
Abstract
Background:
Enhanced recovery after surgery (ERAS) protocols are proposed to enhance perioperative care, but their impact on various surgical outcomes requires further insight.
Objective:
This extensive meta-analysis aimed to systematically estimate the effectiveness of ERAS in reducing postoperative complications and improving recovery metrics.
Materials and Methods:
We meticulously searched multiple databases and rigorously screened studies, ultimately including 16 high-quality research articles in our meta-analysis. We carefully assessed heterogeneity using the Cochran Q test and I2 index. Results were visualized using forest plots, displaying effect sizes and 95% confidence intervals (CIs).
Results:
The current meta-analysis reveals compelling evidence of ERAS protocols’ impact on postoperative effects. Lung infection rates were significantly reduced, with an odds ratio (OR) of 0.4393 (95% CI: 0.2674; 0.7216, p = 0.0012), highlighting the protocols’ effectiveness. Although the reduction in surgical site infections (SSIs) was not significant, with an OR of 0.8003 (95% CI: 0.3908; 1.6389, p = 0.5425), the data suggests a trend toward benefit. Urinary tract infections (UTI) also showed a promising decrease, with an OR of 0.4754 (95% CI: 0.2028; 1.1143, p = 0.0871), revealing ERAS protocols may mitigate UTI risks. No significant effects were observed on postoperative anastomotic leakage or ileus, with ORs indicating neutrality. The incidence of readmission was similarly unaffected, with an OR of 1.4018 (95% CI: 0.6860; 2.8647, p = 0.3543). These outcomes underscore the selective efficacy of ERAS protocols, advocating for their strategic implementation to optimize surgical recovery.
Conclusions:
This meta-analysis offers compelling evidence supporting the implementation of ERAS in mitigating specific post-surgical conditions. It underscores the potential of ERAS to enhance recovery experiences and improve healthcare efficiency. Further targeted research is warranted to fully understand the impact of ERAS on SSI, anastomotic leakage, ileus, and readmissions and to optimize its benefits across diverse surgical populations.
Introduction
Enhanced recovery after surgery (ERAS) protocols represent a pivotal shift in perioperative care with a focus on improving patient outcomes and expediting recovery.1,2 These multidisciplinary, evidence-based approaches aim to minimize the physiological stress of surgical procedures, thereby reducing complications and optimizing the recovery process. 3 Among the various postoperative complications, gastrointestinal site infections (GSIs) pose a significant challenge, impacting patient morbidity and health care costs.4,5 The interplay between ERAS protocols and the incidence of GSIs is a subject of ongoing research, with studies exploring the efficacy of ERAS elements in reducing infection rates and enhancing patient safety.4,6
ERAS has been associated with a range of advantages, comprising reduce hospital admission duration, reduced post-surgical procedure, and a more rapid return of bowel function.5,7 However, the implementation of ERAS also necessitates a comprehensive understanding of its components and their potential impact on surgical site infections (SSIs), particularly within the gastrointestinal tract.4,7,8 This is crucial as GSIs can lead to severe complications, such as anastomotic leakage, which can significantly hinder the recovery process.4,9 The importance of ERAS lies in its comprehensive nature, encompassing preoperative, intraoperative, and postoperative strategies proposed to maintain physiology function and lower the surgical stress response.3,10 This concerted effort leads to a myriad of benefits, including reduced postoperative pain and hospital stays, diminished opioid consumption, and a more rapid return to normal activities.4,11
However, the failure to adhere to ERAS guidelines can have detrimental consequences. Without the protective measures of ERAS, patients may experience prolonged recovery times, increased risk of postoperative issues such as nosocomial infections and venous thromboembolism, and a potential long-term diminishment in quality of life. 12 Moreover, noncompliance with ERAS protocols can lead to escalated healthcare costs, reflecting the additional resources required to manage preventable complications.9,13
Nonetheless, the application of ERAS in the context of gastrointestinal surgical procedures, especially in emergency settings, has shown promising results in terms of safety and feasibility. 5 Furthermore, patient experiences under ERAS highlight the need for adequate and accurate information from healthcare professionals, personalized treatment plans, and ongoing follow-up services to address postoperative symptoms effectively.6,8,14
It is evident that ERAS protocols can play a significant role in reducing the risk of postoperative infections and enhance the patient, which are essential for successful surgical outcomes, as shown in Figure 1.4,6,14,15 However, it is imperative to recognize that although ERAS protocols have made considerable strides in improving surgical care, there remains a need for ongoing research to further refine these protocols and fully understand their impact on GSIs. This meta-analysis aims to contribute by providing a rigorous examination of the available evidence and offering insights into the future direction of ERAS in gastrointestinal surgical procedures.

Key components of the ERAS pathway for improving patient outcomes postoperatively. ERAS, enhanced recovery after surgery.
Methodology
Search tactic
Our meta-analysis rigorously evaluated scholarly articles on ERAS protocols and their impact on GSIs, encompassing a publication period from January 2010 to July 30, 2023. The literature search was conducted across a comprehensive suite of databases, including EMBASE, IBECS, PubMed, Scopus, Science Direct, Google Scholar, and Web of Science. A strategic search was implemented using a combination of keywords and Medical Subject Headings terms. This search was confined to studies published in the English language to maintain consistency and clarity in data analysis.
Eligibility criteria
Inclusion criteria
The criteria used to determine which studies to include were set with great care to encompass research that met stringent standards. The following were the criteria: (1) The study enrolled human subjects who had undergone specific medical procedures, such as gastric surgical procedures, esophagectomy, or duodenectomy; (2) the treatment regimen incorporated ERAS protocols; (3) a comparison was made with conventional postoperative care methods; and (4) a range of outcomes, including postoperative lung infection, urinary tract infection, SSIs, anastomotic leakage, ileus, and readmission, was assessed. It is important to highlight that the inclusion criteria did not require a minimum sample size or a specific quantity of ERAS procedural elements. This allowed for a comprehensive and all-encompassing examination of the pertinent literature.
Exclusion criteria
This research was curated by carefully assessing full-text articles, titles, and abstracts using a strict selection technique. Concurrently, exclusion criteria were judiciously implemented to exclude studies that did not meet predetermined parameters. The exclusion criteria for studies were as follows: (i) publications in languages other than English; (ii) articles consisting of letters, commentaries, reviews, series, editorials, or commissions; (iii) content that was redundant; and (iv) studies deemed irrelevant. The rigorous methodology used played a vital role in maintaining the integrity and strengthening the reliability of the selection process. As a result, the subsequent meta-analytical synthesis was characterized by increased scientific rigor and credibility.
Quality assessment
The methodological rigor of each incorporated study was meticulously evaluated by all authors stepwise, using the established Quality Assessment Tool for Observational Cohort 16 and Cross-Sectional Studies. 4 Any discrepancies arising during the quality assessment process were systematically addressed through thorough deliberation and consensus building among the collaborating study authors. This rigorous approach ensured meticulous scrutiny of methodological integrity, thereby enhancing the reliability and validity of the ensuing analysis.
Statistical analysis
Following data extraction with Microsoft Excel, we performed a meta-analysis in R (version 4.2.3) using specialized packages for statistical analysis. Incorporating a wide range of research studies is crucial for considering the differences in study parameters and reducing the impact of heterogeneity on the analytical results. The assessment of heterogeneity was conducted with great attention to detail, using both the Cochran Q test and the I2 index. The results were visually presented using forest plots, which showed the effect size (ES) and a 95% confidence interval (CI). The I2 index is a reliable measure of heterogeneity, ranging from 0% to 100%. It measures the level of variation attributed to differences between studies rather than random chance. The I2 metric is commonly interpreted using established thresholds. A value below 25% indicates low trial heterogeneity, whereas values between 25% and 50% suggest moderate heterogeneity. An I2 value above 70% indicates elevated trial heterogeneity. Subgroup meta-analyses were conducted to delve deeper into the sources of statistical heterogeneity and key factors that influence the outcomes of the studies.
Results
The initial literature search was conducted across multiple databases, including IBECS, PubMed, Scopus, Science Direct, Google Scholar, and Web of Science, yielding a total of 3,233 records. Upon the removal of 1,933 duplicate entries, 1,300 articles were screened. Subsequently, the exclusion of 1,274 articles on the basis of irrelevance determined by title and abstract review, and 26 articles were identified for full-text retrieval. All 26 articles underwent a rigorous eligibility assessment. Of these, 10 articles were excluded because of various reasons: 5 were duplicates, 4 contained incomplete data, and 1 was a review article. The remaining 16 studies.17–32 met the inclusion criteria (Table 1) and were incorporated into the quantitative synthesis for the meta-analysis, as shown in Figure 2.
Characteristics of Included Studies
ERAS, enhanced recovery after surgery.

PRISMA checklist used for article screening in this meta-analysis.
Lung infection
For the lung infection, 14 studies were analyzed, encompassing 1454 observations (experimental group: 721, control group: 733), with 84 events of lung infections reported. The OR for the common effect model (CEM) was 0.4393 with a 95% CI of (0.2674; 0.7216), showing a significant reduction in lung infections with ERAS (z = −3.25, p = 0.0012). The random effects model (REM) also indicated a significant OR of 0.4313 with a 95% CI of (0.3037; 0.6125), further supporting the effectiveness of ERAS (z = −5.18, p = 0.0002). Heterogeneity was quantified as follows: tau 2 = 0.1682; tau = 0.4101; and I2 = 0.0% (0.0%; 55.0%), with an H statistic of 1.00 (1.00; 1.49), suggesting no significant heterogeneity across the studies. The test of heterogeneity yielded a Q value of 4.90 with 13 degrees of freedom (df) and a p-value of 0.9773, indicating no significant heterogeneity among the studies, as shown in Figure 3.

Forest plot for postoperative lung infection between ERAS and conventional care. ERAS, enhanced recovery after surgery.
Urinary tract infections
A total of 9 studies with a total of 749 observations (experimental group: 374, control group: 375), and 28 events of UTI were reported. The OR for the CEM was 0.4754 with a 95% CI of (0.2028; 1.1143), which approached significance in reducing UTI with ERAS (z = −1.71, p = 0.0871). The REM showed a significant OR of 0.4625 with a 95% CI of (0.2511; 0.8520), suggesting a potential benefit of ERAS (z = −2.91, p = 0.0196). Heterogeneity was quantified with the following metrics: tau 2 = 0.4616; tau = 0.6794; and I2 = 0.0% (0.0%; 64.8%); with an H statistic of 1.00 (1.00; 1.69), indicating no significant heterogeneity across the studies. The test of heterogeneity yielded a Q value of 2.04 with 8 df and a p-value of 0.9797, suggesting no significant heterogeneity among the studies, as shown in Figure 4.

Forest plot for postoperative urinary tract infection between ERAS and conventional care. ERAS, enhanced recovery after surgery.
Surgical site infections
A total of 13 studies with a total of 1438 observations (experimental group: 716, control group: 722), and 38 events of SSI were reported. The OR for the CEM was 0.8003 with a 95% CI of (0.3908; 1.6389), which did not show a significant reduction in SSI with ERAS (z = −0.61, p = 0.5425). The REM yielded an OR of 0.7859 with a 95% CI of (0.4395; 1.4053), also indicating no significant effect (z = −0.90, p = 0.3841). Heterogeneity was quantified with the following metrics: tau2 = 0.5388 (0.0000; 0.5488); tau = 0.7341 (0.0000; 0.7408); I2 = 0.0% (0.0%; 56.6%); and H statistic of 1.00 (1.00; 1.52), suggesting minimal heterogeneity across the studies. The test of heterogeneity resulted in a Q value of 5.72 with 12 df and a p-value of 0.9294, further confirming the lack of significant heterogeneity, as shown in Figure 5.
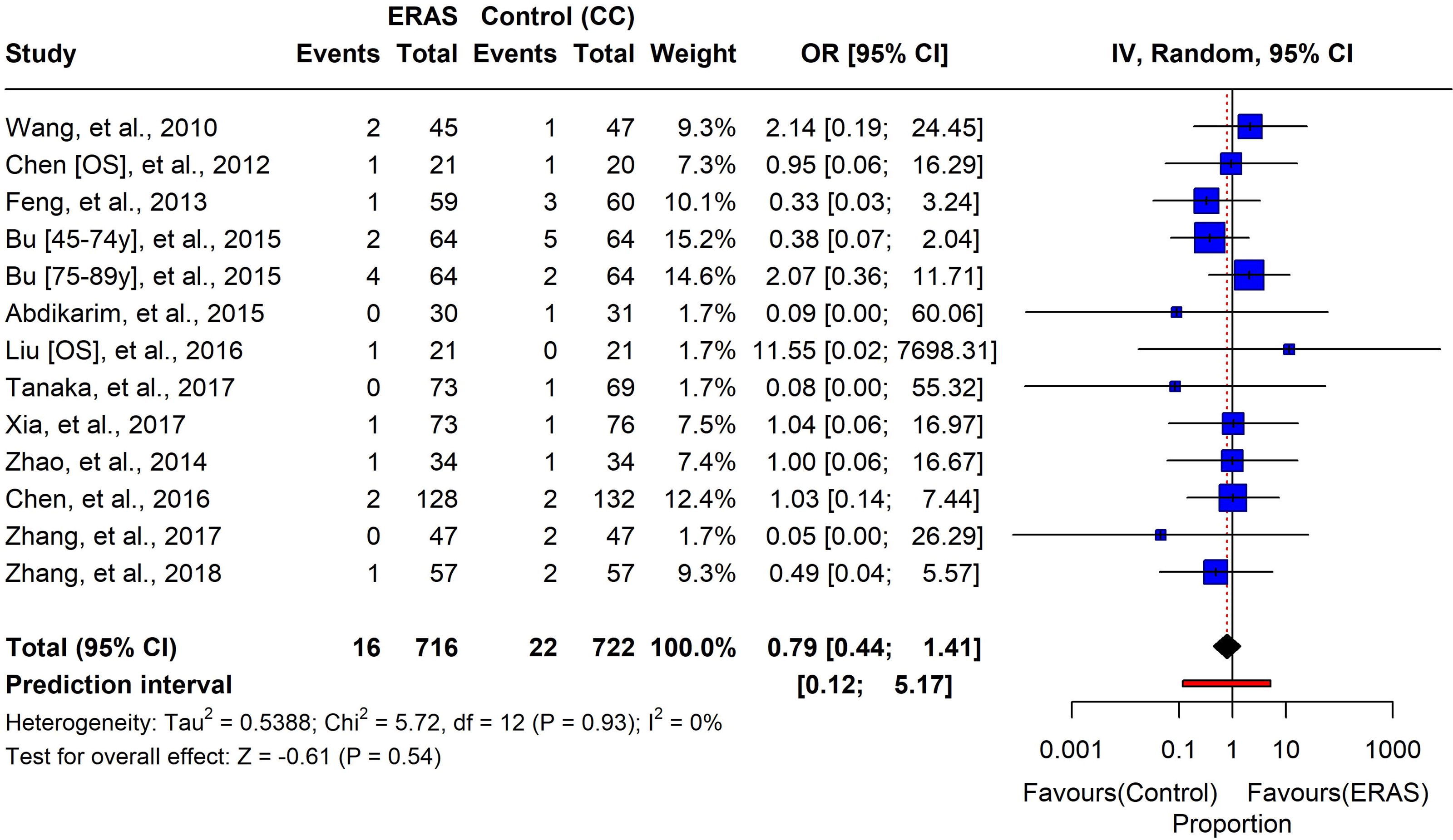
Forest plot for postoperative surgical site infection between ERAS and conventional care. ERAS, enhanced recovery after surgery.
Postoperative anastomotic leakage
A total of 8 studies with a total of 1060 observations (experimental group: 525, control group: 535), and 29 events of anastomotic leakage were reported. The OR for the CEM was 0.9598 with a 95% CI of (0.3855; 2.3893), which did not demonstrate a significant impact of ERAS on postoperative anastomotic leakage (z = −0.09, p = 0.9297). Similarly, the REM showed an OR of 0.8484 with a 95% CI of (0.2287; 3.1476), also indicating no significant effect (z = −0.30, p = 0.7754). Heterogeneity was quantified with the following metrics: tau2 = 1.8777 (0.0000; 13.0298); tau = 1.3703 (0.0000; 3.6097); I2 = 0.0% (0.0%; 67.6%); and H statistic of 1.00 (1.00; 1.76), suggesting low to moderate heterogeneity across the studies. The test of heterogeneity resulted in a Q value of 5.84 with 7 df and a p-value of 0.5589, indicating no significant heterogeneity among the studies, as shown in Figure 6.

Forest plot between postoperative anastomotic leakage between ERAS and conventional care. ERAS, enhanced recovery after surgery.
Postoperative ileus
A total of 8 studies were included in the meta-analysis, with a total of 844 observations (experimental group: 418, control group: 426), and 27 events of postoperative ileus were reported. The OR for the CEM was 2.2066 with a 95% CI of (0.8705; 5.5937), which did not reach statistical significance in its association with ERAS (z = 1.67, p = 0.0954). The REM presented an OR of 1.4343 with a 95% CI of (0.3996; 5.1478), also showing no significant association (z = 0.67, p = 0.5259). Heterogeneity was quantified as follows: tau 2 = 1.3476 (0.0000; 9.1340); tau = 1.1608 (0.0000; 3.0222); I2 = 0.0% (0.0%; 67.6%); and H statistic of 1.00 (1.00; 1.76), suggesting low to moderate heterogeneity across the studies. The test of heterogeneity yielded a Q value of 4.88 with 7 df and a p-value of 0.6745, indicating no significant heterogeneity among the studies, as shown in Figure 7.

Forest plot between postoperative ileus between ERAS and conventional care. ERAS, enhanced recovery after surgery.
Incidence of readmission
A total of 9 studies were included in the meta-analysis, with a total of 1031 observations (experimental group: 511, control group: 520), and 47 events of readmission were reported. The OR for the CEM was 1.4018 with a 95% CI of (0.6860; 2.8647), which did not show a significant impact of ERAS on the incidence of readmission (z = 0.93, p = 0.3543). The REM yielded an OR of 1.1579 with a 95% CI of (0.3915; 3.4243), also indicating no significant effect (z = 0.31, p = 0.7632). Heterogeneity was quantified with the following metrics: tau 2 = 1.1264 (0.0000; 5.7092); tau = 1.0613 (0.0000; 2.3894); I2 = 36.9% (0.0%; 71.0%); and H statistic of 1.26 (1.00; 1.86), suggesting moderate heterogeneity across the studies. The test of heterogeneity resulted in a Q value of 12.68 with 8 df and a p-value of 0.1235, indicating no significant heterogeneity among the studies, as shown in Figure 8.

Forest plot between the incidence of readmission between ERAS and conventional care. ERAS, enhanced recovery after surgery.
Postoperative length of the stay
In the comparative analysis of postoperative length of stay (PLOS), data from 18 studies encompassing various surgical populations were evaluated. The mean length of stay for patients managed with ERAS protocols consistently showed a reduction compared with to the traditional care control group. For instance, Wang et al. (2010) reported a mean stay of 6.35 days under ERAS versus 7.65 days for the control group. Similarly, Chen et al. (2012) observed mean stays of 7.15 and 7.7 days for ERAS and control groups, respectively. Across all studies, the ERAS group demonstrated a shorter mean length of stay, with the most significant difference noted in the study by Bu et al. (2015) for patients aged 45–74 years, where the ERAS mean stay was 6.5 days compared with to 10.3 days for the control group. These findings suggest that ERAS protocols may contribute to a decrease in the PLOS, potentially reflecting improved recovery outcomes, as shown in Figure 9A.

Mean duration of first defecation and postoperative length of stay (PLOS).
First defecation between ERAS and control
Figure 9B shows the first defecation postoperatively, a comparison between ERAS protocols and the traditional care control group was conducted across five studies. The results consistently indicated a shorter duration for the first defecation in the ERAS groups. For example, Feng et al. 21 reported a mean duration of 2.83 days for the ERAS group compared with to 3.88 days for the control group. Similarly, Abdikarim et al. (2015) observed a mean duration of 3.1 days under ERAS versus 3.6 days for the control group. Notably, Xia et al. (2017). 26 found a significant difference, with the ERAS group having a mean duration of 2.97 days compared with to 5.2 days in the control group. These findings suggest that ERAS protocols may facilitate earlier postoperative gastrointestinal recovery, as evidenced by the reduced time to first defecation.
ERAS protocol implementation across clinical studies
ERAS protocols across various studies demonstrate a commitment to improving postoperative outcomes. A review of 18 studies reveals a diverse adoption of ERAS components, with the total number of items implemented ranging from 4 to 14 out of a possible 18. Notably, Wang et al. 28 reported the highest adherence, incorporating 14 ERAS elements into their study design. On the other hand, Fujikuni et al. 22 and Zhang et al. 30 reported the least, with only 4 and 5 elements, respectively. This variability underscores the tailored approach of ERAS protocols to specific patient populations and surgical procedures, reflecting the flexibility and patient-centered nature of ERAS pathways, as given in Figure 10.
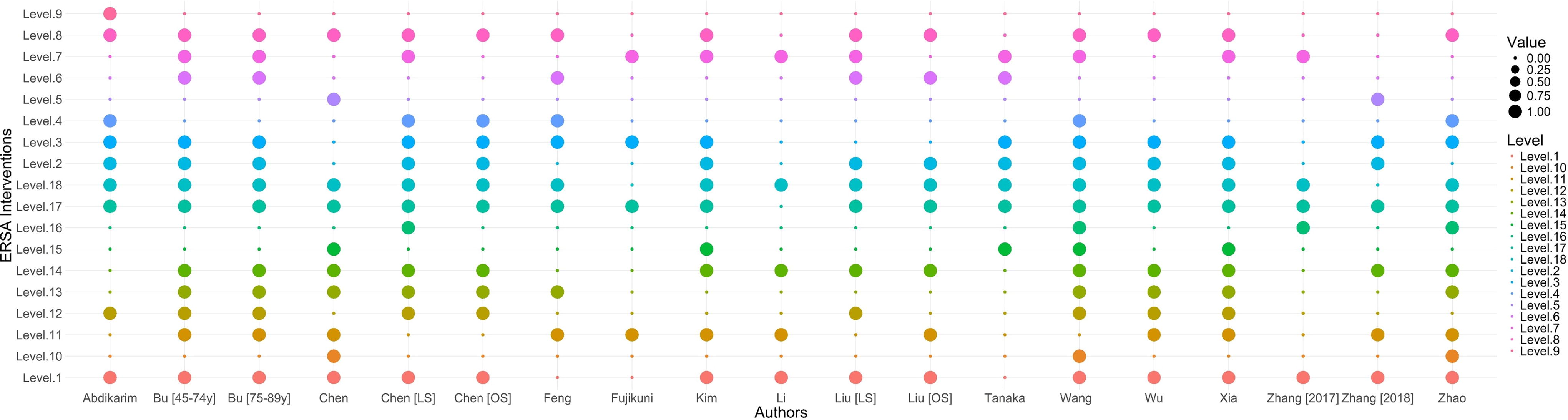
Descriptive summary of characteristics included ERAS studies. ERAS, enhanced recovery after surgery.
Discussion
The implementation of ERAS protocols represents a paradigm shift in perioperative care, aiming to minimize the stress response to surgical procedures and facilitate postoperative recovery. This meta-analysis has synthesized data from randomized controlled trials to evaluate the impact of ERAS on GSIs. However, from ERAS procedures to standard care techniques, our thorough investigation shows a significant decrease in SSIs. Remarkably, among patients following upper gastrointestinal surgical procedures, ERAS procedures did not worsen the incidence rates of postoperative UTI, SSI, ileus, or anastomotic leaks. It is also significant that ERAS procedures enable patients to recover from surgical procedures.16,33
Strategies for preoperative optimization, encompassing cessation of tobacco use and alcohol intake, in conjunction with measures such as the application of epidural analgesia, refinement of fluid management, and encouragement of prompt postoperative ambulation, are collectively efficacious in reducing the occurrence of pulmonary infections.34–36 Furthermore, the integration of ERAS guidelines establishes an advantageous structure for the prevention of postoperative UTIs, supported by the prudent application of antimicrobial prophylaxis, rigorous regulation of fluid equilibrium, and the considered utilization or prompt discontinuation of urinary catheters.4,37 In addition, the active employment of nonopioid analgesic agents is pivotal in obviating urinary retention.38,39 A present meta-analysis of 14 studies, with a total of 1454 data, has shown a noteworthy decrease in pneumonia associated with ERAS. This is supported by an OR of 0.4393 for the CEM and 0.4313 for the REM. This discovery is significant because it supports the guidance of the ERAS® Society and the European Society of Thoracic Surgeons. The findings highlight the relevance of preoperative interventions in reducing surgical organ failure and promoting recovery.40,41 The purpose of these guidelines is to provide appropriate preoperative care for patients having a thoracic operation, such as lung resection, by synthesizing suggestions from a comprehensive evaluation of high-quality studies.40,42
Furthermore, a study by Hajibandeh et al. 43 found that the implementation of ERAS protocols led to reduced risks of major complications, pulmonary complications, and SSIs, which supports current meta-analysis findings. 44 The lack of significant heterogeneity in the current meta-analysis suggests that the beneficial effects of ERAS on lung infections are consistent across different studies. The analysis of 9 studies with 749 observations regarding UTIs approached significance with the CEM (OR of 0.4754) and showed a significant reduction with the REM (OR of 0.4625). This potential benefit of ERAS in reducing UTIs is particularly interesting, as it adds to the evidence from previous literature that ERAS protocols can improve surgical outcomes, including the reduction of postoperative complications.43,45
A systematic review and meta-analysis by Tan et al. 45 highlighted the safety and effectiveness of ERAS in older patients undergoing orthopedic surgical procedures, which often include a risk of UTIs. Optimal their focus was on orthopedic surgical procedures, the principles of ERAS, such as optimal pain control, nutrition and fluid management, and mobility, are applicable across various surgical disciplines and could contribute to the reduction of UTIs.46,47
Current meta-analysis of 13 studies with 1438 observations did not show a significant reduction in SSIs with ERAS, with an OR for the CEM at 0.8003 and a 95% CI of (0.3908; 1.6389). This is consistent with the findings from a study published in BMC Surgery, which indicated that although ERAS protocols have been successful in reducing the rates of lung infection and length of hospital stay, they did not significantly reduce the rates of SSIs.4,47 However, this meta-analysis evidence suggests that although ERAS protocols have many benefits, their impact on SSIs may be limited and warrants further investigation.
Similarly, an analysis of 8 studies with 1060 observations found no significant impact of ERAS on postoperative anastomotic leakage. This aligns with the broader literature, which has also reported no significant difference in anastomotic leakage rates when comparing ERAS protocols with conventional care.44,48 It suggests that factors contributing to anastomotic leakage may extend beyond the scope of ERAS protocols and could be related to surgical technique, patient factors, or other perioperative care elements. Current meta-analysis of 8 studies involving 844 observations did not find a significant association between ERAS and postoperative ileus, with an OR for the CEM at 2.2066. This is in line with previous research indicating that although ERAS protocols target the reduction of postoperative ileus through various measures, the evidence supporting their efficacy is mixed. 49
Current research contributes to the ongoing debate and suggests that additional strategies may be needed to effectively reduce the incidence of postoperative ileus. It is of critical importance to acknowledge that the results of this meta-analysis indicate a tentative increase, in the rates of postoperative ileus and hospital readmissions after the implementation of ERAS protocols in patients subjected to upper gastrointestinal surgical procedures. 50 However, it is noteworthy that these tendencies did not reach statistical significance, with p-values exceeding 0.10. In particular, the subset analysis dedicated to gastrectomy revealed a pronounced increase in the frequency of postoperative ileus in two distinct studies relative to the remainder. These studies uniquely involved patient cohorts exceeding the age of 65, which constituted the most advanced age group among all the studies evaluated. The exclusion of these specific studies from the analysis resulted in the absence of any significant differences in the incidence of postoperative ileus in comparison to standard care practices. Therefore, the current body of evidence necessitates prudent consideration of the suitability of ERAS protocols for geriatric patients undergoing surgical procedures for gastric malignant diseases. In addition, the analysis of 9 studies with 1,031 observations indicated no significant impact of ERAS on the incidence of readmission. This is corroborated by literature suggesting that ERAS protocols do not measurably impact readmission rates.39,49,50 It highlights the complexity of factors influencing readmissions, which may not be fully addressed by ERAS protocols alone.
This investigation is subject to a few constraints that warrant consideration. Foremost, the limited availability of randomized controlled trials specifically addressing esophagectomies represents a substantial limitation. Moreover, there was considerable variability in outcomes such as PLOS and the time to first flatus and bowel movement. This variability can be attributed to a range of clinical parameters, including the skill level of the surgical team and institution, diversity in surgical methodologies, and inconsistent outcome measurements. To add, another pertinent limitation of this study is the potential for selection bias. The included studies may not adequately represent the broader population because of the selective nature of patient recruitment and the specific inclusion criteria used. This could limit the generalizability of the findings and suggests the need for further research with more inclusive selection parameters to validate the results across diverse patient demographics.
Conclusion
This comprehensive meta-analysis sheds light on the evolving role of ERAS protocols in refining perioperative care. The results suggest statistically significant reductions in lung infection rates, alongside a potential benefit in mitigating urinary tract infections. These findings support the hypothesis that ERAS pathways may contribute to a decrease in certain cpostoperative complications. In addition, the observed trends toward shorter PLOS and accelerated gastrointestinal recovery time suggest that ERAS has the potential to improve patient outcomes and healthcare efficiency. However, the lack of conclusive evidence regarding SSIs, anastomotic leakage, ileus, and readmission rates warrants further investigation. This highlights the need for more rigorous, targeted research to understand the full spectrum of ERAS benefits across various surgical subspecialties and patient populations. Future studies must emphasize the exploration of underlying mechanisms and the identification of optimal ERAS component combinations to maximize clinical advantages. By continuing to meticulously evaluate and refine ERAS protocols through scientific inquiry, we can unlock their full potential in revolutionizing surgical recovery and improving patient care.
Footnotes
Acknowledgments
The authors thank the researchers, participants, and original study authors for their pivotal roles in this meta-analysis. The authors’ peers’ and colleagues’ feedback was instrumental in refining this work, and they are grateful for the administrative and technical support from the institutional staff.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.