
Abstract
Objective:
To assess the link between systemic immune-inflammation index (SII) and risk of major adverse cardiovascular events (MACE), contrast-induced nephropathy (CIN), and overall mortality in patients with acute myocardial infarction (AMI).
Patients and Methods:
Electronic search of PubMed, EMBASE, Web of Science, and Scopus databases was done for observational studies with the data on the association of SII and outcomes, such as MACE, and CIN in adult (≥18 y) patients with AMI. A random-effects model was used, and the pooled effect sizes were expressed as relative risk (RR) with corresponding 95% confidence intervals (CI). Subgroup analysis was conducted on the basis of the type of AMI (ST elevation myocardial infarction and non-ST elevation myocardial infarction), sample size (≥500 and <500), and study design. GRADE assessment was used to evaluate the certainty of the evidence.
Results:
The analysis included 23 studies. Most studies were conducted in China (n = 13), followed by Turkey (n = 10). Majority of the studies (n = 20) had a retrospective cohort design. Patients with high SII had increased risk of MACE (RR 2.95, 95% CI: 1.25, 6.99; n = 5, I2 = 97.5%), overall mortality (RR 2.59, 95% CI: 1.64, 4.07; n = 6, I2 = 58.0%), and CIN (RR 4.58, 95% CI: 3.44, 6.10; n = 4, I2 = 0.0%), compared with patients with lower SII. Egger’s test detected publication bias for MACE (p = 0.047) and overall mortality (p = 0.012) but not for CIN. These associations remained valid in subgroup analysis.
Conclusion:
Findings suggest that higher SII in patients with AMI is associated with increased risks of MACE, CIN, and overall mortality. This underscores SII’s potential as a prognostic marker in AMI.
Introduction
In recent years, the research focuses on understanding the role of inflammation in the pathogenesis and progression of cardiovascular diseases (CVD).1,2 Systemic immune-inflammation index (SII) was first proposed by Hu et al. to reflect the balance between systemic inflammation and immune response. 3 This index takes into account peripheral blood counts of neutrophils, lymphocytes, and platelets and has been proposed as a novel, easy, and cost-effective prognostic marker in various malignancies and inflammatory conditions.3–7 The utility of SII in predicting outcomes in CVD has become a focus of numerous studies.8–10 A recent review by Ye et al. (2022) that included 13 studies with 153,000 participants found that higher SII levels were significantly linked to an elevated risk of CVD, such as ischemic stroke, hemorrhagic stroke, myocardial infarction, and peripheral arterial disease. 11
Acute myocardial infarction (AMI) is one of the main causes of morbidity and mortality worldwide. 12 Although primary percutaneous coronary intervention (PCI) is considered a preferable treatment method for patients with AMI,13,14 it is often complicated by the development of contrast-induced nephropathy (CIN) that leads to substantial in-hospital and long-term morbidity and mortality.15,16 Understanding the association between SII and AMI outcomes could potentially provide valuable insights into the underlying mechanisms of inflammation-mediated cardiac injury and identify high-risk patients who may benefit from tailored therapeutic strategies. This study aims to evaluate the association of SII with important outcomes, such as major adverse cardiovascular events (MACE), CIN, and overall mortality following AMI. The underlying hypothesis was that high level of SII would be associated with increased risk of adverse outcomes in patients with AMI. Although CIN is primarily a complication arising from interventions for AMI, its inclusion as one of the outcomes is because of its clinical relevance and the potential interaction between systemic inflammation and CIN development. Inflammation could exacerbate CIN risk, and understanding this relationship may lead to better patient management and preventative strategies post-AMI.
Patients and Methods
Database search and tactic used
Electronic search of PubMed, Web of Science, Scopus, and Embase databases was done using a well-defined search tactic that consisted of the following key words: (“Acute Myocardial Infarction”[Mesh] OR “Myocardial Infarction”[Mesh] OR “Heart Attack” OR “AMI”) AND (“Inflammation”[Mesh] OR “Systemic Immune-Inflammation Index” OR “SII”) AND (“Prognosis” OR “Mortality” OR “MACE” OR “nephropathy” OR “CIN” OR “Treatment Outcome”). Studies that were published between January 1, 1990, and March 15, 2024, were considered eligible for inclusion. Bibliography sections of the studies were further searched for any relevant studies. The adherence to the PRISMA guidelines was ensured, 17 and the study protocol was prospectively registered at PROSPERO with the registration number CRD42024526309.
Criteria for inclusion and exclusion
Inclusion criteria were set to identify studies meeting specific parameters. We included studies published in the English language to ensure consistency and to avoid potential challenges in accurately translating and interpreting nuanced medical and scientific terms, which could lead to errors or misinterpretations. By focusing on English-language studies, we also aimed to ensure that the data are verifiable by a broad audience of researchers and clinicians. Eligible studies were required to investigate the relationship between SII and significant outcomes of AMI. The exposure of interest was SII which is calculated as neutrophil count (109/L) × platelet count (109/L)/lymphocyte count (109/L). Studies including SII as either a categorical or continuous variable were considered. There were no exclusions on the basis of the cutoff criteria used to define low and high SII. Importantly, SII measurements in eligible studies were required to be taken at the time of AMI presentation, not following management, as measuring SII at the time of AMI presentation would provide an accurate reflection of the patient’s baseline inflammatory and immune status at the onset of the event. SII levels can be substantially influenced by various medical interventions that patients undergo after an AMI, such as antiplatelet therapy, statins, or other anti-inflammatory treatments. Measuring SII after these interventions could introduce confounding factors that may obscure the true relationship between baseline inflammation and clinical outcomes. By restricting the inclusion of studies reporting measurements to the time of AMI presentation, we intended to minimize these confounding effects, ensuring that the SII values used in the analysis more accurately reflect the initial pathophysiological state. Also, for SII to be a reliable prognostic marker, it is essential that the measurements correspond to the period when clinical decisions are made, which is typically at the time of presentation. SII levels measured at this critical juncture are more likely to provide valuable information for predicting adverse outcomes, and guiding early risk stratification and management strategies. The outcomes of interest included MACE, CIN, and mortality. Studies involving adult participants (aged ≥18 y) were eligible. Both cohort (prospective and retrospective) and case–control study designs were included. The review incorporated studies published between January 1, 1990, and March 15, 2024. Studies with patients that had cardiac conditions other than AMI were excluded. Additionally, studies not reporting on specific outcomes of interest were excluded. Case reports, case series, conference abstracts, and reviews were considered for exclusion.
Selection of studies and data extraction
After literature search, the initial set of studies was deduplicated. Two authors (W.S. and Z.C.) independently conducted screening of the title and abstract of the remaining studies, and relevant studies underwent full-text evaluation to identify studies that meet the eligibility criteria. Data extraction from the finalized set of studies was independently performed by two authors (W.S. and Z.C.), utilizing a structured form that underwent pilot-testing and refinement for efficiency. Any discrepancies in decisions regarding study inclusion and data extraction were resolved through discussions.
Quality assessment
Quality assessment was done using the Newcastle–Ottawa Scale (NOS) 18 that evaluates studies on the basis of three key categories: selection of study groups, comparability of groups, and ascertainment of exposure or outcome. Each category comprises several items, with individual scoring, with a maximum score of 9 points. 18 Scores above 6 were considered of satisfactory quality.
Statistical analysis
Analysis was performed using STATA version 15.0. We did not establish any cutoffs for SII. Instead, we relied on the cutoff values reported in the individual studies and used their classification of SII levels as high or low. Pooled effect sizes were presented as relative risk (RR) along with 95% confidence intervals (CI). Our primary analysis focused on the exposure being categorical, specifically high and low SII categories, on the basis of cutoffs adopted by individual studies. We reasoned that a categorical exposure would have greater clinical decision-making influence and facilitate a better understanding of associations with outcomes. A random-effects model was planned for all outcomes because of anticipated substantial differences in baseline characteristics and methodology among included studies. Publication bias was assessed using funnel plots and Egger’s test. 19 Subgroup analysis was conducted on the basis of the type of AMI (ST elevation myocardial infarction [STEMI] and non-ST elevation myocardial infarction [NSTEMI]), sample size (≥500 and <500), and study design: p < 0.05 was statistically significant. We evaluated the certainty of the evidence using the standard GRADE approach and GRADE Pro software. 20
Results
A total of 975 studies were identified by the initial search across the databases. Following the removal of 276 duplicate studies, titles and abstracts of 699 studies were screened, leading to the exclusion of 656 studies. After full-text examination, additional 20 studies were excluded. The final analysis included 23 studies21–43 with a total of 31,716 patients (Fig. 1). Key characteristics of these studies are outlined in Table 1. Most included studies (n = 20) had a retrospective cohort design, two studies had a prospective cohort design, and one was a case–control study. Thirteen studies were conducted in China, and the remaining 10 studies were done in Turkey. Age of the patients ranged from 55 to 75 y, and most patients were males (60%–80%). Fifteen studies reported data of predominantly STEMI patients, whereas in eight studies, most patients had NSTEMI. Most patients underwent PCI. Included studies used different cutoffs to define low and high SII. The definitions adopted for MACE and CIN were clearly defined in studies that reported on these outcomes. Although the definitions of CIN were largely homogenous across the studies, there was a variability in the clinical events categorized as MACE. Most studies defined MACE as a composite of cardiovascular death, myocardial infarction, stroke, unstable angina, and coronary revascularization. Some studies expanded this definition to also include all-cause death, malignant arrhythmias, acute heart failure, transient ischemic attack, and stent thrombosis.

Flow of the study selection.
Included Studies and Their Characteristics
SII = systemic immune-inflammation index; MACE = major adverse cardiovascular events; CIN = contrast-induced nephropathy; NOS = Newcastle–Ottawa Scale score; RC = retrospective cohort; STEMI = ST elevation myocardial infarction; PCI = percutaneous intervention; MI = myocardial infarction; TIA = transient ischemic attack; CAG = coronary artery angiography; NSTEMI = non-ST elevation myocardial infarction; PC = prospective cohort.
Fifteen studies had a NOS score of 7, and eight studies had a score of 8. The mean NOS score was 7.35, indicating good quality.
MACE
High SII correlated with the increased risk of MACE within one year of follow-up (RR 2.95, 95% CI: 1.25, 6.99; n = 5, I2 = 97.5%) (Fig. 2). There was evidence of publication bias on Egger’s test (p = 0.047) and on funnel plot (Supplementary Fig. S1). The overall certainty of evidence was judged to be “very low” according to the GRADE assessment criteria (Supplementary Table S1). Similar findings were observed when SII was considered as a continuous exposure, wherein each unit increase in SII was associated with the increase in the risk of MACE (RR 1.30, 95% CI: 1.01, 1.66; n = 4, I2 = 87.9%) (Supplementary Fig. S2). On subgroup analysis, the association remained substantial when studies with patients who have STEMI and studies with retrospective cohort design were pooled (Table 2). Further, irrespective of the sample size, the association remained substantial. There were no studies examining this association in patients diagnosed with NSTEMI (Table 2).

Risk of MACE among those with high SII, compared with those with low SII. SII = systemic immune-inflammation index; MACE = major adverse cardiovascular events.
Findings of the Subgroup Analysis
Statistical significance at p < 0.05.
MACE = major adverse cardiovascular event; CIN = contrast-induced nephropathy; RR = relative risk; CI = confidence interval; AMI = acute myocardial infarction; STEMI = ST elevation myocardial infarction; NSTEMI = non-ST elevation myocardial infarction; RC = retrospective cohort.
Overall mortality
Patients with high SII presented with increased risk of overall mortality within a year of follow-up (RR 2.59, 95% CI: 1.64, 4.07; n = 6, I2 = 58.0%) (Fig. 3), with the evidence of publication bias (p = 0.0120; Supplementary Fig. S3). The overall certainty of evidence was judged to be “very low” according to the GRADE assessment criteria (Supplementary Table S1). When SII was considered as a continuous exposure, the risk of overall mortality with each unit increase in SII approached statistical significance (RR 1.05, 95% CI: 0.94, 1.16; n = 4, I2 = 78.1%) (Supplementary Fig. S4). Subgroup analysis demonstrated that the increase in the risk of mortality with high SII was present across all subgroups, that is, STEMI and NSTEMI, low and high sample size, and in retrospective cohort studies (Table 2).
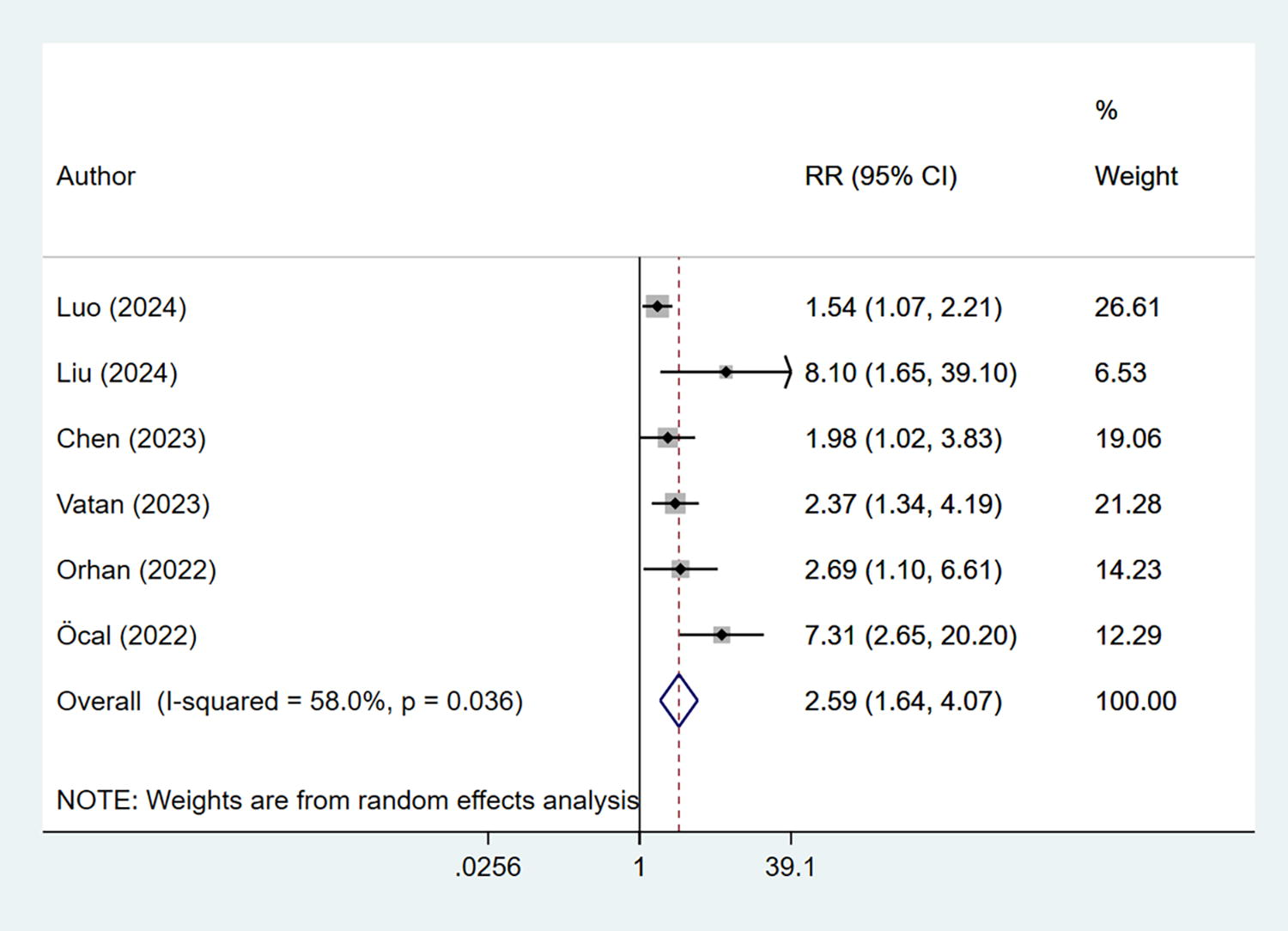
Risk of overall mortality among those with high SII, compared with those with low SII. SII = systemic immune-inflammation index.
CIN
Pooled analysis showed that high SII was linked to the increased risk of CIN (RR 4.58, 95% CI: 3.44, 6.10; n = 4, I2 = 0.0%) (Fig. 4), with no evidence of publication bias (Supplementary Fig. S5). The overall certainty of evidence was judged to be “moderate” according to the GRADE assessment criteria (Supplementary Table S1). When SII was considered as a continuous exposure, each unit increase in SII was associated with elevated risk of CIN (RR 1.01, 95% CI: 1.00, 1.02; n = 5, I2 = 89.0%) (Supplementary Fig. S6). Subgroup analysis revealed that the increased risk of CIN associated with high SII was consistent across all subgroups, including STEMI and NSTEMI, regardless of sample size, and in studies utilizing a retrospective cohort design (Table 2).

Risk of CIN among those with high SII, compared with those with low SII. CIN, contrast-induced nephropathy; SII, systemic immune-inflammation index.
Discussion
Our findings suggest a significant association between elevated SII and adverse outcomes in patients with AMI. High SII correlated with a nearly threefold increase in the MACE risk, more than twofold increase in overall mortality, and a nearly fivefold increase in the risk of CIN. These associations persisted in various subgroups, including patients with ST-segment elevation myocardial infarction and studies with a retrospective cohort design, which further supports the robustness of our results. The certainty of the evidence from our study was judged to be “very low” for MACE and mortality-related outcomes and “moderate” for the outcome related to CIN.
On the basis of the findings of this review, the potential for SII values to influence clinical treatment decisions in patients who suffered AMI might seem promising, particularly for risk stratification and guiding the timing of interventions. It may appear that elevated SII levels could identify high-risk patients who may benefit from more intensive monitoring or targeted therapies. There is also the possibility that SII trends could inform prognosis and treatment response. However, the current evidence is of “very low” certainty, as per GRADE assessment, and not robust enough to support definitive clinical recommendations. Standardized SII thresholds and further research are needed to validate its use in clinical practice and to explore how SII-guided strategies could improve outcomes in patients who suffered AMI.
The association between elevated SII levels and increased risk of MACE can be attributed to several potential mechanisms. Studies show that systemic inflammation plays a pivotal role in the pathogenesis of atherosclerosis, which is the underlying cause of most MACE events.44,45 Elevated SII levels reflect an imbalance in the systemic immune response, with higher neutrophil and platelet counts coupled with lower lymphocyte counts. This dysregulated immune response contributes to endothelial dysfunction, plaque destabilization, and thrombosis, ultimately increasing the risk of MACE, such as myocardial infarction, stroke, and cardiovascular death.46,47 Second, high SII levels are indicative of a prothrombotic state that is characterized by increased platelet activation and aggregation48,49 and higher risk of thrombosis of coronary arteries, leading to acute coronary events. Additionally, elevated neutrophil levels contribute to oxidative stress and tissue damage, exacerbating myocardial injury during ischemic events. 50 Moreover, systemic inflammation, mediated by elevated SII levels, could promote the progression of coronary artery disease by inducing vascular remodeling, fibrosis, and smooth muscle cell proliferation.51,52 These pathological changes further compromise coronary blood flow and increase susceptibility to plaque rupture and subsequent MACE. Therefore, targeting systemic inflammation and immune dysregulation may potentially be a useful therapeutic tactic for reducing the risk of MACE and improving outcomes in patients who suffered AMI.
We found higher risk of CIN in patients who suffered AMI with elevated SII. Systemic inflammation, reflected by elevated SII levels, can lead to endothelial dysfunction and impaired renal perfusion. 53 Inflammatory mediators, such as cytokines and chemokines, disrupt normal renal hemodynamics, reducing renal blood flow and compromising renal function.54,55 Collectively, these events exacerbate renal vasoconstrictive response to contrast media, further impairing renal perfusion and increasing the risk of CIN development. Additionally, the prothrombotic state, associated with high SII levels, may contribute to microvascular thrombosis within the renal vasculature, leading to renal ischemia and tissue injury.48,49 The combination of impaired renal perfusion and microvascular thrombosis worsens renal hypoxia and oxidative stress, further compromising renal function and predisposing to CIN. Studies demonstrated that contrast-induced renal injury triggers inflammatory cascade characterized by the release of proinflammatory cytokines and recruitment of leukocytes to the renal interstitium.56,57 In patients with pre-existing systemic inflammation, such as those with high SII levels, this inflammatory response may be amplified, leading to more severe renal injury and a higher risk of developing CIN. Therefore, strategies aimed at mitigating systemic inflammation and preserving renal function may be crucial in reducing the incidence of CIN and improving outcomes in high-risk patients undergoing contrast-enhanced procedures.
The observed elevated risk of overall mortality in patients with high SII could be linked to adverse cardiovascular outcomes. The prothrombotic state associated with high SII levels increases the risk of thrombotic events, such as recurrent myocardial infarction and ischemic stroke.48,49 Furthermore, systemic inflammation exacerbates myocardial injury, impairs healing, and contributes to adverse cardiac remodeling, leading to ventricular dysfunction and heart failure.58,59 Elevated SII levels may also indicate underlying comorbidities and disease severity, further increasing mortality risk.
In our analysis, the detection of publication bias suggests that the observed associations between elevated SII and increased risks of MACE and overall mortality may be inflated. This means that the actual risk associated with high SII levels could be lower than what our meta-analysis indicates. As a result, the strength of the evidence supporting SII as a prognostic marker for these outcomes is weakened. It underscores the need for more balanced and comprehensive research, including the publication of studies with nonsunbstantial or negative results, to provide a more accurate assessment of the relationship. The implications of publication bias highlight the need for a cautious interpretation of the data and emphasize the importance of ongoing research to validate these findings.
Our study has limitations. The observational nature of the included studies prevents us from establishing causality, and residual confounding may have influenced the observed associations. Additionally, we observed heterogeneity among the included studies, particularly in terms of patient characteristics, follow-up duration, and outcome definitions, which may have introduced bias. Most of the included studies were retrospective in nature, which carries a risk of selection bias and limited the generalizability of our results. Also, studies were restricted to two countries, i.e., China and Turkey, and therefore, our findings have very limited external generalizability. We found presence of publication bias for MACE and overall mortality, potentially skewing our results. Moreover, the lack of standardized cutoff values for defining high and low SII levels across studies may have contributed to variability in the observed associations. Similarly, variations in the timing and methods of SII measurement, as well as differences in the treatment strategies and follow-up protocols among studies, may have influenced our results. Furthermore, we restricted our review to studies published in English language. This may have contributed to the possibility of publication bias and a less comprehensive global perspective.
Conclusion and way forward
Our findings suggest a potential association between elevated SII and increased risks of MACE, CIN, and overall mortality in patients with AMI. However, the high level of bias, substantial heterogeneity in the findings, and the very low quality of evidence warrant caution in interpreting these results. These associations should be considered hypothesis-generating rather than definitive conclusions. Although the findings hint at the potential utility of SII as a prognostic marker, more rigorous and well-designed studies are needed to validate its role in clinical practice. At this stage, SII should not be routinely incorporated into risk assessment protocols without further validation.
The observed association between SII and adverse outcomes emphasizes the need for continued research into the role of systemic inflammation and immune dysregulation in AMI. Prospective studies are necessary to assess the incremental predictive value of SII beyond traditional risk factors and to explore potential therapeutic implications. Until higher-quality evidence is available, any consideration of anti-inflammatory or immune-modulating therapies in patients who suffered AMI with elevated SII levels should be approached with caution and within the context of clinical trials. Finally, the association of SII with CIN highlights the importance of vigilance in patients who suffered AMI and are undergoing contrast-enhanced procedures.
Footnotes
Data Availability
The data underlying this article will be shared upon reasonable request to the corresponding author.
Authors’ Contributions
W.S. and Z.C.: Conceptualization and design. W.S., Z.C., and Y.L.: Methodology, formal analysis, and data curation. W.S. and Z.C.: Supervise, write, review, and edit.
Funding Information
No specific funding was obtained for the trials.
Author Disclosure Statement
The authors have no relevant financial relationships or conflicts of interest to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.