
Abstract
Background:
Surgical site infections (SSIs) remain a conundrum for neurosurgeons. This study examines the efficacy and outcome of vacuum sealing drainage (VSD) in the treatment of pyogenic SSIs following intracranial neurosurgery.
Methods:
Twenty patients with SSIs, who received surgical intervention, were treated retrospectively with VSD during the past five years. Primary surgical procedure types, SSI types, VSD replacements, pathogenic germs, antibiotic therapy, and infection control were reviewed and discussed.
Results:
Of the 20 infections, 13 (65%) were extradural and 7 (35%) were extradural SSIs combined with intracranial infections (including 5 meningitis, 1 subdural abscess, and 1 brain abscess). All the patients consented to medical device implantation (including 5 titanium webs, 6 bone flap fixation devices, and 12 duraplasties), most of which were removed during debridement. The median duration from primary surgical procedure to an SSI diagnosis was 19 days (range: 7 to 365 d). All the patients also agreed to debridement and VSD treatment; VSD was replaced 0 to 5 times (median, one time) every 4 to 7 days and kept for 4 to 35 days (median, 14 d). Seven (35%) patients had defined bacterial infections, with Staphylococcus aureus being the dominant infection. The deployed standard VSD and antibiotic treatment ensured full recovery from SSIs, including from intracranial infections: 14 (70%) patients had recovered fully by follow-up, and no infection-associated death was registered; 6 (30%) patients died of severe primary affections.
Conclusion:
VSD-assisted therapy is safe and effective against SSIs after intracranial neurosurgery.
Introduction
Although brain surgery technology and asepsis have observed substantial developments in recent times, surgical site infections (SSIs) after intracranial neurosurgery occasionally persist and remain a worldwide clinical conundrum.1,2 Different centers and countries have reported varied rates of SSIs, ranging from <1% to >8%.2–5 Identified risk factors of SSIs after intracranial neurosurgery are as follows: the female gender, cerebrospinal fluid (CSF) leak, CSF drainage, the duration of operations, prior same-side craniotomy, prosthetic implants, and procedures on dry skin antiseptics, among others.6–9 An SSI often results in pain, altered consciousness, prolonged hospital stays, increased expenses, permanent sequelae, and morbidity and mortality.
SSIs post-neurosurgery have been classified into two categories: Extradural and intradural infections. 10 Some studies have also grouped SSIs into superficial incisional SSIs, deep incisional SSIs, and organ/space SSIs.3,11,12 Extradural SSIs include skin or subcutaneous tissue infections, soft tissue (fascia and muscle layer) infections, aponeurosis/skull bone infections, and epidural infections, during which a patient’s cerebral dura mater is completely intact and sealed off, without symptoms of an intracranial infection. Extradural SSIs are treated mainly with antimicrobial therapy, medical implant removal, debridement, and drainage.10,13 Intradural SSIs are recognized specifically as intracranial infections (a brain abscess, a subdural abscess, meningitis, encephalitis, or ventriculitis), which are severe and rapidly progressive. These severe post-operative complications require immediate and vigorous medical and/or surgical interventions, for instance, long-term antibiotic therapy, abscess excision or incision drainage, external ventricular drainage (EVD), and lumbar cistern drainage (LCD).14–16 Once the cerebral dura mater has been destroyed, extradural and intradural SSIs typically occur simultaneously, posing a life-threatening clinical challenge to neurosurgeons.
SSIs with focal pyogenic infections, such as subcutaneous tissue abscesses, subdural empyema, and brain abscesses, can be treated effectively and as required with surgical treatment. In most cases, excision and/or drainage of abscesses can adequately ensure the healing of pyogenic SSIs. Reportedly, a closed-incisional negative pressure therapy eases SSIs in spine surgical procedures, 17 and negative pressure wound therapy is arguably more effective against SSIs after vascular, abdominal, orthopedic, and thoracic surgeries than conventional procedures. 18 Vacuum sealing drainage (VSD), a core technique of negative pressure wound therapy, demonstrably exerts therapeutic efficacies against SSIs following spinal surgeries and multiple wound infections.19–21 However, the efficacy and outcome of VSD against SSIs after intracranial neurosurgery are still to be investigated fully.
This study retrospectively reviews the severe SSI cases treated at our department during the past five years. The investigation focused primarily on the patients with soft tissue abscesses with/without intracranial infections, who received surgical treatment administered using VSD. The efficacy of the technique and post-operative outcomes are presented and discussed in this study.
Methods
Study design and population
This retrospective study was conducted at the Neurosurgery Department of the Zhongnan Hospital of Wuhan University. The protocol was reviewed and approved by the Medical Ethics Committee of the Zhongnan Hospital of Wuhan University and applied in accordance with the Declaration of Helsinki. The patient group consisted of consecutive patients with post-intracranial neurosurgery pyogenic SSIs treated at the institution between March 2018 and May 2023. All the patients presented with severe soft tissue abscesses and needed surgical intervention with VSD. Surgical and antimicrobial therapies were performed following a standardized algorithm. An interdisciplinary team of infectiologists, pharmacists, and neurosurgeons was set up to evaluate every patient with an SSI. Data were collected from electronic medical charts and organized in a standardized case report form.
Definition of SSI
On the basis of criteria established by the Centers for Disease Control and Prevention (CDC) in 2023,22,23 an SSI was defined as any infection occurring within 30 or 90 days after the NHSN operative procedure or up to one year when prosthetic materials are implanted.
Extradural SSIs in this study, including skin or subcutaneous tissue infections, soft tissue (fascia and muscle layer) infections, aponeurosis/skull bone infections, and epidural infections, had to meet at least one of the following criteria for inclusion: 1) Purulent wound discharge; 2) (an) organism(s) isolated from an aseptically obtained specimen; 3) local signs or symptoms of an infection, such as localized pain, tenderness, swelling, or heat; 4) CT scanning or MRI showing subcutaneous tissue or epidural abscesses; and 5) the presence of wound infections during surgical procedures by neurosurgeons.
Intracranial infections, including brain abscesses, subdural abscesses, meningitis, encephalitis, and ventriculitis, had to meet at least one of the following criteria for inclusion: 1) (an) Organism(s) isolated from an CSF or intracranial abscess specimen; 2) typical symptoms of high fever, headache, meningeal signs, dysfunction of cranial nerves, and altered consciousness in the absence of other recognized causes; 3) increased white cell counts, decreased glucose concentration, and elevated proteins in the CSF; 4) CT scanning or MRI showing brain or subdural abscesses; and 5) the presence of intracranial infections during surgical procedures by neurosurgeons.
Surgical and antimicrobial treatment
Immediately after the diagnosis of SSIs, pyogenic extradural SSIs were subjected to empirical antibiotic therapy, then to surgical treatment of the original incision, and subsequently to a standardized protocol, such as preoperative hair removal and antibiotic therapy. The pus, necrotic tissues, inflammatory granulation, and scar tissues were excised, and the wound was flushed alternately with 3% hydrogen peroxide, diluted povidone iodine, and physiologic saline at least three times. Next, subhealthy tissues were eliminated, and the dead space was excavated completely. Finally, the wound was flushed repeatedly and stanched fully, and VSD was deployed. The VSD product was replaced every 4 to 7 days until the wound surface regained freshness and new granulation tissues were covered adequately. Upon successfully and completely curbing the infection and achieving effective generation of new granulation tissues, the deep soft tissue was repaired, and the skin flap was sutured. Wound vacuuming was kept between −20 and −40 kPa.
Pyogenic extradural SSIs combined with intracranial infections also received surgical intervention employing VSD according to the procedure above (Fig. 1). Antibiotic agents (vancomycin for gram-positive bacteria and meropenem for gram-negative bacteria) with decent brain tissue or meninges penetration properties were used intravenously and intrathecally for 4 to 6 weeks and adjusted accordingly after drug sensitivity testing. LCD was conducted regularly for CSF drainage and intrathecal injection. Intracranial abscesses, such as subdural empyema and brain abscesses, were excised and drained, and bone flaps and medical materials were removed. Wound vacuuming was kept at −20 kPa to avoid excessive CSF loss.
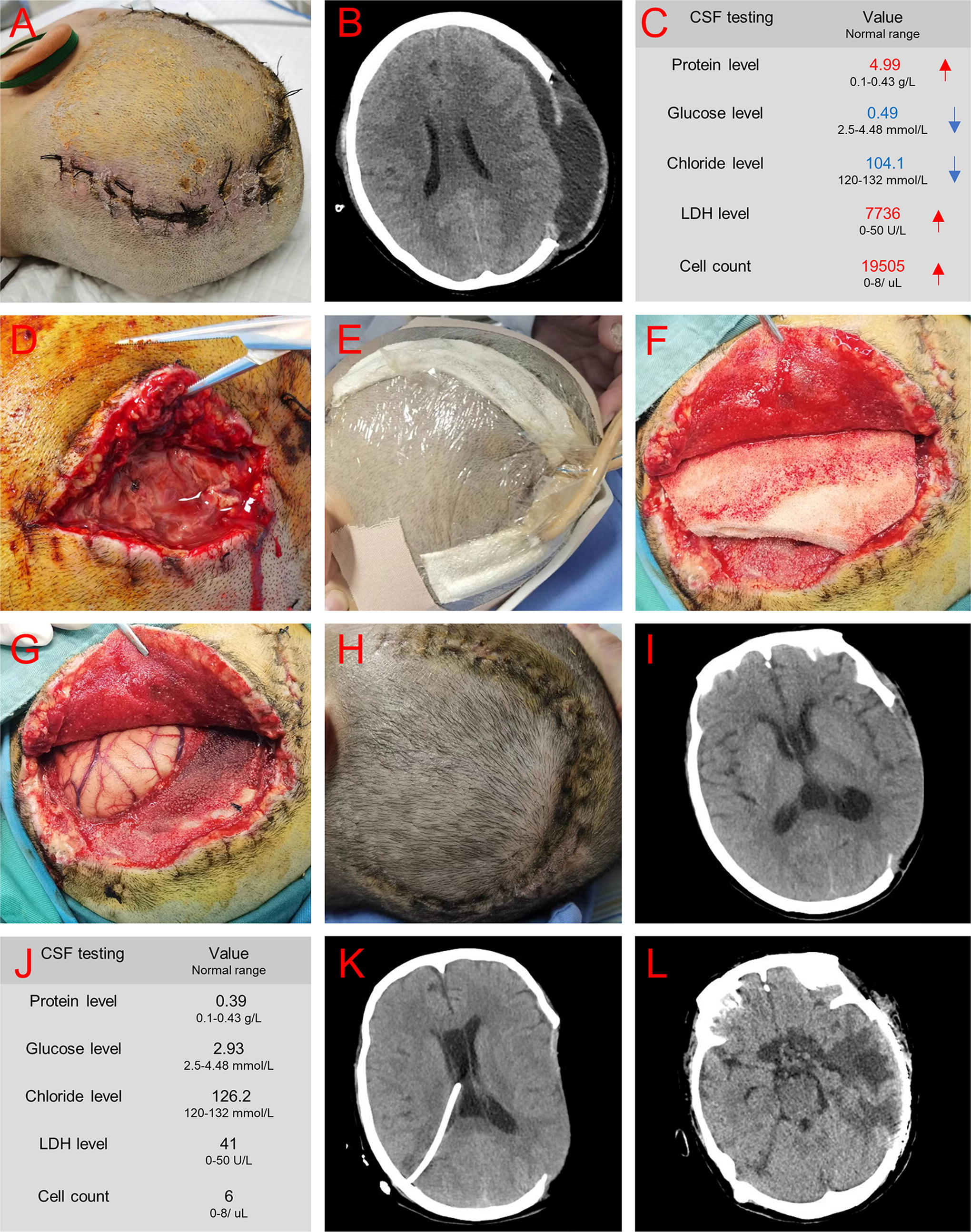
A 42-year-old female patient consented to the decompression and hematoma removal operation for two weeks after she was diagnosed with brain trauma.
Follow-up evaluation
Clinical signs or symptoms, intercurrent surgical procedures, drug use, disease chronicity treatment, and general health status were evaluated during follow-up visits. Patients were declared infection free if every one of the following criteria was met: 1) No sign or symptom of recurrent infections, 2) no requirement of antimicrobial therapy, 3) no laboratory-determined sign of recurrent abscesses, 4) no infection-related death, and 5) no subsequent need for surgical interventions against infections.
Results
Characteristics of the patients and infections
Demographics, clinical symptoms, and laboratory findings vis-à-vis SSIs after intracranial neurosurgery are detailed in Table 1. Of the 20 patients with SSIs, 13 (65%) were diagnosed with extradural SSIs (including one skin or subcutaneous tissue infection, two skull bone infections, six epidural infections, and four titanium web-associated infections) and 7 (35%) with extradural SSIs combined with intracranial infections (including five meningitis, one subdural abscess, and one brain abscess). All the patients presented with local signs of an infection and purulent wound discharges. All seven patients with intracranial infections presented with high fever, headache, meningeal symptoms, increased white cell counts, decreased glucose concentrations, and elevated proteins in the CSF; five (71%) of them exhibited altered consciousness. Six (46%) of the patients with extradural SSIs and only one (14%) with an intracranial infection had normal white blood cell counts and procalcitonin concentrations.
Demographics, Clinical Symptoms, and Laboratory Findings in 20 Patients with SSIs After Intracranial Neurosurgery
CSF, cerebrospinal fluid; WBC, white blood cell; PCT, procalcitonin; SSI, surgical site infection.
Characteristics of primary surgical procedures
As shown in Table 1, three patients with brain trauma were subjected to decompression and evacuation of intracranial hematoma operations. Eight patients experienced intracranial hematoma; four of them agreed to decompression and evacuation of intracranial hematoma operations, and two each of the remaining four underwent an evacuation of intracranial hematoma operation and trepanation and drainage operations, respectively. Five patients agreed to the titanium web-using cranioplasty operation. Four patients with brain tumors (including two gliomas, one meningioma, and one craniopharyngioma) received tumor resection operations. The median time taken to perceive SSIs in extradural SSIs and in intracranial infections post-neurosurgery was 30 days and 10 days, respectively (Table 2).
Surgical and Antimicrobial Treatments and Outcomes in 20 Patients with SSIs After Intracranial Neurosurgery
Etiology examination and antimicrobial treatment
The overall pathogen detection rate was low. Of the 13 patients with extradural SSIs, clear microorganism infections were detected in only 2 of them (Table 2): One was infected with Enterobacter cloacae, and the other with Enterobacter cloacae and Staphylococcus capitis, all of which were sensitive to antibiotic agents such as cephalosporin and levofloxacin. All these patients agreed to an empirical antibiotic therapy (including second- and third-generation cephalosporins, piperacillin–tazobactam, and levofloxacin), with the antibiotic agents adjusted accordingly on the basis of drug sensitivity testing. Of the seven patients with intracranial infections, clear microorganism infections (including two Staphylococcus aureus, one Enterococcus faecium, one extensively drug-resistant Klebsiella pneumoniae, and one Staphylococcus aureus with Pseudomonas aeruginosa) were detected in the CSF of five of them. These patients were given vancomycin and meropenem for at least four weeks, with the antibiotic agents adjusted to polymyxin and meropenem against extensively drug-resistant Klebsiella pneumoniae.
Surgical treatment
All the patients agreed to debridement and VSD (Table 2). Of the five patients with cranioplasty, three consented to titanium web removal because of the severity of infections and lengthy implantation, and two approved of titanium web retention after complete debridement. The bone flaps and bone fixation devices in patients with osteomyelitis and subdural abscesses were removed. Intracranial abscesses were excised and drained. VSD was replaced every 4–7 days, with the median number of VSD used for every patient equaling two, and the median duration for VSD application being 14 days. Five patients with intracranial infections consented to LCD, and one accepted EVD for CSF drainage and the injection of antibiotic agents.
Outcome
After a median follow-up period of 18 weeks (Table 2), all the patients were declared free of infection. Three patients with extradural SSIs died after recurrent glioma, hydrocephalous, and recurrent chronic subdural hematoma, respectively, whereas three patients with intracranial infections died after a prolonged deep coma. No patient died of an infection.
Discussion
This retrospective study examined 20 patients who underwent debridement and VSD to treat SSIs after intracranial neurosurgery. The outcome shows that the deployed standard surgical and antimicrobial treatments effectively controlled and cured the diagnosed pyogenic infections. No patient endured a recurrent infection and/or an infection-related death during follow-up.
Prosthetic implants are an important risk factor for SSIs after first-time neurosurgery.8,24 In this study, all the patients consented to the implantation of medical devices, including a bone flap fixation device, a titanium web, and artificial dura mater. Five (20%) patients with titanium web implants contracted SSIs—a considerable proportion, because the percentage of patients acquiescing in cranioplasty in the department was low. The rates of SSI contractions following cranioplasty differ among investigations, ranging from 5.89% to 9.9%.25–27 Reportedly, the leading causative pathogen associated with neurosurgical implant infections is Staphylococcus aureus. 25 This investigation found that two patients with cranioplasty had defined bacterial infections, including one Staphylococcus aureus and one Enterococcus faecium. The positive rate of bacterial culture in this study was only 35%, with Staphylococcus aureus accounting for the highest proportion, consistent with previous findings.3,10 Hence, preventing SSIs during neurosurgery, especially cranioplasty, requires paying more attention. In a recent study, a low-cost wound healing protocol (consisting of vitamin and mineral supplementations, fluid supplementation, and oxygen support) reduced post-cranioplasty infection rates. 28
Although widely applied against various organ and tissue infections,18,29 VSD has rarely been reported to exert efficacy against post-intracranial neurosurgery SSIs. Allegedly, VSD is potent against primary thoracolumbar spondylodiscitis 30 and SSIs after posterior spinal internal fixation. 19 In this study, the utilization of standard surgical procedure with vacuum-assisted closure (VSD) effectively controlled and treated all patient infections, even in cases where traditional debridement and drainage methods were unsuccessful (Fig. 2). The application of VSD, with an average of two replacements and a duration of 14 days, led to rapid suppression of infections and the formation of new granulation tissue, resulting in shorter hospital stays and cost reduction. Notably, VSD appeared to play a role in reducing intracranial infections without causing excessive CSF loss. Patients with intracranial infections experienced benefits from VSD treatment, possibly because of mechanisms such as improved drainage, enhanced local oxygenation, and better microcirculation facilitated by VSD, as well as its local anti-inflammatory properties. Further investigation is warranted to fully understand these mechanisms. Furthermore, VSD has been shown to reduce the rate of SSIs, 31 particularly after spinal surgical procedure.17,32 Therefore, VSD’s efficacy in preventing SSIs in patients at substantial risk of infection after intracranial neurosurgery requires the attention of scholars.
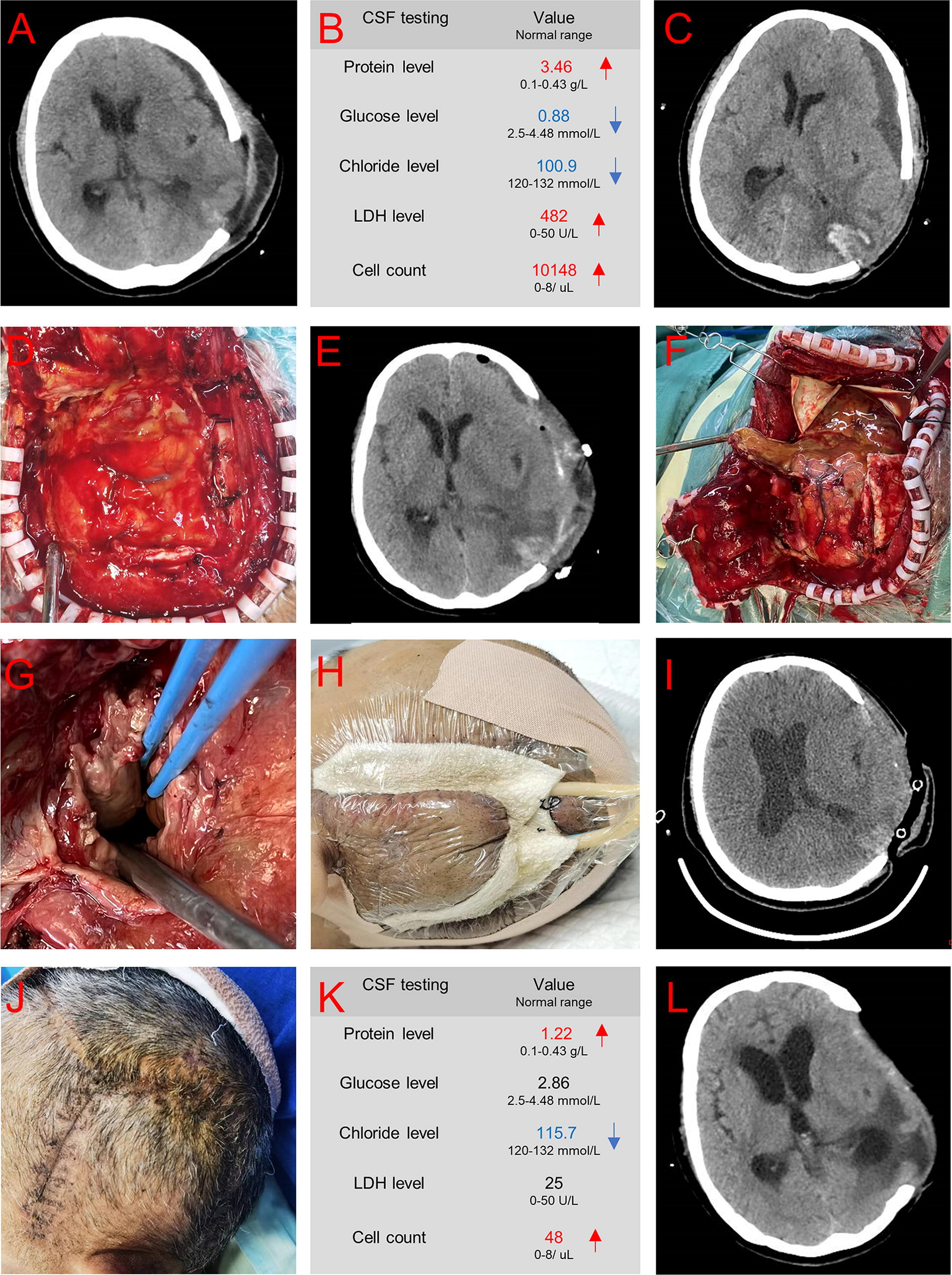
A 54-year-old female patient consented to the decompression and hematoma removal operation 12 days after she was diagnosed with a left temporal lobe hematoma.
Despite the discoveries made in this study, there are a few limitations that need to be acknowledged. First, the research was conducted at a single center and involved a limited number of samples. Second, it was a retrospective observational study that lacked a control group, which hinders the ability to conclusively determine whether the observed high treatment success was solely attributable to the efficacy of VSD. Even though patients who did not respond to conventional therapy eventually recovered after VSD treatment, the absence of a control group complicates the interpretation of these results. Therefore, it is imperative to conduct prospective studies that directly compare the effectiveness of VSD-assisted treatment with traditional approaches in preventing SSIs following intracranial neurosurgery.
Conclusion
VSD is safe and effective against severe post-intracranial neurosurgery SSIs, with short- and medium-term follow-ups confirming its excellent efficacy. To our limited knowledge, this discussion of the effectiveness and outcome of VSD against SSIs post-intracranial neurosurgery is the first of its kind. Prospective controlled studies must, hence, be conducted to confirm the results of this investigation.
Footnotes
Acknowledgments
Sections of this article have been submitted to a preprint platform (https://www.researchgate.net/). This information can be accessed online using a web link (![]() ).
).
Authors’ Contributions
S.R. and Y.L.: Conception and design of the study, collection and/or assembly of data, data analysis and interpretation, and article writing. X.Y.S., Q.W., and X.H.W.: Collection and/or assembly of data. C.M., Z.W.X., Z.L., and R.G.: Provision of study materials and data analysis and interpretation. J.C.C. and W.W.: Conception and design of the study, financial support, and final approval of the article. All authors read and approved the final article.
Data Availability
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Medical Ethics Committee of Zhongnan Hospital of Wuhan University and applied in accordance with the Declaration of Helsinki. The need for informed consent was waived by the Medical Ethics Committee of Zhongnan Hospital of Wuhan university for this retrospective study.
Funding Information
This work was supported by the
Author Disclosure Statement
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices examined in this article. The authors declare that they have no competing interest.