
Abstract
Background:
Antimicrobial resistance represents a continuing threat to the health of patients with intra-abdominal infections (IAIs). This study aimed to provide clinicians with guidance to optimize antibiotic therapy.
Methods:
The clinical data and antibiotic susceptibility results of pathogens from patients with IAIs from 2017 to 2022 were retrospectively collected. The 6-year period was segmented into two stages, namely, the early (2017–2020) and recent stages (2021–2022). The distribution and antibiotic resistance of pathogens were compared between the stages.
Results:
In total, 5,795 pathogens were isolated from 2,283 patients diagnosed with IAIs. Gram-negative bacteria, Gram-positive bacteria, and fungi accounted for 71.0%, 21.4%, and 7.5% of the isolates, respectively. Klebsiella pneumoniae (1,037, 17.9%) was the primary isolate. The proportion of extended-spectrum β-lactamase-producing Enterobacteriaceae was 89.8% (2,028/2,259), with extended-spectrum β-lactamase-producing Escherichia coli and K. pneumoniae accounting for 27.4% and 43.2%, respectively, of all such isolates. The carbapenem resistance rates of E. coli and K. pneumoniae were 17.1% and 75.9%, respectively. Compared with that in the early stage, the imipenem resistance rate of E. coli was significantly higher in the recent stage (13.8% vs. 25.1%, p < 0.001). Among Gram-positive bacteria, 88 strains of vancomycin-resistant Enterococcus were detected, giving a resistance rate of 10.3%, and the detection rate of methicillin-resistant Staphylococcus aureus was 65.7%.
Conclusions:
Enterobacteriales and non-fermentative bacteria from IAIs remain highly resistant to carbapenems. The epidemiological characteristics and antibiotic resistance profiles of pathogens in various regions should be closely monitored to mitigate the appearance of drug-resistant bacteria in clinical settings.
Introduction
Intra-abdominal infections (IAIs) represent the second most common infectious disease in the intensive care unit (ICU), and they carry high mortality rates.1,2 They primarily encompass infections of various abdominal viscera, such as necrotizing pancreatitis, biliary tract infection, and digestive tract fistula complicated by IAIs. The common pathogens include Enterobacteriales, non-fermentative bacteria, and Enterococcus. Escherichia coli and Klebsiella pneumoniae are the prevalent isolates in the Asia–Pacific region.3,4 However, nosocomial infections caused by carbapenem-resistant Enterobacteriaceae (CRE) have become more prevalent in recent years,5,6 and they are associated with considerably high mortality and disability rates. According to relevant research, the mortality rate of severe IAIs caused by CRE exceeds 50%, posing an enormous challenge to global public health.7,8 In the last decade, a number of international large-scale studies on pathogens surveillance and antimicrobial resistance revealed that the distribution and antibiotic resistance of pathogens significantly differed in different regions.3,6,9 Therefore, it is particularly vital to continuously monitor antimicrobial resistance in regional IAIs and select reasonable empirical antibiotic therapy to further improve the prognosis of patients and reduce the mortality of IAIs.
This study analyzed the epidemiological characteristics and antibiotic susceptibility of pathogens causing IAIs over a 6-year period with a focus on the resistance of Enterobacteriales and non-fermentative bacteria to β-lactam antibiotics, as well as the prevalence of CRE.
Methods
Collection of clinical data and isolates
The clinical data of 2,283 patients with IAIs admitted to Jinling Hospital, Nanjing Medical University, from January 1, 2017, to December 31, 2022, were retrospectively collected. In total, 5,795 strains were isolated, including 3,082 (53.2%) from the ICU. Nanjing Jinling Hospital is a representative Grade-III Class-A hospital in eastern China with 3,100 beds. In recent years, this hospital has admitted an average of 53,000 inpatients, and 27,000 surgeries are performed annually. More than 500 patients with intestinal fistula complicated by IAIs were admitted. In this study, patients aged ≥18 years who met the diagnostic criteria of IAIs as defined by the expert consensus on sepsis 10 were eligible. The exclusion criteria were as follows: hospitalization duration <72 h, pregnancy in women, prior organ transplantation, incomplete clinical data, and suspected IAIs caused by parasites or viruses. The following collected clinical data were collected: demographic data (i.e., age, gender); etiologies of IAIs, such as necrotizing pancreatitis, digestive tract fistula, and simple biliary tract infection; complications, including hypertension, diabetes mellitus, cancers, other chronic underlying diseases, sepsis, and septic shock; and the results of species identification and antibiotic susceptibility testing. The majority of abdominal specimens, including pus, pancreatic fluid, and abdominal drainage fluid, were collected during hospitalization. Only the initial positive culture result for each pathogen was included. The isolates were cultured in the Clinical Microbiology Laboratory of Nanjing Jinling Hospital.
Approval for this study was obtained from the Clinical Research Ethics Committee of Nanjing Jinling Hospital, and the requirement for informed consent was waived (ethics approval number: 2024DZKY-001-01).
Antibiotic sensitivity testing and species identification
All isolates were identified and tested using the VITEK2-Compact automatic microbial analysis system at the Clinical Microbiology Laboratory of Nanjing Jinling Hospital. The results of antibiotic susceptibility testing were interpreted following the latest standard of the Clinical and Laboratory Standards Institute (CLSI). In this study, the method recommended by CLSI was used for interpreting extended-spectrum β-lactamase-producing Enterobacteriaceae (ESBL-E). 11
Statistical analysis
SPSS 25.0 was used for data analysis. Descriptive statistics were conducted for both continuous and categorical data. The independent-sample t-test was used for continuous data. Non-normally distributed data were analyzed using the Mann–Whitney U test. Categorical data were presented as frequencies and percentages, and the differences between the stages were compared using the chi-squared test or Fisher exact test. p < 0.05 denoted statistical significance.
Results
Basic information of patients with IAIs collected from 2017 to 2022
The 2,283 patients with IAIs included 1,601 men and 682 women with an average age of 48.5 years. The direct etiologies of IAIs mainly included necrotizing pancreatitis (3,034/5,795, 52.4%), digestive tract fistula (2,904/5,795, 50.1%), biliary tract infection complicated by other diseases (1,266/4,595, 21.8%), and simple biliary tract infection (481/5,795, 8.3%, Supplementary Table S1).
The specimens collected for IAIs included abdominal drainage fluid (813, 35.6%), pus (617, 27.0%), pancreatic juice (558, 24.4%), and bile (201, 8.8%). Polymicrobial-associated IAIs were detected in 1,614 cases (70.7%), whereas the remaining 669 cases (29.3%) involved monomicrobial IAIs (Fig. 1a).
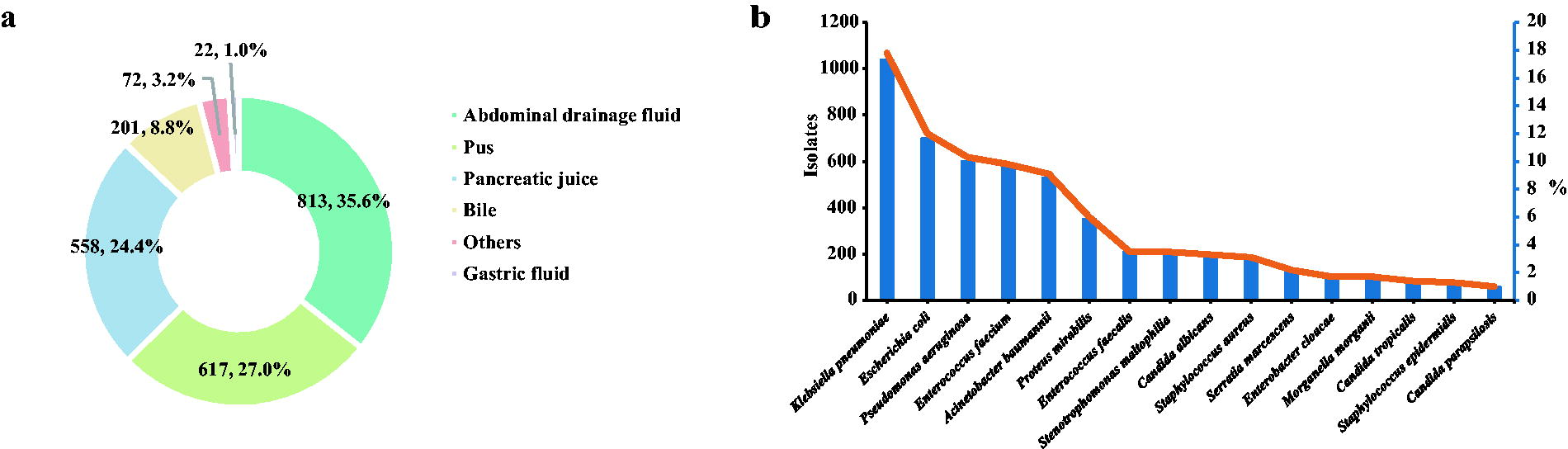
Composition of pathogens
The top five isolates were K. pneumoniae (1037, 17.9%), E. coli (697, 12.0%), Pseudomonas aeruginosa (600, 10.4%), Enterococcus faecium (573, 9.9%), and Acinetobacter baumannii (529, 9.1%, Table 1, Fig. 1b), which collectively accounted for 59.3% of all isolates. Gram-negative bacteria constituted the majority of isolates (4,117, 71.0%). These isolates included 2,399 strains of Enterobacteriales (41.4%), which principally consisted of Klebsiella spp. (1,132, 43.6%). Non-fermentative bacteria accounted for 1,419 strains (24.5%), predominantly consisting of Pseudomonas spp. (611, 43.1%) and Acinetobacter spp. Gram-positive bacteria comprised 1,243 isolates (21.4%), mainly including E. faecium (573, 46.2%), E. faecalis (208, 16.8%), and Staphylococcus aureus (181, 14.6%). Fungi comprised 435 isolates (7.5%, Supplementary Fig. S1a–e).
Composition of Pathogens in IAIs from 2017 to 2022
IAIs = intra-abdominal infections.
Antibiotic resistance of pathogens
The resistance rate of Enterobacteriales to carbapenems (imipenem or meropenem) was 45.8% (1,190/2,599), and E. coli and K. pneumoniae accounted for 10.0% and 66.5%, respectively, of carbapenem-resistant isolates (Fig. 2a). The resistance rates of K. pneumoniae to cephalosporins, β-lactamase inhibitors, and quinolones were relatively high, ranging from 72.1% to 87.4%. Conversely, the resistance rates of E. coli to piperacillin/tazobactam (21.7%), imipenem (17.1%), and cefotiam (19.7%) were comparatively low, whereas resistance to other β-lactam antibiotics remained relatively frequent (49.2%–89.8%).
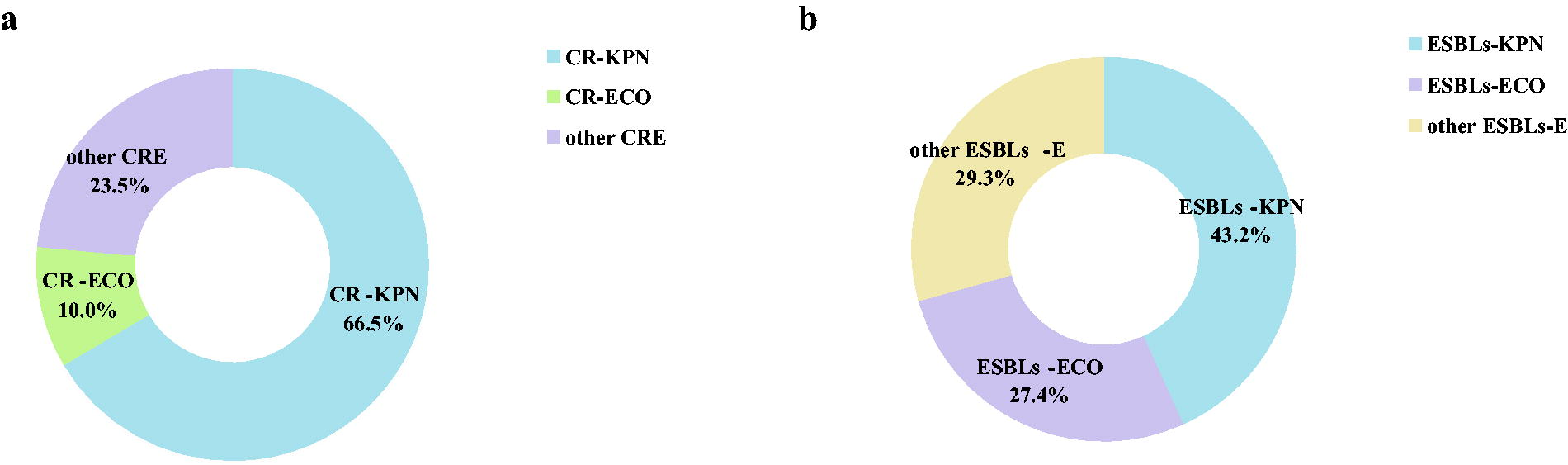
The detection rate of ESBL-E was 89.8% (2028/2259), with ESBL-producing E. coli (ESBL-ECO) and K. pneumoniae (ESBL-KPN) accounting for 27.4% and 43.2%, respectively, of ESBL-E isolates (Fig. 2b). The resistance rates of ESBL-E to amikacin (23.3%), imipenem (43.7%), and piperacillin/tazobactam (47.7%) were comparatively low, whereas resistance to cephalosporins and quinolone antibiotics was common (65.2%–78.6%).
Regarding non-fermentative bacteria, P. aeruginosa exhibited a relatively high rate of amikacin sensitivity (84.0%). Nevertheless, A. baumannii displayed high resistance to ampicillin/sulbactam, imipenem, and cephalosporins (92.4%–97.9%, Table 2).
Sensitivity of Major Gram-Negative Bacteria Detected in IAIs to Commonly Used Antibiotics
“–*” indicates that the pathogen is naturally resistant to the antibiotic. “–” indicates that the data are incomplete.
AMP = ampicillin; PIP = piperacillin; ATM = aztreonam; TZP = piperacillin/tazobactam; SAM = ampicillin/sulbactam; LVX = levofloxacin; CIP = ciprofloxacin; CZO = cefazolin; CTT = cefotiam; CXM = cefuroxime; CAZ = ceftazidime; FEP = cefepime; CRO = ceftriaxone; IPM = imipenem; MPM = meropenem; SXT = compound sulfamethoxazole; AMK = amikacin; GEN = gentamicin; TOB = tobramycin.
Concerning Gram-positive bacteria, E. faecium was more frequently resistant to common antibiotics than E. faecalis, although both pathogens were sensitive to linezolid and trimethoprim/sulfamethoxazole. In total, 88 vancomycin-resistant Enterococcus (VRE) isolates were detected, giving a resistance rate of 10.3%. The detection rate of methicillin-resistant S. aureus was 65.7%, and S. aureus was 100% sensitive to vancomycin, linezolid, and tigecycline (Table 3).
Sensitivity of Major Gram-Positive Bacteria Detected in IAIs to Commonly Used Antibiotics
“–” indicates that the data are incomplete. Methicillin-resistant S. aureus, herein refers to S. aureus resistant to oxacillin.
PEN = penicillin G; OXA = oxacillin; MFX = moxifloxacin; TCY = tetracycline; CLI = clindamycin; ERY = erythromycin; VAN = vancomycin; QDA = quinupristin/dalfopristin; STH = streptomycin; RIF = rifampin; TGC = tigecycline; LNZ = linezolid; SXT = compound sulfamethoxazole.
Antibiotic resistance profiles of pathogens in the early and recent stages
From 2017 to 2020, increasing resistance rates were observed for five major bacterial isolates. However, since 2020, both resistance and detection rates have notably decreased, particularly concerning the resistance of K. pneumoniae and P. aeruginosa to β-lactam antibiotics. In addition, the detection rates of K. pneumoniae and E. coli also decreased after 2020. The resistance of A. baumannii to gentamicin and cefepime displayed a downward trend (Supplementary Fig. S2a–f). Consequently, the study period was divided into two stages for comparison, namely, the early (2017–2020) and recent stages (2021–2022). Patients treated in the recent stage were older (p = 0.019), and the proportion of IAIs caused by digestive tract fistula and intra-abdominal abscesses increased (p = 0.001 and p = 0.011, respectively, Supplementary Table S2).
Regarding Enterobacteriales, the resistance rates of K. pneumoniae to ampicillin/sulbactam and cefotiam were significantly lower (both p < 0.001) in the recent stage, whereas the rate of imipenem resistance did not significantly change (76.5% vs. 74.5%, p = 0.482). Conversely, in E. coli, increased rates of piperacillin/tazobactam (p = 0.002) and imipenem resistance (13.8% vs. 25.1%, p < 0.001) were observed in the recent stage. Concerning CRE, most isolates were carbapenem-resistant K. pneumoniae (CR-KPN; 791/1190, 66.5%). Carbapenem-resistant E. coli (CR-ECO) comprised a low proportion of isolates in both stages (8.8% vs. 12.3%, p = 0.055). Regarding ESBL-E, the detection rate of ESBL-KPN remained comparatively high in both stages (43.8% vs. 42.1%, p = 0.471), whereas the proportion of ESBL-ECO was relatively lower in the recent stage (28.8% vs. 24.3%, p = 0.034, Supplementary Fig. S3). Concerning non-fermentative bacteria, the resistance rates of P. aeruginosa to piperacillin/tazobactam, amikacin, and gentamicin decreased notably in the recent stage (p < 0.001, p = 0.005, and p = 0.010, respectively). Similarly, the resistance rates of A. baumannii to ampicillin/sulbactam and cefazolin were lower in the recent stage (p = 0.010 and p = 0.006, respectively), whereas that of levofloxacin was higher (p < 0.001).
Concerning Gram-positive bacteria, there was no remarkable change in the vancomycin resistance rate in E. faecium in the recent stage (11.6% vs. 13.2%, p = 0.579, Supplementary Tables S3, S4, S5, S6 and S7).
Antibiotic resistance of pathogens before and after the onset of the coronavirus disease 2019 pandemic
On the basis of the onset of coronavirus disease 2019 (COVID-19), the 6-year period was divided into the pre-infection (2017–2019) and post-infection stages (2020–2022). Compared with patients encountered in the pre-infection stage, those treated in the post-infection stage exhibited higher rates of hypertension, diabetes mellitus, and malnutrition (p = 0.031, p = 0.001, and p = 0.001, respectively), whereas no significant differences in disease severity rates (sepsis and septic shock) were discovered.
For K. pneumoniae, the amikacin and cefazolin resistance rates were higher in the post-infection stage (p = 0.015 and p < 0.001, respectively). Likewise, in E. coli, the piperacillin/tazobactam, imipenem, amikacin, and levofloxacin resistance rates were higher in the post-infection stage (p = 0.004, p < 0.001, p < 0.001, and p = 0.008, respectively). Among Enterobacteriales, the detection rate of CR-ECO increased over time (8.2% vs. 11.8%, p = 0.037), as did the ciprofloxacin and levofloxacin resistance rates in P. aeruginosa (p = 0.003 and p = 0.002, respectively). The resistance rates of A. baumannii to levofloxacin increased over time (p = 0.003), as did the resistance rates of E. faecium to vancomycin and tetracycline increased (p < 0.001 and p = 0.030, respectively, Supplementary Tables S8, S9, S10, S11, S12 and S13).
Discussion
The findings of this study revealed that K. pneumoniae exhibited the highest detection rate (17.9%) in IAIs induced by necrotizing pancreatitis, biliary tract infection, and digestive tract fistula, contradicting prior research in which E. coli was the predominant isolate. 12 This could be attributed to the impairment of intestinal barrier function and dysbiosis of the intestinal flora, resulting in alterations in the bacterial composition of IAIs. 13 Furthermore, the patients with IAIs admitted to our center were mainly accompanied with intestinal fistula, even sepsis. Only a few patients experienced simple biliary tract infections and appendicitis. It is noteworthy that the rates of imipenem (75.9% vs. 24.8%) and meropenem resistance (76.3% vs. 26.0%) in K. pneumoniae were considerably higher than those reported by the China Antimicrobial Surveillance Network in 2023. 14 The high drug resistance and detection rates of K. pneumoniae in this study might be related to the serious illness of most patients.
Meanwhile, recent studies suggested that the resistance of K. pneumoniae to carbapenems in central and eastern China, particularly in Jiangsu and Zhejiang provinces, was apparently higher than that in other regions, in line with our findings.3,15 Because K. pneumoniae has strong genetic plasticity, virulence or drug resistance genes can widely spread through horizontal transfer, contributing to the high mortality rate of CR-KPN in the ICU 16 and representing an intractable challenge to clinical therapy.6,17 On the basis of the high resistance rate of K. pneumoniae in our center, 58.7% (84/143) of isolates produced K. pneumoniae carbapenemase (KPC) in 2015–2016. 18 Then, 231 patients with blood infections caused by CR-KPN were conducted in another article from 2020 to 2022, 10.8% of CR-KPN isolates harbored blaKPC and blaNDM, and 89.2% produced KPC, 19 highlighting the significance of epidemiological surveillance. Therefore, strict adherence to infection control measures and judicious antibiotic use are crucial to mitigating the emergence of drug-resistant bacteria.
Concerning other Gram-negative bacteria, the rate of imipenem resistance in E. coli was 17.1%, where a significant increase was observed in the recent stage (13.8% vs. 25.1%, p < 0.001). Among non-fermentative bacteria, the imipenem resistance rates in A. baumannii and P. aeruginosa were 97.9% and 71.5%, respectively. The current study revealed a high rate of resistance among Gram-negative bacteria to a variety of antibiotics commonly used in clinical practice, especially carbapenems. This might be attributable to the fact that most patients were transferred from other hospitals, and most of them had already developed infections caused by multidrug-resistant strains before admission or had received long-term antimicrobial therapy.
In recent years, antimicrobial resistance has become increasingly serious, especially with the emergence of CRE. The detection rate of CRE in this study was 45.8%, with the majority being CR-KPN (66.5%), in line with previous findings.12,20 Additionally, prior research indicated that previous carbapenem use was a significant risk factor for CRE infection,12,21 with other factors including invasive procedures, ICU hospitalization, intravascular catheter usage, and ICU admission within the past 90 days. 22 Given the high prevalence of CRE in our hospital, it is imperative to promptly standardize empirical antibiotic therapy, reduce the misuse of carbapenems, and strengthen the active surveillance of CRE by clinical departments to curb the development of bacterial resistance.
The detection rate of ESBL-E was 81.4%, with ESBL-KPN accounting for 43.2% of the isolates, which was significantly higher than that reported in the Asia–Pacific region. 23 ESBL-E exhibited comparatively high rates of resistance to cephalosporins and quinolones (65.2%–78.6%). Consequently, these two antibiotic classes are no longer recommended as empirical antibiotic therapy for IAIs.24,25 However, ESBL-E remained highly sensitive to piperacillin/tazobactam and imipenem with susceptibility rates of 52.3% and 56.3%, respectively. These findings were consistent with those of The Study for Monitoring Antimicrobial Resistance Trends,9,26 which described piperacillin/tazobactam and carbapenems as the most effective antibiotics for treating ESBL-E.27,28 The plasmid-mediated transfer of ESBL genes can confer resistance to several antibiotics. 29 Additionally, intestinal colonization of ESBL-E was identified as an independent risk factor for surgical site infection. 30 Consequently, active detection of ESBL-E is imperative.
Drug resistance in A. baumannii has escalated over time. 31 The resistance of A. baumannii to commonly used β-lactam antibiotics was notably common (92.4%–97.9%), whereas levofloxacin resistance was less frequent (71.8%). This trend aligns with findings from another single-center study conducted in China, suggesting that combination therapy involving levofloxacin and other antibiotics could represent a viable alternative tactic. 32 Nonetheless, it was noteworthy that levofloxacin resistance in A. baumannii was evidently more common in the recent stage (66.7% vs. 82.7%, p < 0.001). Hence, enhanced surveillance of carbapenem-resistant A. baumannii is warranted in the future.
In line with the findings of De et al.,1,28 Enterococcus (68.5%) was the most common Gram-positive bacterium. The resistance rates of E. faecium to oxacillin and quinolones were comparatively high (94.0%–96.6%), indicating that they should be cautiously used in the clinic. Furthermore, 88 VRE isolates were detected, resulting in a resistance rate of 10.3%. Additionally, the vancomycin resistance rate in E. faecium increased during the post-infection stage of COVID-19 (p < 0.001), and the rate was significantly higher than that reported in other studies.10,33 Considering the epidemic threat posed by VRE in central and eastern Europe 34 and the specific condition in our hospital, particularly concerning patients with IAIs complicated by sepsis or septic shock, the indications for vancomycin should be strictly regulated to reduce the prevalence of VRE and prevent cross-infection and nosocomial spread.
This study observed a significant downward trend in pathogen resistance to various antibiotics after 2021. Compared with the findings in the early stage, the ampicillin/sulbactam resistance rate in K. pneumoniae decreased from 89.4% to 79.8% (p < 0.001) and the piperacillin/tazobactam resistance rate in P. aeruginosa decreased from 46.3% to 40.7% (p < 0.001) in the recent stage, which might be attributable to the implementation of infection and control measures within the hospital, including strengthened management of β-lactamase inhibitor compounds.
Meanwhile, the resistance rates of E. coli to piperacillin/tazobactam (p = 0.004), amikacin (p < 0.001), and levofloxacin (p = 0.008), and that of P. aeruginosa to levofloxacin (p = 0.003) increased during the post-infection stage, consistent with the findings of relevant domestic studies.35,36 Data from The Lancet indicated that ∼95% of patients diagnosed with COVID-19, in the absence of concomitant bacterial infection, received broad-spectrum antibiotics. 37 This highlights a global imbalance in antibiotic management exacerbated by viral infections, leading to a dramatic increase, in antimicrobial resistance. Previous research revealed that patients with COVID-19 complicated by IAIs had a serious condition necessitating more invasive procedures, 38 potentially fueling the development of CRE. In line with this, the detection rate of CRE-ECO increased over time in this study (8.2% vs. 11.8%, p = 0.037).
Two or more pathogens were detected in 70.7% of patients with IAIs, indicating polymicrobial-associated IAIs. The potential causes include the higher numbers of IAIs caused by intestinal fistula. This both complicates antibiotic use and increases the inflammatory burden in patients. A review of international consensus regarding IAIs indicated that carbapenem-based combination antimicrobial therapy is recommended. 39 This combination therapy has been verified to improve survival in patients with blood stream infections caused by CRE. 40
Although antibiotic therapy plays an indispensable role in IAI treatment, both domestic and international guidelines generally emphasize that early infection source control is the key aspect of treatment.41,42 Delayed or incomplete infection source control can result in adverse events such as prolonged hospital stays and an increased incidence of severe cases, as well as increased bacterial resistance attributable to prolonged anti-infective therapy. 3 Therefore, clinical workers must pay attention to this issue.
This study had multiple limitations. First, this was a single-center retrospective study. However, Jinling Hospital is the largest center for intestinal fistula and IAIs treatment in China, and critically ill patients arrive at our hospital from other institutions throughout the country. Thus, our research might reflect the serious situation of drug-resistant bacteria related to IAIs across China rather than regional resistance. Second, susceptibility testing for individual antibiotics was not fully performed in this study.
Conclusions
Our findings illustrated the evolving trends in the epidemiological characteristics and antimicrobial resistance of pathogens associated with IAIs in China over time. Furthermore, they shed light on the true prevalence of antimicrobial resistance among pathogens during the COVID-19 pandemic. In particular, the resistance of Gram-negative bacteria to carbapenems is becoming an increasingly serious problem, underscoring the need for continuous surveillance of antimicrobial resistance trends for pathogens across different regions.
Footnotes
Acknowledgments
Authors’ Contributions
M.W. and J.R. devised and designed the study. M.W., J.L., Z.Z., Y.C., W.W., J.W., S.T., and L.W. were responsible for the collection of clinical data and resolution of problems via discussion as necessary. M.W. served as the primary statistician for the study and drafted the article. All authors reviewed the article, which was revised in response to comments by M.W., T.Z., and X.W. J.R. was responsible for the article as a whole. All authors read and approved the final article.
Author Disclosure Statement
All authors have nothing to disclose.
Funding Information
The study was supported by the Key Research and Development Program of Jiangsu Province (BE2022823), Jiangsu Provincial Medical Innovation Center (CXZX202217), Jiangsu Key Research and Development Plan (BE2021727), and Navigation Project of Clinical Research (22LCYY-LH4).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.