
Abstract
Introduction:
Total cystectomy and hepatectomy are the main radical surgical procedures for hepatic cystic echinococcosis (CE). When CE lesions severely invade intrahepatic biliary ducts and vessels or single or multiple lesions occupy one hepatic lobe, performing total cystectomy is not indicated. This study aimed to analyze the clinical efficiency of anatomical hepatectomy in the treatment of patients with hepatic CE.
Methods:
Clinical data of 74 patients with hepatic CE who received anatomical hepatectomy were retrospectively analyzed from January 2005 to January 2022. The patients were classified into the intrahepatic biliary duct invasion group (group A), the intrahepatic vessel invasion group (group B), and the hepatic lobe occupation group (group C).
Results:
Among these 74 patients who received anatomical hepatectomy, right hepatectomy was performed in 20 cases (27.03%), left hepatectomy in 26 cases (35.13%), right posterior lobectomy in nine cases (12.16%), and left lateral sectionectomy in 19 cases (25.68%). Short-term post-operative complications occurred in seven cases (9.50%), including abdominal abscess in one case, pleural effusion in three cases, intestinal obstruction in one case, incision infection in one case, and ascites in one case. Long-term post-operative complications occurred in four cases (5.4%), including recurrences of CE in two cases and incisional hernias in another two cases. There were no statistical differences in the concentrations of total bilirubin, alanine aminotransferase, and aspartic transaminase before and after surgery between groups (p > 0.05). However, differences in operative time, short-term post-operative complications, average hospital stay, and number of open hepatectomy cases were statistically significant between groups (p < 0.05). The differences in cases receiving hepatic portal occlusion, intra-operative blood loss, and intra-operative blood transfusion were not statistically significant between groups (p > 0.05).
Conclusions:
Anatomical hepatectomy is an effective and feasible surgical procedure for patients with hepatic CE with severe invasion of intrahepatic biliary ducts and vessels or patients with huge lesions occupying one hepatic lobe, which effectively avoids residual cavity-related complications.
Post-operative complications, notably biliary leakage and recurrence of cystic echinococcosis (CE), present significant challenges in the management of patients with hepatic CE following surgery. Total cystectomy, a radical surgical approach for the treatment of CE lesions, has been shown to substantially mitigate these complications. This procedure, by meticulously removing the entire cyst, offers a promising tactic in reducing the incidence of both biliary leakage and CE recurrence, which are among the primary post-operative concerns in patients with hepatic CE.1,2 In clinical practice, the feasibility of total cystectomy for CE is limited by the size and location of cysts, rendering this approach suitable for only a select few cases. Consequently, subtotal cystectomy has emerged as the predominant surgical technique. Despite efforts to detect and suture biliary leakage in the residual cavity by injecting methylene blue into the cystic duct during the procedure, refractory complications, including persistent biliary leakage and infection of the residual cavity, continue to afflict some patients.3–5 These complications are particularly challenging in instances where the leakage is proximal to the porta hepatis, leading to post-operative hepatic alterations such as hyperplasia, hypertrophy, and atrophy. Such changes can induce rotation of the porta hepatis, resulting in severe hilar biliary duct stricture and intrahepatic calculosis. Consequently, these post-operative complications significantly complicate the management of patients with hepatic CE upon readmission, 6 presenting a formidable challenge to the medical staff tasked with their care.
Our department, a leading center for the treatment of patients with hepatic (CE), has consistently prioritized the management of post-operative complications. Drawing on our extensive clinical experience, we have observed that hepatectomy significantly diminishes the incidence of these complications. This retrospective study, therefore, seeks to analyze the clinical characteristics and outcomes of 74 patients with hepatic CE who underwent hepatectomy between January 2005 and January 2022 in our department. The findings aim to serve as a reference for medical professionals when addressing similar cases in their clinical practice, thereby enhancing patient care and outcomes.
Methods
Ethics
Design of this study was in accordance with the Helsinki Declaration and approved by the Human Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University. Informed consent for their data collection and publication was obtained from all patients in their native language. Patients under the age of 18 were not included in this study.
Study subjects
A retrospective analysis involving 1,355 patients with hepatic CE who received surgical treatment from January 2005 to January 2022 in our department was conducted in this study. Study subjects were selected according to the following eligibility indications: (i) Diagnosis of hepatic CE was clearly determined through pre-operative abdominal ultrasound (US), computed tomography (CT), and post-operative histological findings of surgical specimens; (ii) patients whose CE lesions were >5 cm in size; (iii) patients who received anatomical hepatectomy; and (iv) patients with complete clinical data. On the contrary, patients were excluded from the study according to the following criteria: (i) Patients complicated with other organ CE, (ii) patients with hepatic CE who received hepatectomy because of post-operative complications, and (iii) patients who received partial hepatectomy.
In this cohort, surgical interventions for hepatic CE varied, with endocystectomy performed in 998 cases, total cystectomy in 283 cases, and anatomical hepatectomy in 74 cases. The anatomical hepatectomy group comprised 36 male and 38 female patients, ranging in age from 12 to 68 years, with a median age of 39 years. The clinical manifestations among these patients included abdominal pain in 31 cases, fever in two cases, and jaundice in three cases, whereas the remaining 38 cases were diagnosed with hepatic CE during physical examinations. Primary hepatic CE was identified in 39 patients, whereas recurrent hepatic CE was observed in 35 patients. The distribution of CE cysts showed that 52 patients had a single CE cyst, and 22 patients had multiple CE cysts. Utilizing the World Health Organization Informal Working Group on Echinococcosis international US classification system, the cysts were categorized as follows: CE1 in nine cases, CE2 in 45 cases, CE3 in four cases, CE4 in 15 cases, and CE5 in one case.
Pre-operative assessment
Pre-operative US, enhanced CT, magnetic resonance imaging (MRI), magnetic resonance cholangiopancreatogrphy (MRCP), and echinococcus-specific antibody detection tests were performed to make a pre-operative diagnosis. Among these patients, 27 cases were positive for specific echinococcus antibody, and 15 cases were negative. Echinococcus-specific antibody detection test was not performed in 32 cases. In addition, CE lesion size, location, involvement of adjacent vessels, biliary ducts, and distal liver atrophy were determined through enhanced CT and MRCP. Pre-operative imaging demonstrated that there was distal liver atrophy in 22 cases. Typical imaging is shown in Figure 1.
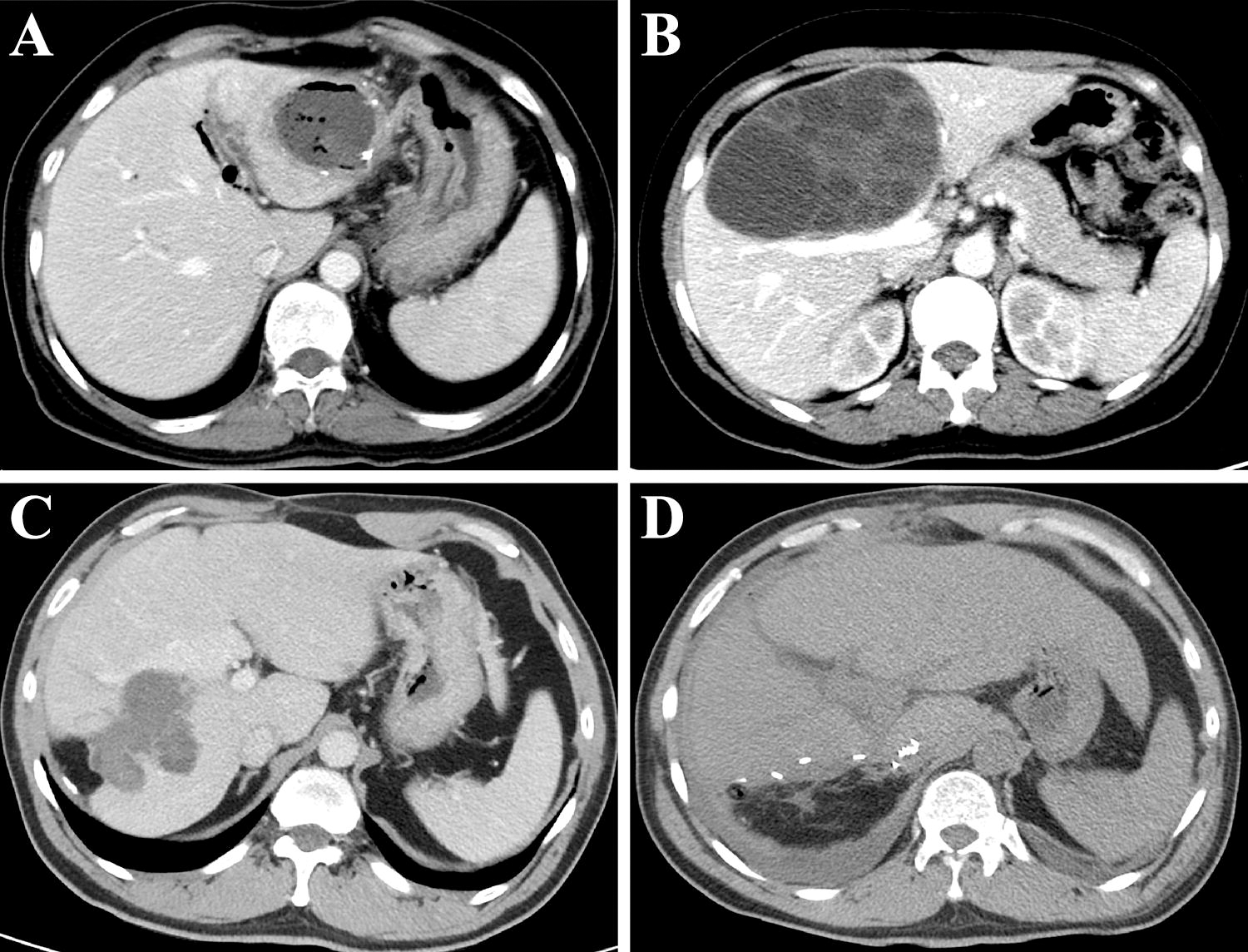
Typical imaging pictures.
Surgical procedures
In this study, 74 patients underwent anatomical hepatectomy for hepatic CE, with the procedures distributed as follows: right hepatectomy in 20 cases, left hepatectomy in 26 cases, right posterior lobectomy in nine cases, and left lateral sectionectomy in 19 cases. The hepatectomies were categorized into open (30 cases) and non-open (44 cases) approaches.
For the open hepatectomy group, the surgical protocol was meticulously designed to minimize post-operative complications. Initially, the surgical area was safeguarded with hypertonic saline gauze. An endocystectomy was performed, followed by the thorough management of the residual cavity using 10% hypertonic saline. The hepatic tissue designated for removal was then identified. Subsequent steps involved the dissection of the porta hepatis, ligation of the hepatic artery, and portal vein branches of the targeted hepatic lobe. The removal of hepatic tissue was executed along the ischemia line, employing either the wallet method or a cavitation ultrasonic surgical aspirator knife, with the hepatic vein being resected thereafter. Following cholecystectomy, the cystic duct was located, and a drainage tube was inserted and ligated. To identify any biliary leakage, methylene blue solution was injected into the biliary duct, with immediate suturing performed in cases of leakage. In instances of multiple CE lesions, a subtotal cystectomy was conducted.
The non-open hepatectomy procedures were similarly comprehensive but tailored for minimally invasive approaches. After determining the hepatic lobe for resection via pre-operative imaging, the same sequential steps of porta hepatis dissection, vessel ligation, tissue excision, and cholecystectomy were followed. Biliary leakage tests using methylene blue solution and subsequent suturing for leaks were also integral to this approach (Figure 2).

Intra-operative photos.
Among these patients, 14 cases with multiple CE lesions underwent endocystectomy and cholecystectomy. In addition, nine patients experiencing rupture of hepatic CE cysts into the biliary tract received a combination of cholecystectomy, common biliary duct exploration, and T-tube drainage. Biliary leakage, whether in the hepatic wound or residual cavity, was promptly addressed with suturing in all patients. This comprehensive approach to both open and non-open hepatectomy underscores our commitment to minimizing the risk of post-operative complications and ensuring the meticulous management of hepatic CE.
Method and content of follow-ups
Patients underwent follow-up through both telephone consultations and outpatient visits, scheduled at six-month intervals during the initial post-operative year and subsequently on an annual basis from the second year onwards. The duration of follow-up ranged from 1.9 to 18.5 years, with a median follow-up period of 11.8 years.
The follow-up assessments included abdominal US or CT scans. It was imperative that the examining physician was briefed on the patient’s history of CE treatment prior to conducting the examination. During these follow-ups, patients were monitored for any signs of recurrence or the emergence of other long-term complications post-surgery.
Statistical analysis
To summarize the characteristics of the patients, a descriptive approach was employed. The statistical analyses were conducted using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA) and GraphPad Prism 8.0 (GraphPad Software, San Diego, CA, USA). Quantitative data were presented as mean ± standard deviation. For statistical comparisons between groups, Student’s t-test and one-way analysis of variance were utilized. A p-value of <0.05 was considered to indicate statistical significance, with the significance threshold set at the 5% concentration.
Results
Causes of classification and characteristics of different group patients
The study classified 74 patients with hepatic CE who underwent hepatectomy into three groups on the basis of pre-operative clinical symptoms, imaging studies, and intra-operative findings: the intrahepatic biliary duct invasion group (group A), the intrahepatic vessel invasion group (group B), and the hepatic lobe occupation group (group C).
Intrahepatic biliary duct invasion group (group A): This group comprised 29 patients whose CE cysts had invaded the biliary duct of one hepatic lobe, as determined by pre-operative symptoms, enhanced abdominal CT, and MRCP. Anatomical hepatectomy was performed. Clinical manifestations before surgery included abdominal pain in 16 patients, fever in two, and jaundice in four. Distal liver atrophy was observed in 16 patients, with five experiencing intrahepatic calculi. Invasion occurred in the left hepatic lobe biliary duct in 14 patients, the right hepatic lobe duct in 11, and the right posterior hepatic lobe duct in four. Biliary fistulae in the residual CE cyst cavity were noted in 24 patients, with nine cases exhibiting rupture into the biliary tract. In addition, fibrosis and calcification of the CE cyst wall were present in 14 patients. Surgical interventions included left hepatectomy in 13 patients, left lateral sectionectomy in one, and right hepatectomy in all 11 patients with right lobe involvement. Right posterior lobectomy was performed in four cases. Open hepatectomy was conducted in 23 cases, whereas six underwent a non-open approach. Short-term post-operative complications were noted in four patients, with long-term complications in three, including two recurrences of hepatic CE and one incisional hernia.
Intrahepatic vessel invasion group (group B): Fifteen patients underwent anatomical lobectomy because of CE cyst invasion into intrahepatic vessels, with no specific pre-operative symptoms reported. Enhanced CT or MRI revealed left portal vein invasion in three cases, right portal vein in one, left hepatic vein in nine, and right hepatic vein in two, with notable cyst wall calcification in two cases. Surgical approaches included open right hepatectomy for cases involving the right portal or hepatic vein. Left hepatectomy was performed in two patients with left portal vein involvement and left lateral sectionectomy in one. Among those with left hepatic vein invasion, three underwent left hepatectomy and six had left lateral sectionectomy. Post-operatively, pleural effusion was observed in one patient, with no long-term complications reported.
Hepatic lobe occupied group (group C): This group consisted of 30 patients with single or multiple CE cysts occupying one hepatic lobe, confirmed through pre-operative enhanced CT or MRI, with no specific symptoms. Fibrosis or calcification of the CE cyst wall was present in 10 patients. Surgical procedures included open hepatectomy in one patient and non-open approaches in 29. Specifically, right hepatectomy was performed in six cases, left hepatectomy in nine, left lateral sectionectomy in 10, and right posterior lobectomy in five. Short-term complications included ascites in one patient and pleural effusion in another, with one case of incisional hernia as a long-term complication.
Intra-operative conditions
The operative duration for all patients averaged 220 min, with the mean volume of blood loss recorded at 225.7 mL. Blood transfusions were necessitated for 10 patients, amounting to a total transfusion volume of 37 units. Furthermore, during the hepatectomy procedure, hepatic portal occlusion was performed at various times in 14 patients.
Post-operative complications
Following the surgical procedures, a biliary fistula was not observed in any of the patients. During their hospitalization, a minority of patients (n = 7, 9.5%) experienced short-term post-operative complications. Specifically, an abdominal abscess was identified in one patient, which significantly improved following puncture and drainage under US guidance, coupled with anti-inflammatory treatment. Pleural effusion was diagnosed in three patients, all of whom received puncture and drainage under US guidance as well. One patient with intestinal obstruction improved with conservative treatment and was subsequently discharged. In addition, surgical site infection was reported in one patient, who was treated with anti-inflammatory medication and received fresh wound dressings. Conservative treatment was also administered to one patient who developed post-operative ascites.
In terms of long-term post-operative complications, they were reported in four patients (5.4%). Among these, one patient passed away due to a disease unrelated to the surgery. Out of the total cohort, 69 patients were successfully followed up, whereas four (5.4%) were lost to follow-up. Recurrence of CE was detected in two patients (2.7%) through follow-up US or CT scans, necessitating reoperation. The recurrence was confirmed by post-operative pathological examination. In addition, two patients developed incisional hernias and underwent surgical repair, with satisfactory recovery post-surgery.
Comparison of pre-operative, intra-operative, and post-operative parameters
Through analyzing main laboratory tests and liver function indices, it was demonstrated that there were no significant differences in the concentrations of total bilirubin, alanine aminotransferase (ALT), and aspartic transaminase (AST) before and after surgery (p > 0.05). However, there were statistical differences in the concentrations of white blood count (WBC), hemoglobin (Hb), and albumin before and after the operation (p < 0.05).
In the comparative analysis of pre-operative general data among the groups, no significant differences were observed (p > 0.05). However, a detailed examination of main laboratory tests and liver function indices before and after surgery revealed a significant disparity in pre-operative ALT concentrations among the groups (p < 0.05), with the intrahepatic biliary duct invasion group exhibiting greater pre-operative ALT concentrations compared with the other two groups. Conversely, the concentrations of WBCs, Hb, AST, albumin, total bilirubin, and post-operative ALT did not differ significantly across the groups (p > 0.05).
Statistically significant differences were noted in operative time, short-term post-operative complications, average hospital stay, and the number of open hepatectomy cases between the groups (p < 0.05). Specifically, the intrahepatic biliary duct invasion group had a higher incidence of open hepatectomy, which correlated with longer operative times, extended hospital stays, and an increased frequency of post-operative complications compared with the other groups. In contrast, the occurrence of hepatic portal occlusion, intra-operative blood loss, and the necessity for intra-operative blood transfusion did not show statistical significance between the groups (p > 0.05). These findings are detailed in Tables 1–3.
Clinical Characteristics of the Study Participants
CE = cystic echinococcosis; SD = standard deviation.
Intra-Operative Parameters
Laboratorial Analysis
ALT = alanine aminotransferase; AST= aspartic transaminase; Hb = hemoglobin; WBC = white blood count.
Discussion
Endocystectomy, a traditional surgical approach for treating hepatic CE, is recognized for its simplicity and safety. This method’s accessibility makes it a viable option for implementation in primary healthcare facilities. Despite its advantages, the procedure often results in the formation of a post-operative residual cavity, frequently complicated by a biliary fistula, presenting a significant challenge.7,8 Studies have indicated that the incidence of post-operative complications, including infections of the residual cavity, effusion, and biliary leakage, remains high following endocystectomy, causing considerable distress to patients.5,9,10 In response, various surgical modifications have been developed, achieving notable advancements.1,11–13 Total cystectomy, in particular, has emerged as a superior alternative, offering minimal damage to the host liver while preserving the surrounding intrahepatic biliary ducts. Furthermore, this technique effectively eliminates the residual cavity, significantly reducing the occurrence of stubborn complications associated with it.14–16 Consequently, the therapeutic outcomes of total cystectomy in patients with hepatic CE have been highly satisfactory.
In clinical practice, the management of hepatic CE presents significant challenges, particularly when cysts are centrally located, exerting pressure on the larger intrahepatic blood vessels and biliary ducts near the porta hepatis during their prolonged growth. This compression affects not only the CE cysts but also the surrounding normal or atrophic liver tissues, which are closely associated with these vessels and ducts. Situations often arise where multiple cysts or a large single cyst nearly occupies an entire hepatic lobe, with some normal or atrophic liver tissues present at their distal ends. In such cases, the intimate adhesion between CE cysts and the surrounding blood vessels and biliary ducts renders complete cyst removal highly improbable. Improper execution of endocystectomy may lead to the formation of an inverted reverse Ω-shaped residual cavity between the liver tissues, resulting in unsatisfactory outcomes for residual cavity drainage and a propensity for complications, such as residual cavity infection, subsegmental abscess, and pulmonary infection. Furthermore, fibrosis or calcification of the residual cavity wall complicates the management of biliary leakage, potentially leading to persistent biliary leakage or sinus formation.2–4
Recent studies have highlighted that post-operative biliary leakage from the residual cavity can induce contraction of said cavity, potentially causing severe complications such as hilar biliary duct stenosis, distal liver atrophy, and intrahepatic calculi. 6 Patients with such complications should not be simply treated for hepatic CE; rather, they should be considered as suffering from potentially life-threatening complex hepatobiliary diseases. 7 From our perspective, patients with hepatic CE with complex conditions require pre-operative evaluation to facilitate simultaneous treatment of the invaded biliary ducts and blood vessels through anatomical hepatectomy. Although theoretically, the risk of intra-operative bleeding and other serious complications during hepatectomy may be higher compared with endocystectomy, several studies have reported findings that contradict this assumption.8,11,17 Anatomical hepatectomy, commonly employed for hepatic tumors, can also be considered a viable treatment option for hepatic CE cysts, especially when these cysts invade intrahepatic biliary ducts, blood vessels, or occupy an entire hepatic lobe.
The surgical management of hepatic CE remains a subject of debate, with no consensus on the specific indications for hepatectomy.17,18 Ramia et al., through an analysis of 49 cases, suggested that indications for major hepatectomy in hepatic CE include extensive hepatic involvement, significant biliary and vascular invasion, or recurrence of CE cysts. 19 However, their study did not delve into the detailed analysis of the invasion of blood vessels and biliary ducts. Clinically, the identification of biliary duct or blood vessel invasion is challenging, especially when large CE cysts compress both the hilar biliary ducts and blood vessels simultaneously.
In this study, our findings reveal distinct characteristics of patients with hepatic CE with intrahepatic biliary duct invasion, including pre-operative cholangitis or residual cavity infection, elevated ALT and AST concentrations, and distal biliary duct dilation because of compression of the common biliary duct. In addition, atrophic hepatic tissue and calculi formation were observed. Intra-operatively, biliary leakage near the hepatic hilum in the residual cavity of CE cysts was detected, confirming the invasion of CE cysts into intrahepatic biliary ducts. Among the 15 patients with vascular invasion, 11 had hepatic vein invasion, whereas the remaining four had portal vein invasion. Unlike those with biliary invasion, patients with vascular invasion exhibited no symptoms of cholangitis or residual cavity infection prior to surgery, and their pre-operative liver function indices were within normal ranges. Imaging revealed compression of either the portal vein or hepatic vein, with no intrahepatic biliary duct dilatation. No biliary leakage was observed in the residual cavity post-open hepatectomy. Patients with hepatic lobe occupation by one or multiple CE cysts did not show invasion into intrahepatic blood vessels and biliary ducts. The clinical characteristics, surgical procedures, and prognosis of patients across the three groups—those with severe biliary duct invasion, vascular invasion, and hepatic lobe occupation—were markedly different.
Our results also indicate that patients with hepatic CE with biliary duct invasion exhibited symptoms of cholangitis and evidence of CE cysts breaking into biliary ducts. These patients often presented with distal liver atrophy or calculi, and their pre-operative ALT concentrations were greater than those in other groups, suggesting that CE cyst invasion into biliary ducts led to biliary-related symptoms and impaired liver function. Such alterations were not observed in patients with vascular invasion or hepatic lobe occupation, likely because of the specific growth pattern of CE cysts that affects only vascular structures or surrounding liver tissues without impacting liver function.
Interestingly, a significant number of patients with biliary invasion underwent open hepatectomy. It was crucial to ascertain the extent of biliary invasion during surgery, especially when biliary leakage was located near the porta hepatis, to avoid damaging contralateral biliary ducts. For the other two groups, closed hepatectomy was the primary surgical approach. Pre-operative enhanced CT scans were used to identify invaded blood vessels and occupied liver tissues, eliminating the need for intra-operative exploration of CE cyst invasion.
After adjusting for confounding factors such as intra-operative blood loss, blood transfusion, and the number of cases with hepatic portal occlusion, we found that operative time and hospital stay were longer for patients with biliary duct invasion. These patients also experienced more post-operative complications, likely because the majority undergoing anatomical hepatectomy to address biliary duct complications. Furthermore, patients with hepatic CE with biliary invasion exhibited atrophic peripheral hepatic tissue and severe local adhesion. This comprehensive analysis underscores the importance of pre-operative, intra-operative, and post-operative data in guiding the surgical management of patients with hepatic CE with varying degrees of complexity.
In cases where CE cysts extensively invade the main biliary ducts or blood vessels of a single hepatic lobe, or when a hepatic lobe is entirely occupied by CE cysts and associated with distal hepatic tissue atrophy, a radical treatment approach, including anatomical hepatectomy, is warranted. This surgical tactic entails the removal of the affected hepatic lobe along with the invaded biliary ducts and vascular structures. The current study principally investigates the surgical indications for anatomical hepatectomy and the necessity of excising distal liver tissues devoid of atrophy for several reasons: (i) Invasion of CE cysts into the biliary ducts or blood vessels of a hepatic lobe results in an insufficient volume of distal residual hepatic tissue post-removal. Retaining such tissue could lead to the formation of an inverted reverse Ω-shaped residual cavity, impeding the drainage of the cavity and potentially giving rise to complications associated with the residual cavity. (ii) Given the liver’s robust regenerative capacity, the remaining hepatic tissue is likely to sustain a considerable volume and function post-operatively. (iii) The complete resection of CE cysts along with distal hepatic tissue minimizes the liver dissection surface, significantly reducing intra-operative blood loss.
This study, however, is not without its limitations and deficiencies. Its retrospective nature and small sample size may introduce bias. Open hepatectomy, often performed in cases with biliary duct invasion to ensure complete cyst removal, was found to result in more complications compared with closed hepatectomy. In addition, operative times and post-operative hospital stays were longer. Thus, pre-operative identification of the biliary duct invasion site and the hepatic lobe to be removed, followed by direct closed hepatectomy, may decrease post-operative complications. This hypothesis warrants validation through multicenter prospective studies. The primary objective of performing hepatectomy in patients with hepatic CE is to lower the post-operative recurrence rate. Previous research has indicated a relatively low recurrence rate of hepatic CE following hepatectomy. Our study’s follow-up results revealed a 2.7% recurrence rate post-anatomical hepatectomy, exclusively observed in the biliary tract invasion group, suggesting a correlation with the employment of open hepatectomy and internal cystectomy.
Conclusions
Anatomical hepatectomy represents a viable and safe surgical option for the management of hepatic CE cysts that significantly invade the intrahepatic main biliary ducts and blood vessels or a single hepatic lobe. This approach effectively mitigates the risk of complications related to residual cavities.
Consent for Publication
All patients signed written informed consent for publication of relevant data.
Footnotes
Authors’ Contributions
Adureheman A., Abuduaini A., H.M., Ayifuhan A., T.J., R.Z., and Q.G. contributed to the data collection and data analysis. Y.S. and T.A. contributed to the study design. Adureheman A. and P.S. contributed to article writing and review. All authors viewed the results and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was supported by the