
Abstract
Background:
This study aims to elucidate the clinical characteristics of Shewanella-related surgical site infections (SSIs) and assess the risk of mortality in patients by establishing a predictive model.
Patients and Methods:
A retrospective analysis of medical history and laboratory data of Shewanella-related SSI patients over the past decade was conducted via the electronic medical record (EMR) system. A predictive model for mortality risk in Shewanella-related SSI patients was established using plasma interleukin-6 (IL-6) levels combined with the Howell-PIRO scoring system.
Results:
Over the past 10 years, 45 strains of Shewanella were isolated from specimens such as bile, drainage fluid, and whole blood in patients with digestive tract SSIs. Among them, 21 of 45 (46.67%) patients underwent malignant tumor resection of the digestive system, 14 of 45 (31.11%) underwent endoscopic retrograde cholangiopancreatography (ERCP) common bile duct exploration or the stone removal, and seven of 45 (15.56%) were trauma repair patients with fractures and abdominal injuries. Among the 45 Shewanella-related SSI patients, 10 died within 30 days of infection, six cases involved infections with more than two other types of bacteria. The combined use of IL-6 and Howell-PIRO scores for mortality risk assessment yielded an receiver operating characteristic (ROC) curve with an area under the curve (AUC) of 0.9350, a positive predictive value of 92.71%, a negative predictive value of 94.58%, a diagnostic sensitivity of 95.35%, and a diagnostic specificity of 92.14%—all higher than the model using IL-6 or Howell-PIRO scores alone.
Conclusions:
We found that residents in coastal areas faced an increased risk of Shewanella-related SSI. Moreover, the higher the number of concurrent microbial infections occurring alongside Shewanella-related SSI, the greater the mortality rate among patients. The combined application of plasma IL-6 levels and the Howell-PIRO scoring system is beneficial for assessing patient mortality risk and guiding timely and proactive clinical interventions.
Surgical site infection (SSI) is a common health-care–associated infection, occurring at the limited surgical incision site or even spreading to adjacent deep tissues. Because of the abundance of micro-organisms, patients undergoing digestive tract surgeries had higher risk of developing SSIs compared with those undergoing other procedures. Data from the National Healthcare Safety Network (NHSN) in the United States revealed that up to 10% of SSIs occurred after biliary, hepatic, or pancreatic surgeries, approximately 5% after colon surgeries, and approximately 0.7% after gallbladder surgeries. 1 For a long time, common pathogens regarding post-operative SSIs in the digestive tract included Escherichia coli, Proteus, and Klebsiella from the Enterobacteriaceae family, followed by Enterococcus, Streptococcus, and Anaerobic. 2 With advances in clinical microbiology techniques, uncommon pathogens have been isolated and identified from SSI patients, and the Shewanella genus is one such example.
The Shewanella genus is a globally distributed microbe with facultative anaerobic, motile, gram-negative rods, and is part of the microbial community in marine environments. First described by Derby and Hammer in 1931, 3 clinical infections caused by Shewanella species started to be reported globally decades later.4,5 Among the 62 recognized species of Shewanella, Shewanella putrefaciens, Shewanella haliotis, and Shewanella algae are considered closely associated with human infections, with clinical infections most commonly attributed to Shewanella algae. 6 Initially cases were often reported in tropical and temperate coastal regions.7,8 Most cases involved skin and soft tissue infections resulting from contact with seawater after mucosal or skin damage, as well as Shewanella septicemia after the consumption of raw seafood. Other cases included infections of the hepatobiliary system and the ears.9,10
Our research has identified a growing number of patients with Shewanella-related SSIs, many of whom lacked the contact history with seawater or seafood. Therefore, we propose that this bacterium may be a human colonizer. However, existing literature primarily consists of case reports, and current research has yet to provide sufficient evidence to fully substantiate this viewpoint. To clarify the relation between this bacterium and the host, as well as to understand its significance and prognostic factors in SSIs, we conducted a retrospective analysis of cases over a 10-year period in our hospital.
Patients and Methods
This study collected the clinical information of patients who had isolated Shewanella species between September 2013 and May 2023 via the electronic medical record (EMR) system. This hospital is one of the top healthcare organizations in local with 2.7 million outpatient amount and exceeding 107,000 surgical cases annually. The clinical data of the first isolation with this bacterium were included in the study, and all isolations of the same strain from the same patient within the following 30 days were considered as part of the same event.
The definition of SSI used in this study is as follows: a surgery-related infection occurring in the surgical incision or adjacent site within 30 days post-operatively, with an extension to 90 days post-operatively if there is implantation of artificial materials during the procedure. Mixed infection refers to the isolation of pathogens other than Shewanella species from the same patient or site after excluding exogenous contaminating bacteria. The hospital SSI incidence rate was 4.2%.
If Shewanella species are isolated from a sterile site or as a single isolate from another site, it is defined as definite pathogen. If Shewanella species are isolated from an infected site along with multiple other micro-organisms, it is defined as probable pathogen. If there are no apparent signs or symptoms of infection at the isolation site, it is defined as colonization pathogen.
Microbiology
The identification of strains is based on gram staining and colony morphology, achieved through standard biochemical reaction experiments and commercial identification systems. During the study, because of updates in instruments and methods, we used the VITEK system (bioMérieux, Marcy l'Etoile, France) and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) for the identification of Shewanella species separately. If the selected methods are insufficient to differentiate strains to the species level reliably, they are reported directly to the Shewanella genus. Antibiotic susceptibility testing is conducted using the disc diffusion method, and interpretation is done according to the standards of the Clinical and Laboratory Standards Institute (CLSI) for “Other Non-Enterobacteriaceae,” categorizing strains as resistant (R), intermediate (I), or susceptible (S). If a strain shows resistance to three or more drug categories simultaneously, it is considered a multi-drug–resistant strain.
Prognostic assessment
Interleukin-6 (IL-6) is a sensitive indicator that can reflect the infection. The Howell-PIRO scoring system covers most factors related to the occurrence and development of severe infections, including body response, organ dysfunction, underlying diseases, and malignancies. These factors are relatively easy to obtain and are ideal for predicting patient prognosis, so we try to use plasma IL-6 combined with the Howell-PIRO model to evaluate patients' risk of mortality. Receiver operating characteristic (ROC) curves are constructed for comparing sensitivity, specificity, positive predictive value, and negative predictive value, respectively. Statistical significance is determined if p < 0.05. Statistical analysis is performed using GraphPad Prism 9 software (GraphPad Software, San Diego, CA, USA).
Results
Patient characteristics
Over the course of 10 years, a total of 45 strains of Shewanella were isolated from patients with SSI in our hospital. The incidence rate of Shewanella-related SSIs is 0.14%. The male-to-female ratio among patients was 3.6:1, with ages ranging from 42 to 88 years (median age, 66 years). Among the patients, 21 of 45 (46.67%) underwent malignant tumor resection, 14 of 45 (31.11%) underwent endoscopic retrograde cholangiopancreatography (ERCP) common bile duct exploration or the stone removal, and seven of 45 (15.56%) were trauma repair patients with fractures and abdominal injuries. Except for three patients with gallstones who consumed fully cooked seafood in the week before admission, the remaining patients had no history of contact with seawater or seafood. Ten of 45 SSI patients (22.22%) died within 30 days of infection, including eight cases with malignant tumors, one case with facial burns, and one case with abdominal trauma (Table 1). Among the 10 deceased patients, one case involved infections with three other types of bacteria, four cases involved infections with two other types, and two cases involved infections with one other type.
Patient Basic Information and Clinical Characteristics
“Days of infection” in the table refers to the time when patients developed post-operative infections.
“Median days of infection” indicates the average number of days after surgery infections occurred.
The notation “(10/45)” indicates that 10 patients died due to Shewanella-related surgical site infections of the total 45 patients who experienced such infections.
Microbiology
Among the 45 isolated strains, 32 of 45 (71.11%) were identified as Shewanella putrefaciens, and 13 of 45 (28.89%) as Shewanella algae. Among these, 15 of 45 (33.33%) were single isolates, considered as definite pathogens. The majority, 30 of 45 (66.67%), exhibited mixed infections, with one case having infections from three other bacterial species and five cases having infections from two other species. Among the isolates from mixed infections, Escherichia coli was isolated in 10 strains, Klebsiella oxytoca in five strains, Enterobacter cloacae in three strains, Staphylococcus aureus in three strains, Citrobacter freundii in three strains, Enterococcus faecalis in two strains, Pseudomonas aeruginosa in two strains, Proteus mirabilis in two strains, and single strains of Clostridium perfringens, Morganella morganii, Corynebacterium striatum, Pseudomonas fluorescens, Enterobacter gergoviae, Candida tropicalis, Klebsiella pneumoniae, and Enterobacter aerogenes (Table 2).
Information on Isolated Strains
Regarding specimen sources, 16 of 45 (35.56%) were from bile, 12 of 45 (26.67%) from blood, 9 of 45 (20.00%) from secretions and purulent fluid, and 8 of 45 (17.77%) from drainage fluid.
Drug sensitivity testing
Antibiotic susceptibility testing results (Table 3) indicate that overall, the highest resistance rate is observed with amoxicillin-clavulanic acid at 12 of 45 (26.67%), followed by cefoperazone-sulbactam at 10 of 45 (22.22%), ciprofloxacin at nine of 45 (20.00%), and cefotaxime at nine of 45 (20.00%). Among Shewanella putrefaciens, the highest resistance rate is seen with ciprofloxacin at nine of 32 (28.13%), followed by amoxicillin-clavulanic acid at six of 32 (18.75%) and cefoperazone-sulbactam at five of 32 (15.63%). In Shewanella algae, the highest resistance rate is observed with amoxicillin-clavulanic acid at six of 13 (46.15%), followed by cefoperazone-sulbactam at five of 13 (38.46%) and amikacin at three of 13 (23.08%). Additionally, for ciprofloxacin, cefepime, gentamicin, and levofloxacin, the resistance rate of Shewanella putrefaciens is higher than that of Shewanella algae. Both strains show relatively high intermediate sensitivity to piperacillin-tazobactam.
Antimicrobial Susceptibility Test Results for Forty-Five Cases of Shewanella Species
In this study, a total of 10 multi-drug-resistant Shewanella strains were identified, with one strain resistant to nine antibiotic agents, six strains resistant to six antibiotic agents, one strain resistant to five antibiotic agents, and two strains resistant to four antibiotic agents. Among patients with multi-drug-resistant Shewanella isolates, six cases had malignant tumors, and four of them died after antibiotic therapy. No multi-drug-resistant strains were found among other isolates from mixed infections.
Plasma IL-6 and Howell-PIRO model combined assessment of patient mortality risk
Among the 45 Shewanella-associated SSI patients, 10 died within 30 days of infection, all of whom were male. The plasma IL-6 levels and Howell-PIRO scores in the death group were higher than those in the survival group, and the differences were statistically significant (Table 4). There was no significant difference in age between the two groups (Table 5).
Howell-PIRO Model Evaluation System
COPD = chronic obstructive pulmonary disease; BUN = blood urea nitrogen; SBP = systolic blood pressure.
Basic Information, IL-6 Levels and Howell-PIRO Scores in the Survival and Death Group
IL-6 = interleukin-6.
The ROC curve analysis (Fig. 1) shows that when solely using the Howell-PIRO score for patient mortality risk assessment, the area under the curve (AUC) is 0.8751, with a positive predictive value of 79.31%, negative predictive value of 78.38%, diagnostic sensitivity of 74.19%, and diagnostic specificity of 82.86%. When solely using IL-6 to assess patient mortality risk, the AUC is 0.8269, with a positive predictive value of 83.33%, negative predictive value of 66.67%, diagnostic sensitivity of 86.15%, and diagnostic specificity of 74.31%. When using IL-6 and Howell-PIRO scores in combination to assess patient mortality risk, the AUC is 0.9350, with a positive predictive value of 92.71%, negative predictive value of 94.58%, diagnostic sensitivity of 93.35%, and diagnostic specificity of 92.14% (Table 6).
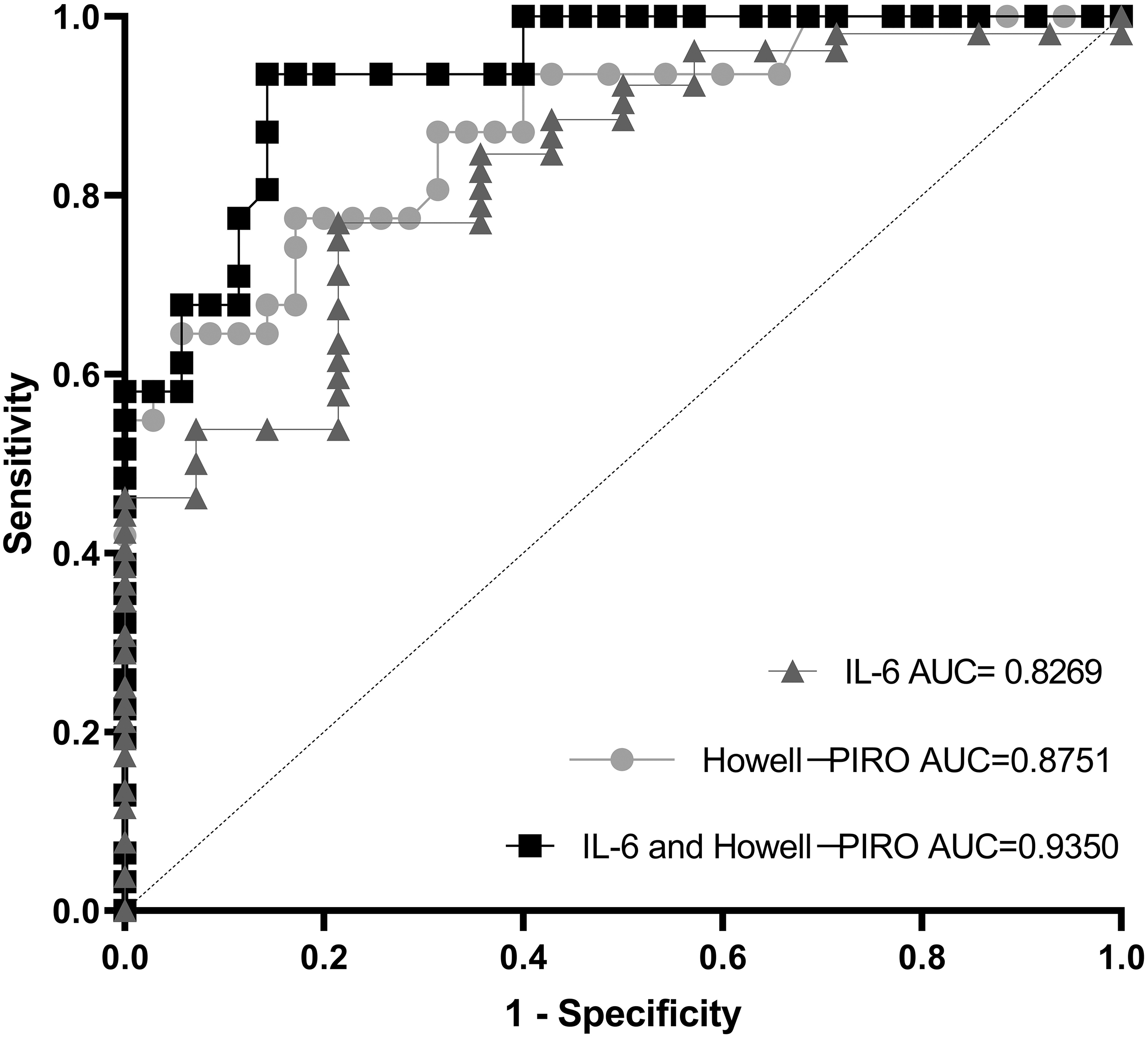
Receiver operating characteristic (ROC) curve for evaluating patient prognosis with the combined use of plasma interleukin- 6 (IL-6) and Howell-PIRO.
Evaluation of Patient Prognosis With the Combined Use of Plasma IL-6 Levels and Howell-PIRO Scores
IL-6 = interleukin-6; AUC = area under the curve; CI = confidence interval.
Discussion
Surgical site infection is the most common and costliest health-care–associated infection, accounting for 38% of hospital infections. 11 In the United States, at least one in 24 hospitalized surgical patients experienced one post-operative SSI. 12 Despite the promotion and widespread adoption of techniques such as laparoscopy, hand hygiene, incision protection, and prophylactic antibiotic treatment, which have reduced the incidence of SSI by approximately 50%, post-operative SSIs in gastrointestinal surgeries remain at a high-risk level. In this study, patients with Shewanella-related SSI underwent various surgeries, including ERCP, bile duct exploration, esophageal cancer radical surgery, gastric cancer radical surgery, and colorectal cancer radical surgery. Although these surgeries fall into the category of clean-contaminated wounds, and patients received pre-operative prophylactic antibiotic treatment, SSI still occurred post-operatively. This suggests that the current use of prophylactic antibiotic agents may not provide adequate coverage for potential pathogens.
The Shewanella genus is a common micro-organism in marine environments, and contact with seawater is a recognized a risk factor for related infections. Although the genus was discovered more than 70 years ago, clinical infection reports related to Shewanella primarily focus on skin and soft tissue infections and bacteremia.13,14 Research on Shewanella-related SSI is scarce. 15 This scarcity could be attributed to our limited understanding of the relation between this genus and hosts, as well as the unclear role playing in the occurrence and development of SSIs.
In this study, among the 45 patients with SSIs, Shewanella genus were identified as the definitive pathogen in 15 of 45 cases (33.33%), whereas the majority, 30 of 45 cases (66.67%), presented with mixed infections, a pattern that seems align with the characteristics of colonization-associated infections, 16 consistent with reports by Holt et al. 17 Wincy et al. 18 found thatShewanella and other intestinal microbes were commonly colonized asymptomatically in the bile ducts and drainage tubes of patients with hepatobiliary diseases. They suggested that these colonizing microbes may evolve into severe infections, such as bacteremia, in appropriate clinical settings, such as acute biliary obstruction. To et al. 19 also observed asymptomatic colonization of Shewanella species within drainage tubes. A medical history investigation in this study revealed that the majority of patients, 42 of 45 (93.33%), had no contact with seawater or seafood. The three patients who had consumed seafood claimed that it was thoroughly cooked and properly handled. Therefore, we speculate that the occurrence of Shewanella-related SSI in this study may be related to the coastal location and the lifestyle of the inhabitants. However, due to the lack of relevant research on the distribution of Shewanella species in the digestive systems of healthy individuals in coastal areas, whether Shewanella species exists in a colonized form in the digestive systems of coastal residents remains to be further clarified.
We also observed that Shewanella-related SSIs were more common in patients undergoing surgeries related to the hepatobiliary system, accounting for 22 of 45 (48.88%). Some researchers have reported 16 cases of soft tissue infections associated with putrefactive Shewanella, with 75% having concurrent hepatobiliary diseases. 20 This observation might be attributed to the presence of numerous genes involved in bile decomposition and utilization of fatty acids, making it well-suited for survival in high-fat and high-bile environment. 21
For hepatobiliary diseases, we typically use a prophylactic antibiotic such as cefoperazone-sulbactam or cefotetan. The frequent occurrence of Shewanella-related SSI also suggests that the limitation of current prophylactic antibiotic use and the potential emergence of antibiotic resistance. According to our drug sensitivity test results, Shewanella genus exhibits over 20% resistance to third-generation cephalosporins, especially in Shewanella algae, which shows a resistance rate as high as 46.15% to amoxicillin-clavulanate and 38.46% to cefoperazone-sulbactam. Among the 10 multi-drug–resistant strains, six strains were resistant to six commonly used antibiotic agents, consistent with the findings of Zago et al. 22 They isolated Shewanella from estuarine water samples in China and found their resistance to ampicillin, amikacin, cefpodoxime, cefepime, chloramphenicol, ciprofloxacin, erythromycin, kanamycin, and trimethoprim-sulfamethoxazole. Our study results indicate that Shewanella was more sensitive to sulfamethoxazole, aminoglycosides, carbapenems, and quinolones. This suggests that, under the premise of general patient well-being, the combination of cephalosporins with sulfamethoxazole or aminoglycosides can reduce the risk of post-operative Shewanella-related SSIs. 23 Although there is a rising trend in antimicrobial resistance among Shewanella genus, given the relatively low incidence rate of Shewanella-related SSIs and the current prophylactic antibiotic regimens for gastrointestinal surgeries, there is currently no need for specific antibiotic prophylaxis measures against Shewanella-related SSIs. Our research findings indicated that Shewanella genus were more sensitive to complex novobiocin, aminoglycosides, carbapenems, and quinolones. Hence, the combination therapy of cephalosporins with complex novobiocin or aminoglycosides can effectively treat established Shewanella-related SSIs.
Among the 10 deceased patients, seven had infections combined with other bacteria. One case involved infections with three other types of bacteria, four cases involved infections with two other types, and two cases involved infections with one other type. In our study, the greater the variety of mixed infections with other micro-organisms in patients with Shewanella-related SSIs, the poorer the overall condition of the host, indicating a higher mortality rate. We adopted a combined approach using IL-6 and the Howell-PIRO scoring system to establish a model to assess the mortality rate, providing effective predictions of patients’' prognosis. The Howell-PIRO scoring system is designed for stratifying and prognostic evaluation of patients with sepsis, incorporating predisposition (P), infection (I), response (R), and organ dysfunction (O) caused by pathogenic factors. 24 This system is commonly used for assessing emergency blood stream infection patients.
Plasma IL-6 levels directly reflect the patient's infection status, with higher sensitivity and specificity compared to C-reactive protein (CRP) and procalcitonin (PCT). Although a certain level of IL-6 contributes to the activation of collective immune cell function, excessively high plasma IL-6 levels often indicate a state of imbalance in inflammatory cytokines. In severe cases, this imbalance can lead to a cytokine storm, resulting in a poor prognosis and extremely high mortality rates. 25 In our study, the death group with Shewanella genus infections exhibited higher plasma IL-6 levels and Howell-PIRO scores than the survival group. In one case, the plasma IL-6 level reached 7,217.71 pg/mL, indicating a cytokine storm level. Through the combined application of plasma IL-6 levels and the Howell-PIRO scoring system, we were able to increase the positive predictive value of patient mortality risk to 92.71%, raise the negative predictive value to 94.58%, and achieve a diagnostic sensitivity of 93.35% and specificity of 92.14%. According to our research model, patients with poor general conditions, multiple underlying diseases, higher Howell-PIRO scores, and elevated plasma IL-6 levels should receive prompt and aggressive treatment, potentially contributing to a reduction in mortality rates.
Conclusions
Because of the retrospective study, there may be some bias in the statistical results for the relatively small number of cases. Additionally, during the statistical process, there might be a lack of consideration for the impact of other pathogenic microorganisms or drug treatments on patient prognosis. Despite these limitations, we believe that residents in coastal areas faced a significantly increased risk of Shewanella-related SSIs. Despite obtaining only 45 clinical isolates of Shewanella over 10 years, Shewanella is widely distributed in marine environments. Our research findings indicated a gradual increase in resistance to cephalosporins and quinolones of Shewanella, along with several multi-drug–resistant strains isolated within the past two years. Although there is an emerging trend of antimicrobial resistance among Shewanella, the current incidence rate of Shewanella-related SSIs remains relatively low. Moreover, existing prophylactic antibiotic regimens can cover the majority susceptible Shewanella strains, suggesting that specific antibiotic prophylaxis measures against Shewanella-related SSIs are not yet necessary. For established Shewanella-related SSIs, combination therapy with cephalosporins and compounds such as complex novobiocin or aminoglycosides can yield favorable treatment outcomes. Additionally, the combined application of plasma IL-6 levels and the Howell-PIRO scoring system aids in assessing the prognosis of patients with such SSIs, facilitating timely clinical intervention to reduce mortality rates.
Footnotes
Authors' Contributions
Conception: Gu. Design: Li. Supervision: Zhao. Materials: Li, Zhao, Ye. Data collection and/or processing: Zhang. Analysis and/or interpretation: Yang, Huang. Literature review: Gu, Wu. Writing: Li, Zhao. Critical review: Gu.
Funding Information
The authors received no financial support for this article's research, authorship or publication.
Author Disclosure Statement
No competing financial interests exist, according to the policy of the journal. The ethical approval for the study was taken from the institute ethical committee. No. Dean/2023/EC/0153, Dated: 12-05-2023.