
Abstract
Background:
Pituitary abscess (PA), a rare complication following transsphenoidal (TS) surgery for pituitary adenoma with an incidence of 0.2%, poses a significant risk; carrying potential morbidity, recurrence, and the necessity for reoperation. Timely suspicion, diagnosis, and treatment are imperative.
Patients and Methods:
We present two cases and provide a literature review on the symptoms, risk factors, diagnosis, treatment, and outcomes associated with secondary PAs following TS surgery for adenoma.
Results:
We identified 12 articles reporting a total of 45 cases, in addition to our 2 cases. The primary symptoms were headache and visual impairment, with no fever or specific infectious parameters observed. Predominant risk factors identified included cerebrospinal fluid (CSF) leakage and prior radiotherapy (RT). Our first patient, a 45-year-old male, presented 10 weeks after TS surgery with sudden-onset symptoms, whereas our second patient, a 64-year-old female, presented 22 years postoperatively. In the first case, intraoperative CSF leakage, with the patient’s history of allergic rhinitis and frequent nasal irrigation possibly contributed to the development of abscess. In the second case, RT was considered a potential risk factor. Severe headache and subclinical signs of infection associated with a cystic lesion of the pituitary gland were common findings. Both patients underwent endoscopic TS drainage and received appropriate antibiotic therapy, resulting in complete recovery without recurrence.
Conclusions:
When faced with severe headaches in a patient with a history of TS surgery for a pituitary adenoma, coupled with radiological evidence showing a cystic appearance with peripheral enhancement, taking a proactive approach to promptly identify and intervene in secondary PAs is essential for mitigating potential complications and optimizing patient outcomes.
Introduction
Transsphenoidal (TS) surgery has emerged as the gold standard for pituitary adenoma surgery in the 20st century owing to its minimally invasive nature, rapid recovery time, and improved endocrinological outcomes. 1 However, even in experienced hands at pituitary centers, complications such as rhinologic issues, cerebrospinal fluid (CSF) leakage, vascular or neural injury, endocrine complications, and infections may arise.2,3 Pituitary abscess (PA) represents a rare yet life-threatening entity in the sellar region, and accounts for 0.1%–0.6% of all pituitary lesions. 4 Although two-thirds of PAs are primary, one-third are secondary to pre-existing pituitary lesions such as pituitary adenomas, Rathke’s cleft cysts (RCC), and craniopharyngiomas.5–7 Presently, a history of TS surgery for sellar lesion is recognized as a common risk factor for secondary PAs.6,8 In addition to its association with significant morbidity and mortality, delays in diagnosis and treatment of PA heightens the risk of persistent endocrine abnormalities or visual impairments. 9 Moreover, diagnosing PA remains challenging owing to its nonspecific clinical presentation, radiological findings, inconclusive laboratory tests, and microbiological evaluation. Although reporting our two cases of secondary PA, a rare complication following TS surgery for pituitary adenoma, our goal is to draw attention to the symptoms, risk factors, diagnosis, early treatment, and outcomes associated with this condition.
Patients and Methods
Drawing from the extensive experience of the senior author (N.G.) encompassing 1,805 TS pituitary surgeries over 30 years (1993–2022), we meticulously analyzed the data of our two cases of microbiologically and pathologically proven secondary PA, which manifested following TS surgery for pituitary adenoma. The first case emerged 10 weeks after the procedure, whereas the second case occurred 22 years post-TS pituitary adenomectomy, representing the longest time interval reported in the literature.
Literature search
In addition to reporting our cases, we conducted a comparative analysis with previously reported cases in the literature, delineating the frequency, clinical presentation, laboratory and radiological characteristics, treatment modalities, and outcomes of patients with PA following TS surgery. On November 20th, 2023, we performed a PubMed MEDLINE (National Library of Medicine) search following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 guidelines. 10 Two reviewers (O.B., B.B.A.) independently screened articles for eligibility and a third reviewer (N.G.) resolved any differences. Studies were screened for eligibility using title and abstract. Then, studies underwent a full text review. Data were extracted independently by two reviewers (O.B., B.B.A.).
Inclusion and exclusion criteria
The search utilized the keywords “pituitary abscess” without any limitations on date or article type. Relevant references within captured articles were also scrutinized. Articles written in English were included, whereas those discussing animal subjects were excluded. Furthermore, articles solely focusing on primary PA and abscesses associated with lesions other than pituitary adenomas, such as RCC and craniopharyngiomas, were excluded. Articles describing PA occurring simultaneously within a pituitary adenoma were excluded from our search criteria. Figure 1 illustrates a PRISMA flow diagram summarizing the article inclusion process. In total, 12 articles detailing PA cases subsequent to TS surgery for pituitary adenoma were meticulously analyzed (Table 1).
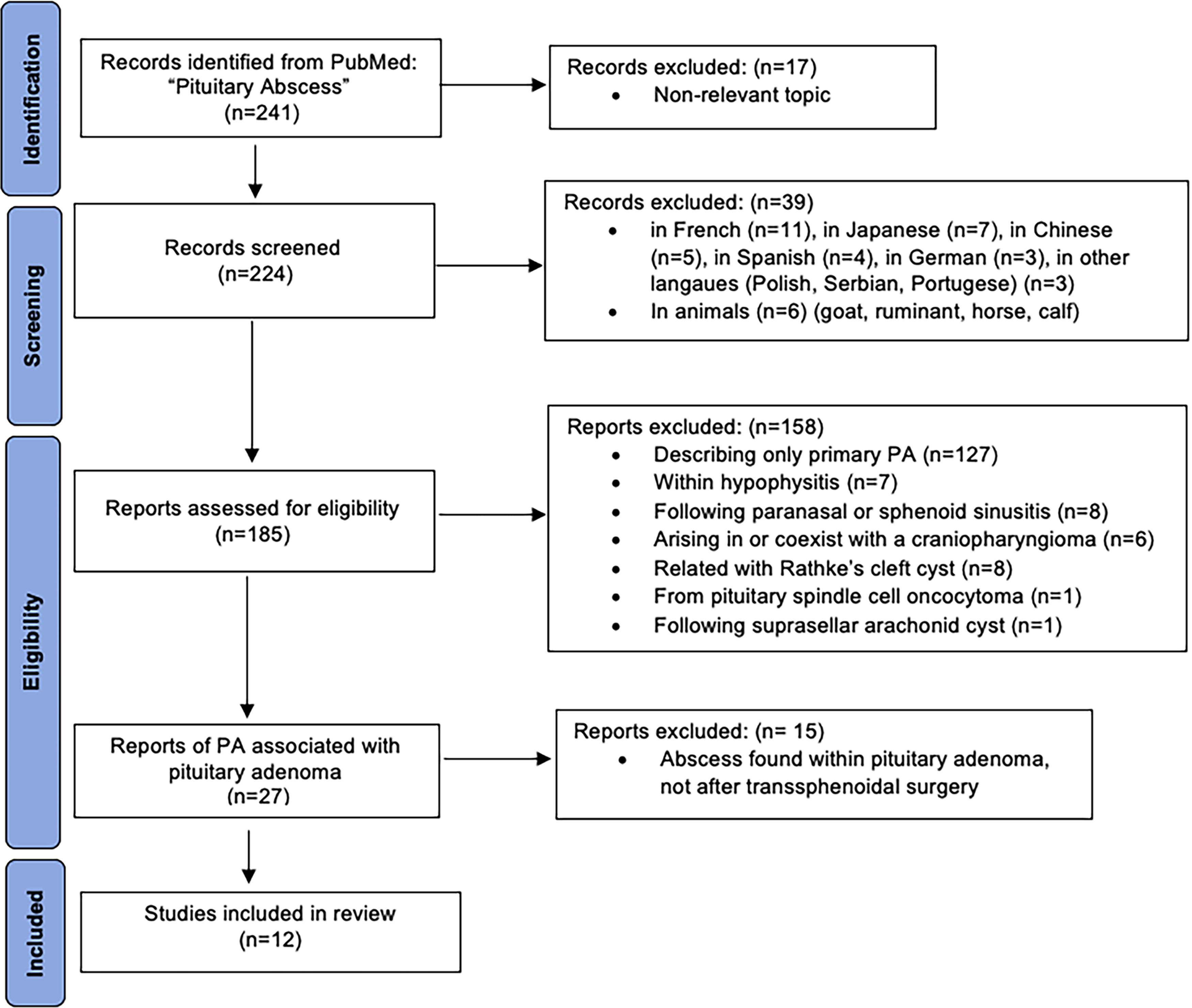
PRISMA flowchart for “Secondary Pituitary Abscess Following Transsphenoidal Surgery for Pituitary Adenoma.”
Pituitary Abscess after Transsphenoidal Surgery for Pituitary Adenoma Reported in the Literature
Time interval between the onset of PA symptoms and first surgery.
Risk factor other than previous TS surgery.
Authors did not specify for each case.
ABX = antibiotics; CRP = C-reactive protein; CSF = cerebrospinal fluid; CT = computed tomography; DI = diabetes insipidus; E2 = estradiol; ESR = erythrocyte sedimentation rate; F = female; GH = growth hormone; HA = headache; HT = hypertension; IGF-1 = insulin-like growth factor-1; LP = lumbar puncture; NA = not available; NF = nonfunctional; M = male; MRI = magnetic resonance imaging; MRSA = methicillin-resistant staphylococcus aureus; MRSE = methicillin-resistant staphylococcus epidermidis; MSSA = methicillin-sensitive staphylococcus aureus; PRL = prolactin; RCC = Rathke’s cleft cyst; RT = radiotherapy; TS = transsphenoidal; TSH = thyroid-stimulating hormone; WBC = white blood cell.
Results
Case 1
A 45-year-old male patient presented to our outpatient clinic in 2014 following an incidental finding of a pituitary macroadenoma (13 × 14 mm × 15 mm) on cranial magnetic resonance imaging (MRI) conducted after a car accident (Fig. 2). Neurological examination, visual acuity, and visual field were normal. Endocrinological evaluation revealed a nonfunctional (NF) tumor (Free thyroxine (fT4): 17.44 pmol/L, thyroid-stimulating hormone (TSH): 2.36 uIU/mL, luteinizing hormone (LH): 4.13 mIu/mL, follicle-stimulating hormone (FSH): 3.98 mIu/mL, cortisol: 11.68 ug/dL, insulin-like growth factor 1 (IGF-1): 123.3 ng/mL). Total testosterone levels were below normal at 2.8 ng/mL (normal range: 2.84–8.0), with slightly elevated prolactin (PRL) at 18.21 ng/mL (normal range: 4.04–15.2). Adrenal and thyroid axes were within normal limits. His medical history included allergic rhinitis because of childhood and prior surgery for a deviated nasal septum. The pituitary tumor, which exhibited a soft consistency, was successfully removed via a binostril endoscopic TS approach. Intraoperatively, CSF leakage was noted, and the tumor cavity was managed with fibrillar surgicele packing, whereas the sellar floor was closed using autologous bone fragments and fibrin glue. During the early postoperative period, the patient reported nasal congestion and difficulty in breathing, likely attributable to a hypersensitivity reaction to fibrine glue. Decongestant therapy was initiated, and postoperative PRL levels decreased to 12.2 ng/mL, whereas free testosterone levels remained low at 2.92 pg/mL (normal range: 8.69–54.69 pg/mL). The patient was discharged on day 4 after surgery. Pathological examination revealed a gonadotroph pituitary adenoma with dura invasion and folliculostellar cell proliferation (GFAP+/s100+), immunopositive for FSH, and LH (Ki-67 1% positive, p53 negative, no mitoses).

Patient 1, first MRI of the pituitary gland (Coronal sections T1-w
Ten weeks post-surgery, the patient presented with severe headache unresponsive to pain medication, accompanied by greenish-yellow nasal discharge. The patient admitted to overusing nasal decongestants, administering them eight times daily. Notably, there was no presence of fever or leukocytosis, with only a slight elevation in C-reactive protein (CRP) levels (0.53 mg/dL) and neutrophil percentage (87.1%). Pituitary MRI revealed a round shaped, rim-enhanced cystic lesion indicative of an abscess associated with pansinusitis (Fig. 3). Emergency reoperation via a binostril endoscopic TS approach revealed congested nasal mucosa and sphenoid sinus filled with fibrin glue. Bone fragments were removed, and the pus-filled cavity was drained. Antibiotics were administered following culture material retrieval. The cavity was washed with isotonic saline solution. The sella floor was not reconstructed. Immediately after surgery, the patient’s headache resolved. The pathology of the lesion consisted of dense lymphocytes, plasma cells, polymorphonuclear lymphocytes, granulation tissue, and necrosis. Microbiology of the pus showed 1–2 leukocytes and many gram-positive cocci. Klebsiella pneumoniae, Streptococcus pneumoniae, and methicillin-sensitive Staphylococcus aureus (MSSA) were cultured. The patient received intravenous antibiotic treatment with ceftriaxone and metronidazole for a duration of six weeks. Postoperative evaluations showed no additional endocrine axis deficiencies. Over eight years of follow-up, the patient remained free of recurrence.

Patient 1, MRI after readmission (Coronal sections T1-w
Case 2
A 42-year-old female patient initially presented to our outpatient clinic in 2000 with a pituitary macroadenoma (20 × 20 mm × 18 mm) invading the left cavernous sinus (Knosp grade IV). Her visual acuity, visual field, and neurological examination were normal. Endocrinological evaluation a NF tumor (Free triiodothyronine (fT3): 4.26 pmol/L, fT4: 7.73 pmol/L, LH <0.50 mIu/mL, FSH: 0.59 mIu/mL, Estradiol (E2): 28 pg/mL, PRL: 808.87 uIU/mL, cortisol <0.20 ug/dL). Gross-total tumor resection was achieved via a sublabial TS microsurgical approach. Pathological examination confirmed a NF pituitary adenoma. In 2001, radiotherapy (RT) was administered for residual cavernous sinus lesion post-surgery. Subsequently, the patient received treatment including steroids, thyroid hormone replacement, and desmopressin owing to panhypopituitarism and diabetes insipidus.
After 22 years of progression-free follow-up, the patient sought urgent care at another center owing to complaints of headache and dizziness. Visual acuity and visual fields remained normal. Hyponatremia was detected and managed symptomatically. Hormonal assessments revealed NF status (Cortisol: 4.41 ug/dL, PRL: 5 µg/L, IGF-1: 79 µg/L, growth hormone [GH]: 0.03 ng/mL, ACTH: 2.09 pg/mL, TSH: 0.01 mU/L, fT4: 16 ng/L, fT3: 1.85 ng/L, FSH <0.3 U/L, LH: 0.78 U/L). Hyponatremia was attributed to inadequate steroid replacement during a urinary tract infection, prompting the initiation of steroid coverage. Post-treatment, control levels reached 15.6 µg/L. Pituitary MRI revealed a cystic degenerating recurrent macroadenoma-like lesion on the left half of the pituitary gland (11 × 13 mm × 12 mm, central cystic periphery solid-enhancing) (Fig. 4). The patient’s white blood cell (WBC) count was 7450/µL, erythrocyte sedimentation rate (ESR) was 24 mm/h (normal range: 0–20 mm/h), and CRP level was 35.41 mg/dL. Suspecting a recurrent, fast-growing tumor or PA owing to suspicious MRI findings and clinical characteristics, the patient was referred to our center for further evaluation. Undergoing early endoscopic TS surgery, the pus-filled tumor cavity was drained, and it was washed with an isotonic saline solution. Antibiotics were withheld until material for culture was obtained. Pathological examination revealed evidence of acute and subacute inflammation in a focal area with fungal hyphae and spores in an isolated fragment (Fig. 5). MSSA was cultured, leading to a six-week postoperative course of ceftriaxone, metronidazole, and vancomycin.

Patient 2, MRI of the pituitary gland after readmission (Coronal sections T1-w
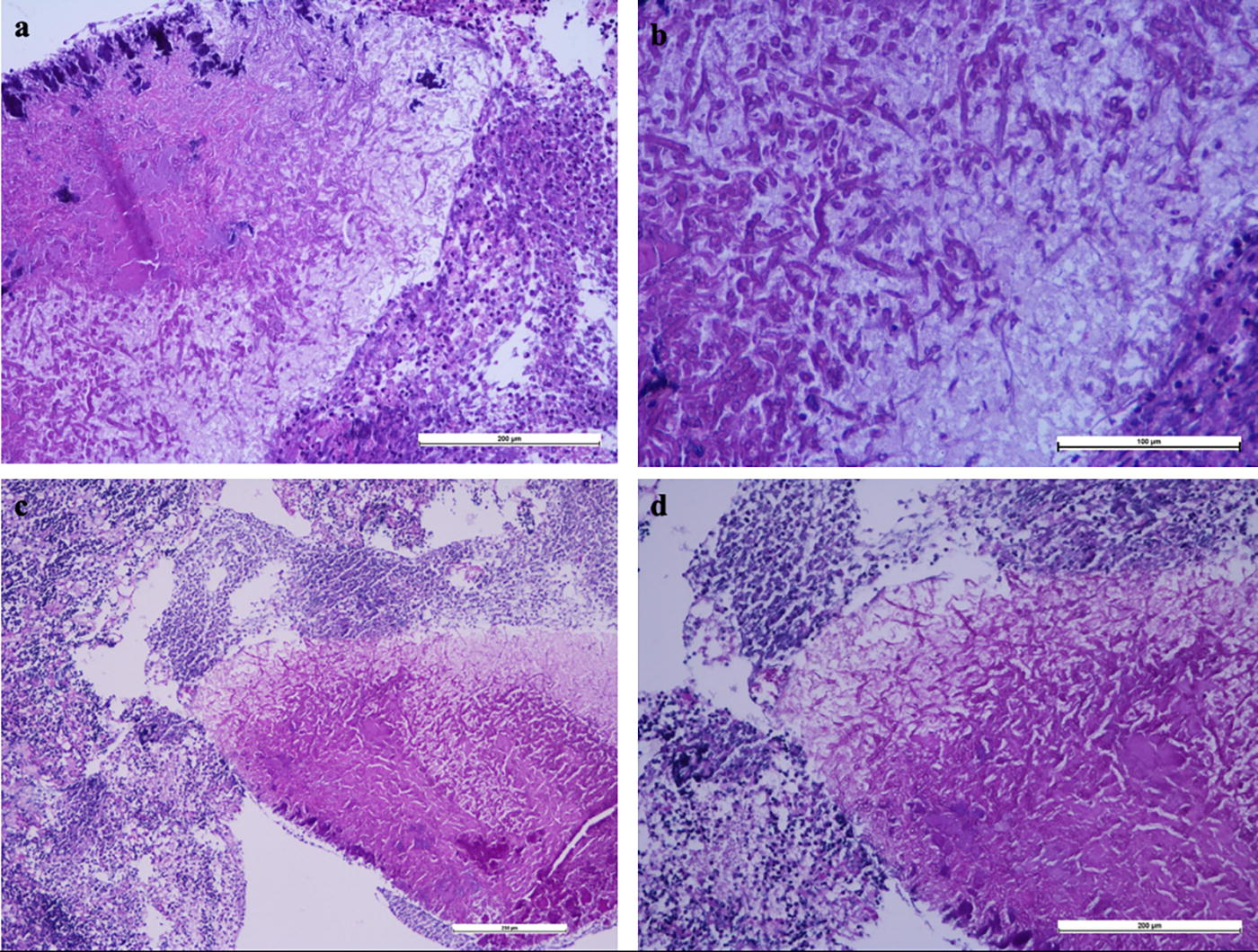
Abscess areas and fungal hyphae with Hematoxylin and Eosin (H&E) (
Discussion
PAs are rare entities in the sellar region. 19 Although two-thirds of PAs are primary, one-third are secondary to pre-existing pituitary lesions such as pituitary adenomas, RCC, and craniopharyngiomas.1,5,6,13 A history of pituitary surgery is also recognized as a common risk factor for secondary PAs.6,8,20 Vates et al. conducted a review spanning 30 years, identifying 24 PA cases among 3,500 patients who underwent surgery for pituitary disorders, with secondary PA occurring in 10 patients previously operated for pituitary or sphenoid sinus disease (including 6 patients with pituitary adenoma). 6 Gao et al. reported 66 PAs in 6,361 consecutive patients (1.04%) undergoing pituitary disease surgery over 23 years (46 primary, 20 secondary). 21 Wang et al. documented 12 cases of PA following TS surgery over an 11-year period, 5 whereas Li et al. presented 23 cases of secondary PA after TS surgery over 14 years. 22 Although Wang et al. did not provide the total number of cases, Li et al. calculated the incidence of secondary PA after TS surgery at 0.34% (23 cases among 6,832 patients, including 8 RCC, 11 NF pituitary adenoma, and 4 somatotropic adenoma cases). Therefore, the incidence of secondary PA after TS surgery for pituitary adenoma ranges from 0.17% to 0.22% (6 of 3,500 patients in Vates et al., 15 of 6,832 patients in Li et al.). The two cases presented here serve as illustrations of secondary PAs within the reporting neurosurgeon’s 30 years of experience, which included 1,805 patients; the incidence in our series was 0.11%.
By reviewing the literature, the total number of PA cases following TS surgery for pituitary adenoma is 47, including our cases (Table 1). The age distribution of cases ranged from 19 to 70 years, with an average of 44.12 years. Out of these cases, 25 were women and 16 were men (Vates et al. did not specified their 6 cases gender of patients). 6 The initial pathology of the adenoma was reported as NF and GH secreting or somatotropic adenomas, with authors using both historical and contemporary histological classifications.1,11,12,18 Some recent articles omit the histological classification of the initial adenoma post-TS surgery. Given the focus of this article on PA after TS surgery for pituitary adenoma, cases categorized as secondary PA by Gao et al. were excluded owing to the lack of specified primary pathology and time intervals between PA symptom onset and initial surgery. 21 The interval between secondary PA diagnosis and prior TS surgery for pituitary adenoma ranged from 20 days to 8 years.5,14,17,22 Approximately half of secondary PAs manifested within six months post-surgery. 22 Consistently, our first patient presented with PA symptoms 10 weeks after endoscopic TS surgery, whereas the second patient presented 22 years postoperatively, representing the longest delay reported to date. 14 One could say that it is easier to assess early-onset PA than late-onset cases. Regardless of the time elapsed post-surgery, timely diagnosis remains paramount.
Primary PAs may stem from direct extension from paranasal sinuses, meningitis, cavernous sinus thrombosis, or hematogenous spread.6,9,23 Previous TS pituitary surgery emerges as the primary risk factor for secondary PAs. 22 Structural disruptions in the sphenoidal sinus and sella floor, along with compromised immune defenses in the sella turcica, may facilitate infection spread.1,15 Iatrogenic retrograde infection from the sphenoid sinus to the sella region is posited as the primary mechanism for PA post-TS surgery. 5 Risk factors include sphenoidotomy size, postoperative nasal care frequency, reactions to foreign bodies, prior CSF leak, cavernous sinus thrombosis, postoperative meningitis, and patient comorbidities.1,8,14,24–27 RT may also contribute, possibly by affecting bone or fat grafts used for sellar defect reconstruction. 28 Notably, only our first patient had a history of intraoperative CSF leak, whereas in his case excessive postoperative nasal care may have contributed to the development of PA. The second patient’s PA may be linked to RT, albeit inconclusive.
Headache is the most common secondary PA symptom, 9 occurring in 69.7% to 92% of cases.8,9 Headache characteristics range from mild to severe. 5 Visual impairments or visual field defects and endocrine dysfunction are the other main symptoms.15,21 Wang et al. found that 7 of 12 patients (58%) diagnosed with panhypopituitarism had various clinical manifestations, whereas 6 of 12 patients (50%) in their case series complained of visual impairments. Stringer et al. performed a comprehensive systemic review of PA and found that visual disturbances occurred in 47.3% of PA. 9 In this review, the most common endocrine abnormality was panhypopituitarism (41.1%), followed by diabetes insipidus (24.8%), whereas only 15.5% of PA patients had normal endocrinological tests. Interestingly, in a very recent publication, Zhuang et al. 16 found hypopituitarism (15 of 15 cases, 100%) to be the most common symptom in their 15 cases of PA, followed by headache (14 of 15 cases, 93.3%), sinusitis (8 of 15 cases, 53.3%), and visual field loss (6 of 15 cases, 40%). Our first case showed acute signs of nasal discharge and headache with subclinical signs of infection. The second patient, who suffered from severe headache, was initially found to have hypocortisolemia and hyponatremia during an urinary tract infection. Our two patients did not develop new-onset hypopituitarism or visual impairment due to PA.
PA diagnosis proves challenging owing to nonspecific clinical and radiological findings and inconclusive microbiologic evaluation. 27 Fever, elevated CRP, or leukocyte counts lack sensitivity for PA detection.5,9 Only half of the patients with PA have the signs of infection. 9 In our first patient, only the neutrophil granulocyte percentage was elevated, whereas the other infection parameters were within normal limits. Our second patient also had only a slight increase in CRP and ESR. Classical PA MRI features include a sellar cystic or partially cystic mass, hypointense or isointense on T1-weighted imaging, and hyperintense or isointense on T2-weighted imaging with peripheral ring contrast enhancement after gadolinium injection. 5 However, these features may vary, leading to misdiagnosis. 9 Signal intensity may vary depending on the characteristics of the abscess, such as protein or hemorrhage. Or, because, it is a rare entity, an abscess may not be directly suspected. In our cases, MRI initially suggested cystic recurrent adenoma or RCC, underscoring the need for suspicion given prior TS surgery. Besides, there are no well-established criteria for a conclusive preoperative diagnosis. However, new imaging techniques, such as nuclear medicine modalities (18-FDG PET scan), could be promising in the near future. 27
Diagnosis typically occurs intraoperatively via purulent material culture, 29 yet microbiological cultures exhibit low sensitivity (about 54.8%).6,9 Wang et al. 5 isolated the causative organism in only 5 of 12 patients (42%), whereas Zhuang et al. 16 found a culture-positive rate of 33.3%. Gao et al. found different gram staining or bacterial cultures positivity rate between primary PA (6 positive in 46 primary PA, 13%) and secondary PA (7 positive in 20, 35%). 21 The absence of preoperative suspicion, preoperative antibiotic use, and inadequate collection of pus material could account for negative microbiological cultures. However, contrary to these findings in the literature, both of our patients exhibited bacterial growth, guiding tailored antibiotic therapy on the basis of these culture, and antibiotic sensitivity profiles. It is advisable to initiate antibiotic treatment only following the collection of cultures in cases of clinical suspicion. In our cases, antibiotics were withheld until material for culture was obtained. At this point, to reach conclusive microbiological testing, our suggested optimized approach is to perform surgery early and avoid administering empirical antibiotics, including prophylactic use, before surgery. In addition, commencing intravenous antibiotic therapy post-TS surgery and adjusting treatment on the basis of microbiological culture results is a prudent approach.
The most common bacterial organism in secondary PA is Staphylococcus aureus and the most common fungal organism Aspergillus. 9 Kobayashi et al. reported three cases of Streptococcus pneumonia meningoencephalitis after TS surgery with a prevalence of 0.15% (3 in 1,965 patients). In the series of Gao et al., the main pathogenic microorganism in secondary PA was Aspergillus fumigatus while Gram-positive or Gram-negative bacteria in primary PA. 21 In our first case, Klebsiella pneumoniae, Streptococcus pneumoniae, and MSSA were identified, whereas the second case presented MSSA and fungal infestation.
There is no consensus on the treatment approach for secondary PA. Treatment recommendations typically involve TS drainage using endoscopic or microsurgical techniques, along with microbiology-guided antibiotic therapy. 14 Presently, the endoscopic approach is favored owing to its minimally invasive nature, enabling both diagnosis and treatment. 15 Timely TS surgery is imperative for favorable outcomes, with complete cure rates estimated at around 60%. Approximately, 30% of cases recover after a combined approach involving surgical and medical treatments targeting hormonal or visual impairment. 6 Although some medical centers prefer a 1–2 week course of intravenous antibiotic therapy followed by oral antibiotics for 2–4 weeks, we opted for a six-week intravenous antibiotic regimen post-surgery. The various antibiotic treatment regimens used for secondary PA after TS surgery for pituitary adenoma cases are summarized in Table 1. For empirical broad-spectrum antibiotic therapy, intravenous third-generation cephalosporins or a combination of ceftriaxone and vancomycin is most commonly used in different clinics. 16
Recurrence rates of PA have been reported to be as high as 20%.5,22 However, considering ourselves fortunate, the follow-up of our two cases remained free of recurrence. In some instances, recurrence may necessitate a second or third operation, or RT may be administered to the patient.1,5 Better outcomes or full recovery can be achieved through timely suspicion, diagnosis, and treatment. Primary objective is to minimally intervene while restoring hormonal levels to baseline. 30 These patients often require long-term hormone replacement therapy for hypopituitarism. 8 Moreover, if the patient presents with clinical visual impairment, delays in abscess drainage could result in persistent visual disturbances. 1 Therefore, prompt intervention is essential to mitigate such risks and achieve optimal outcomes.
Conclusion
The incidence of secondary PA after TS surgery for pituitary adenoma is about 0.2%. PA may develop 20 days to 22 years after TS surgery. Diagnosis is difficult due to nonspecific clinical and radiological findings and inconclusive microbiologic evaluation, as it may manifest without fever or specific infectious parameters. Timely suspicion, diagnosis, and accurate treatment are imperative given its potential complications, such as permanent hormonal deficiencies or visual impairment. Therefore, when encountering severe headache alongside a history of TS surgery for a pituitary adenoma, coupled with a cystic appearance featuring peripheral contrast enhancement on radiological imaging, prompt consideration, and action toward an abscess are warranted. To obtain a conclusive microbiologic examination, we recommend early reoperation surgery and avoiding the administration of empirical antibiotics before surgery. This proactive stance ensures timely intervention, aiding in mitigating potential complications and optimizing patient outcomes.
Statement of Ethics
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Ethical approval is not required for this study in accordance with local or national guidelines.
Footnotes
Data Availability
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Authors’ Contributions
O.B. and N.G.: Study conception and design. B.B.A., F.D., S.K., and N.G.: Material preparation and data collection. S.K.: Radiological data. H.K.: Microbiological data. O.B., S.K., H.K., S.K., and N.G.: Analysis and interpretation of results. O.B., B.B.A., and N.G.: Draft article preparation. N.G.: Critical revision of the article. S.K. and N.G.: Study supervision. All authors reviewed the results and approved the final version of the article.
Funding Information
The authors of this study stated that they did not receive any financial support.
Author Disclosure Statement
The authors state that there is no conflict of interest regarding this article.