
Abstract
Objective:
This study employed uni-variable and multi-variable Mendelian randomization (MVMR) analyses, utilizing publicly available genome-wide association study (GWAS) data, to assess the causal relationship between body composition measures such as body mass index (BMI), waist circumference (WC), and the occurrence of surgical site infection (SSI).
Patients and Methods:
GWAS summary statistical data were obtained for BMI, WC, and SSI from the MRC Integrated Epidemiology Unit (MRC-IEU) database, inverse variance weighted (IVW) method was used as the main analysis, and supplement sensitivity analysis (including heterogeneity test, pleiotropy analysis, leave-one-out analysis, and Mendelian Randomization Pleiotropy RESidual Sum and Outlier (MR-PRESSO)) was used to check the robustness of the results.
Results:
The MR analysis showed that the increase in BMI and WC predicted by genes had a substantial causal effect on the incidence of SSI (IVW: odds ratio [OR] = 1.003, 95% confidence interval [CI] = 1.002–1.004, p < 0.001; IVW: OR = 1.003, 95% CI = 1.002–1.005, p < 0.001), respectively, and the MVMR analysis showed that after jointly incorporating smoking and alcohol parameters, the impact of BMI and WC on SSI remained substantial (OR = 1.003, 95% CI = 1.002–1.004, p < 0.001; OR = 1.004, 95% CI = 1.002–1.005, p < 0.001).
Conclusion:
We further support the causal relationship between increased body composition including BMI and WC and the occurrence of SSI, highlighting the importance of SSI prevention in patients with obesity. Further research is required to mitigate the occurrence of surgical incisions in patients with obesity in the future.
The threat posed by health-care–associated infections (HAIs) to patients’ health is of utmost severity and continues to present a substantial challenge for healthcare service providers on a global scale. 1 Surgical site infections (SSI) continue to pose a substantial burden in terms of morbidity and mortality, constituting approximately one-fifth of all HAIs.2,3 The overall pooled incidence of SSI was 2.5% globally. 4 The occurrence of SSIs has substantial implications for both patients and healthcare systems, encompassing patient discomfort, prolonged hospitalization periods, and increased healthcare expenditures. Notably, SSIs have been associated with an approximate extension of hospital stays by 10 days. Similarly, it increased the cost of therapy and the cost of an operation by 300%–400% 5 and increased the rate of hospital readmissions and jeopardized health outcomes. However, as a result of poor infection prevention practices, SSI is substantially greater in low- and middle-income countries compared with high-income countries.6,7
Numerous studies8–10 have been conducted in the past to investigate the intrinsic and extrinsic factors contributing to the pathogenesis of SSI. Effective reduction of SSI incidence can be achieved through meticulous management of extrinsic factors, including adherence to surgical aseptic procedures, optimization of operating room environment, and appropriate surgical techniques. The control of these external factors relies on hospital management practices, which can be enhanced through systematic interventions. However, 11 internal factors primarily rely on an individual patient’s immune response, underlying medical conditions, and lifestyle habits; their control is challenging owing to difficulties in evaluation. Among these intrinsic factors, the one that cannot be overlooked is the impact of obesity.
The persisting inconsistencies in the findings regarding the etiological association between body mass index (BMI) and SSI cannot be overlooked. For instance, a systematic review revealed that SSI class, study design, or patient BMI did not impact study results in a meta-regression model. 12 The literature has demonstrated that there exists a synergistic effect between BMI, smoking, and diabetes mellitus in relation to the increased susceptibility to SSI.13,14 The independent association between BMI and SSI has not been firmly established, in summary.
Mendelian randomization (MR) analysis 15 is an epidemiological research method that evaluates the causal relationship between exposure and outcomes by using one or more genetic variations, such as single nucleotide polymorphisms (SNPs). MR research can greatly avoid the influence of reverse causality and confounding factors in traditional epidemiological studies.
Considering the above advantages of MR analysis, this study intends to explore the causal relationship between BMI, waist circumference (WC), and SSI by using published genome-wide association studies (GWAS) data for uni-variable and multi-variable MR (MVMR) analysis. The findings of our study not only offer robust evidence for the etiology of obesity and SSI but also provide valuable recommendations for future prevention tactics targeting SSI.
Patients and Methods
Research design and data sources
This study follows the hypothesis that (1) genetic variation is closely related to risk factors, (2) genetic variation is not related to confounding factors, and (3) genetic variation only affects outcomes through risk factors, as shown in the study design in Figure 1. We obtained GWAS data for BMI, WC, and SSI from the Integrated Epidemiology Unit (IEU) OpenGWAS project website (https://gwas.mrcieu.ac.uk/), with a website visit time of December 14, 2023. The BMI summary data include 461,460 participants and 9,851,967 SNPs, whereas the WC summary data include 462,166 participants and 9,851,867 SNPs. The summary data of SSI (main ICD10: T81.4 Infection following a procedure, not elsewhere classified) include ncase 2,305 and ncontrol 460,705 participants, with 9,851,867 SNPs, both from the European population, regardless of gender (Table 1).
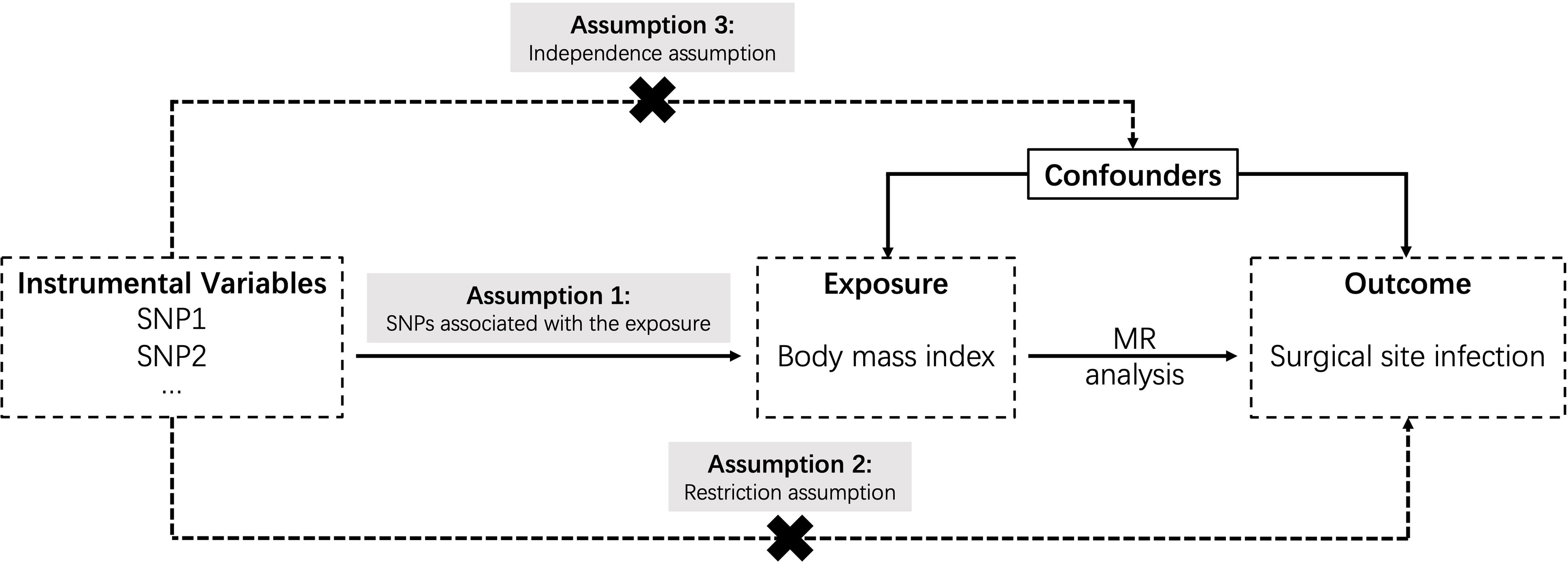
Design of Mendelian randomization study.
Summary of the GWAS Included in This Two-Sample MR Study
Output from GWAS pipeline using Pheasant-derived parameters from UK Biobank.
GWAS = genome-wide association study; MR = Mendelian randomization; SNP = single nucleotide polymorphism; BMI = body mass index; WC = waist circumference; SSI = surgical site infection.
Instrumental variables
The selected instrumental variable (IV) must satisfy three main assumptions: (1) have strong correlation with exposure, (2) have no correlation with outcome through confounding pathways, and (3) have no direct correlation with outcome, only indirect correlation through exposure. The data analysis adopts the “TwoSample MR” and “MRPRESSO” packages in R software version 4.1.2. Using p < 5 × 10−8 as the screening criteria, SNP loci with statistical significance were selected from BMI and WC as the IVs for preliminary screening. The linkage imbalance coefficient r2 = 0.001 was set, and the region width was set to 10,000 kb to ensure the independence of each SNP and exclude the influence of gene polymorphism on the results. In addition, we also excluded SNPs closely related to the results (p < 5 × 10−8). Finally, the intensity of IV was quantified using the F statistic. If F > 10, it indicates that the included SNPs have a lower likelihood of weak instrumental bias. The calculation formula for the F statistic is F =
Uni-variable and multi-variable Mendelian randomization
The inverse variance weighted (IVW) method has the highest statistical efficiency among all MR methods; therefore, we make it the main analysis method for uni-variable MR. In order to avoid bias in IVW results caused by the level pleiotropy of any single SNP, four other MR methods were used to enhance the robustness of the results, including MR-Egger, weighted median estimator, weighted mode, and simple mode. We also conducted MVMR analysis to evaluate whether the effects of BMI and WC on SSI are independent of the two common risk factors of smoking and alcohol consumption.
Sensitivity analysis
When IVs have pleiotropy, there may be bias in IVW estimation. Therefore, we added some sensitivity analysis to further confirm the reliability of the results. First, the Cochran’s Q test is used to determine the heterogeneity of SNPs. When p < 0.05, heterogeneity is considered to exist, and the focus is on the results of the random effects IVW method. In order to detect potential biases in horizontal pleiotropy, MR-Egger regression was used. If the intercept term in MR-Egger regression is not equal to 0 and has statistical significance, it indicates that the study has horizontal pleiotropy. In addition, a leave-one-out test was conducted to perform sensitivity analysis, removing each SNP in sequence. If there is no substantial difference between the calculated MR results of the remaining SNPs and the total results, it indicates that the MR results are robust. The above methods are all implemented using the “TwoSample MR” package in R 4.1.2 software to verify, and the inspection level α = 0.05.
Results
Selection of IVs
A total of 383 SNPs highly correlated with SSI were screened from BMI, and 18 SNPs related to outcome were excluded. Among them, rs7928320 was an incompatible allele; rs10887578, rs11250094, rs11634851, rs12507026, rs1454687, rs1860750, rs2396625, rs347551, rs396755, rs4737188, rs59086897, rs6597975, rs7568228, rs765874, rs7704382, rs9388446, and rs961498 were palindrome with moderate allele frequency. After MR-PRESSO analysis, there were no outliers and 365 SNPs were ultimately included, with R2 = 2.6%. The distribution range of the F statistic corresponding to a single SNP was 26.76–1204.07, indicating that weak IVs were not used in the MR analysis. The basic information of SNPs is shown in Table 2 and Supplementary Table S1. Similarly, 322 SNPs highly correlated with SSI were screened from WC, removing 12 SNPs related to outcome for being palindromic with intermediate allele frequencies: rs10406327, rs10887578, rs11666480, rs11778934, rs13264909, rs1405261, rs1441098, rs1454687, rs165656, rs347551, rs3949781, rs4856720. After MR-PRESSO analysis, there were no outliers. Finally, 310 SNPs were included in the study, and the basic information of SNPs can be found in Table 2 and Supplementary Table S1.
The SNPs of BMI and WC Associated with SSI
More SNPs information can be found in Supplementary Table S1.
SNP = single nucleotide polymorphism; EA = effect allele; OA = other allele; EAF = effect allele frequency; CHR = chromosome; POS = position; BMI = body mass index; WC = waist circumference; SSI = surgical site infection; SE = standard error.
Uni-variable MR analysis of BMI, WC, and SSI
The increase in BMI and WC predicted by genetics is associated with an increased risk of SSI, and the causal effects obtained by the five methods are consistent; see Table 3 and Figures 2–4 for detail. The IVW analysis showed a statistically significant association between BMI, WC, and the risk of SSI occurrence (odds ratio [OR] = 1.003, 95% confidence interval [CI] = 1.002–1.004, p < 0.001; OR = 1.003, 95% CI = 1.002–1.005, p < 0.001), respectively.
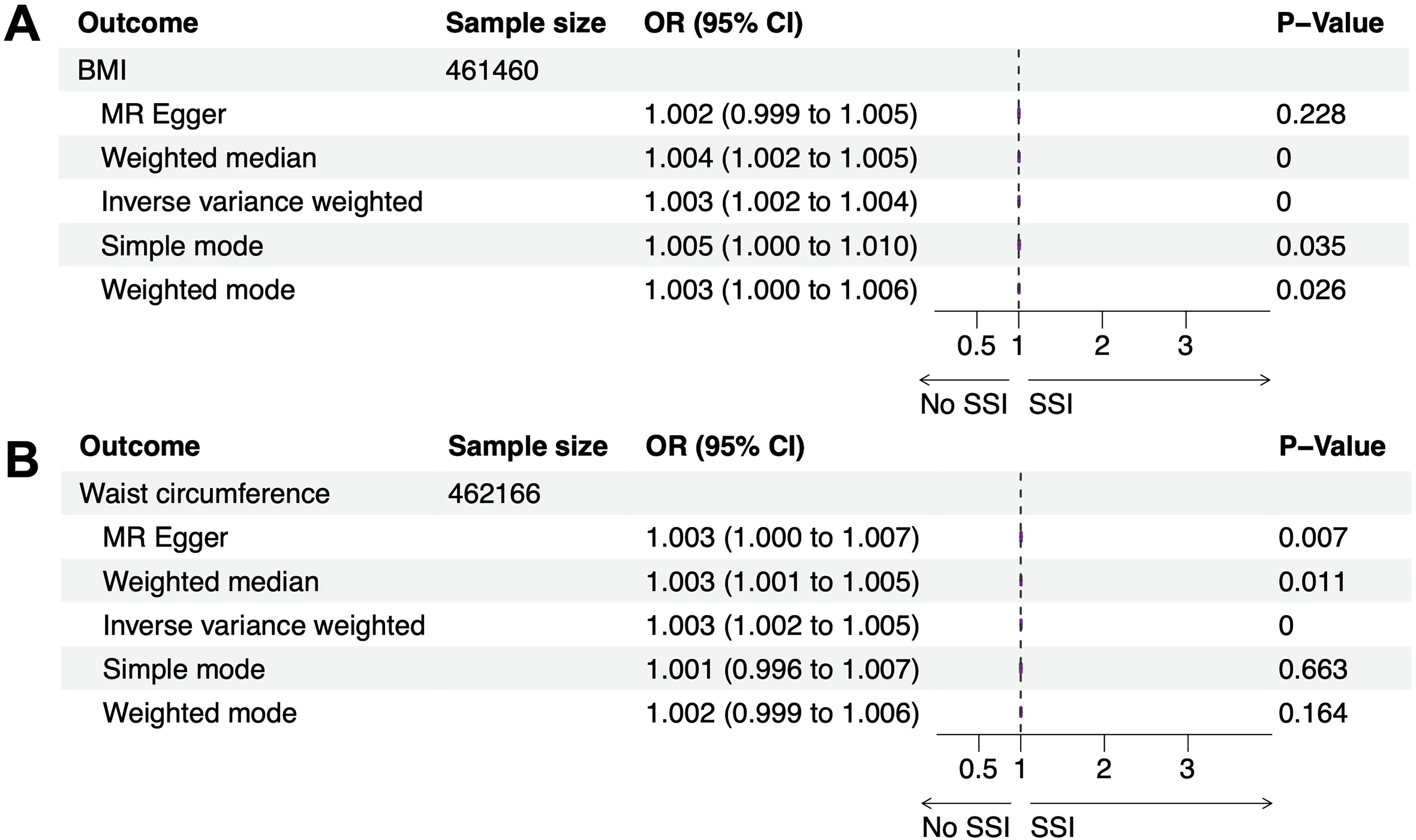
Classic forest plot for MR analysis.

Forest plot of the two-sample MR analysis.

Scatter plot of the two-sample MR analysis.
Uni-variable MR Results of the Relationship Between BMI, WC, and SSI
MR = Mendelian randomization; BMI = body mass index; WC = waist circumference; SSI = surgical site infection; OR = odds ratio; CI = confidence interval.
Sensitivity analysis
The IVW and MR-Egger methods for Cochran’s Q-test showed no heterogeneity, and no evidence of horizontal pleiotropy was observed in the intercept term of MR-Egger regression. The MR-PRESSO pleiotropy test showed no outlier SNPs (Table 4), indicating that the causal relationship between the selected IVs and BMI, WC, and SSI is not affected by horizontal pleiotropy, and the results are reliable. The leave-one-out forest plot suggests unbiased SNPs (Fig. 5), and eliminating any SNPs does not substantially affect the estimation of causal correlation, indicating the robustness of the MR analysis results. The funnel plot shows that all SNPs included are basically symmetrical, with no substantial bias, indicating that the differences between IVs are small (Fig. 6).

Results of leave-one-out sensitivity analysis.

Funnel plot of the two-sample MR analysis.
Sensitivity Analysis of Two-Sample MR Study
MR = Mendelian randomization; IVW = inverse variance weighted; SE = standard error; BMI = body mass index; WC = waist circumference; SSI = surgical site infection.
MVMR analysis
After correcting for the effects of smoking and alcohol consumption indicators, MVMR analysis was performed on BMI and WC, and the results showed that BMI and WC still had a substantial genetic predictive effect on SSI (OR = 1.003, 95% CI = 1.002–1.004, p < 0.001; OR = 1.004, 95% CI = 1.002–1.005, p < 0.001), respectively, as shown in Table 5.
Results of Multi-variable Mendelian Randomization Studies
MVMR = multi-variable Mendelian randomization; SNP = single nucleotide polymorphism; SE = standard error; OR = odds ratio; CI = confidence interval; BMI = body mass index; SSI = surgical site infection; WC = waist circumference.
Discussion
The findings of this study offered robust and compelling evidence, at a high level, supporting the independent role of BMI as a causative factor for SSI. In our study, MR analysis was used to exclude confounding factors, resulting in greater accuracy and confidence in the results. First, compared with observational studies, MR analysis has advantages such as avoiding confounding factors, reverse causal relationships, and saving time and resources; second, this study did not reveal potential level pleiotropy, thus confirming the reliability of the conclusion; and third, this study conducted a multi-variable study to further validate the credibility of the research results. The escalating prevalence of obesity in recent years, particularly the substantial increase in bariatric surgical procedures, underscores the imperative and immediacy of implementing effective measures to prevent SSI among individuals with obesity.16,17
The insufficient blood supply of adipose tissue and the presence of a non-healing cavity in patients with obesity have been extensively studied, leading to a consensus that these factors increase the risk of surgical infection. 18 Relevant studies have demonstrated that excessive body weight is associated with greater incidence rates of complications such as incision infection and dehiscence, making it an important prognostic factor.19–21 Foreign research suggests that obesity contributes to increased rates of SSI, possibly because of the formation of dead spaces and hematomas in subcutaneous adipose tissue at the operative site, which has limited vascularity and thus inadequate blood supply.22–24 This heightened risk subsequently leads to increased occurrences of anastomotic leakage and incisional dehiscence. The 2016+ American College of Surgeons / Surgical Infection Society (ACS/SIS) Guidelines specifically identify overweight and obesity as modifiable patient-related risk factors intrinsic to SSI development, alongside preoperative serum albumin concentrations below 35.0 g/L and bilirubin concentrations exceeding 17.1 mcmol/L. 25 Previous studies have shown that the serum immunoglobulin G (IgG), IgM, and IgA values of patients with obesity are substantially lower than those of the same age and normal weight population. Among obese individuals, the number of serum immunoglobulins, complement C3 and C4, and T and B lymphocytes is substantially lower than that of non-obese individuals, indicating poor immunity.26,27 In addition, obesity affects the immune system and leads to metabolic disorders. 28 Indeed, the incidence of SSI in patients with obesity is closely associated with the surgical expertise and skill of surgeons. Enhancing the level of surgical proficiency plays a substantial role in preventing and treating surgical infections. 29 Some experts have highlighted that certain guidelines have not adequately addressed this aspect. Regrettably, the World Health Organization’s global guidelines for SSI prevention do not provide further elaboration on this matter. The 2016+ACS/SIS Guidelines acknowledge the risk factors for SSI during prolonged operations, and it is understandable that obesity contributes to an increased risk owing to the complexity of the procedure or exacerbation of malnutrition, which can impact operation duration. 30
Our study still has some limitations: First, this study only observed a causal relationship between BMI, WC, and SSI at the dual sample gene level. In the future, larger sample MR studies and randomized controlled trials (RCTs) are needed to verify the results. Second, the research population is limited to the European population, and it cannot be proved whether the research results can be extended to other populations; In addition, there is inherent bias in MR research, and even if measures are taken to identify and eliminate abnormal variations, the possibility of unobserved pleiotropic impression results cannot be ruled out.
Conclusion
To sum up, this study used a two-sample, MVMR analysis method, and the results showed a positive correlation between body composition including BMI and WC and the risk of SSI, indicating the importance of SSI prevention in patients with obesity. More research is needed in the future to validate our conclusions and elucidate the underlying biological mechanisms.
Footnotes
Acknowledgment
The authors are grateful to the researchers who provided the original data.
Authors’ Contributions
Conception and design: Y.W. and K.L. Administrative support: K.L. Provision of study materials or patients: N.C. Collection and assembly of data: J.Y. and Y.Y. Data analysis and interpretation: J.Y. and N.C. Manuscript writing: J.Y. and Y.W. Final approval of article: All authors.
Data Availability Statement
Funding Information
This work is supported by the
Author Disclosure Statement
All authors have completed the International Committee of Medical Journal Editors (ICMJE) uniform disclosure form. The authors have no conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.