
Abstract
Background:
Fournier gangrene (FG) is a form of necrotizing fasciitis involving the perineal, peri-anal, and genital structures, and has exceptionally high mortality rates. To help in early detection of high-risk patients, we aimed to systematically review factors associated with mortality from FG.
Patients and Methods:
Searches were conducted in PubMed, Embase and Scopus. In our review, a minimum of five patients were required and this was to exclude studies with exceedingly small sample sizes, such as case reports and small case series, with minimal relevance in comparison to larger scale studies. Patient characteristics, causative microbes, anatomic areas of infection, presence of comorbidities, severity scores, causes of FG, and complications were extracted and compared to identify factors related to mortality.
Results:
A total of 57 studies were included in the review. Across 3,646 study participants, the mortality rate of FG was 20.41%. The mean age of non-survivors was 61.27 years. There were more total male deaths, however, the mortality rate was higher in females. Diabetes mellitus was the most common comorbidity in those who died, but the highest mortality rate was seen in HIV patients (54.17%). Mortality rates did not differ widely among antibiotic agents. Regarding causative organisms, fungal infections had the highest rates of mortality (68.18%) and the most common microbe leading to death was Escherichia coli.
Conclusions:
Female gender, comorbidities, anatomic distribution, development of sepsis, and fungal infection all increased risk for mortality. Early identification of risk factors, and provision of appropriate treatment are crucial in reducing mortality rates of high-risk patients with FG.
Fournier gangrene (FG) is a form of necrotizing fasciitis involving the perineal, peri-anal, and genital structures.1,2 Most cases are of colorectal, urogenital or trauma origin. 3 All genders and age ranges can be affected; however, frequency is higher in males compared with females (10:1) with increased rates also occurring in those above 50 years of age.1,4
Fournier gangrene pathogenesis typically arises from a polymicrobial synergism between aerobic and anerobic bacteria within genital areas.5,6 Aerobic microbes increase platelet aggregation and complement fixation whereas anaerobic bacteria form collagenase and heparinase producing clots. 7 Together they create a micro-environment promoting rapid, polymicrobial dissemination causing massive inflammation. 2 This leads to obliterative endarteritis and progressive gangrene across the overlying skin, fascia, and genitalia.7–9 These responses can be amplified by predisposing factors that lower the host's immunity, creating a favorable environment for the opportunistic spread of bacteria.10,11
Patients with FG tend to have a pattern of symptoms, and this condition is hence diagnosed clinically. Talwar et al. 12 describes the clinical course of FG beginning with symptoms of fever and lethargy for up to a week. This then progresses to genital tenderness and pain, evolving to erythema, and then dusky, macerated skin with subcutaneous crepitation. In late stages, obvious gangrene with purulent discharge is noted, which has a feculent odor and “dishwater” type discharge because of anaerobic infection. 5 Experiencing systemic signs out of proportion to the extent of injury/disease is another important marker of FG. 7 Furthermore, clinical signs of sepsis/septic shock, such as hypotension, tachycardia and mental obtundation have been described previously in the literature as potential indicators of FG severity.13–15
Imaging can be helpful in assessing atypical presentations or to guide surgical management. 7 However, because of the rapid and severe progression of FG, imaging should not delay treatment. Treatment regimens typically consist of broad-spectrum antibiotic agents, hemodynamic support, and aggressive surgical debridement.16,17
The mortality rates of FG currently remain exceptionally high, at up to 40%. 17 There is an urgent need for better detection of mortality causes that will help improve management. Although prior reviews have described comorbidities, etiologies, 10 and the predictive value of biochemical markers and severity scores, such as the Fournier gangrene severity index (FGSI), 18 the current understanding of microbes and additional patient-specific risk factors for FG mortality remains poorly understood. Therefore, to guide surveillance efforts and to improve overall patient outcomes, the purpose of this systematic review was to evaluate risk factors associated with mortality among patients with FG thoroughly.
Patients and Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA). 19 On January 11, 2024, PubMed, Embase and Scopus databases were searched. Because FG is a type of necrotizing fasciitis, to allow for as many relevant articles as possible, search terms were broadly inclusive of necrotizing fasciitis. Studies eligible for inclusion were those that include at least five patients who died from FG, describe at least one modifiable/non-modifiable factor associated with FG mortality (aside from demographic factors such as age and gender), peer-reviewed full-text studies, and were available in English. Relevant eligible study types include cohort studies, case-control studies, cross-sectional analyses, case series or clinical trials. However, studies that only provided abstracts alone were excluded. Studies were not restricted across location, or date. The following article types were not eligible for inclusion: qualitative studies, reviews, editorials, and commentaries.
After the completion of searches, three reviewers (P.S., A.M., and K.V.) independently screened the articles according to the inclusion and exclusion criteria. After duplicates were removed, studies were screened by their title and abstract. The articles that remained were then analyzed according to their full text by two reviewers (P.S. and A.M.) with discrepancies being sorted by a third reviewer (K.V.) for a final consensus to be reached between all three reviewers regarding articles to be accepted for this review.
Patient data and study characteristics were then extracted from the included set of articles. The patient data included information regarding number, city and country of the participants, causative microbes, age, gender, anatomic areas of infection, presence of comorbidities in survivors and non-survivors, causes of FG and complications during hospitalization, and severity scores. All of these were stratified and recorded according to mortality rate. Additional related risk factors of both survivors and non-survivors were also obtained. These include, but are not limited to, factors such as medical and surgical information, time course, and surface area involvement. Study characteristics included evaluation of the study design, objectives, sources of data, proportion of FG deaths within the FG population and study limitations. This extraction was conducted using MS Excel (Microsoft, Redmond, WA).
Because of the heterogeneity of data and inconsistencies in reporting of data across the included studies, a meta-analysis was not possible for this review. Instead, following approaches previously taken,20,21 data was pooled across included studies to investigate the overall and stratified factors associated with trends for mortality. Categorical data was pooled for patients across studies and shown in tabular format. Although continuous data and odds/hazard ratios were not able to be pooled in this manner, trends across studies for continuous variables (such as age, and severity scores) and odds/hazards ratios were qualitatively analyzed and described in our review. Data for stratified variables were only included in the pooled analysis if there was explicit reporting of the relevant variable (e.g., gender, causative microbe[s]) for patients.
All studies that met the inclusion criteria were evaluated for their methodologic quality using the Joanna Briggs Institute's (JBI) critical appraisal tools. 22 Following a similar study undertaken previously 20 relative scores (in percentages) were used to compare differences in methodologic quality across study methodologies using the JBI tools. Numeric scores for each article were based on the total number of “yes” or “no”/“unclear” metrics of the JBI checklist for that study methodology (an “unclear” was assigned the same score as a “no”), as has been conducted previously.23,24 If a parameter on the checklist was marked as “not applicable” (NA) for a study, then that parameter did not contribute to the percentage score of that study.
To assess for heterogeneity across studies, we followed existing recommendations for systematic reviews without meta-analyses. 25 This heterogeneity assessment was done by comparing study/methodologic characteristics of included articles on the following parameters: study location, date of study, study design, population size, and number/percentage of patients who died. We also classified studies in terms of overall quality based on JBI quality assessment scores. Studies with a quality assessment score of 0% to 50.0% were classified as low quality, those with a score of 50.1% to 75.0% were classified as moderate quality, and those with a score above 75.0% were denoted as high quality.
Results
Searches produced a total of 6,869 results. After the removal of duplicates, a total of 3,822 studies were screened. A total of 3,341 articles were removed after screening by abstract, an additional 424 articles were removed after screening by full text. Common reasons for exclusion of articles were studies not being specific to FG, not stratifying for mortality, and reporting less than five deaths. In total 57 studies were eligible for inclusion in our systematic review.26–82 The entire screening process is depicted in Figure 1.
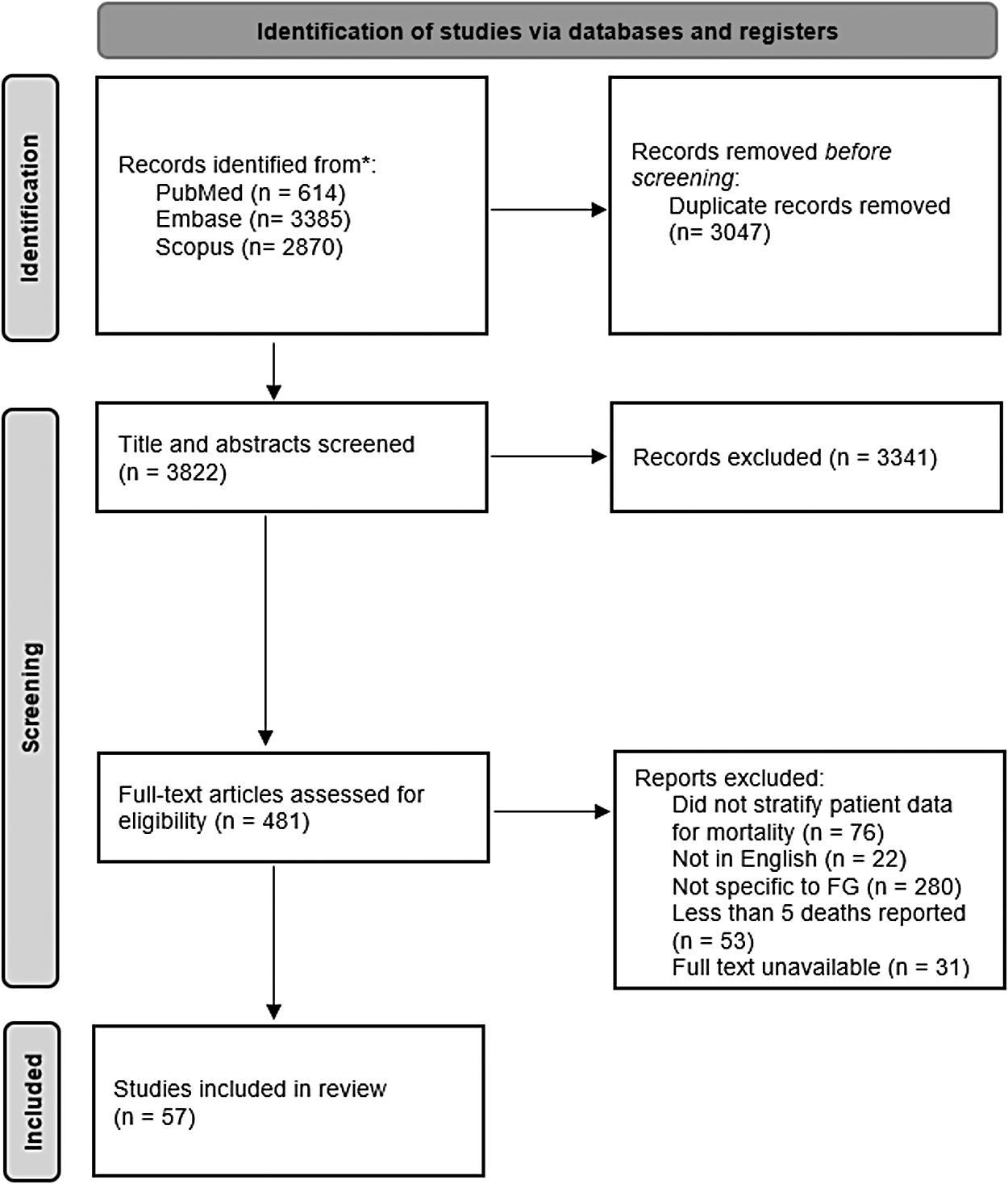
Workflow for screening studies (Adapted from Page et al., 2020).
A full list of study characteristics, by individual study, is shown in Supplementary Table S1. In terms of study heterogeneity, there was wide variation across studies included. Twenty-five different countries were represented across the included studies, with 23 studies28,29,31,32,37–40,45–47,52,55,58,59,63,67,69,70,75,77,79,81 occurring in Europe, 16 studies27,33–35,43,44,48,49,50,57,61,62,71,54,74,82 in Asia, 10 studies36,41,56,60,65,66,68,72,73,78 in North America, six studies26,30 53,64,76,80 in Africa, and two studies42,51 in South America. Studies were commonly conducted in Turkey29,31,37,46,47,55,58,67,70,75,77,79,81 (n = 13), the United States36,41,56,60,66,68,72,73 (n = 8), Germany38–40,59 (n = 4), South Korea48,54,82 (n = 3), Spain45,63,69 (n = 3), and Taiwan,35,50,61(n = 3). Two studies were conducted in each of the respective countries: Morocco,30,76 China,33,49 Brazil,42,51 Greece,52,59 Pakistan,62,71 and Mexico.65,78 A single study was conducted in each of the following countries: Nigeria, 26 Philippines, 27 Croatia, 28 Slovenia, 28 Italy, 32 India, 34 Iran, 43 Kuwait, 44 Tunisia, 53 Lithuania, 57 Zimbabwe, 64 Japan, 74 and Yemen. 80
Regarding years in which studies took place, three studies45,68,72 were from 1980 to 1989, three studies60,66,73 were from 1990 to 1999, 10 studies31,32,38,41,54,55,58,61,65,78 were from 2000 to 2009, 28 studies28–30,33,35,36,39,40,44,46,48,50–52,56,57,59,62–64,67,69,71,74–77,79 were from 2010 to 2019 and 13 studies26,27,34,37,42,43,47,49,53,70,80–82 were from 2020 to 2023. Median study sample size was 45, with a range of eight total participants 32 to 636 participants. 52 In terms of patients who died across studies, the median total was 10, and the range was from five deaths32,34,49,51,52,67,68,75 to 65 deaths, 74 with proportions ranging from 9.60% 75 to 62.50% 32 (median, 22.29%). The largest study included in this review had 64 patients who died, and an overall mortality rate of 10.1% (636 total participants), 56 followed by a study with sample size of 329 and a mortality rate of 19.76% (65 total deaths). 74
A visual depiction of relative quality assessment scores is shown in Figure 2. The majority of studies included had a retrospective cohort design (n = 49).26-31,33-41,44-55,57–61,63,65–78,80–82 The other three study designs among included studies were a prospective cohort design (n = 4),56,62,64,79 case series (n = 3),32,42,68 and a cross-sectional design (n = 1). 43 In terms of relative study quality assessment scores, the mean score across all included studies was 70.50% (standard deviation [SD], 18.86; range, 22.22–100.00). Cohort studies had a mean score of 69.83% (SD, 18.72; range, 22.22–100.00), the three-case series had a mean score of 76.67% (SD, 25.19; range, 50.00–100.00), and the single cross-sectional study had a score of 87.5%. Twenty-six studies27,30,32,33,37,41–43,48–50,52,53,55,56,58,60,63,64,66,70,74,77,79,80,82 had a score that was ranked as high (75.01% or above), 22 studies26,31,36,38,40,44,46,47,51,54,57,59,62,65,67,69,71,75,76,78,81 had score ranked as moderate (50.01%–75.00%), and nine studies28,29,34,35,45,61,68,72,73 had a score ranked as low (50.00% or less). The most common methodologic flaws denoted from the quality assessments included limited identification of confounding factors and limited strategies to deal with confounding variables, inconsistencies in study participant follow-up, and dissimilarities in groups that underwent comparison. Full quality assessments are shown in Supplementary Tables S2 to S4.
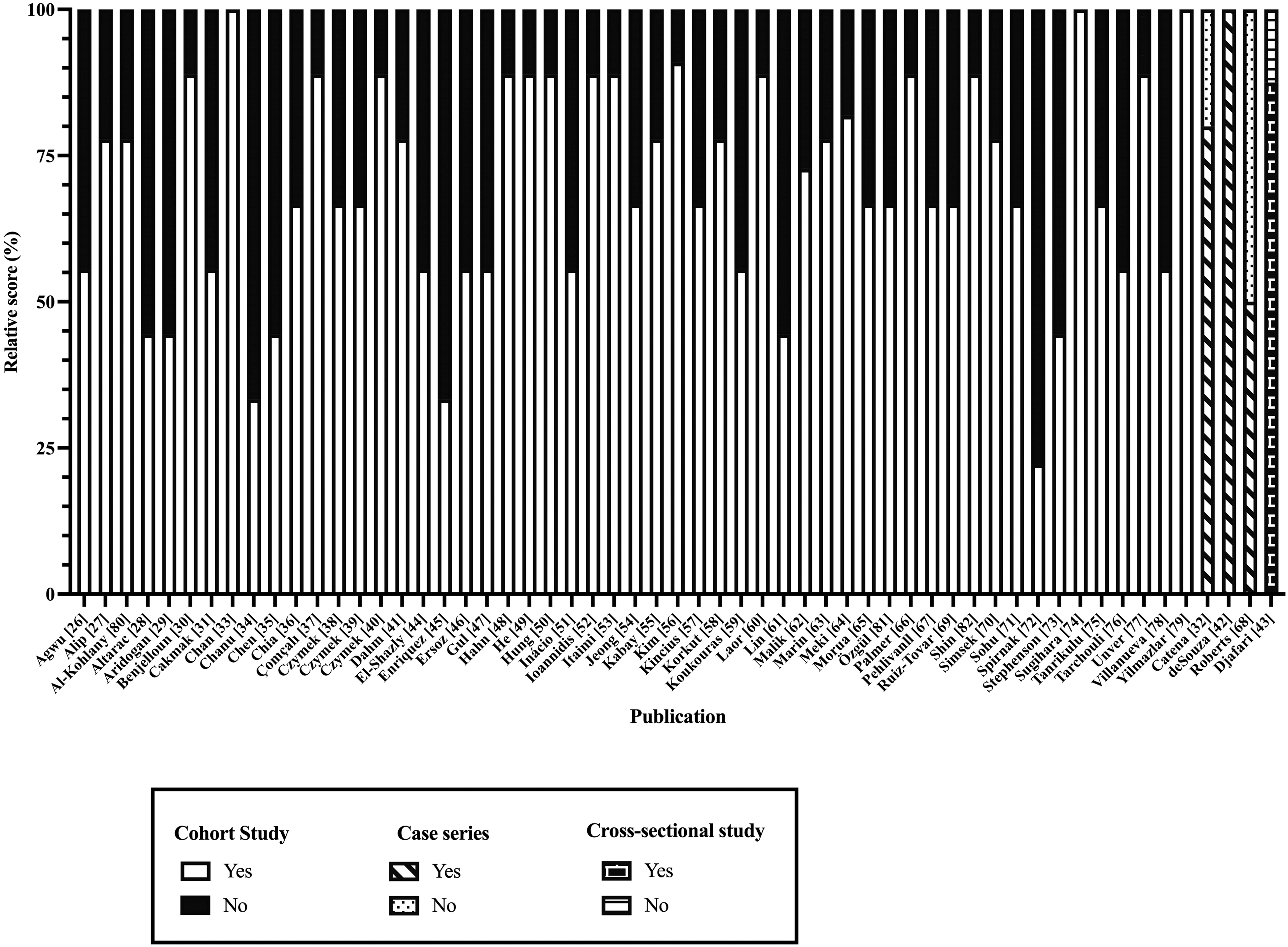
Relative quality assessments scores for studies included in this systematic review.
In terms of FG mortality, 744 patients died out of a total of 3,646 study participants, corresponding to a death rate of 20.41%. The mean FGSI score for non-survivors was 10.09 versus 4.33 for survivors with studies consistently showing a cutoff score of nine or more being greatly associated with mortality (odds ratio [OR], 4.11; 95% confidence interval [CI], 1.15–14.73; p = 0.024). 50
The mean age of those who died was 61.27 years, whereas the mean age of survivors of 53.21 years. Çomçalı et al. 37 and Kincius et al. 57 both found that age was associated with a higher risk for mortality. Mortality rates were notably higher among females (29.76%) compared with males (20.48%). However, two studies that analyzed gender as a potential risk factor for mortality found that being female was not statistically associated with FG mortality.74,79
Causative microbes varied widely across those who died. A full list of microbial causes of FG are shown in Table 1. Those infected with aerobes had comparable death rates to those infected with anaerobes (31.96% and 33.12%, respectively), and those infected with gram-negative organisms had similar rates of death to infected with gram-positive microbes (33.48% compared with 30.00%). Forty of 57 articles reported on microbiology data, and of these, 12 studies reported on positive findings for fungal infections; however, aside from these 12, the remaining studies were often unclear on if fungal infections, in addition to bacterial infections, were cultured. In the cases in which they were reported, those infected with fungi had particularly high death rates at 68.18%. In terms of microbes/species, highest rates of death occurred from FG due to Candida albicans (61.11%), Proteus species (60.00%), Pseudomonas species (47.83%), and Acinetobacter species (44.44%). Although Escherichia coli was the most common microbe found both with those who developed FG and those who died from FG, the death rate for those infected with Escherichia coli (25.97%) was lower compared with other microbes. Drug-resistant infections were relatively uncommon and had lower mortality rates.
Causative Microbes for Those Who Died from FG
FG = Fournier gangrene.
Pooled characteristics, including risk factors, management, cause of death, and site of infection, are shown in Table 2. In terms of anatomy, FG occurred most in the genitourinary and colorectal/anorectal/peri-anal regions; however, the highest rates of mortality due to FG occurred when it was present in the vulval region (61.54%), and the perineal region (37.72%). Fournier gangrene advancing beyond the genital area to the abdominal wall elevated mortality (OR, 7.5; 95% CI, 1.2–57.2; p = 0.033) 69 and a 1% increase in surface area involvement was linked to a mortality increase of almost 21-fold (OR, 20.8; p = 0.001). 57 Those with comorbidities consistently had high mortality rates; these rates were the highest for those with human immunodeficiency virus (HIV). Individuals with at least one of the following conditions had death rates above 40%: hematologic disorders/immunosuppression, malignancy, liver disease, renal insufficiency/renal failure and obesity. Furthermore, those with the following conditions had death rates above 30%: hypertension, cardiovascular disease other than hypertension, lung diseas,e and neurologic/psychiatric disease. Although diabetes mellitus was the most common co-occurring condition among those with FG (1,162 cases), the mortality rate (27.54%) was lower than those with other conditions. However, this did vary across studies. For example, across individual studies, death rates for those with diabetes mellitus were as high as 85.71%, 57 80%, 64 and 77.27%. 62
Pooled Patient Characteristics and Death Rates for Those With FG
FG = Fournier gangrene; FGSI = Fournier gangrene severity index; HIV = human immunodeficiency virus; VAC = vacuum-assisted closure.
In terms of modifiable risk factors related to lifestyle, both smoking and alcoholism were reported across studies. Smoking status was reported in only six studies33,42,48,52,63,70. Of the 90 reported patients with FG who smoke, 41 died (45.56%). Alcoholism was reported in 57 patients, 17 of whom died (29.82%). Body mass index (BMI) was inconsistently reported across studies, however, obesity status was reported more consistently. Of the individuals who were classified as obese, 23 were morbidly obese with a mortality rate of 47.83% and 24 were classified as obese only, with a mortality rate of 37.50%.
Sepsis and septic shock were common complications. Patients who developed sepsis and septic shock had especially high mortality rates at 61.08% for sepsis, and 53.33% for septic shock. In a study by Hahn et al. 48 100% of those with FG who developed septic shock ultimately died.
Management was typically a combination of surgical and non-surgical. With surgical intervention, and especially debridement being at the forefront of FG care, almost all patients received debridement. Other most frequently conducted surgeries among those who died were colostomy, cystostomy, and orchidectomy. Increased length of time before surgical debridement were also predictive of mortality. Early colostomy had an odds ratio of 0.14 for death (95% CI, 0.02–1.20) whereas delayed colostomy had an odds ratio of 9.63 (95% CI, 1.64–56.37). 50 Increased need of operations (OR, 1.7; 95% CI, 1.2–2.5l; p = 0.004) and repeat surgery increased mortality, 71 with patients needing more than four debridements increased mortality rates by almost nine-fold (OR, 8.7; 95% CI, 1.7–102.3; p = 0.043). 69
For non-surgical management, death rates were exceedingly high for those who had some form of mechanical ventilation (77.78%), and those who received inotropes (90.48%). Mortality rates did not differ widely among those receiving one, or multiple antibiotics. However, those who were given antibiotic agents prior to diagnosis/admission had mortality rates 1.73 times higher than those who did not receive antibiotic agents (31.68% death rate for those given antibiotic agents, compared with 18.33% for those who were not).
Discussion
Our review, which has included findings from 25 countries and 3,646 participants, has shown that individuals with FG have a notably high mortality rate of approximately 20%, which is in line with mortality rates from prior literature. 83 Although studies in this review were conducted across a wide array of geographic settings, there were not clear trends observed regarding geographic differences of risk factors. For example, fungal infections were reported in studies conducted in six countries: Turkey,29,70,85 the United States, 36 Germany,38,40 South Korea,48,82 Taiwan,50,61 and Mexico,65,78 but no pattern regarding geography was noted. Similarly, conditions such as diabetes mellitus and hypertension did not demonstrate clear patterns or trends.
There are two main prognostic scoring scales that are specific and with good reliability for assessing FG severity and risk of mortality. 84 Previously, the FGSI score by Laor et al. 60 that analyzes clinical signs and laboratory markers to predict patient outcomes was widely utilized. This has been expanded by Yılmazlar et al. 85 through the Uludag Fournier gangrene severity index (UFGSI), which includes age, and extent of disease to the FGSI. Various other scores, such as the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, 86 neutrophile-lymphocyte ratio (NLR), 87 Acute Physiology and Chronic Health Evaluation (APACHE II) 82 and the Charlson comorbidity index (CCI) 88 have also been described in literature, however, they are not specific to FG. Our review builds on these study scores to provide additional risk factors for FG mortality, including information on microbes, comorbidities, treatment factors, and complications. It is hoped that these findings can serve as a guideline for the ongoing development, and modification, of existing guidelines, to better predict factors associated with poor outcomes among patients with FG.
In terms of electrolyte balances as biochemical abnormalities, high/low levels of bicarbonate, sodium, and potassium are included as part of the FGSI, however many studies merely reported their FGSI scores and not the electrolyte imbalances. Therefore, although it is likely that many of these abnormalities were present in non-survivors based on the high overall FGSI scores, it is important that future literature more clearly describes what electrolyte abnormalities are occurring in patients with FG. This may have important clinical implications, especially as past literature on NF has shown that hyponatremia may be an important risk factor for mortality.89–91
To the best of our knowledge, this is the first review to analyze microbes involved with FG mortality. Our findings demonstrate that the causative microbe/microbes of FG may provide indication of the overall level of mortality risk for patients. Those with FG caused by a fungal infection have been shown to have especially high rates of death, and there are several plausible explanations for this. One could be that those who develop fungal infections are more likely to have prior immunosuppression, thereby also increasing their risk for eventual mortality. A second plausible explanation could be that the initial infection may have been treated with a broad-spectrum antibiotic agent, which would be ineffective against a fungal infection. A third possible explanation could be because of a limited supply of antifungal treatments, and those that were used for patients may have been inadequate. This emphasizes the need to prioritize determination of causative microbes when FG develops, and to make additional efforts to also test for the presence of any fungal infections.
It is relevant to denote that, for immunocompromised/immunosuppressed individuals (such as patients with cancer and those living with HIV) with FG, it is recommended that anti-fungal therapy be included in treatment regimens alongside empirical antibiotics; these patients may also benefit from earlier consideration of more intensive treatment, such as early diverting colostomy, to avoid poor outcomes. In addition to this, future research should focus on further elaborating on effective treatment for all patients with FG with a fungal infection and to determine what specific factors increase, and decrease, death rates for those with such infections.
There was minimal difference identified in mortality rates between aerobic (31.96%) and anaerobic microbes (33.12%); however, there was a clear difference between monomicrobial (21.62%) and polymicrobial (31.58%) infections. This was expected as the severity of FG arises from the synergism between these two classes of microbes because they create an opportunistic and unfavorable environment leading to mortality.5,6 Notably, some highly virulent bacteria, such as Clostridium, had shown lower rates of mortality than other, less virulent microbes. This may be due to several factors, such as a lack of polymicrobial infection in these patients, or because of the severity of the highly virulent microbes, there may have been quicker initial response time to surgery. Regardless, limited generalizations can be made here, because a relatively small proportion of patients were identified as having been infected with these microbes.
A group shown to be at a particularly high risk for death was females who were shown to have lower incidence but be at a higher risk of mortality in comparison with males. A possible explanation for this comes from Czymek et al., 39 who state that improved drainage of secretions in the female genitalia helps limit initial FG infection, however, once diagnosis is established, this system is disadvantageous because it can increase the inflammatory process and bacterial dissemination into the pelvis. Differences in genitalia across the genders (with male genitalia being outside the pelvis whereas female genitalia are inside the pelvis), also explain the greater risk for rapid spread of infection to the retroperitoneum among females compared with males.
Others with increased rate of mortality included patients with at least one comorbidity. Therefore, individuals living with comorbidities who develop FG need to be prioritized for urgent care or they otherwise face an exceedingly high mortality risk. Although those with HIV had a mortality rate above 54% in our review, only a limited number of individuals with HIV were included in this study. More large-scale research is needed to better evaluate the risk for mortality among those with HIV, and to determine the factors that elevate the risk of necrotizing fasciitis and FG development among this population; specifically, it will be important to investigate whether those with a low viral load and normalized CD4 cell count have higher levels of risk.
Although individuals with diabetes mellitus had an overall mortality rate that was lower than those with other comorbidities, it is crucial to denote that diabetes mellitus was both shown to be a significant risk factor for the development of FG, and that there were highly variable rates in mortality for those with diabetes mellitus, as several studies demonstrated a mortality rate exceeding 75% among those with diabetes mellitus.57,62,64 Importantly, studies did not consider, nor control for, the extent to which diabetes mellitus was controlled (or uncontrolled) among participants and so, future research should aim to determine what characteristics among those with diabetes mellitus increase the risk of development, and death from FG, as well as other forms of necrotizing fasciitis. This may include an analysis of patient blood sugar levels and/or HbA1c levels and assessing the influence of controlled versus uncontrolled diabetes mellitus. This may assist in improving outcomes of patients with diabetes mellitus in hospital and outpatient settings, because identifying high risk patients may allow for early treatment and prevention.
The development of sepsis and septic shock were commonly described complications and eventual causes of death among patients with FG. This has important clinical implications and demonstrates the urgent severity of sickness for patients with FG with such complications, and the need to maximize immediate treatment usage to keep the patients alive. Linked to this point, there is a need for the development of clear guidelines to treat patients with FG who develop sepsis or septic shock. Similarly, those given inotrope medications and mechanical ventilation had very high rates of death and this is likely because the patients who were given such treatments were already close to death. The usage of such forms of intervention needs to be recognized as additional markers of urgent severity.
Regarding treatment, a paradoxical finding of our review was that those given antibiotic agents prior to admission/diagnosis of FG died more frequently compared with those who were given antibiotic agents after being diagnosed. However, a large proportion of studies did not describe this timing for treatments. One possible explanation for these findings is that antibiotic agents may have been offered prior to surgery, and surgical options may have only been considered after the patient had already deteriorated to a point where they would not be able to recover. Another possible explanation is that inappropriate or weaker antibiotic treatments may have been given at earlier points, prior to a definitive diagnosis being made; this may have contributed to poorer outcomes. This highlights a clear need for more research to be developed to determine the influence of antibiotic regimens prior to diagnosis/admission, the importance of making a definitive diagnosis as soon as possible, and the need to conduct surgery in a timely manner to prevent further deterioration of patients.
For this review, there are several limitations that need to be recognized. Because of the heterogeneity of articles, a meta-analysis is not able to be completed and so, risk factors such as time to initial surgical debridement or number of debridements could not be compared after controlling for other known high-risk factors such as diabetes mellitus status. Although general risk factors were determined across an array of different populations, there was limited stratification of findings across high-risk groups, outlining areas of future research. For example, no studies analyzed risk factors while controlling for immunocompromised patients. It is hence recommended that future studies investigate the extent to which being immunocompromised impacts patient outcomes.
Similarly, it remains unclear what proportion of patients who had developed complications such as sepsis, had comorbidities and non-surgical management. Furthermore, there is limited stratification amongst microbial data, particularly if infections included a mix of various bacteria, or concurrent bacterial and fungal infection. There is also lack of analysis on whether infections by species of microbes with the highest mortality rates required repeated debridement. These are hence important areas in which future research should aim to focus on.
Another limitation of this review is that there were no case control studies included in this review. To better identify risk factors for mortality, it would be ideal to have randomized controlled trials through comparisons of treatments and outcomes for with those who did not develop FG, or developed FG but did not die. However, research involving control groups and conducting randomized prospective trials would be inherently difficult because of the urgency and nature of this acute medical emergency.
Similarly, long-term follow-up of survivors was limited in this review, but would be important for determining risk after leaving hospital settings. It is also worth denoting that this review may have missed some potentially relevant studies due to our inclusion/exclusion criteria (requiring that studies be written in English and have stratified data for patients dying from FG), and due to studies being missed during the process of screening. However, for this review, three reviewers meticulously screened as per the PRISMA guidelines, in an independent manner to ensure that as many relevant articles as possible were included, and to avoid any being missed. Of further relevance is that the requirement of studies including at least five patients who died may have introduced bias and may have potentially resulted in a skew towards a higher overall mortality rate in our review.
Regardless of the limitations of this review, there are also notable strengths; the robustness of these findings is demonstrated by the large number of studies (n = 57), enrolling 3,646 patients across a wide array of geographical and cultural settings, and outlining a range of factors which may influence FG mortality. Therefore, there is notable generalizability to our findings, which are relevant across a wide range of settings in which patients develop FG. The findings of this review have important clinical implications and may have a valuable role in developing guidelines to improve the outcomes of patients with FG.
Conclusions
This review has described several factors associated with FG mortality. Female gender, presence of comorbidities, anatomic distribution, development of sepsis, and fungal infection all have been shown to increase risk for mortality. These findings offer utility in the development of guidelines for addressing FG and lowering risk of death. Future research is needed on the role of antibiotic therapies, and the modifiable factors associated with death among high-risk groups.
Footnotes
Authors' Contributions
Conceptualization: P. Shet, Varshney. Methodology: P. Shet, Mustafa, Varshney. Formal analysis and investigation: P. Shet, Mustafa, Varshney, Rao, Sawdagar, McLennan, Ansari, D. Shet. Writing—original draft: P. Shet, Varshney, Sivathamboo, Campbell. Writing—review and editing: P. Shet, Varshney, Sivathamboo, Campbell.
Funding Information
The authors have received no financial support for the creation of this work.
Author Disclosure Statement
The authors have no conflicts of interest to disclose. The authors have no financial or non-financial interests to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.