
Abstract
Background:
Antibiotics are frequently administered prophylactically to trauma patients with various injury patterns to prevent infectious complications. Trauma patients may also require large volume resuscitation with blood products. Limited data are available to support antibiotic dosing recommendations in this population. We hypothesized that we would be able to develop a population pharmacokinetic model of cefazolin, a frequently used antibiotic in the trauma scenario, from remnant blood samples by pharmacokinetic analysis of trauma patients.
Methods:
Remnant plasma from standard of care chemistry/hematology assessments was retrieved within 48 h of collection and assayed to determine cefazolin concentrations. Population pharmacokinetic analyses were conducted in Pmetrics using R. Linear regression was conducted to assess the effect of blood product resuscitation volume on cefazolin pharmacokinetic parameters.
Results:
Cefazolin concentrations best fitted a two-compartment model (Akaike information criterion: 443.9). The mean ± standard deviation parameters were total body clearance (4.3 ± 1.9L), volume of the central compartment (Vc: 7.7 ± 6.9L), and intercompartment transfer constants (k12: 1.3 ± 0.98 h−1, k21: 0.6 ± 0.45 h−1). No statistical relationships were observed between blood products, volume of blood products, and cefazolin clearance or Vc (R2: 0.0004–0.21, p = 0.08–0.95). Using a 5,000-patient Monte Carlo simulation, 2 g with repeated dosing every 2 h until end of surgery was required to achieve 93.2% probability of 100% free time above the minimum inhibitory concentration (MIC) (fT > MIC) at the ECOFF value for Staphylococcus aureus (2 mg/L).
Conclusions:
In these 15 trauma patients receiving blood transfusion, no relationship with blood volume resuscitation and cefazolin pharmacokinetics was observed. On the basis of this pharmacokinetic model, frequent cefazolin doses are required to maintain 100% fT > MIC.
Background
Infection plays a significant role in trauma patients’ morbidity and mortality because of decreased tissue perfusion, hemorrhagic shock, mechanical contamination of the wound with foreign material, and direct contamination from visceral injury. 1 In fact, among patients that survive longer than 48 h after their initial injury, infection is responsible for the majority of deaths. 2 The prevention of sepsis in this population includes rapid treatment of hemorrhagic shock, antibiotics when indicated, and surgical control of contamination. 3
Antibiotic guidelines for trauma patients differ from one health care facility to another. However, providers at most institutions administer empirical antibiotics for complicated cases such as abdominal trauma requiring exploration, traumatic hemopneumothorax requiring tube thoracostomy, and open fractures. 4 Moreover, in a study investigating the effect of prophylactic antibiotics on the incidence of infectious complications, a short course of a first-generation cephalosporin right after traumatic injury significantly lowered the risk of infection when used in combination with other adequate orthopedic fracture and wound management interventions. 5 Like many other level 1 trauma centers, our hospital uses the first-generation cephalosporin, cefazolin, as prophylaxis and empirical treatment among patients with open fractures. Cefazolin is then often supplemented by additional antibiotics for additional Gram-negative or anaerobic coverage in the case of high-risk open fractures or bowel injury.6–8 For example, while cefazolin is used for all open fractures at our institution, tobramycin is also prescribed in the case of a grade 3 or grade 4 open fractures. In scenarios where patients have suffered more than one injury (open fracture and need for laparotomy for example), cefazolin is considered treating both. Finally, metronidazole is added for anaerobic coverage in patients undergoing laparotomy and noted to have concomitant injury to the bowel.
It is also common that many trauma patients require resuscitation with blood products to prevent death from hemorrhage. Unfortunately, little is known about the effect of transfusion volume on cefazolin pharmacokinetics (PK) in trauma patients, and therefore, the science guiding the re-dosing of antibiotics in this population is limited. A study evaluated the effect of transfusion volume on vancomycin among burn patients reported a statistically significant reduction in vancomycin concentration with greater blood volume replacement; however, they concluded the difference was not of clinical significance. 9 Several additional studies of antibiotics including ampicillin, cefotaxime, piperacillin, cefoperazone, and sulbactam have been conducted in solid organ transplant patients in which high volume of blood product transfusion is common.10–12 Although concentrations for these β-lactam antibiotics were low, the volume of blood transfusion was not available to reference, so conclusions were limited. In contrast, frequent cefazolin doses are recommended in other patient populations, such as those undergoing cardiopulmonary by-pass surgery, obese patients, and those receiving cesarean delivery.13–15
At our institution, the massive transfusion protocol is activated when the provider suspects the patient will require more than four units of blood products or two units of whole blood during the initial resuscitation. Since the goal of prophylaxis for β-lactam antibiotics such as cefazolin is to maintain free concentrations above the minimum inhibitory concentration (MIC) for 100% of the entire surgical period, 16 it is fundamental to understand how blood product transfusion affects antibiotic PK and whether different dosing regimens are required to maintain effective exposure in the trauma population. The aims of this study were first to characterize the PK of cefazolin in bleeding trauma patients and second to assess the impact of resuscitation volumes on cefazolin exposure in order to guide optimal re-dosing.
Methods
Study design and participants
This was a prospective PK study conducted at a level 1 trauma center and was approved by our Institutional Review Board. Informed consent was obtained for healthy volunteers donating fresh whole blood for initial cefazolin stability studies. For the patient component, the study was approved with an informed consent waiver because minimal protected health information was accessed and only remnant plasma samples previously collected as part of routine clinical care were retrieved from the chemistry laboratory to determine cefazolin concentrations. Eligible patient participants included adults ≥18 years of age who presented as a trauma activation in the emergency department, underwent blood product transfusion with a minimum of four units of blood products such as packed red blood cells (PRBC), fresh frozen plasma (FFP), or platelets, or two units of whole blood in the first 12 h of arrival to the hospital, and received intravenous cefazolin in the trauma bay as part of their initial treatment and workup. All patients had chemistry, hematology, or coagulation tubes collected and available for at least 48 h in the chemistry laboratory refrigerator.
Patient data and sample collection
All cefazolin doses, timing of administration, and indication for administration were recorded in real time during resuscitation and for up to 12 h after arrival. In addition, we documented the timing and type of laboratory blood draws, and amount of blood product (whole blood, PRBC, FFP, and platelets) and crystalloid (normal saline and lactated ringers) administration over the initial 12 h after arrival. Patient data such as age, gender, weight, height, serum creatinine, injury details, and presenting hemodynamics were collected from the medical record using a predeveloped data collection tool. Each patient’s course was followed to determine time of surgery and/or procedure for hemorrhage control and/or control of contamination, additional cefazolin doses, blood products, and fluid during surgery. Upon identification of an eligible trauma patient, remnant plasma samples in lithium heparin or ethylenediaminetetraacetic acid (EDTA) vacutainers were collected from the chemistry laboratory refrigerator, recentrifuged at 4500 rpm for 3 min, and then transferred to cryovials for storage at −80° C fridge until analyses.
Cefazolin recovery from remnant plasma
Before the initiation of the patient study, stability studies were conducted to validate the optimal methodology for recovery of cefazolin from remnant blood samples. Approximately 450 mL of fresh whole blood was collected from adult healthy volunteers on the days of the experiment. The volume of the fresh whole blood was measured and then inoculated with cefazolin (Sagent Pharmaceuticals, Schaumburg, IL, lot#2019E0) to achieve a plasma concentration of 100 µg/mL. The inoculated whole blood was then evenly split between vacutainers containing lithium heparin or EDTA, used clinically for chemistry and hematology assessments, respectively. Vacutainers were immersed in a water bath at 37° C for 10 min. To document the 0 h starting concentration, one vacutainer of each type was centrifuged to collect plasma for initial cefazolin concentrations. Vacutainers were then processed and stored as per standard of care in the chemistry laboratory. Sampling continued after 6 h at room temperature and then at 6, 12, 24, and 48 h when stored in the refrigerator. All experiments were conducted in triplicate for each of two healthy volunteers. The accepted threshold for cefazolin recovery was ≥ 90%.
Analytical procedures
Concentration of cefazolin in plasma from the recovery studies and the patient samples was determined using a validated high-performance liquid chromatography assay. 17 The assay used cefaclor as internal standard and had a lower limit of detection of 0.5 µg/mL. Mean interday coefficients of variance for low and high values of cefazolin were 4.4% and 4.4% in lithium heparin plasma samples. For EDTA plasma samples, these values were 5.7% and 4.9%, respectively.
Pharmacokinetic analyses
Cefazolin concentrations were fitted to one- or two-compartment models using the nonparametric adaptive grid algorithm in the Pmetrics package (Laboratory of Applied Pharmacokinetics, Los Angeles, CA) for R. A multiplicative assay variance model was determined by fitting a polynomial to the plot of the interday assay standard deviation versus the measured cefazolin concentrations, respectively, generating the following formulas: Standard deviation (SD) = γ × (0.05 + 0.15 × C), where C is cefazolin concentration, and γ represents all environmental variability excluding the assay. Final model selection was determined on the basis of the Akaike information criterion (AIC) value, visual inspection of the observed versus predicted plots, and assessment of PK parameter estimates for each participant. After selection of a base model, linear regression (SigmaPlot Version 14, Systat Software, San Jose, CA) was applied to determine relationships between PK parameters and patient creatinine clearance, body weight, and volume resuscitation administered. Volume resuscitation was analyzed several ways including total volume received over initial 12 h (all blood products + crystalloid), only blood products, only crystalloid, and then by individual components of blood products (whole blood, PRBC, and FFP).
Monte carlo simulation
Monte Carlo simulation was conducted for cefazolin in Pmetrics. The population PK estimates from the final model were recapitulated in 5000 simulated patients receiving the following doses cefazolin: 1000 mg once, 2000 mg once, 2000 mg q3h, and 2000 mg q2h as an intravenous 3-min bolus injection. Cefazolin concentrations were simulated over 8 h, and the approximate total duration during which the majority of the resuscitation fluid was received and surgery concluded for these patients. The probability of target attainment (PTA) was calculated on the basis of the free cefazolin concentration remaining above the epidemiological cutoff (ECOFF) for Staphylococcus aureus (2 mg/L) for 100% over this 8 hour interval from the European Committee on Antimicrobial Susceptibility Testing website. 18 The PTA over the MIC distribution for Escherichia coli (ECOFF = 4 mg/L) was also evaluated. Free time above the MIC (fT > MIC) of 100% was targeted as this exposure is the recommended goal for antimicrobial prophylaxis. 16 Cefazolin protein binding was assumed to be 90% during all simulations. 19 For comparison, a separate Monte Carlo simulation was conducted using PK parameters collected from healthy adult volunteers. 17 Variability around parameter estimates in the healthy volunteers was inflated during the simulation to a coefficient of variation of 30% on the basis of observations from infected patients. 19
Results
Patient characteristics
Fifteen eligible trauma patients were included from January 2022 until August 2022. All participants were male and generally younger (10/15 were <50 yrs of age) with normal body weights and kidney function (Table 1). Patients were admitted for motor vehicle accidents (n = 10), gunshot/stabbing injuries (n = 4), and self-inflicted injury (n = 1). All patients underwent a surgery and/or procedure for hemorrhage control and/or control of contamination within the first 12 h. Four patients underwent more than one procedure during this time frame. All patients received whole blood and PRBC. Many also received crystalloid (n = 12) and FFP (n = 12), with fewer receiving platelets (n = 7). All patients met at least one criteria for cefazolin administration. All cefazolin doses were administered by IV bolus (1–2 g) over approximately 3 min at varying intervals over the initial 24 h.
Characteristics for the 15 Trauma Patients Receiving Blood Product Resuscitation and Cefazolin
BMI, body mass index; CrCL, creatinine clearance; SD, standard deviation.
Number of cefazolin doses received over 12 h after arrival.
Cefazolin recovery from remnant plasma
Initial cefazolin plasma concentrations in lithium heparin and EDTA vacutainers tubes during healthy volunteer recovery studies were 99.7 ± 3.9 µg/mL and 100.7 ± 4.1 µg/mL. Recovery studies demonstrated that cefazolin could be recovered adequately from lithium heparin vacutainers if done so within 48 h following collection and recovered from EDTA tubes if done so within 24 h following collection (Fig. 1.). This shorter window in EDTA vacutainers was because of recovery in one of the healthy volunteers that declined below 90% after 24 h, so samples from EDTA were restricted to those available and processed within this time after collection.
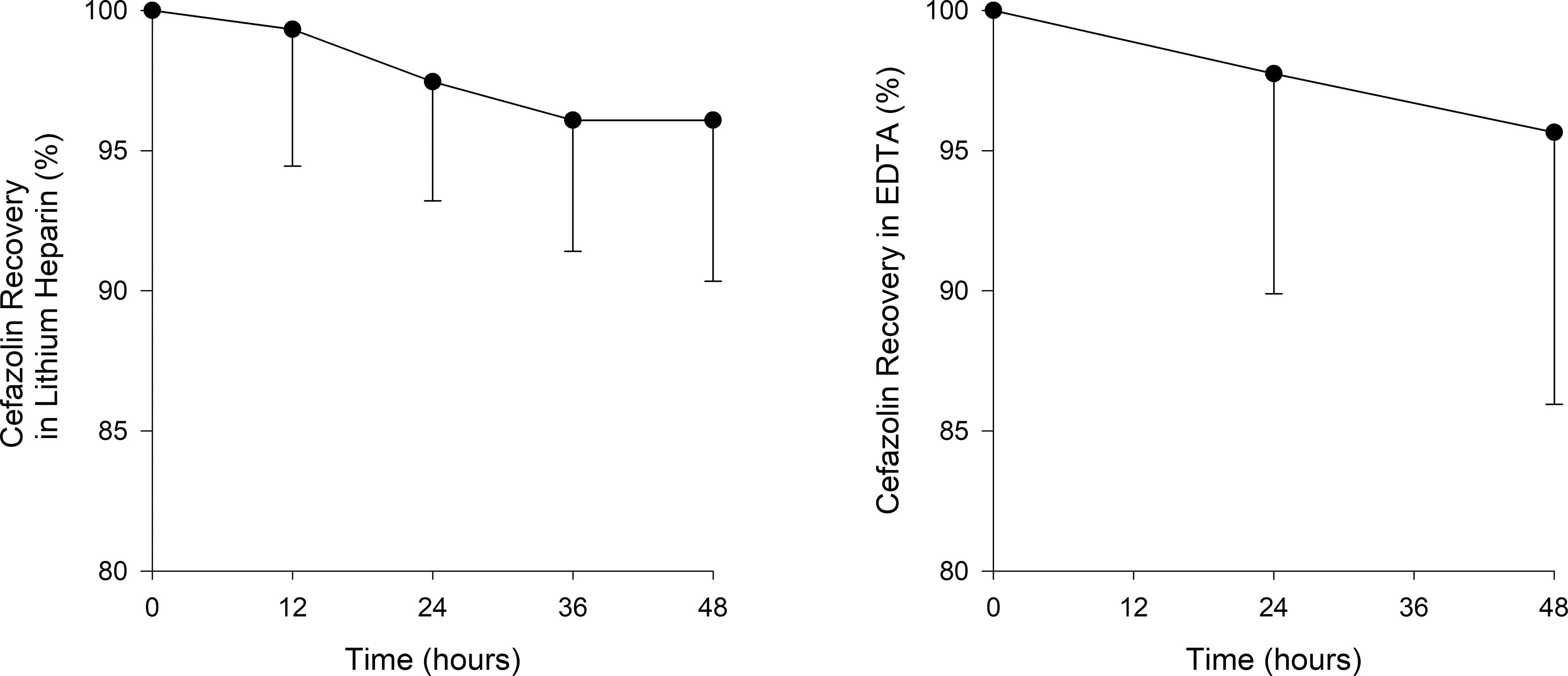
Mean ± standard deviation recovery of cefazolin from plasma collected in lithium heparin (left) and EDTA (right) vacutainers from two healthy volunteers over 48 h. EDTA, ethylenediaminetetraacetic acid.
Analytical procedures
Linear regression was performed to assess relationships between total volume resuscitation, blood product resuscitation, crystalloid alone and individual components of blood product administration and cefazolin total body clearance (CL), and volume of the central compartment (Vc). There was no statically significant relationship between cefazolin PK parameters and resuscitation volumes received (Table 2, Supplementary Fig. S2). As a result, these volumes were not incorporated into the final population PK model.
Coefficient of Determination (R2) and p-Value from Linear Regressions of Cefazolin Pharmacokinetic Parameters with Resuscitation Volumes Patients Received
FFP, fresh frozen plasma; PRBC, packed red blood cells.
All includes blood products (whole blood, packed red blood cells, and fresh-frozen plasma) plus crystalloid.
Blood products only includes whole blood, packed red blood cells, and fresh-frozen plasma.
Pharmacokinetic analysis
A total of 71 remnant plasma samples were available for cefazolin concentration determination. Patients contributed a mean of 4 (range: 2–6) plasma samples. Plasma concentrations ranged from 1.65 to 426.23 µg/mL. The sampling time and concentration related to the last cefazolin dose received are provided in Supplementary Figure S1, demonstrating good dispersion of time points and concentrations over an 8-h interval. A two-compartment model fitted the data better than a one-compartment model (AIC: 443.9 vs. 485.3). Patient demographics such as body weight and CrCL did not improve AIC from the base model. Final cefazolin PK parameters from the base model are presented in Table 3. Shrinkage was acceptable for all parameters with values between 1.71 and 8.38. The population predicted versus observed and MAP-Bayesian individual predicted versus observed plots demonstrated excellent fits (Fig. 2). γ for the final model was 1.21.

Observed versus population-predicted (left) and MAP-Bayesian individual predicted (right) cefazolin concentrations for the final two-compartment base model.
Final Cefazolin Population Pharmacokinetic Parameters from 15 Trauma Patients Receiving Blood Product Resuscitation
CL, total body clearance; Vc, volume of central compartment; k12, intercompartment transfer constant; k21, intercompartment transfer constant; SD, standard deviation.
Monte Carlo simulation
PTAs for various simulated cefazolin dosing regimens are compared with between the trauma patients receiving resuscitation and the healthy volunteer population in Table 4. Trauma patients undergoing resuscitation had numerically higher PTAs at lower doses compared with the healthy volunteers. Frequent (q2h) cefazolin doses of 2 g were required to achieve >90% PTA over the initial 8 h for at the ECOFF of 2 mg/L (Table 4, Fig. 3).

Comparative PTA between trauma patients receiving blood resuscitation and healthy volunteers for a cefazolin 2 g q2h regimen over the MIC distribution of cefazolin against 19,252S. aureus and 381E. coli isolates (bar graphs). MIC, minimum inhibitory concentration; PTA, probability of target attainment.
Comparison of PTA Values between Trauma Patients Receiving Blood Product Resuscitation Versus Healthy Volunteers
MIC, minimum inhibitory concentration; PTA, probability of target attainment.
All cefazolin dosing regimens simulated as an intravenous bolus over 3 min.
Pharmacodynamic target was 100% fT>MIC over an 8-h interval.
Discussion
The goal of an effective antimicrobial prophylaxis regimen is to provide exposure above that necessary to prevent infection from open wounds and surgical interventions caused by the most common targeted bacterial pathogens. This requires optimization of antibiotic dosage and timing combined with consideration of MICs for the most likely pathogens, and finally, host-related factors that could further influence exposure. 7 Although trauma patients may require the administration of blood products to prevent death from hemorrhage, the number of PRBC units administered during surgery is also acknowledged as an infection risk factor. 20 Moreover, bleeding and blood product transfusion further increase frequency of infection and sepsis among trauma patients.21,22 The current antimicrobial surgical prophylaxis guidelines recommend re-dosing of antibiotics in patients with excessive blood loss (i.e., >1,500 mL) during surgery. 7 Unfortunately, robust studies to guide re-dosing of antibiotics in the bleeding trauma patient who is receiving blood product resuscitation are not available. 23 The Eastern Association for the Surgery of Trauma (EAST) clinical practice guidelines provide Level 3 recommendations to increase antibiotic dosing 2-3x in the trauma patients suffering penetrating abdominal trauma with hemorrhagic shock and repeat dosing after transfusion of every 10 units of blood until there is no further blood loss. 24 This guidance considers vasoconstriction in the hemorrhagic shock patient and decreased tissue perfusion, as well as potential for hemodilution, but is largely on the basis of a single study with amikacin. 25 To the best of our knowledge, there are no studies prospectively evaluating antibiotic PK among trauma patients undergoing resuscitation. In this study, we described the PK of cefazolin in trauma patients in hemorrhagic shock and further explored the influence of resuscitation product administration volumes on cefazolin exposure to guide optimal dosing.
Cefazolin concentrations in these 15 male trauma patients undergoing blood product resuscitation were best described by a two-compartment PK model. The final population PK model had low shrinkage values for all parameter estimates, indicating robust individual predictions for these patients. Notably, the observed total body clearance (4.34 L/h) was similar to that reported in male healthy volunteers (3.7–4.8 L/h). 17 This was not surprising given all of the included trauma patients were young males with relatively normal kidney function and body weight on arrival. Clearance estimates were also similar to 16 adult patients receiving cefazolin surgical prophylaxis during cardiopulmonary bypass surgery, where observed clearance was 3.23 L/h for an average patient with a CrCL of ∼81 mL/min. 13 However, their observed volume of the central compartment was lower (3L) compared with with our trauma population (7L), which may be because of cardiopulmonary bypass surgery itself, or other factors present in that patient population (e.g., hypoalbuminemia and peripheral vascular disease).
Importantly, there were no significant relationships identified between the blood product or crystalloid resuscitation volumes and cefazolin clearance or Vc estimates (Table 2, Supplementary Fig. S2). Fluid volumes administered were analyzed in totality as well as split up among the various components. We hypothesized that whole blood or fresh-frozen plasma columns, as opposed to PRBC or platelets, might provide better correlation with cefazolin PK parameter estimates because this β-lactam does not have significant intracellular penetration and has high protein binding. Therefore, it should only be present in plasma before its distribution into tissues. Of note, fresh whole blood resuscitation did provide a p-value of 0.08 with an R2 of 0.21 with total body clearance; however, this appeared to be because of the influence of a single patient with the highest clearance value (Supplementary Fig. S2). Swoboda and colleagues 26 evaluated cefazolin concentrations in relation to blood loss in 11 patients undergoing elective spinal instrumentation surgery; they reported a negative correlation between plasma concentration and volume of blood loss at 60 min. The investigators did not track timing of blood loss and only cumulative blood loss which would track with lower concentrations over the duration of surgery, as opposed to cefazolin clearance or volume of distribution. An earlier study determining effects of blood product transfusion on ampicillin/sulbactam fT > MIC and area under the curve exposure in liver transplant patients also found no relationship with blood product resuscitation volume. 27 The liver transplant patients received on average 10,667 mL of blood product transfusion compared with the 5,013 mL received in these 15 trauma patients. Despite the high resuscitation volumes and wide range of volumes in both studies, these data collectively suggest little influence of blood product resuscitation on β-lactam plasma exposure.
These observations from human studies agree with studies conducted in animals. In 1987, Dickson and colleagues used dogs to determine if hemorrhagic shock and fluid resuscitation alter the PK of cefazolin. 28 Overall, dramatic differences in the cefazolin concentration–time profiles pre- versus post-shock/resuscitation were not observed. However, subtle, nonsignificant increases in volume of distribution were observed with saline resuscitation (14%) and whole blood resuscitation (43%), suggesting increases of extracellular fluid volume after shock of short-time frame and proper resuscitation. In contrast, Brothers and colleagues used a rabbit hemorrhagic shock model to observe increases in cefazolin clearance from peritoneal adipose and iliac artery tissue with greater blood volume removal versus that of control rabbits. 29 Serum half-life did not differ between control animals and those resuscitated with whole blood, while those resuscitated with lactated ringers did experience shorter serum half-lives. This latter study suggests that although plasma (or serum) concentrations may not differ substantially, exposure in tissue may be affected. Further studies assessing the impact of blood product resuscitation on tissue concentrations are needed.
Despite the lack of observed influence of blood product resuscitation on cefazolin plasma PK, low overall cefazolin fT > MIC exposures were observed in this trauma population, thus requiring aggressive dosing to maintain plasma exposures above 100% fT > MIC for the ECOFF of S. aureus (2 mg/L). A dosing regimen of 2 g administered every 2 h should maintain high likelihood of 100% fT > 2 mg/L until blood loss has been controlled (e.g., the end of surgery). Of note, this frequent administration is a result of the desire to maintain free drug concentrations above the MIC for the entire surgical period, or in the case of this study, the entire time at risk for infection. Lower fT > MIC cephalosporin exposures (i.e., 50–70% fT > MIC) have been targeted for treatment of a range of infections and might require less frequent dosing to achieve; however, data specific to cefazolin remain limited. The PTA was similar for this regimen between simulated trauma patients and simulated healthy volunteers, again suggesting that blood product resuscitation does not substantially influence plasma PK. Our observations of low PTA also agree with the cefazolin PK study in cardiopulmonary bypass surgery patients, where a 2 g q2h regimen was also required to maintain 100% fT > MIC for S. aureus. 13 Importantly, PTA for even this aggressive dosing regimen was only ∼50% (Fig. 3) at the ECOFF for E.coli (4 mg/L), and this regimen would provide 100% fT > MIC for ∼80% of E. coli isolates worldwide (see MIC distribution in Fig. 3). Should local epidemiology predict higher E. coli cefazolin MICs or require greater Gram-negative coverage for surgical prophylaxis, addition or substitution with an agent having greater Gram-negative activity should be considered.
Strengths of this study include the preanalytical determination of cefazolin stability in lithium heparin and EDTA vacutainers, thereby permitting robust collection from standard of care samples and the use of population PK methods that can manage sparse sample analyses. These methods could be replicated in larger studies to evaluate PK in patient populations that are otherwise nearly impossible to consent. Limitations include the small sample numbers and the surprising homogeneity of this trauma population. Larger studies with more variable patient demographics including gender, body weight, and acute renal function are warranted to further evaluate the influences of blood product resuscitation on cefazolin PK. In addition, this pilot study did not focus solely on patients who underwent massive transfusion. Instead, we were somewhat more inclusive and chose to study patients who underwent at least four units of blood within the first 12 h. Next, protein binding was not measured in these patients, and a fixed value of 90% was applied during Monte Carlo simulation. Lower protein binding may be observed in critically ill patients, therefore permitting similar fT > MIC exposure with less frequent dosing regimens. Finally, only plasma exposure was evaluated from these remnant samples, so our conclusions should not be extrapolated to changes in tissue concentrations.
In summary, no impact of blood product or crystalloid resuscitation was observed in these 15 trauma patients receiving blood product resuscitation, thereby suggesting re-dosing on the basis of blood loss or administration is unnecessary. Monte Carlo simulations suggest a minimum cefazolin dose of 2 g q2h until blood loss is controlled or end of the surgical procedure will maintain 100% fT > MIC at relevant MICs. This dosing regimen should be evaluated in further clinical trials that also include patient outcomes.
Footnotes
Acknowledgments
The authors acknowledge Christina Sutherland of the Center for Anti-Infective Research and Development for assistance with study coordination and analytical support. The authors would also like to thank the Hartford Hospital Division of Acute Care Surgery physician assistants, Megan Reynolds and Ashley Weisse, for their assistance with data collection. In addition, the authors would like to acknowledge members of the Chemistry Laboratory and the team at Center for Anti-Infective Research and Development, Hartford Hospital for their assistance and valuable input.
Authors’ Contributions
All authors contributed equally in literature search, study design, data collection, data analysis, data interpretation, writing, and critical revision.
Author Disclosure Statement
No author has any disclosures or financial interests.
Funding Information
This study was funded by a grant from the Hartford Hospital Medical Staff with in-kind support from the Center for Anti-Infective Research and Development.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.