
Abstract
Background:
Appropriate antimicrobial therapy for the management of intra-abdominal infection (IAI) continues to evolve based on available literature. The Study to Optimize Peritoneal Infection Therapy (STOP-IT) trial provided evidence to support four days of antibiotic agents in IAI post-source control but excluded patients with a planned re-laparotomy. This study aimed to determine the short- and long-term recurrent infection risk in this population.
Patients and Methods:
This is a single-center, retrospective, observational study of adult patients admitted to a quaternary medical center between January 1, 2016, and August 1, 2022, with IAI requiring planned laparotomy. Patients were designated as receiving five or less days of antibiotic agents (short course) or more than five days (long course) after source control. The primary outcome was IAI recurrence within 30 days.
Results:
Of the 104 patients who met inclusion criteria, 78 were included in analysis. Average age was 57 ± 13.3 years, 56% were male, 94% Caucasian, with a mean Acute Physiology and Chronic Health Evaluation (APACHE) II score of 17 ± 7.09. All other baseline characteristics and clinical severity markers were similar between the two groups. Regarding the primary outcome of IAI recurrence, there was no difference when comparing those who received short course versus those who received long course therapy (41.2% vs. 44.4%; p = 0.781). No differences were found between groups with respect to secondary outcomes.
Conclusions:
In patients admitted with IAI managed with planned re-laparotomy those who received short course antimicrobial therapy were not found to have an increase in IAI recurrence compared to those with longer courses of therapy.
Intra-abdominal infection (IAI) is a leading cause of sepsis and a common cause of morbidity and mortality worldwide.1–3 Complicated IAI results from disruption of the gastrointestinal tract and leads to inflammation of the peritoneum and subsequent sepsis, with reported mortality rates ranging from 7% to 40%.1,4–6 Despite the diverse pathophysiologic processes causing these infections, basic components of management remain the same including resuscitation of patients with systemic inflammatory response syndrome (SIRS), obtaining source control, and administration of antimicrobial therapy to eradicate residual pathogens.5,7,8
Antimicrobial therapy for the management of IAI continues to evolve based on published literature.5, 8 The Study to Optimize Peritoneal Infection Therapy (STOP-IT) trial was published in 2015 comparing two strategies guiding the duration of antimicrobial therapy for the management of IAI. 9 In this study, patients were randomly assigned to receive either short course antimicrobial therapy for four ± one calendar days or antimicrobial agents until two ± one calendar days after clinical resolution of infection, up to a maximum of 10 days. 9 The primary composite end point of surgical site infection, recurrent IAI, or death was not different between the two treatment groups. 9 Based on these results, a fixed four-day course of antimicrobial therapy after source control provides similar outcomes to those who receive longer antimicrobial therapy courses. 9
In light of the STOP-IT trial publication in 2015, the Surgical Infection Society revised their Guideline on the Management of Intra-Abdominal Infection, recommending that antimicrobial therapy be limited to four days in patients who have had adequate source control.5, 8 Additionally, the joint global guideline for the clinical management of patients with IAI states that in the setting of complicated IAI, a short course of antibiotic therapy after adequate source control is a reasonable option. 4
Although STOP-IT provided literature suggesting the adequacy of short course antimicrobial therapy after source control, there were several populations excluded, specifically patients requiring a planned re-laparotomy. 9 This technique has been used for damage control surgery in trauma, vascular, transplant, and acute care surgery. 10 For acute care surgery patients, this technique is being used in the setting of severe shock, planned “second look,” and staged anastomosis/reconstruction in decompensating or unstable patients. 10 Given the practice of re-laparotomy for patients with IAI, there is a need for data to guide clinical management including antimicrobial duration in this population. 5
The purpose of this study was to evaluate the short- and long-term recurrent infection risk in patients admitted for IAI requiring planned re-laparotomy. The primary outcome was IAI recurrence within 30 days, with additional long-term outcome assessment of re-admission for procedural intervention within 90 days.
Patients and Methods
Patient identification
This study was a retrospective chart review of patients with IAI admitted to a single institution from January 1, 2016, through August 1, 2022. Patients were identified by International Classification of Diseases, Ninth Revision (ICD-9), International Classification of Diseases, Tenth Revision (ICD-10) codes, and Current Procedural Terminology (CPT) codes for exploratory laparotomy. Patients aged 18 years or older were included if they required an exploratory laparotomy for damage control surgery for IAI with a second planned laparotomy within 72 hours and received antibiotic agents for IAI at the time of the index procedure. Intra-abdominal infection was verified by at least two independent reviewers to ensure presence of peritoneal contamination. The presence of infection was determined through review of operative notes and identifying documentation of “abscess,” “purulence,” “diffuse peritonitis,” “infectious material,” and other similar dictations.
Patients with ischemia leading to bowel necrosis alone were excluded. Patients were also excluded if they were found to have a necrotizing soft tissue infection that extended into the abdominal wall or peritoneal cavity or had retained foreign materials in the abdominal cavity such as vascular endografts, as antibiotic and surgical management would follow other pre-defined infection-related treatment pathways. Furthermore, patients were excluded if they were transferred from an outside hospital after receiving procedural intervention, a trauma patient or had IAI due to trauma, died within 72 hours of admission, had a perforated gastrointestinal ulcer that was treated within 24 hours of symptom onset, or died prior to achieving source control.
Data collection
This study was approved by the local Institutional Review Board and granted a waiver of the need for informed consent. Data were obtained from the electronic medical record with the utilization of our institution's Center for Clinical and Translational Science. Variables collected included baseline demographics (Table 1), surgical course, clinical course including antimicrobial administration, organ of origin, days before definitive abdominal closure, as well as clinical outcomes including hospital and intensive care unit (ICU) mortality, hospital length of stay (LOS), ICU LOS, total days receiving antibiotic agents, microbiologic cultures, and index operation duration for each eligible patient. Antibiotic days were defined as each day that a patient received one or more antimicrobial agents.
Baseline Characteristics of Patients, According to Study Group a
Abx = antibiotic; BMI = body mass index; ICU = intensive care unit; IA = intra-abdominal; WBC = white blood count; GCS = Glasgow Coma Scale; APACHE II = Acute Physiology and Chronic Health Evaluation; COPD = chronic obstructive pulmonary disease; NOCC = no chronic complications; WTCC = with chronic complications; OR = operating room; Spp = species; AIDS = acquired immune deficiency syndrome; HIV = human immunodeficiency virus; MRSA = methicillin-resistant Staphylococcus aureus.
Non-normally distributed values reported as median (interquartile range, IQR); normally distributed values reported as mean (standard deviation, SD) and categorical values reported as n (%); p: comparing groups using Mann-Whitney U test for ordinal or non-normally distributed continuous data, Fisher exact test for binary data, and χ 2 for categorical data.
Other includes: Alistipes finegoldii, Acinetobacter radio, Bacteroides fragilis, Stenotrophomonas maltophilia, Corynebacterium species, Klebsiella pneumoniae, Citrobacter koseri, Serratia marcescens, Staphylococcus pettenkoferi, Staphylococcus hominis, Staphylococcus epidermidis, Enterococcus faecalis, Streptococcus pyogenes, Coagulase negative Staphylococcus, Ruminococcus gnavus, Lactobacillus gasseri, Lactobacillus rhamnosus, Enterobacter cloacae, Enterobacter aerogenes, Staphylococcus aureus, methicillin resistant Staphylococcus aureus, Pseudomonas aeruginosa.
Other includes: Bacteroides fragilis, Morganella morganii, Enterobacter aerogenes, Parabacteroides distasonis, Proteus mirabilis, Candida krusei, Enterobacter cloacae, Proteus vulgaris, Citrobacter youngae, Candida dubliniensis, Staphylococcus hominis, Aeromonas hydrophila, Staphylococcus epidermidis, Citrobacter freundii, Fusobacterium mortiferum, Escherichia vulneris
Other includes: liver, biliary tract, appendix, more than one source of perforation
The primary outcome was IAI recurrence rates between patients who received five days or less of antibiotic agents after source control achievement compared with those who received more than five days of antibiotic agents. Infection recurrence was defined as any unexpected surgical intervention or re-initiation of antibiotic agents for IAI within 30 days of source control attainment. Secondary outcomes included re-admission within 90 days from source control for procedural intervention associated with the original identified IAI, surgical site infection, inpatient hospital mortality, ICU mortality, hospital LOS, ICU LOS, Clostridioides difficile infection rates, and total antibiotic days for IAI. Surgical site infection was defined as infection that occurred within 30 days of source control that appeared to be related to the index operative procedure, including purulent drainage, organisms isolated from cultures, abscess formation found on direct examination, imaging or re-operation, or confirmed by a surgeon.
Source control was defined as the intervention that stopped ongoing contamination of the peritoneal cavity with removal of any infectious contents and was confirmed by research team review, which included our institutional surgeon investigator, post-graduate year one (PGY-1) pharmacy resident, as well as three acute care surgery clinical pharmacists. Although all included patients had a planned re-laparotomy, the source control date for each patient was determined based on the procedural intervention that may have been the index procedure or a subsequent laparotomy.
Statistical analysis
Values were reported as median with interquartile range (IQR), mean with standard deviation (SD), or counts with percentages unless otherwise stated. Categorical data were analyzed using Pearson χ 2 or Fisher exact test as appropriate. Continuous data were analyzed using independent samples t-test or Mann-Whitney U test as appropriate. SPSS Statistics, version 28 (IBM Corp, Armonk, NY) was utilized for all analysis and an α level of 0.05 was designated for statistical significance.
Results
Overall, 285 patients were identified, of whom 110 were excluded given their exploratory laparotomy was not for IAI (Fig. 1). Additionally, 43 patients did not have an exploratory laparotomy during their admission, 17 did not have a planned re-laparotomy, and 11 patients only had a single laparotomy procedure. A total of 78 patients with IAI and planned re-laparotomy were classified into two groups based on the duration of antibiotic agents received from the date of source control achievement: 51 patients received five or less days and 27 patients received more than five days.
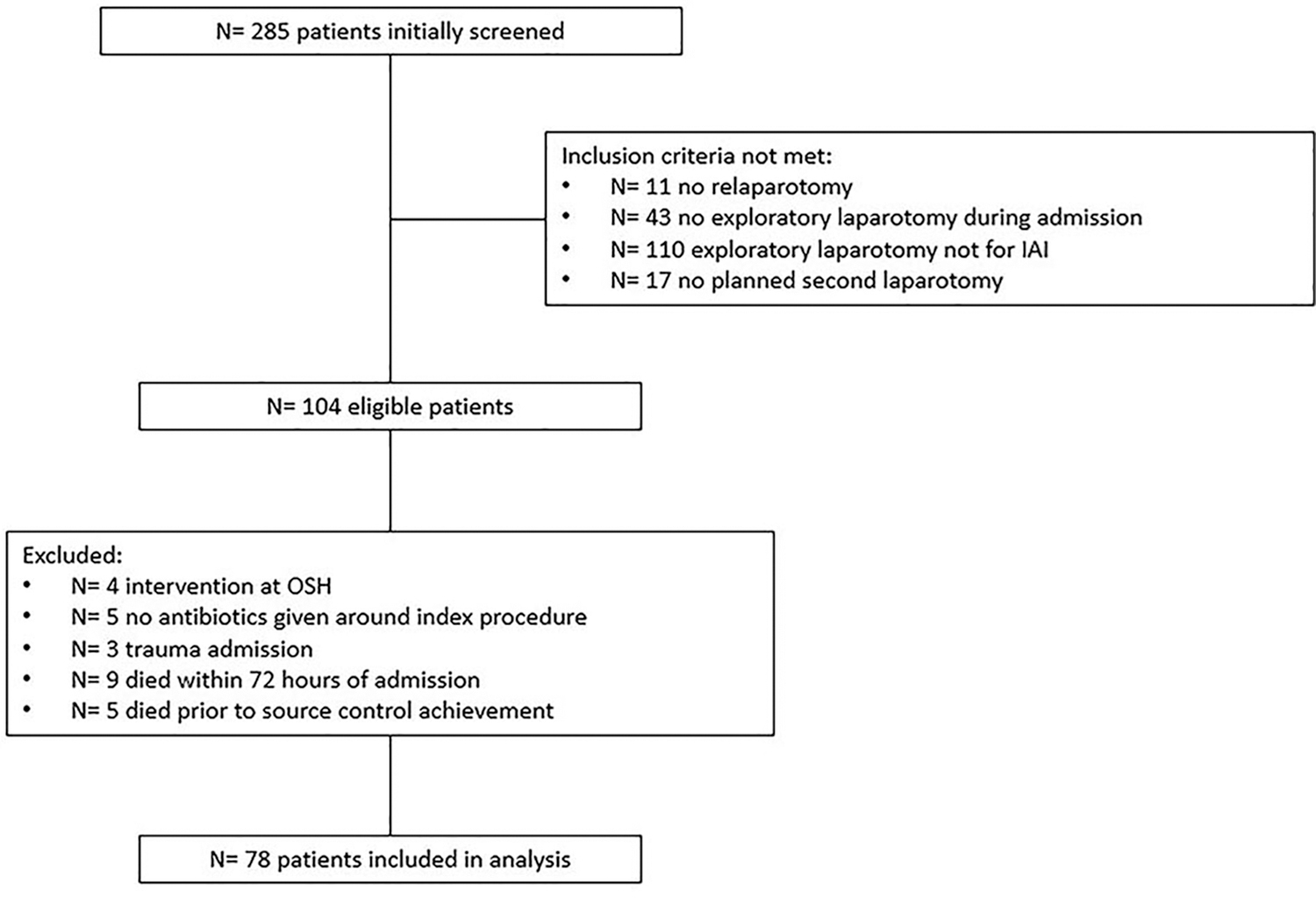
Patient eligibility flowchart. IAI = intra-abdominal infection; OSH = outside hospital.
Of the 78 patients included, baseline demographics were similar between the two groups (Table 1). The two groups were also comparable based on clinical scoring tools, with similar Charlson Comorbidity Index, Acute Physiology and Chronic Health Evaluation (APACHE) II, and Sequential Organ Failure Assessment (SOFA) scores (Table 1). The median number of days before definitive abdominal closure was numerically different between groups, but was not statistically or clinically significant (2 vs. 3 days; p = 0.127). Organ of origin was not statistically different between groups and did not impact the rate of IAI recurrence (Table 1). The rate of recurrent intra-abdominal infection within 30 days of source control was not statistically different between the two groups (41.2% vs. 44.4%; p = 0.781; Table 2).
Primary and Secondary Outcomes a
Abx = antibiotic; ICU = intensive care unit; LOS = length of stay; IAI = intra-abdominal infection.
Non-normally distributed values reported as median (interquartile range, IQR); normally distributed values reported as mean (standard deviation, SD) and categorical values reported as n (%); p: comparing groups using Mann-Whitney U test for ordinal or non-normally distributed continuous data, Fisher exact test for binary data, and χ 2 for categorical data.
In terms of secondary outcomes, there was no difference between the groups for re-admission for procedural intervention within 90 days (25.5% vs. 14.8%; p = 0.390) or surgical site infection (41.2% vs. 44.4%; p = 0.781; Table 2). Hospital and ICU mortality rates were also similar between the two groups (13.7% vs. 22.2%; p = 0.338) and (7.8% vs. 11.1%; p = 0.688) respectively. Median hospital LOS was not statistically different between the two groups (15.8 [10.8–34.5] vs. 23.9 [15.4–33.9] days; p = 0.229), however, patients who received short course antibiotic therapy did have significantly shorter ICU LOS compared with those who received longer course therapy (6.5 [3.2–10.8] vs. 11.4 [4.9–18.0] days; p = 0.038; Table 2). Clostridioides difficile infection only occurred in one patient (Table 2). Additionally, the total duration of antibiotic agents for IAI was longer in the group that received longer durations of therapy compared with those who received short course (5 [5.0–7.0] vs. 10 [7.0–14.0] days; p < 0.001).
Two of the 78 patients (7.6%) had a documented carbapenem-resistant organism. Enterococcus was isolated in 15 of the 78 patients (19.2%), with only one of those being documented vancomycin-resistant Enterococcus (VRE). There were five patients (6.4%) with an extended spectrum β-lactamase (ESBL) isolated that likely contributed to IAI. Of those five patients, one also had ESBL-positive blood culture. A Pseudomonas species was isolated in five patients as a possible source of IAI; one patient also had positive blood cultures. Methicillin-resistant Staphylococcus aureus (MRSA) was isolated in four patients with IAI (5%).
Discussion
The present study found that there was no difference in outcomes for short and long courses of antimicrobial therapy for patients with IAI requiring a planned re-laparotomy. To our knowledge, these findings are the first to evaluate the efficacy of short-course antimicrobial therapy in this population. The findings pair nicely with the known outcomes of the STOP-IT trial and are encouraging and support the rationale that proper obtainment of source control is absolutely essential in the management of patients with IAI. After the publication of this trial in 2015, antibiotic prescribing practices shifted to favor a shorter course of antibiotic agents for patients managed with exploratory laparotomy for IAI. 9
Although STOP-IT provided more definitive guidance for complex surgical patients with variability in overall management and infectious risks, it did not clarify an appropriate antibiotic duration for those requiring multiple laparotomies and specifically patients with an open abdomen requiring further exploration, since it limited inclusion to patients with a singular operation. 9 Implementation of shorter durations of antibiotics has increased although uncertainty has remained for patients requiring damage control surgery utilizing planned relaparotomy. It has been established that independent risk factors for the development of surgical site infections include open surgical approach, emergency operation, and prolonged operative duration.11,12
In conducting this study, consideration was taken that the target population was more high risk when compared with patients included in STOP-IT and the authors acknowledged the potential for the findings to vary from their results. The rate of recurrent IAI was greater than 40% in both groups of our study, with the majority being abscess formation identified on repeat imaging or re-operation. Not surprisingly, the overall average rate of both surgical site infection and intra-abdominal recurrence were substantially higher in our study compared to patients in STOP-IT, with 42.3 % versus 7.7% and 42.3% versus 14.6% respectively. 9
Additionally, our study population had a higher average APACHE II score compared with STOP-IT (17 vs. 10), as well as an overall higher mortality rate (17% vs. 1%) because of more complex surgical requirements. 9 Overall median Charlson comorbidity index score of five correlates with substantial disease burden and roughly 21% 10-year mortality, without considering the acute surgical needs during hospitalization. 13 The higher mortality rate observed in the current study is certainly linked to the surgical needs, however, it is also likely that the higher patient severity of illness is directly contributing to these rates. In the current study, patients who received long-course antibiotic therapy did have numerically higher rates of both hospital and ICU mortality, although not statistically significant. It is unknown if this directly correlates with antibiotic therapy or is associated with the development of surgical site infection, recurrence, or delay in source control attainment.
Diaz et al. 10 evaluated the effect of antibiotic duration in acute care surgery patients with IAI managed with open versus closed abdomen. One of few pieces of literature evaluating this population identified that the overall mortality rate was higher among those managed with planned re-laparotomy who also had higher SOFA (4.7) and APACHE II scores (16.1). 10 The mortality in these patients aligns with the mortality rate observed in the current study, as well as the patients having similarly high SOFA and APACHE II scores. Diaz et al. 10 ultimately found that planned re-laparotomy patients had higher rates of surgical site infection and increased mortality. Longer durations of antibiotic agents were associated with increased rates of surgical site infection and did not improve overall clinical outcomes. Recognizing the similarly high-risk, severely ill patients in the current study, the findings further support the use of short-course antibiotic agents in those managed with planned re-laparotomy. In the present study, given the difference in total days of antibiotic agents between the two groups, but similarly high rates of infection recurrence, neither shortening or prolonging antibiotic duration impacts these clinical outcomes, even in patients requiring multiple laparotomies.
A strength of this study is that it aimed to address the current gap in literature evaluating outcomes in a particularly under investigated high-risk surgical patient population. Additionally, this study was conducted at a large academic medical center that serves as a regional tertiary and quaternary referral center, lending itself to high rates of regional referrals and high acuity patients. The medically complex and geographically diverse patient population captured in this study enhances the applicability of our findings to other comparable institutions and surgical referral sites. Further enhancing the generalizability of our findings, our study not only included a diverse patient population but also included a variety of surgical practices, specifically regarding procedures in which any intervention that appropriately led to source control as defined by the authors (i.e., repair of perforation, resection of perforation, primary re-anastomosis, etc.) were included.
The majority of this study's outcomes and methods were specifically chosen to emulate the design and intent of the STOP-IT trial to allow our data and findings to be applied in a similar manner. 9 Last, utilization of a multidisciplinary team composed of infectious diseases clinical pharmacists, acute care surgery clinical pharmacists, PGY-1 pharmacy resident, and an acute care surgeon adds to the credibility of source control determination, and to the overall approach of this study to optimize patient care and implement change to enhance clinical practice.
As with any study, there are inherent limitations. First, it was retrospective in nature, limiting aspects of data collection and some factors were presumed from documentation. Source control determination was one of the factors determined solely on review and assessment of operative notes, as well as interpretation of surgeon decisions. To mitigate the potential variability and inconsistencies with individual reviewer determination of source control, the authors of this study opted to review all included patients as a research team consisting of three acute care surgery clinical pharmacists, a PGY-1 pharmacy resident, and an institutional surgeon investigator, who was able to provide expertise regarding nuanced interpretation of operative findings and rationale for additional planned procedures. This approach standardized source control determination and allowed the research team to identify any additional confounders for patient outcomes that had not already been identified.
Surgeon variability was another limitation to our study. At our institution, acute care surgery services operate as a cohesive physician group. Multiple surgeons were involved in the care of these patients and there was a lack of standardization for procedural techniques, length of procedures, and planned re-operations. Despite this, with established institution specific protocols for this patient population, and considering these procedures were performed solely at our institution, there was presumed to be some inherent similarities in surgical standards for exploratory laparotomy cases and indications for planned second laparotomy.
Additionally, given our high regional referrals, most patients included were transferred from an outside hospital for surgical intervention at our institution. The authors specifically chose to allow transfers to represent our typical patient population accurately, which is likely consistent with other similar institutions. Recognizing this, there is potential that we did not account for the true total duration of antibiotic therapy that may have been initiated at another institution. However, source control is a requirement of proper IAI treatment and procedural intervention only occurred at the study institution.
Patients were excluded if they were transferred from an outside hospital after procedural intervention because external records could not be obtained accurately for these patients, and there was predicted to be variability in surgical interpretation and decision making from outside institutions likely impacting clinical outcomes. Furthermore, many patients had concomitant infections, particularly bacteremia, that required prolonged antibiotic durations, and may have impacted the rates of infectious outcomes. To minimize this potential confounder, the authors evaluated each of these cases to differentiate the antibiotic regimens and indication to denote when IAI treatment ended, but another agent may have been continued for alternate sources of infection. In these cases, we were unable to confirm if IAI was the cause of concomitant bacteremia for a proportion of our patient population. Upon reviewing the patient's medical record and culture data, educated inferences could be made. However, it was not always clear based on isolated organisms and would be an end point for further evaluation.
Last, given the diverse patient population, surgeon variability, and retrospective nature of this study, we did not account for the method of source control in our analysis. Rates of complications potentially differ based on the method in which source control was obtained and any unexpected procedure and technique-related complications (i.e., anastomotic leaks, improper drain placement) that may have affected the duration of antibiotic agents that were prescribed. Although these are important considerations, our study demonstrates that regardless of surgical approach and patient-specific factors, antibiotic duration may not directly correlate with infectious outcomes.
Conclusions
In this study, patients with IAI requiring a planned re-laparotomy who were treated with short-course (≤5 days) antibiotic agents after source control had similar recurrent infection rates compared with those who received longer durations (>5 days) after source control. A reduced ICU LOS was also noted in the short-course cohort. These findings suggest that longer durations of antimicrobial agents may not confer any additional clinical benefit in this high-risk surgical patient population. Future randomized controlled trials would be valuable in determining the validity of our findings and ability to implement changes in clinical practice.
Footnotes
Authors' Contributions
Conceptualization: Hochstetler, Parli, Olney, Bishop, Warriner, VanHoose, Mynatt, Ali. Data curation: Bishop, Olney, Parli, Ali, Mynatt, VanHoose, Warriner, Hochstetler. Formal analysis: Schadler. Funding acquisition: Hochstetler. Investigation: Hochstetler, Parli, Olney, Bishop, Warriner, VanHoose, Mynatt, Ali. Methodology: Hochstetler, Parli, Olney, Bishop, Warriner, VanHoose, Mynatt, Ali. Project administration: Hochstetler.
Resources: Hochstetler, Parli, Olney, Bishop, Warriner, VanHoose, Mynatt, Ali.
Software: Schadler. Supervision: Parli, Olney, Bishop, Warriner, VanHoose, Mynatt, Ali. Validation: Hochstetler, Parli, Olney, Bishop, Warriner, VanHoose, Mynatt, Ali. Writing—original draft: Hochstetler. Writing—review and editing: Hochstetler, Parli, Olney, Bishop, Warriner, VanHoose, Mynatt, Ali.
Funding Information
The project described was supported by the National Institutes of Health (NIH) National Center for Advancing Translational Sciences through grant number UL1TR001998. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author Disclosure Statement
No competing financial interests exist.