infection rates by wound class are 1.3% to 2.9% for clean, 2.4% to 7.7% for clean-contaminated, 6.4% to 15.2% for contaminated, and 7.1% to 40% for dirty wounds. 2
There are published clinical practice guidelines for the management of SAP procedures, and each hospital in Turkey is required to establish its own local SAP policy.3,4 Among the antibiotic agents prescribed worldwide to hospitalized patients, 12% to 19% are for SAP and more than 50% of these antibiotic agents prescribed by surgeons are inappropriate according to SAP guidelines.5,6 The rate of full compliance with SAP guidelines in Turkey is very low and does not exceed 35%, and the compliance rate for antibiotic selection and time of first dose administration is relatively higher, whereas the compliance rate for antibiotic duration is very low.7–11
The aim of this multicenter study was to determine the rate of appropriate antibiotic class, timing of first dose, duration, as well as the availability of discharge prescriptions and finally the rate of full compliance with SAP procedures in Turkey.
Materials and Methods
Study design
This study was designed as a national, multicenter, prospective, observational, descriptive study to determine the compliance with prophylactic antibiotic use procedures in patients undergoing operation in Turkey. No intervention was performed during the study.
Study setting, population, and duration
The study was conducted in 47 hospitals from 28 provinces in seven different regions of Turkey, 13 of which were secondary care hospitals and 34 of which were tertiary care hospitals (Fig. 1).
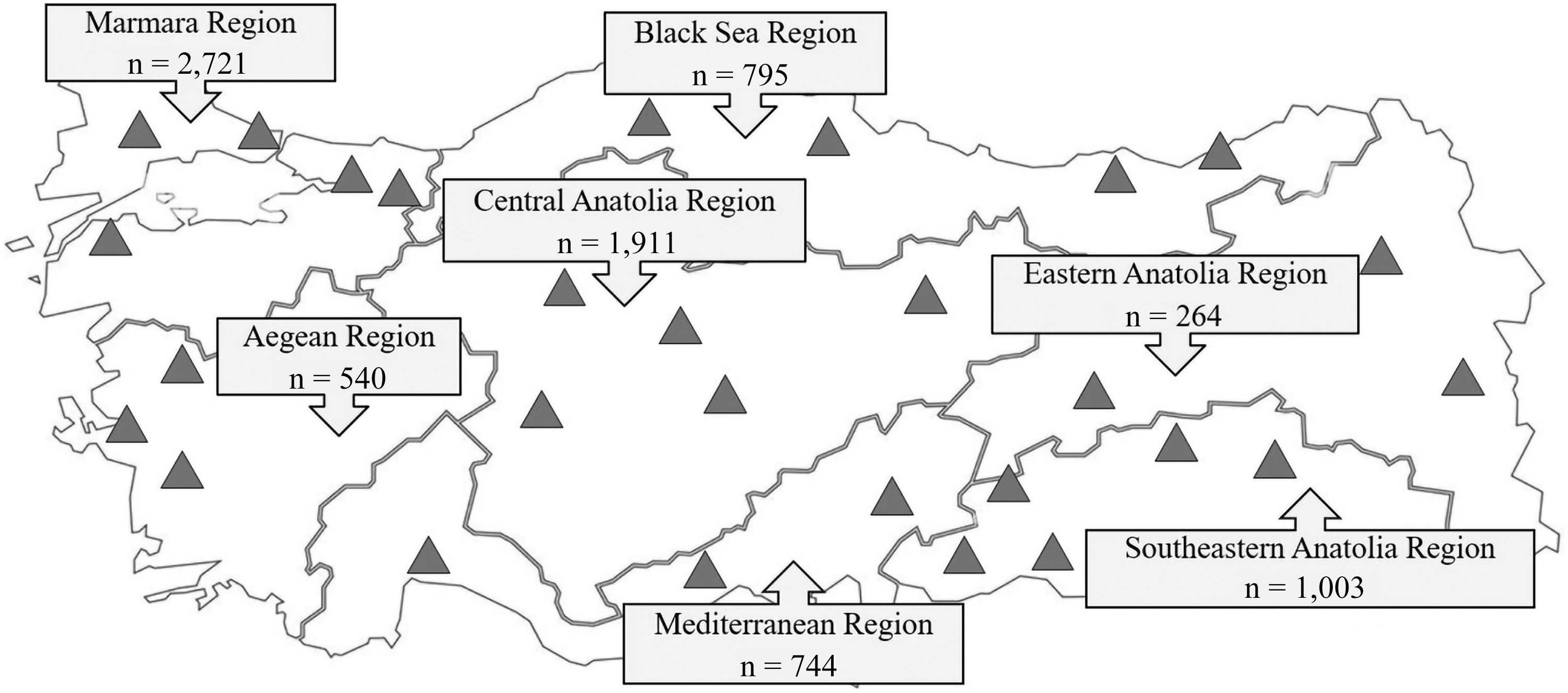
Distribution of patients in accordance with geographic regions in the study (n = 7,978); triangle indicates the provinces where the participating hospitals are located. The numbers in the boxes indicate the number of patients participating in the study from the relevant region.
All patients over 18 years of age who underwent scheduled/elective and emergent/urgent operation in all surgical units between June 6, 2022, and June 10, 2022, were included in the study. All patients were followed prospectively from the day SAP was initiated until the day it was discontinued. If SAP was not interrupted, follow-up continued until the patient was discharged from the hospital. In addition, whether patients received additional oral or parenteral antimicrobial agents as part of SAP at discharge was recorded.
Clinical standards for the administration of SAP
Clinical standards for SAP management in Turkey are based on three main guidelines. These guidelines include “Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery” (the American Society of Health-System Pharmacists [ASHP], the Infectious Disease Society of America [IDSA]; the Surgical Infection Society [SIS]; the Society for Healthcare Epidemiology of America [SHEA]); “Prevention Guidelines for the Prevention of Surgical Site Infection” (U.S. Centers for Disease Control and Prevention); and “Global Guidelines for the Prevention of Surgical Site Infection” (World Health Organization).3,4,10 The investigators were asked to assess whether there were significant differences between the institutional local guidelines and the quad-society guideline “Clinical Practice Guideline for Antimicrobial Prophylaxis in Surgery.” In general, local guidelines were consistent with the the quad-society guideline. Therefore, non-compliance in the study was assessed based on the quad-society guideline.
Indication for SAP, wound type, anatomic site of operation, type of operation, duration of operation, class of antibiotic, time of administration of SAP, and duration of SAP were the parameters considered in terms of compliance with SAP.
Patients who received pre-operative antibiotic treatment for surgical site-associated or non-site–associated infections or patients who received prolonged antibiotic use because of post-operative dirty-infected wounds were not considered non-compliant with SAP procedures and these patients were excluded from further analyses.
Data collection and analyses
A standard file using Excel (Microsoft Corp., Redmond, WA) program was created and sent to the responsible investigators at the participating centers. Patient demographic and clinical characteristics including the American Society of Anesthesiologists (ASA) score, wound class, type of anesthesia, type of operation, duration of operation, antibiotic class, time of SAP administration, and duration of SAP were recorded by infection control nurses or surgical nurses. The assessment of compliance with SAP was performed according to the quad-society guideline (Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery) and SAP instructions in the hospitals by the investigators at the centers. The role of the coordinating investigators as follows: standardization of the data in the Excel sheet, to review the database for mismatches between columns. When detected, the patients' database was sent back to the principal investigator to be corrected.
Baseline characteristics were presented as mean and standard deviation in years for age and as frequencies and percentages for categorical variables. We performed z-test analyzes to calculate the difference in SAP compliance rates between the subgroups. All statistical analyzes were performed by MedicReS E-PICOS AI Smart Biostatistics Software® version 21.3 (Medical & Research and Support Society, New York, NY).
Ethical approval
The Health Sciences University, Fatih Sultan Mehmet Training and Research Hospital, Clinical Research Ethics Committee (26.05.2022, 2022/10) approved the study.
Results
Of the total 7,978 patients included in the study, 1,369 were operated on in secondary care hospitals and 6,609 in tertiary care hospitals. The age of the patients ranged from 18 to 91 years (mean, 50; standard deviation [SD], 18 years) and 3,704 (46.4%) were male. When analyzing the distribution of patients according to department, the three clinics with the highest number of patients included in the study were general surgery (n = 1,972; 24.7%), gynecology (n = 1,248; 15.6%), and orthopedics (n = 1,158; 14.5%). Planned/elective operation was performed in 6,994 (87.7%), open operation in 6,329 (79.3%), and general anesthesia in 4,322 (54.2%) patients. According to wound class, 5,259 (65.9%) patients had clean, 2,347 (29.4%) clean-contaminated, 237 (3%) contaminated, and 135 (1.7%) dirty-infected wounds (Table 1).
Baseline Demographic and Clinical Parameters
The route of administration of SAP was the intravenous (IV) route in all patients. Cefazolin (n = 4,701; 61.5%) was the most commonly used antibiotic for SAP in the study, followed by third-generation cephalosporins (n = 596; 7.8%), and no SAP was prescribed in 712 (9.3%) patients with clean wounds. The most common time to start SAP was within 30 minutes before operation (n = 2,252; 32.5%), followed by 30 to 60 minutes before operation (n = 1,638; 23.6%). Due to reasons such as bleeding or prolonged operation, 420 patients received additional SAP doses. The duration of inpatient IV SAP was <24 hours in 3,516 (50.7%) patients, whereas it was prolonged until discharge in 1,505 (21.7%) patients. A total of 3,516 patients had received SAP for <24 hours, of whom 3,386 (96.3%) had received a single dose and 130 (3.7%) had received more than one dose. In addition to inpatient IV antibiotic agents, 4,458 (58.3%) patients were prescribed oral antibiotic agents at discharge as part of prolonged SAP (Table 2).
Distribution of Clinical Data Related to Prophylactic Antibiotic Use in the Study (n = 7,646 a )
SAP = surgical antibiotic prophylaxis; IV = intravenous.
Three hundred thirty-two patients were excluded from the analysis because they received antimicrobial agents for treatment of infection rather than prophylaxis.
In addition to a , 712 patients (120 from secondary hospitals, 592 from tertiary hospitals) were excluded from the analysis because they did not receive prophylaxis.
Proportion of those receiving a single dose of SAP with IV SAP administration duration <24 h.
Proportion of those receiving multidose SAP with IV SAP administration duration <24 h.
The diagram of the study that shows the stages of the SAP compliance assessment is shown in Figure 2. Of 7,978 cases included in the study, 332 were excluded from further analyzes because they were already receiving antimicrobial treatment for a pre-existing infection or were receiving prolonged antibiotic use due to dirty-infected wounds. Surgical antimicrobial prophylaxis antimicrobial adherence analyzes were performed on the remaining 7,646 cases. Of these patients, 1,874 (25%) did not receive SAP with the appropriate antibiotic class, including 145 who did not receive SAP when it was indicated, and 1,729 who received SAP that was not appropriate for the antibiotic class. The remaining 5,772 patients who received SAP with the appropriate antibiotic class were further evaluated for the timing of SAP administration. Of these, 5,047 patients received SAP at the appropriate administration time, whereas 725 patients did not. Of the remaining 5,047 patients, 1,991 received prolonged SAP, resulting in 3,056 patients with an appropriate class, timing, and duration of SAP, meaning in-hospital-SAP-compliance rate was 40%.
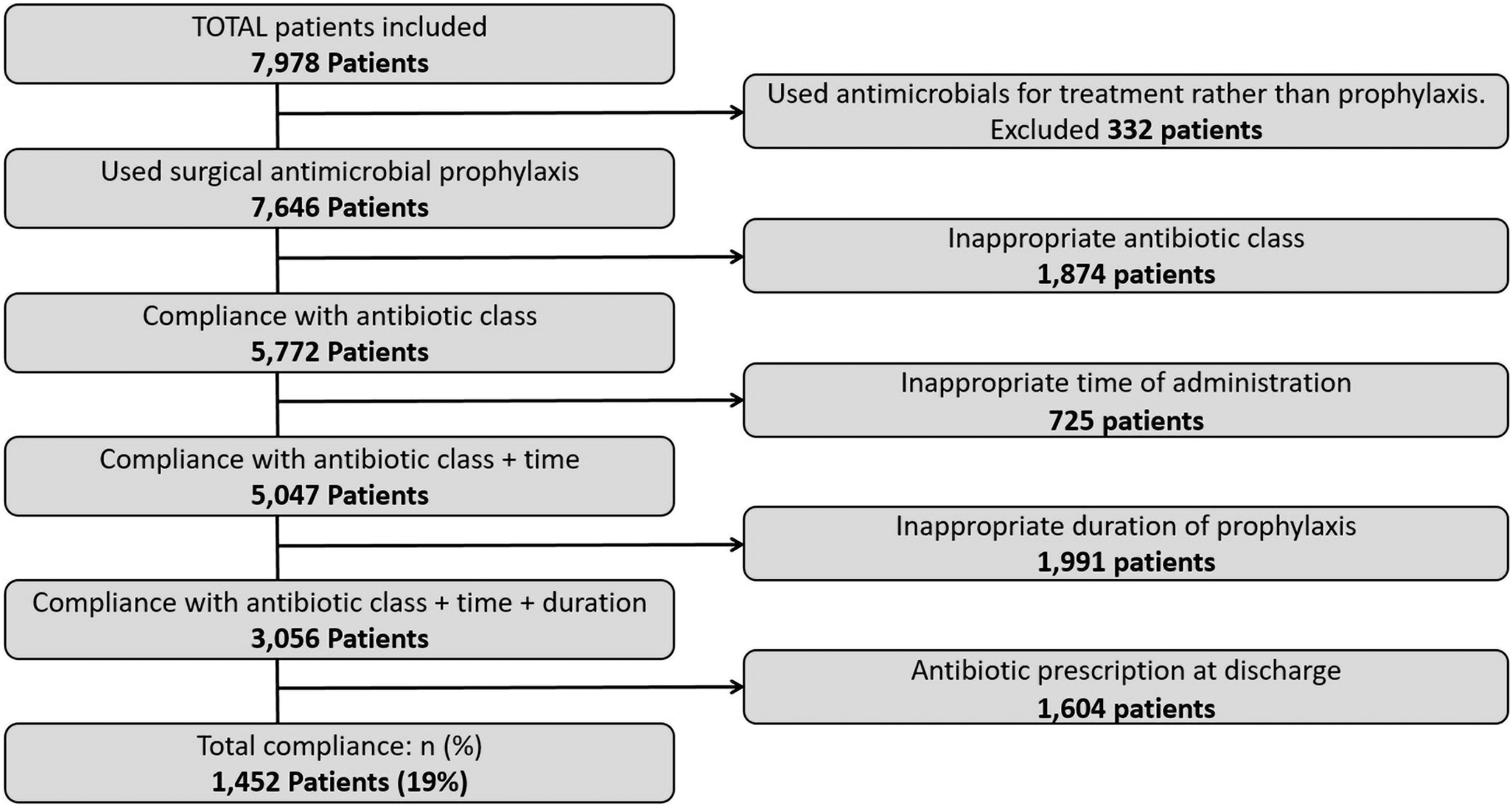
Flowchart of prophylaxis compliance.
We then examined how many of these patients were prescribed antibiotic agents at discharge. This further analyzes showed that 1,604 patients were prescribed antibiotic agents at discharge, and when these patients were considered to have prolonged SAP, the actual SAP compliance rate was calculated to be 19% (n = 1,452).
The difference in the distribution of patients by hospital level, class of surgery type, open/laparoscopic surgery and wound type of appropriate antibiotic selection, appropriate administration time, and duration of SAP and their combination is shown in Table 3. Surgical antimicrobial prophylaxis compliance was higher in tertiary hospitals than in secondary hospitals (19.6% vs. 16.0%; p < 0.01), and in open surgery than in laparoscopic surgery (19.7% vs. 16.2%; p = 0.001). There was no difference in SAP compliance between scheduled/elective surgery and emergency/urgent surgery (19.1% vs. 18.5%; p = 0.69). When evaluated by surgical wound type, SAP compliance was 22.3% in clean wounds, 12.9% in clean-contaminated wounds, 7.0% in contaminated wounds, and 9.6% in dirty infected wounds. According to these proportions, the difference between clean wounds and clean-contaminated wounds (p < 0.001) and between clean wounds and contaminated wounds (p < 0.001) was statistically significant.
Surgical Antimicrobial Prophylaxis Compliance Rates
Three hundred thirty-two patients were excluded from the analysis because they used antimicrobial agents for treatment of infection rather than prophylaxis.
Patients who were prescribed antibiotic agents at discharge were also included in the evaluation of antibiotic duration adherence.
The difference between clean wound and contaminated wound (p < 0.001); clean wound and dirty/infected wound (p < 0.001); clean/contaminated wound and contaminated wound (p = 0.001); clean/contaminated wound and dirty/infected wound (p < 0.001) is statistically significant.
The difference between clean wounds and clean contaminated wounds (p < 0.001) and between clean wounds and contaminated wounds (p < 0.001) is statistically significant.
The difference between clean wounds and clean contaminated wounds (p < 0.001) and between clean wounds and contaminated wounds (p < 0.001) is statistically significant.
According to the class of inappropriate antibiotic use for SAP, the three clinics with the highest rate were general surgery (40.4%), urology (24.5%), and orthopedics (20.5%), whereas the clinics with the lowest rate were thoracic surgery (1.1%) and plastic surgery (1.4%).
The lowest compliance with the timing and duration of SAP was observed in thoracic surgery (3.2%), whereas the best compliance was observed in ophthalmology (48.5%) and plastic surgery (45.3%). Overall, the departments with the highest rate of full compliance with SAP were plastic surgery (44.7%) and ophthalmology (43.9%), whereas thoracic surgery (3.2%) and urology (6.9%) had the lowest SAP compliance rates.
Discussion
Surgical antimicrobial prophylaxis is very important for the prevention of post-operative infections. Lack of SAP or improper use of SAP can lead to an increase in surgical infection rates. On the other hand, prolonged SAP and the use of broad-spectrum antibiotic agents have negative aspects such as increased costs and an increase in antibiotic resistance rates. The compliance with SAP in Turkey is very low according to literature. The aim of this multicenter study is to reveal the current rate of SAP compliance whether concordant with the literature.
The results of our study, which included 7,978 surgical patients from 47 centers in 28 cities, are very important in terms of providing current SAP compliance rates and detailed data on the use of SAP in Turkey, which has high rates of antibiotic resistance. We found that the rate of appropriate SAP implementation in Turkey is still very low at 19%. According to the literature, the overall rate of compliance with SAP guidelines in Turkey does not exceed 35%, and there are even studies that show that the rate of fully compliant SAP is as low as 13.7%.8–11 In addition, recent data from studies conducted in the last 5 years show that compliance rates vary worldwide, ranging from 15% to 84.3%.12–15
Adherence to the choice of antibiotic class and timing of antimicrobial agents is relatively better compared with the duration of antibiotic use, according to our study results and literature from Turkey.16–18 The compliance rate of appropriate choice of antibiotic class was 75.5% in our study, and cefazolin was the most commonly used antibiotic for SAP in our study, followed by third-generation cephalosporins. The primary antibiotic that was commonly used inappropriately in Turkey is ceftriaxone. 16 Studies have reported that third-generation cephalosporins are the most commonly used antibiotic in intra-abdominal, spinal, central nervous system, and urologic operations and the most commonly used alternative antibiotic in other operations.17,19 The compliance rate with the time of administration of the first dose of antibiotic agents was 85.6% in our study and similar rates are reported in studies from Turkey.7, 10
A recent randomized controlled trial showed no additional benefit of long-term SAP, 20 and several studies have also compared single-dose and multiple-dose SAP and found them equally effective.21–23 The main reason for non-compliance with SAP in developing countries is prolonged duration of SAP.12,19 Consistent with the literature, the most common reason for non-compliance in our results was non-adherence to the duration of antimicrobial use, with 50.7% noncompliant. According to the results of a multicenter study from Turkey, the rate of adherence to duration was higher than our results at 70.9%, but discharge prescription was not evaluated in this study. 16 Studies in the 2000s reported adherence rates for duration of antibiotic use of 47.7% and 20% in Turkey.18,19 It has been observed that these rates have not improved sufficiently in the intervening years.
As one of the key findings of our study, the rate of antibiotic prescription at discharge after operation was 58.3% and we found that SAP compliance rates decreased from 40% to 19% when considering the rate of antibiotic prescription at discharge. A recent Brazilian national survey also showed that 75% of surgeons maintained antibiotic agents for additional days after discharge. 24 Prescribing at discharge is addressed in few studies from Turkey. According to one study, the discharge-prescribing rate was 80.6%, which was higher than our results, but was reduced to 9.4% by training activities after the intervention. 9 With regard to prolonged SAP in Turkey, oral antibiotic prescription at discharge is one of the most important issues to be highlighted and prevented.
The first step in overcoming SAP noncompliance and improving SAP compliance is to identify the cause of noncompliance. Are surgeons unaware that SAP guidelines exist, or do they believe that the recommendations in these guidelines are inadequate? In Turkey, each hospital is required to develop and distribute SAP guidelines to clinicians. These should be distributed to all clinicians in the hospital, and the importance of complying with SAP should be constantly reiterated through training provided by the Infection Control Committee and the Antibiotic Control Committee. As in the rest of the world, long-term use of antimicrobial agents is believed to improve surgical outcomes in Turkey. Although 53.8% of surgeons were aware of written SAP procedures in their hospitals, 34% of surgeons surveyed reported that SAP practices were in line with their institution's guidelines, according to a 2017 multicenter survey of 410 surgeons in Turkey. 25 Of surgeons, 17% believe that the antibiotic recommendations in SAP guidelines are insufficient to prevent surgical infections, meaning that the considerable portion of SAP noncompliance is due to a lack of confidence in the adequacy of the recommended guidelines.
According to this survey, it was also determined that 56.1% of the surgeons who participated in the survey did not attend any training meeting on SAP within the institution. Surgical antimicrobial prophylaxis compliance was higher in those who received surgical prophylaxis training in the last three years, meaning that SAP compliance of surgeons can be increased with antimicrobial stewardship programs and training activities. 25
Martzivanou et al. 26 aimed to demonstrate the change in compliance with SAP guidelines through an intervention aimed at training healthcare staff. After 3 months of training and audit, compliance rates increased, hospitalizations decreased and antibiotic costs decreased. A study by Díaz-Madriz et al. 27 used a five-year antimicrobial stewardship program to increase surgeon compliance with SAP. Selection of the appropriate antibiotic class for SAP increased by up to 80% after this intervention. Cefazolin use increased more than ninefold while ceftriaxone use among surgeons increased. The rate of SAP administration at the appropriate time and duration increased from 69.1% to 78.0% and no increase in SSI rates was detected in the post-operative follow-up.26,27
As part of a study by Bozkurt et al. 28 from Turkey analyzing antimicrobial consumption and costs, unnecessary SAP implementation decreased from 17.2% to 6.2% and inappropriate SAP implementation decreased from 72.5% to 37.5%, whereas the proportion of appropriate SAP increased from 10.3% to 56.3% through their implementations. Their interventions were based on identifying one physician from each clinic, close contact with them, educational activities, close monitoring of practices, and regular communication of results to each physician. In a study by Karaali et al. 28 in Turkey, the overall SAP compliance rate increased from 8% to 52.1% after the intervention of a model based on a surgical team leader with SAP training and regular staff training.
Conclusions
In conclusion, SAP compliance rates in Turkey are still very low, despite the fact that each hospital has its own SAP guidelines and even restrictive measures regarding the prescription of antibiotic agents in the hospital. The results of the studies from Turkey show that current practices to increase SAP compliance do not seem to be sufficient to convince surgeons and create sustainable behavioral changes in surgeons. To increase compliance with SAP practices, achievable SAP compliance goals should be set at the national level, local efforts to increase SAP compliance rates should be standardized within a national program developed in line with these goals, and SAP compliance data should be shared regularly and systematically. All efforts to increase SAP compliance should put surgeons at the center of all activities, taking into account the healthcare infrastructure and epidemiologic factors specific to our country, and should aim to convince surgeons and address their concerns.
Limitations of the study
This study, which included 7,978 patients from 47 hospitals in 28 provinces from all regions of Turkey, is one of the most comprehensive studies on SAP. However, the selection of the 47 participating centers in the study design was based on the voluntary participation of the infectious disease specialists in the participating centers, and no epidemiological method such as stratified sampling was used to minimize selection bias. Therefore, the interpretation of the study results as data for Turkey as a whole should be with caution.
There were 332 patients who were already receiving antimicrobial treatment for a pre-existing infection. Because this situation was not anticipated during the study design phase and detailed data were not collected on these patients during the data collection phase, further evaluation for SAP appropriateness analyses could not be performed.
The study did not assess the effectiveness of prolonged SAP, nor did it monitor patients' adherence to the oral prophylaxis prescription provided upon discharge. Although this is not a limitation because the aim of the study was to evaluate surgeon compliance with SAP, it should be taken into consideration when interpreting the results.
Footnotes
Acknowledgments
The Surgical Prophylaxis Working Group of the Association for the Prevention of Infectious Diseases (BUHASDER) conducted this study
We would like to express our gratitude to our esteemed colleague Dr. Mehmet Selim Şahin, specialist in Infectious Diseases and Clinical Microbiology, who lost his life in the great earthquake that occurred in Turkey on February 6, 2023, while working at Adıyaman University Faculty of Medicine Adıyaman Training and Research Hospital, his family and loved ones. We would like to thank our esteemed colleague Associate Professor Fatma Gümüşer for her contributions to our study.
Authors' Contributions
Conceptualization: S.Ç.E., E.Y. Data curation: S.Ç.E., E.Y., G.A.Ö., M.Ç.S., A.T., C.A., D.A., D.S., C.A., E.Z., Ş.K., M.Ç., Ş.Ç., İ.E.Y., F.Ç., F.A., Ö.A., M.B., D.Ö., L.H., E.C.Ü., D.G.A., A.Ş., G.Ü., A.E.G., S.T.Ş., Y.Ö., S.Ü., S.S., F.Y.K., J.A., S.A.I., Ö.G., N.T., S.Ş., M.Ö., P.E.K., M.E.I., A.K., K.K., A.C.Y., S.V., Y.O., Y.Ç., N.Ö.Y., S.K., A.B., Z.C.D., Ş.K. Formal analyzes: S.Ç.E., E.Y., H.K.R. Investigation: S.Ç.E., E.Y., G.A.Ö., M.Ç.S., C.A., D.A., D.S., C.A., E.Z., Ş.K., M.Ç., Ş.Ç., İ.E.Y, F.A., Ö.A., M.B., D.Ö., L.H., E.C.Ü., D.G.A., A.Ş., G.Ü., A.E.G., S.T.Ş., Y.Ö., S.Ü., S.S., F.Y.K., J.A., S.A.I., Ö.G., N.T., S.Ş., M.Ö., P.E.K., M.E.I., A.K., K.K., A.C.Y., S.V., Y.O., N.Ö.Y., S.K., A.B., Z.C.D. Methodology: S.Ç.E., E.Y. Project administration: S.Ç.E., E.Y. Resources: S.Ç.E., E.Y., G.A.Ö., M.Ç.S., A.T., C.A., D.A., D.S., C.A., E.Z., Ş.K., M.Ç., Ş.Ç., İ.E.Y., F.Ç., F.A., Ö.A., M.B., D.Ö., L.H., E.C.Ü., D.G.A., A.Ş., G.Ü., A.E.G., S.T.Ş., Y.Ö., S.Ü., S.S., F.Y.K., J.A., S.A.I., Ö.G., N.T., S.Ş., M.Ö., P.E.K., M.E.I., A.K., K.K., A.C.Y., S.V., Y.O., Y.Ç., N.Ö.Y., S.K., A.B., Z.C.D., Ş.K. Supervision: S.Ç.E., E.Y., Ş.K. Visualization: S.Ç.E., E.Y., A.T., F.Ç., Y.Ç., H.K.R., Ş.K. Writing—original draft: S.Ç.E., E.Y. Writing—review and editing: S.Ç.E., E.Y.
Funding Information
The authors received no funding for this study or the preparation of the manuscript.
Author Disclosure Statement
The authors have no conflicts of interest or financial relations to declare. All authors meet the Surgical Infections requirements for authorship.