
Abstract
Background:
Candida species account for approximately 15% of hospital-associated infections, causing fatal consequences, especially in critically ill patients. This study aimed to evaluate invasive candidiasis (IC) risk factors in critically ill patients undergoing surgery.
Patients and Methods:
We retrospectively reviewed the medical records of 583 patients who underwent emergency surgery for complicated intra-abdominal infections between January 2016 and December 2021. Patients were divided into two groups according to the presence or absence of IC during their hospital stay. IC was defined as culture-proven candidemia and intra-abdominal candidiasis.
Results:
This study included 373 patients for the final analysis, of whom 320 were discharged without IC (IC absent group) and 53 presented with IC (IC present group) during their hospital stay. The IC present group showed a higher in-hospital mortality rate (35.8 vs. 8.8%; p < 0.001), with 66.0% of the patients diagnosed within 10 days, whereas only 6.5% were diagnosed beyond 20 days after admission. Stomach (odds ratio [OR], 4.188; 95% confidence interval [CI], 1.204–14.561; p = 0.024) and duodenum (OR, 7.595; 95% CI, 1.934–29.832; p = 0.004) as infection origin, higher Acute Physiology and Chronic Health Evaluation II (APACHE II) score (OR, 1.097; 95% CI, 1.044–1.152; p < 0.001), and lower initial systolic blood pressure (OR, 0.983; 95% CI, 0.968–0.997; p = 0.018) were risk factors of IC after emergency gastrointestinal surgery.
Conclusions:
Patients who had stomach and duodenum as infection origin, higher APACHE II scores, and lower initial systolic blood pressure had a higher risk of developing IC during their hospital stay after emergency gastrointestinal surgery. Prophylactic antifungal agents can be carefully considered for critically ill patients with these features.
Fungal infections account for approximately 15% of hospital-acquired infections. 1 Specifically, invasive candidiasis (IC) is a group of conditions, including candidemia, deep-seated candidiasis, and deep-seated candidiasis with associated candidemia, impacting mortality and morbidity rates in critically ill patients. 2 Despite the widespread use of antifungal agents, previous studies have shown that the mortality rates in the intensive care unit (ICU) for candidemia and intra-abdominal candidiasis (IAC) are still high, with a range of 38% to 42.6% and 25% to 60%, respectively.3–6
Intra-abdominal candidiasis often occurs comorbid with peritonitis and intra-abdominal abscesses, with approximately 40% of patients experiencing gastrointestinal perforation, necrotizing pancreatitis, and repeated abdominal surgeries, predisposing them to high-risk IC and life-threatening consequences. 3 Therefore, awareness, prompt diagnosis, and appropriate antifungal therapy remain essential for IC treatment. However, the low sensitivity and specificity of diagnostic tests can make accurate and early detection challenging, leading to potential delays in appropriate treatment. 7
Candida albicans remains a major causative strain of IC. However, recent studies have reported increased strains, such as Candida glabrata, showing resistance to traditional antifungal agents such as fluconazole. 6 Furthermore, multinational or multicenter studies have demonstrated variations in the types and resistance patterns of Candida strains based on the hospital's size, location, and time frame. 8 Therefore, understanding the characteristics of IC cases treated in different regions and hospitals and accumulating data on antifungal resistance patterns are critical for effective infection management.
The existing studies on IC based on domestic ICUs are limited. Therefore, this study aimed to analyze IC characteristics and risk factors in patients admitted to the ICU after emergency gastrointestinal surgery in a single tertiary hospital in South Korea. Additionally, this research aimed to identify risk factors contributing to adverse outcomes in patients and provide helpful information for appropriate prophylactic antifungal therapy.
Patients and Methods
The retrospective, single-center study enrolled adult patients aged 18 years and older who were admitted through the emergency department, underwent emergency gastrointestinal surgery, and were subsequently admitted to the ICU between January 2016 and December 2021. Of the 583 patients who met the inclusion criteria, 210 with an ICU stay of longer than 24 hours, patients who had trauma, and those without complicated intra-abdominal infection (cIAI) were excluded, leaving a total of 373 patients. These 373 patients included in the final analysis were divided into two groups based on the presence or absence of IC during their hospitalization (Fig. 1).
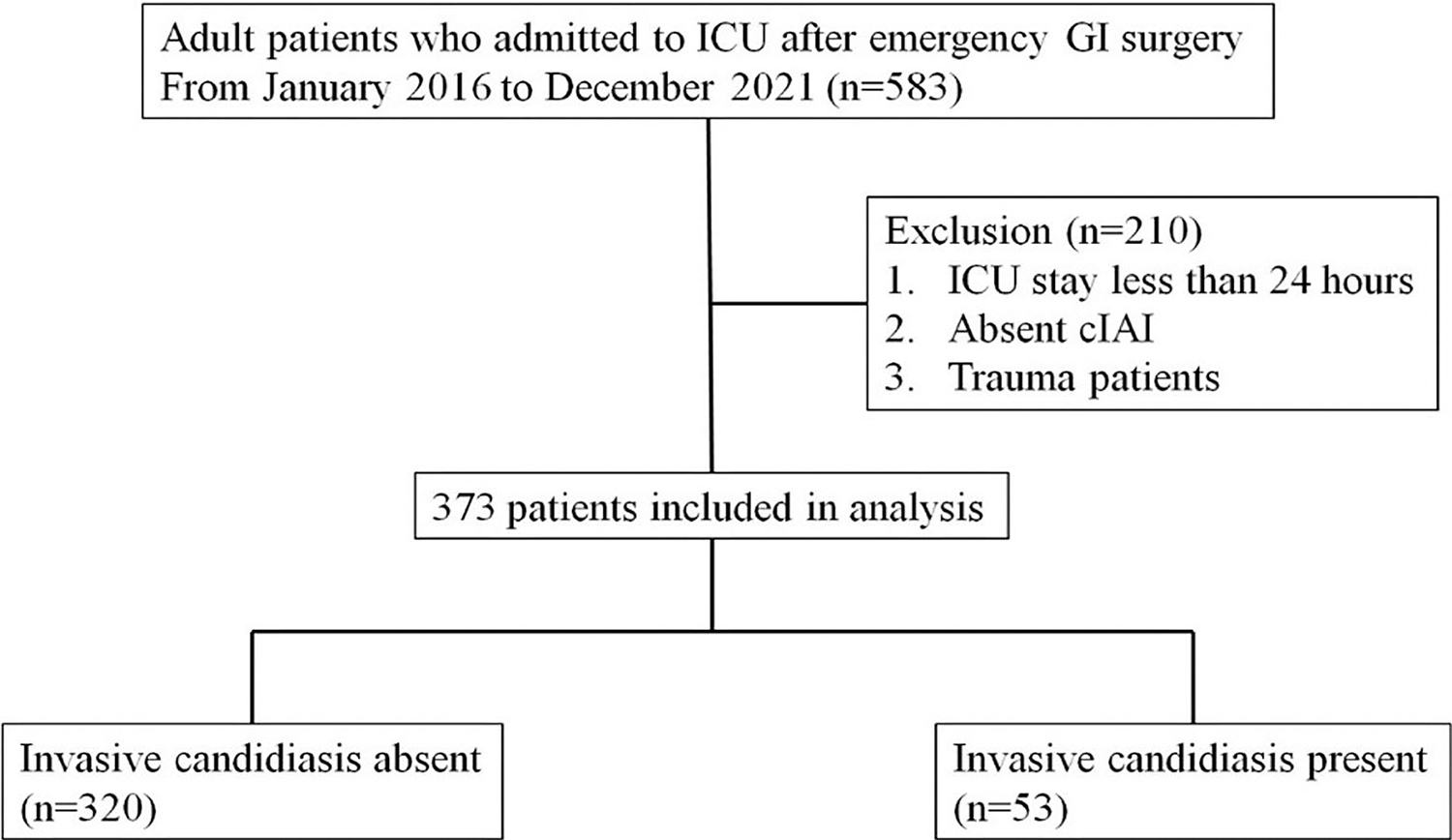
Flow diagram of patient selection. ICU = intensive care unit; GI = gastrointestinal; cIAI = complicated intra-abdominal infection.
Invasive candidiasis was defined as a positive culture for candida in blood or intra-abdominal fluid during hospitalization. Critically ill patients admitted to the ICU underwent culture tests every three to four days. In cases in which cIAI was treated surgically, intra-abdominal fluid were also cultured.
Various patient information, including essential patient characteristics such as age, gender, and underlying conditions (hypertension, heart failure, arrhythmia, diabetes mellitus, chronic kidney disease, liver disease, steroid use, respiratory disease, neurologic disorders, bedridden status) were obtained through retrospective review of electronic medical records. Additionally, disease severity was assessed using scores like Sequential Organ Failure Assessment (SOFA), quick Sequential Organ Failure Assessment (qSOFA), Nutrition Risk in the Critically Ill, and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores. Information regarding the patient's vital signs at admission to the emergency department, mental status at presentation, and the use of vasopressors within 24 hours was also collected. Furthermore, initial blood test results, length of hospital stay, ICU admission duration, duration of mechanical ventilation, in-hospital mortality, mortality within 30 days of discharge, blood and intra-abdominal fluid culture results, date of positive culture if candida was cultured, the occurrence of urinary tract infection, and pneumonia during hospitalization were also recorded.
All statistical values were assessed for normality using the Shapiro-Wilk test. Based on the results, normally distributed data were expressed as mean ± standard deviation or as median (first quartile, third quartile). Ratios were presented as n (%). The Student t-test was used to compare normally distributed variables, whereas the Mann-Whitney U test was used for variables that did not follow a normal distribution. The χ 2 test was used for comparing ratios, and if the Fisher exact test was required, the results were displayed accordingly.
Survival analysis for the two groups divided according to the presence of IC was conducted using Kaplan-Meier survival curves, and the comparison between the two groups was performed using the log-rank test. Multivariable regression analysis was conducted using the maximum likelihood method and backward stepwise selection to determine risk factors for IC. SPSS Statistics, version 28 (IBM Corp, Armonk, NY) was used for all statistical analyses in this study, and the level of statistical significance was set at p < 0.05.
This study was conducted as a retrospective review of medical records and received approval from our institution's Institutional Review Board (2023-01-003).
Results
Baseline characteristics
There were no differences in underlying conditions and infection mechanisms between the IC absent and IC present groups, except for respiratory diseases (8.1% vs. 17.0%; p = 0.025). However, differences were observed in the primary organs of infection within the gastrointestinal tract, excluding the colon (32.8% vs. 24.5%; p = 0.230) and rectum (43.1% vs. 39.6%; p = 0.633). The IC absent group showed a higher proportion of appendicitis or cholecystitis (15.3% vs. 3.8%; p = 0.028), whereas the IC present group had a higher proportion of stomach (26.4% vs. 10.9%; p = 0.002) and duodenum (15.1% vs. 5.0%; p = 0.006) involvement (Table 1).
Baseline Characteristics
IC = invasive candidiasis; HTN = hypertension; HF = heart failure; DM = diabetes mellitus; CRF = chronic renal failure; GI = gastrointestinal; GB = gallbladder.
Results from Mann-Whitney test.
Results from Fisher exact test.
Scores reflecting the initial disease severity of the patients and initial clinical variables
The scores reflecting the initial disease severity of the patients were all higher in the IC present group compared with the IC absent group. Specifically, the APACHE II score (29 [20.5, 36] vs. 20 [14, 29]; p < 0.001), qSOFA score (1 [0.5, 2] vs. 0 [0, 1]; p < 0.001), and SOFA score (5 [3.5–8] vs. 4 [2–6]; p < 0.001) were higher in the IC present group. Regarding the initial vital signs, only the initial body temperature (36.8 [36.15–37.2] vs. 36.8 [36.2–37.4] °C; p = 0.607) did not show any difference between the two groups. However, the IC present group had lower initial systolic blood pressure (106 [83–121] vs. 119.5 [100–141.5] mm Hg; p < 0.001), higher respiratory rate (20 [20–24] vs. 20 [18–20] per minute; p < 0.001), and higher heart rate (103 [83.5–117.5] vs. 90 [79–109] beats per minute/min; p = 0.019). Additionally, the proportion of patients with altered consciousness (17.0% vs. 3.4%; p < 0.001) and those who received vasopressors within 24 hours of admission (64.2% vs. 26.9%; p < 0.001) and proton pump inhibitor post-operatively (64.2% vs. 38.4%; p < 0.001) were higher in the IC present group (Table 2).
Initial Disease Severity Scores and Initial Clinical Variables
IC = invasive candidiasis; APACHE II = Acute Physiology and Chronic Health Evaluation II; SOFA = Sequential Organ Failure Assessment; qSOFA = quick Sequential Organ Failure Assessment; SBP = systolic blood pressure; BT = body temperature; PPI = proton pump inhibitor.
Results from Mann-Whitney test.
Initial laboratory results
The IC present group had higher levels of procalcitonin (37.87 [7.13–78.68] vs. 8.06 [4.09–46.23] ng/mL; p = 0.026), phosphate (4.40 [3.13–5.28] vs. 3.65 [2.50–5.35] mg/dL; p = 0.005), blood urea nitrogen (37.40 [29.20–45.40] vs. 31.35 [20.18–46.40] mg/dL; p < 0.001), creatinine (1.76 [1.26–2.17] vs. 1.32 [0.88–2.19] mg/dL; p = 0.001), and international normalized ratio (1.23 [1.12–1.43] vs. 1.17 [1.08–1.42]; p = 0.042) in the initial blood tests. Contrastingly, fibrinogen (432.34 ± 32.42 vs. 513.85 ± 12.31 mg/dL; p = 0.014) was lower in the IC present group. No differences were observed between the two groups in the remaining parameters (Table 3).
Initial Laboratory Results
IC = invasive candidiasis; CRP = C-reactive protein; WBC = white blood cell; PLT = platelet; Ca = calcium; P = phosphate; BUN = blood urea nitrogen; AST = aspartate transaminase; ALT = alanine transaminase; ALP = alkaline phosphatase; INR = international normalized ratio.
Results from Mann-Whitney test.
Clinical outcomes
Patients in the IC present group had longer hospitalization periods (44 [30–80.75] vs. 26 [14–45] days; p < 0.001), ICU admission durations (21.5 [10–37] vs. 7 [4–16] days; p < 0.001), and durations of mechanical ventilation (16 [8–29] vs. 5 [2–12] days; p < 0.001). The proportion of in-hospital mortality within the admission period was also higher in the IC present group (35.8% vs. 8.8%; p < 0.001). Although not statistically significant, the proportion of mortality within 30 days after discharge was similarly higher in the IC present group (15.1% vs. 7.2%; p = 0.053; Table 4).
Clinical Outcomes
IC = invasive candidiasis; HLOS = hospital length of stay; ICU LOS = intensive care unit length of stay; MV = mechanical ventilation.
Results from Mann-Whitney test.
Kaplan-Meier survival curve
In the survival analysis performed for in-hospital mortality between the IC present and IC absent groups, the survival rate was lower in the IC present group than in the IC absent group. The log rank (Mantel-Cox) test showed a difference between the two curves (p = 0.041), indicating a statistically significant difference in survival between the two groups (Fig. F2).

Kaplan-Meier survival curve for in-hospital mortality. IC = invasive candidiasis; HLOS = hospital length of stay.
Bacterial culture results
In the culture tests, the proportion of identified bacteria was higher in the IC present group compared with the IC absent group for blood (58.5% vs. 19.7%; p < 0.001), intra-abdominal (IA) fluid (66.0% vs. 31.9%; p < 0.001), and sputum (62.3% vs. 23.8%; p < 0.001; Table 5). Among patients with Candida identified in blood or IA fluid culture, the analysis of the timing of Candida identification revealed that 66% of cases were identified within 10 days, whereas only 6.5% were identified after 19 days (Fig. 3).

Patients on each hospital day confirmed with Candida infection through blood or intra-abdominal cultures.
Bacterial Culture Results
IC = invasive candidiasis; IA = intra-abdominal; UTI = urinary tract infection.
Microorganisms isolated from both blood and IA fluid cultures were examined (Supplementary Table S1). Analysis of blood cultures revealed a predominant presence of gram-positive bacteria in both IC present and IC absent groups, with percentages of 83.9% and 65.1%, respectively. In contrast, IA fluid cultures demonstrated a more balanced distribution between gram-positive and gram-negative bacteria compared with the results obtained from blood cultures.
Antibiotic resistance profile was also examined (Supplementary Table S2). In blood cultures, the IC present group demonstrated a statistically higher incidence of resistance to carbapenem among gram-negative bacteria (60.0% vs. 8.0%; p = 0.022) compared with IC absent group. In IA fluid cultures, IC present group exhibited a higher prevalence of extended-spectrum β-lactamase (ESBL)-producing bacteria (71.4% vs. 36.8%; p = 0.033) and carbapenem resistance (50.0% vs. 14.0%; p = 0.003) compared with the IC absent group.
Analysis of risk factors
Multivariable regression analysis results, predicting the occurrence of IC, identified several risk factors. Patients with infection in the stomach (odds ratio [OR], 4.188, 95% confidence interval [CI], 1.204–14.561; p = 0.024) and duodenum (OR, 7.595, 95% CI, 1.934–29.832; p = 0.004) as the primary organs of infection were associated with a higher risk of IC. Additionally, higher APACHE II score (OR, 1.097, 95% CI, 1.044–1.152; p < 0.001) and lower initial systolic blood pressure (OR, 0.983, 95% CI, 0.968–0.997; p = 0.018) were similarly identified as factors associated with an increased risk of IC (Table 6).
Multivariable Logistic Regression Analysis of Predictors for Invasive Candidiasis
OR = odds ratio, CI = confidence interval, APACHE II = Acute Physiology and Chronic Health Evaluation II, SBP = systolic blood pressure.
Discussion
This study analysis revealed that patients who presented with IC had higher disease severity upon admission, and all clinical outcomes, including hospitalization period, ICU admission duration, mechanical ventilation duration, 30-day mortality rate, and in-hospital mortality rate, were worse. Multivarianle regression analysis showed that IC was more likely to occur in patients with infections in the upper gastrointestinal tract, higher disease severity (indicated by higher APACHE II scores), and lower initial systolic blood pressure.
Previous studies in Europe and the United States also reported higher mortality and morbidity rates in the group with IC than those without IC.1,9–11. Similarly, in the present study, the clinical outcomes were not different from those reported in previous research. The multivariable regression analysis in this study identified gastric and duodenal perforations, higher APACHE II scores, and lower initial systolic blood pressure as risk factors for IC. Studies have suggested that proton pump inhibitor (PPI) therapy creates a favorable environment in the upper gastrointestinal tract for candida colonization by removing the acidic barrier. 12 Considering that most patients with gastric and duodenal perforations included in this study had peptic ulcers, the use of PPIs and the high incidence of IC could be associated. Furthermore, APACHE II scores and initial systolic blood pressure are physiologic parameters reflecting the severity of the disease. Therefore, it is reasonable to assume that as the disease severity increases, the incidence of IC increases correspondingly.
Previous studies, including a meta-analysis, suggest immunosuppressive therapy, including steroids, as a risk factor for candidemia.10,13–15 However, this study showed no difference in steroid use between the group with IC and those without IC. It should be noted that the study population was limited to patients who underwent emergency surgery, which might have influenced the patient population. Additionally, all patients had cIAI and were severely ill, requiring treatment in the ICU for more than 24 hours. This high severity of illness among the patients may have considerably impacted the study results.
Broad-spectrum antibiotic use is one of the risk factors identified in previous studies.13,14,16 Patients undergoing emergency surgery for cIAI are all administered broad-spectrum empirical antibiotic agents. Research in mice models has shown that the administration of total parenteral nutrition (TPN) and antibiotic agents can influence the changes in gut microbiota, contributing to the proliferation induced by pathogenic microorganisms.17,18 Consequently, alterations in gut microbiota can impair gut barrier function, thereby serving as a gateway for invasive candida infections.18,19
Therefore, it is essential to consider whether prophylactic administration of antifungal agents would benefit high-risk patients with such risk factors. Some randomized controlled trials have revealed that using antifungal agents did not reduce the incidence of IC.20,21 Furthermore, research results have shown that administering antifungal agents to critically ill patients receiving mechanical ventilation without a definite diagnosis of IC did not impact the mortality rate. 22 Many cases might not have had actual Candida infection. Consequently, using antifungal agents without a confirmed diagnosis of IC, even in critically ill patients who commonly have various risk factors, may seem to provide no benefit. However, studies readily demonstrate that early administration of antifungal agents in confirmed cases of IC impacts patient outcomes.23–25 Considering the high mortality rate of IC mentioned earlier and the limitations of slow and inaccurate fungal culture tests, prophylactic antifungal therapy in patients with identified specific risk factors could improve patient prognosis.
Some studies report that the prophylactic use of fluconazole positively impacted patient outcomes in cases in which abdominal surgery was performed because of gastrointestinal perforation or anastomotic leakage.26,27 Additionally, when analyzing the culture test results, Candida was identified within 10 days in 66% of patients and within five days in 34% of patients (Fig. 3). Although factors such as prolonged hospitalization, antibiotic use, and TPN administration might influence Candida infection, this study's findings suggest that Candida can be detected early in the hospitalization period in many high-risk patients. Again, this underscores the use of prophylactic antifungal agents in such patients. However, further large-scale studies are needed to accumulate more data on the impact of prophylactic antifungal agents in high-risk patients undergoing emergency surgery for cIAI.
This study has limitations because it was a retrospective study conducted in a single institution, and the number of confirmed IC cases was limited. However, given the scarcity of domestic research analyzing IC characteristics and risk factors in critically ill patients, this study may provide valuable insights for future multicenter or prospective studies on candida infection. Moreover, presenting early risk factors for IC through multivariable analysis could serve as a reference for making decisions regarding using prophylactic antifungal agents in critical care settings.
Conclusions
This study aimed to analyze IC characteristics and risk factors in critically ill patients admitted to the ICU after emergency gastrointestinal surgery to aid in appropriate prophylactic antifungal therapy. Through multivariable analysis, the study identified upper gastrointestinal perforation, high APACHE II scores, and low initial blood pressure as risk factors for IC. Being vigilant in these patients and considering early prophylactic antifungal therapy may help improve patient outcomes.
Footnotes
Authors' Contributions
Study design: Jung, Park, Yang, Kwak. Data extraction from electronic medical records: Jung, Park. Assessment of literature: Yang, Kwak. Analysis: Jung. Figure and table design: Park, Yang, Kwak. Drafting the manuscript: Jark. All authors reviewed the manuscript.
Data Availability
Data and materials can be provided upon appropriate requests.
Funding Information
No funding was received.
Author Disclosure Statement
This study was conducted as a retrospective review of medical records and received approval from our institution's Institutional Review Board (2023-01-003). Consent to participate is waived due to the nature of the study. The authors have no conflicts of interest regarding this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.