
Abstract
Background:
This study aimed to investigate the clinical value of inflammatory factors for predicting anastomotic leakage (AL) after laparoscopic colorectal cancer surgery and establish a nomogram model to assess the probability of its occurrence.
Patients and Methods:
Data of 637 patients who underwent laparoscopic colorectal cancer surgery between June 2019 and June 2022 were collected. Differences in procalcitonin (PCT), C-reactive protein (CRP), and white blood cell (WBC) levels before surgery and on postoperative day (POD) 3 and 5 were compared between patients with and without AL (AL and non-AL groups, respectively). The diagnostic accuracy was determined using the area under the receiver operating characteristic curve (AUC), and a nomogram model was developed.
Results:
Post-operative AL occurred in 46 (7.2%) patients. Procalcitonin, CRP, and WBC levels on POD 3 and 5 were higher in the AL group than in the non-AL group. The AUCs of PCT, CRP, and WBC levels for predicting AL on POD 3 were 0.833, 0.757, and 0.756, respectively, which were better than those on POD 5 (AUC = 0.669, 0.581, and 0.588, respectively). The nomogram model for AL was developed based on five variables (PCT, CRP, WBC, American Society of Anesthesiologists [ASA] grade and comorbidities), and it had an AUC of 0.922. Calibration curves demonstrated that the nomogram had good fit. The Delong test showed that the AUC of the nomogram for predicting the probability of AL was higher than that of PCT alone (z = 2.311, p = 0.02).
Conclusions:
Procalcitonin measured on POD 3 seems to be a promising negative predictor of AL after laparoscopic colorectal cancer surgery. Furthermore, the nomogram model developed in our study, which utilizes a series of predictors that can be easily accessed, has demonstrated potential to further improve the prediction accuracy.
Colorectal cancer is the third most common cancer and the second leading cause of cancer-related death. 1 Because of recent technological developments in surgical oncology, laparoscopic surgery has become widely used for surgical management of colorectal cancer. However, it is associated with a potentially delayed diagnosis of post-operative anastomotic leakage (AL), 2 which is one of the most common complications of laparoscopic colorectal cancer resection. Anastomotic leakage can lead to infection or other complications, which further lead to prolonged hospital stay, increased costs, peri-operative mortality, local tumor recurrence, and reduced long-term survival. 3 Early diagnosis of AL is critical for improving patient outcomes. However, early diagnosis remains a challenge for surgeons. Currently, there is still a lack of evidence regarding reliable biomarkers for the early individualized prediction of AL after laparoscopic colorectal cancer surgery. These predictive biomarkers could potentially ensure early and safe discharge.
Studies 4 have suggested an association between infection markers and post-operative complications including AL. Zielińska-Borkowska et al. 5 reported that procalcitonin (PCT), rather than interleukin-6 (IL-6), is a reliable indicator for the early identification of AL after colorectal surgery, and safety verification of early discharge. High serum C-reactive protein (CRP) and white blood cell (WBC) levels could also be associated with septic intra-abdominal complications such as early-stage AL.6,7 However, few studies have investigated the predictive values of PCT, CRP, and WBC levels for AL after laparoscopic colorectal cancer surgery. Additionally, the few previous studies that compared the value of PCT and CRP in predicting post-operative AL reported controversial findings.8,9 It also needs to be explored whether PCT combined with CRP and WBC counts can improve the accuracy of predicting post-operative AL.
In the present study, we investigated the clinical value of inflammatory factors in predicting AL after laparoscopic colorectal cancer surgery based on a large sample size. We also developed and validated an efficient and reliable clinical nomogram model for the assessment of AL. Our results would help colorectal surgeons assess the risk of post-operative AL more easily and promote enhanced post-operative recovery.
Patients and Methods
Study population
Medical records of patients who underwent laparoscopic colorectal cancer surgery between June 2019 and June 2022 at the Union Hospital, TongJi Medical College, Huazhong University of Science and Technology, were analyzed retrospectively. The inclusion criteria were as follows: age ≥18 years; pre-operative colonoscopy biopsy-confirmed colon cancer or rectal cancer; pre-operative imaging confirmed no distant metastasis; underwent laparoscopic surgery; and complete resection. The exclusion criteria were as follows: pre-operative ongoing infection; laparotomy or unplanned conversion to laparotomy; or irretrievable data. A flow chart of the patient selection process is shown n Figure 1. This study was conducted in accordance with the principles established in the Declaration of Helsinki and was approved by the Ethics Committee of the Union Hospital, TongJi Medical College, Huazhong University of Science and Technology. The data were anonymized and the requirement for informed consent was waived.

Flow diagram of included and excluded patients.
Definition of AL and all infection complications
In our study, AL was clinically defined as the discharge of pus, feces, or gas from the abdominal drain; peritonitis caused by leakage; and development of a pelvic abscess. All symptomatic AL were confirmed using computed tomography (CT) or contrast-enhanced fluoroscopy. 10 Post-operative infectious complications (AL, wound infection, pneumonia, urinary tract infection, central venous catheter infection, etc.) were classified into grades 1 to 4 according to the Clavien-Dindo classification system as follows: grade 1, any deviation from the normal post-operative course without life-threatening events, permanent disability or prolonged hospital stay; grade 2, potentially life-threatening complications without any residual disability; grade 3, residual disability, including organ resection or persistence of life-threatening conditions; and grade 4, death caused by complications.
Data collection
Data regarding gender, age, body mass index (BMI), smoking history, American Society of Anesthesiologists (ASA) physical status classification, pre-operative comorbidities (diabetes mellitus, cardiovascular disease, renal failure, and malnutrition), operation time, neoadjuvant therapy, prophylactic stoma, resection site, and tumor-node-metastasis (TNM) stage were documented. Serum WBC, CRP, and PCT levels were recorded before surgery and on post-operative day (POD) 3 and 5. Tumor-node-metastasis staging was performed according to the eighth edition of the American Joint Committee on Cancer Staging Manual.
Statistical analysis
T-tests were used to assess differences in continuous variables between the AL and non-AL groups. Multivariable logistic regression analysis was conducted to screen independent predictors for AL. Receiver operating characteristic (ROC) curve analysis was used to determine the optimal cutoff value of each variable for predicting AL. A diagnostic nomogram model was constructed based on the potential predictive variables. The model for the nomogram was selected using a stepwise forward method. The choice of final model was determined by the minimum Akaike Information Criterion (AIC). Comparisons of area under the curves (AUC) were performed using DeLong's test. Receiver operating characteristic, calibration, and decision curves were drawn to evaluate the predictive power of the model. Statistical significance was considered at a two-tailed p < 0.05. All statistical analyses were conducted using STATA, version 15 (StataCorp, College Station, TX) and SPSS Statistics, version 22.0 (IBM Corp, Armonk, NY) software.
Results
Baseline characteristics
Based on the inclusion and exclusion criteria, 637 patients were included in this study. These included 402 males and 235 females. The mean age was 59 ± 12 years and mean BMI was 23.02 ± 3.42 kg/m2. A total of 165 (26%) patients had pre-operative comorbidities. More than 96% of the patients were classified as ASA 1 or 2 (19.5% and 77.2%, respectively). Only 21 patients (3.3%) were classified as ASA 3. All surgeries were completed laparoscopically without any peri-operative deaths. The average operative time was 236 ± 84 minutes. One hundred patients (15.7%) underwent pre-operative neoadjuvant therapy. Left hemicolectomy was performed in 170 (26.7%), right hemicolectomy in 149 (23.4%), proctectomy in 314 (49.3%), and total colectomy in 4 (0.6%) cases. Prophylactic ileostomy was performed in 125 (19.6%) cases, during surgery. Fifty, 111, 123, and 353 patients were diagnosed with TNM stage 0, 1, 2, and 3, respectively.
Incidence of AL
Post-operative infectious complications occurred in 95 (14.9%) patients, of whom 46 (7.2%) had post-operative AL. The other infectious complications included eight wound infections, 32 cases of pneumonia, three urinary tract infections, and six central venous catheter infections. The median time interval between surgery and AL diagnosis was six days (interquartile range, 5–7 days). Two patients underwent secondary surgical treatment, three received adequate abdominal drainage, and 41 were treated with anti-infection treatment and nutritional support; all patients had grade 2 AL. All patients were ultimately discharged uneventfully after receiving active and effective treatment. The patients were divided into AL and non-AL groups. Patients with infectious complications other than AL were excluded from the non-AL group to create a more homogeneous group. The baseline characteristics of the two groups are listed in Table 1. Pre-operative comorbidities were more common in the AL group as compared with the non-AL group (p < 0.001).
Clinical Characteristic of Patients With and Without AL
AL = anastomotic leakage; ASA = American Society of Anesthesiologists; BMI = body mass index; TNM = tumor-node-metastasis stage.
Indicates statistical significance at p < 0.05.
Cutoff and clinical value of PCT, CRP, and WBC levels for diagnosing post-operative AL
There were no statistically significant differences in pre-operative PCT, CRP, or WBC levels between the AL and non-AL groups. The PCT, CRP and WBC levels on POD 3 were higher in the AL group than in the non-AL group (PCT, 2.33 ng/mL vs. 0.92 ng/mL; p < 0.001; CRP, 125.89 mg/L vs. 81.5 mg/L; p < 0.001; WBC, 10.32 × 109/L vs. 7.82 × 109/L; p < 0.001). Similarly, the PCT, CRP, and WBC levels on POD 5 were higher in the AL group than in the non-AL group (PCT, 0.98 ng/mL vs. 0.54 ng/mL; p = 0.022; CRP, 54.43 mg/L vs. 43.16 mg/L; p = 0.023; WBC, 7.15 × 109/L vs. 6.35 × 109/L; p = 0.016; Table 2).
Comparison of WBC, PCT, and CRP between Non-AL Group and AL Group
AL = anastomotic leakage; WBC = white blood cell; CRP = C-reactive protein; PCT = procalcitonin; POD = postoperative day; PRE = pre-operative.
Indicates statistical significance at p < 0.05.
The diagnostic performances of WBC, PCT, and CRP levels (both on POD 3 and POD 5) for AL were assessed using ROC curves, and the optimal cutoff value of each indicator was obtained. The optimal WBC cutoff on POD 3 was 8.8 × 109/L. At this cutoff, the AUC was 0.756, the sensitivity was 73.9%, the specificity was 70.7%, the negative predictive value (NPV) was 98%, and the positive predictive value (PPV) was 21.9%. The optimal cutoff for PCT was 1.0 ng/mL. At this cutoff, the AUC, specificity, sensitivity, NPV, and PPV were 0.833, 73.8%, 89.1%, 98%, and 25%, respectively. The optimal cutoff was 72.1 mg/L for POD 3 CRP. At this cutoff, the AUC was 0.757, the specificity was 48.0%, the sensitivity was 91.3%, the NPV was 99.2%, and the PPV was 14%. The optimal cutoffs for WBC, PCT, and CRP on POD 5 were 6.57 × 109/L, 0.18 ng/mL, and 42.6 mg/L, respectively. The corresponding AUCs, sensitivities, specificities, NPVs, and PPVs have been presented in Figure 2 and Table 3.

Receiver operating characteristic (ROC) curves of white blood cell (WBC) count (
Comparison of the Accuracy of WBC, CRP, and PCT to Predict AL
AL = anastomotic leakage; AUC = area under the curve; CI = confidence interval; WBC = white blood cell; CRP = C-reactive protein; NPV = negative predictive value; PCT = procalcitonin; POD = post-operative day; PPV = positive predictive value.
Performance of PCT, CRP for diagnosing post-operative infectious complications
We also assessed the performance of CRP and PCT levels as diagnostic markers for all post-operative infectious complications after laparoscopic colorectal cancer resection. There were no statistically significant differences in the pre-operative PCT and CRP levels between the infected and non-infected groups. PCT and CRP levels on POD3/5 were significantly higher in the infected group than in the non-infected group (Supplementary Table S1). The AUCs of PCT and CRP levels on POD 3 were 0.634 (95% confidence interval [CI], 0.551–0.717) and 0.742 (95% CI, 0.689–0.794), respectively. The AUCs of the ROC plots for PCT and CRP levels on POD 5 were 0.739 (95% CI, 0.686–0.791), and 0.790 (95% CI, 0.732–0.849), respectively.
Construction of the diagnostic nomogram model
To achieve an early diagnosis of AL, PCT, CRP, and WBC levels on POD 3 were selected as candidate predictive parameters for AL after laparoscopic colorectal cancer surgery. We also incorporated risk factors (pre-operative comorbidities, age and ASA grade) for variables selection. Using stepwise regression method, these variables were subsequently filtered in the multivariate logistic regression model (Supplementary Table S2). Finally, the model including WBC, CRP, PCT, ASA and pre-operative comorbidities reached the minimal AIC (196.89), which showed the best goodness of fit. Therefore, a nomogram model for AL risk assessment was constructed, with high PCT having the highest score (10.1 points), followed by high ASA grade (10 points), high CRP (8.6 points), high WBC levels (7.3 points), and pre-operative comorbidities (7 points). The total score was computed by summing the individual scores based on the patient's clinical parameters. The total score was subsequently located on the total point line, and a straight line was drawn to estimate the patient's probability of AL from the nomogram. As demonstrated in Figure 3, the higher total scores, the higher risk of AL.

The diagnostic nomogram model for anastomotic leakage (AL) after colorectal cancer surgery.
Validation of the diagnostic nomogram model
Internal validation demonstrated that the AUC for the AL prediction nomogram was 0.922 (Fig. 4A). Calibration plots for AL probability showed that there was optimal concordance between the predicted and observed occurrences (Fig. 4B). The decision curve demonstrated a high net benefit across the entire spectrum of probability thresholds (Fig. 4C), indicating that the model could provide additional clinical benefits when predicting AL probability thresholds from 13% to 84%. Moreover, at a probability threshold of 10%, the net reduction in intervention was approximately 60 per 100 patients (Fig. 4D). These results indicate the predictive performance and discriminative ability of this model. In addition, the AUC of the nomogram for predicting the probability of AL was higher than that of PCT alone (z = 2.311, p = 0.02).
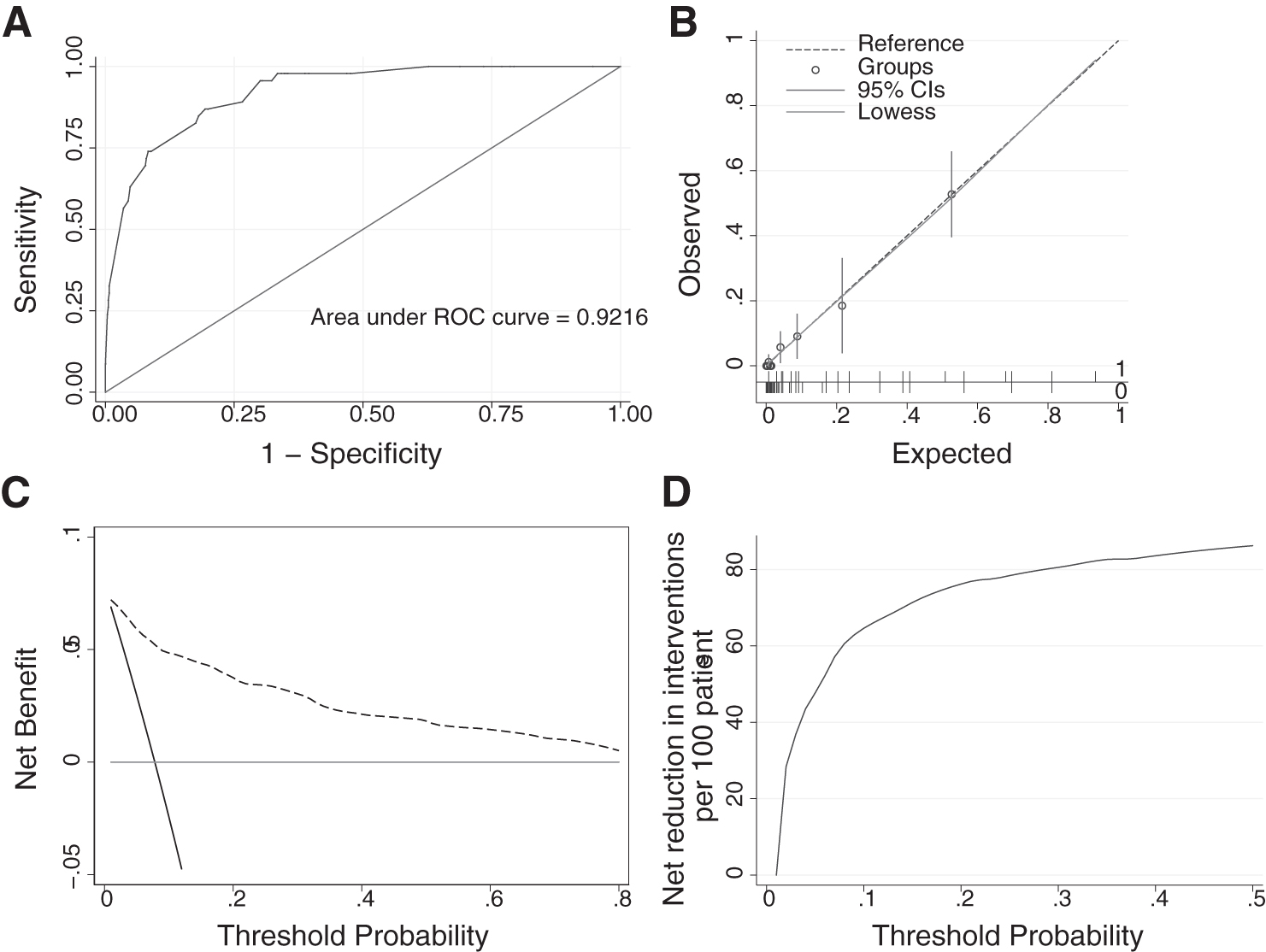
The performance of the nomogram.
Discussion
In recent years, laparoscopic surgery has been increasingly widely used for the surgical management of colorectal cancer. Its advantages over open surgery included smaller surgical wounds, rapid recovery time, and shorter hospital stay. However, AL is still one of the most serious post-operative complications of colorectal surgery, resulting in a mortality rate of 1.7% to 16.4%.11,12 Therefore, the accurate diagnosis and early management of AL are of great clinical importance. Anastomotic leakage is generally asymptomatic in the early stages. In the later stages, it is characterized by the drainage of free fecal fluid from the abdominal or pelvic drain site after surgery. Systemic symptoms such as chills, fever, and septic shock may occur with an increased severity of infection. 13 Anastomotic leakage increases the length of hospital stay and hospitalization costs, and also worsen prognosis. 14
In this study, high ASA grades and pre-operative comorbidities were more prevalent in the AL group than in the non-AL group. Therefore, preventive and protective measures should be implemented after surgery in patients with higher ASA scores and pre-operative comorbidities, such as obesity, diabetes mellitus, and immunosuppression. However, in patients without the abovementioned high-risk factors, delayed intervention after false-negative CT scans was associated with increased mortality and a longer hospital stay. 15 Therefore, early detection of post-operative AL is of great importance in clinical practice.
Studies have suggested that inflammatory markers could contribute to the early recognition of AL after colorectal surgery.16,17 Although the WBC count is the most commonly used metric to investigate infection, its role in identifying post-operative AL remains controversial. Muñoz et al. 18 observed that the WBC count was not a specific marker for detecting post-operative AL after laparoscopic colorectal surgery. However, Morimoto et al. 19 reported that pre-operative WBC count was an independent predictor of AL after left-sided colorectal cancer surgery; a WBC count greater than the cutoff value was crucial for identifying infectious complications such as AL. In our study, we observed that WBC levels on POD 3 could be useful in excluding the possibility of leakage; however, the predictive value was relatively low. Further studies are required to confirm the diagnostic performance of WBC count as a marker for post-operative AL.
C-reactive protein, a non-specific acute-phase protein, is mainly derived from hepatocytes in response to IL-6. During acute infection, CRP levels increase substantially. C-reactive protein levels have been used to identify infectious complications, including AL, after colorectal surgery. 20 Bertocchi et al. 21 reported that a change in the CRP trajectory is a potential marker for AL. Furthermore, consecutive CRP measurements are useful for predicting AL in females undergoing laparoscopic colorectal resection for deep infiltrating endometriosis. Jin et al. 22 indicated that the CRP level is a reliable predictor of AL after laparoscopic transabdominal rectal resection surgery.
Interestingly, relatively few studies have examined the role of CRP levels in detecting AL after laparoscopic colorectal surgery. Our results demonstrated that serum CRP on POD 3 is a helpful negative biomarker for the early diagnosis of AL in patients who have undergone laparoscopic colorectal cancer surgery. C-reactive protein levels may also offer superior diagnostic accuracy compared with WBC count in the detection of AL. Therefore, CRP measurement on POD 3 is useful as a predictor of AL after laparoscopic colorectal cancer surgery.
Procalcitonin is a glycoprotein without hormonal activity. It is a diagnostic biomarker for bacterial infection and is widely considered to be a suitable tool for detecting sepsis and severe bacterial infections in the early stages. 23 Recent studies24,25 have reported that serum PCT levels were positively correlated with the severity of the AL-induced inflammatory response after colorectal cancer surgery. Hence, PCT may be a useful indicator for the early diagnosis of AL. However, the optimal time to assess PCT levels as a predictor of AL remains unclear. Bruce et al. 26 observed that PCT levels on POD 5 had the highest diagnostic accuracy for AL, whereas Xu et al. 27 demonstrated that serum PCT levels on POD 3 have great clinical value for the early diagnosis of AL. Therefore, it is essential to identify the optimal time for PCT measurement for the early prediction of AL.
Moreover, there were discrepancies in the study findings regarding the accuracy of CRP and PCT in predicting AL after colorectal surgery. 28 This could be related to different objectives, end points, and surgical approaches. In our study, PCT on POD 3 exhibited better diagnostic accuracy than CRP on POD 3 (AUC = 0.833 and 0.757, respectively), indicating that PCT is a better predictor of AL in patients undergoing laparoscopic colorectal cancer surgery. Furthermore, the AUC of CRP was higher than that of PCT for detecting all infective complications in our study, which is consistent with the findings of Amanai et al. 29 This could be because the pathogen distributions at different infection sites are different. Grotelueschen et al. 30 observed that gram-negative Escherichia coli and Enterobacteriaceae were the most frequently detected micro-organisms in patients with colorectal leakage. Yan et al. 31 indicated that PCT exhibited good discrimination between Escherichia coli and non-fermentative gram-negative bacteria. Therefore, PCT may outperform CRP in predicting AL, it was not superior to CRP in predicting all infectious complications after colorectal cancer surgery.
Further studies are required to investigate whether PCT and other inflammation markers can be combined for more effective prediction of AL. In this study, we explored the diagnostic value of PCT, CRP, and WBC levels for AL after laparoscopic colorectal cancer surgery. We observed that the serum levels of these three potential biomarkers were significantly higher in the AL group than in the non-AL group, especially on POD 3. Furthermore, ROC curve analysis indicated that WBC, PCT, and CRP levels on POD 3 had a better diagnostic accuracy for AL than those on POD 5. Therefore, we used these biomarkers on POD 3 as potential predictors for model construction. After successively performing stepwise regression analysis, CRP, PCT, and WBC levels on POD 3 were used to construct a nomogram to diagnose AL after laparoscopic colorectal cancer surgery.
Nomograms are graphical representations that are intuitive and easy to use. They have been widely applied in the medical field to generate the individual probability of a clinical event to develop personalized medicine further. 32 Recent studies33,34 have reported various nomogram models for predicting the likelihood of post-operative complications after tumor resection. However, a diagnostic nomogram model for AL after laparoscopic colorectal cancer surgery has not been explored extensively. In this study, we constructed a nomogram-based diagnostic model by combining PCT 3, CRP 3, WBC 3, ASA and pre-operative comorbidities. The nomogram demonstrated that higher total points based on the sum of the assigned number of points for each predictor in the model were associated with an increased risk of AL. Then the CT scan or contrast-enhanced fluoroscopy may be needed to make a definitive diagnosis in clinical practice. In addition, the Delong test showed that the diagnostic performance of the combined model was better than that of PCT alone.
The performance of the model was also verified. An AUC of 92.2% indicated good discrimination capacity. The calibration curve indicated acceptable agreement between the predicted and actual values for AL occurrence. Furthermore, the decision curve revealed that when the threshold probability was between 0.13 and 0.84, screening strategies based on our nomogram AL risk estimates resulted in superior net benefit as compared with screen-none or screen-all strategies.
This study had several limitations. First, we constructed a diagnostic nomogram based on a retrospective review of medical records. Secondly, our analysis only included single-center data. Third, external validation in different subsets of patients with AL is yet to be performed. Therefore, more prospective studies are required to confirm these results. However, to the best of our knowledge, this is the first study to establish a diagnostic nomogram to investigate the clinical value of post-operative PCT combined with CRP and WBC for predicting the occurrence of AL after laparoscopic colorectal cancer surgery. Hence, the study findings have implication for clinical practice.
Conclusions
In conclusion, our study suggests that PCT measured on POD 3 may have clinical value in predicting AL after laparoscopic colorectal cancer surgery. Furthermore, a nomogram model including PCT, CRP, WBC, ASA grade and pre-operative comorbidities might further improve diagnostic accuracy, and could be considered for adoption in clinical practice once validated in further clinical research.
Footnotes
Authors' Contributions
Conceptualization: Zhang, Tao. Data curation: L. Yang. Resources: P. Yang. Writing—original draft: L. Yang. Writing—review and editing: Zhang, Tao.
Funding acquisition: Zhang, Tao. Project administration: Zhang, Tao. Supervision: Zhang. Formal analysis: W. Yang, Du, Liu. Methodology: Huang, Lv. Validation: Tao. Visualization: Tao.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding Information
This study was supported by the National Natural Science Foundation of China (No. 82072736 and 81702386).
Author Disclosure Statement
All authors have no conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.