
Abstract
Background:
Stent graft infection (SGI) caused by Burkholderia cepacia complex is rare. The usage of ascending-to-descending aortic bypass (ADAB) in such situations has not yet been fully discussed.
Methods:
Case report and literature review.
Results:
We describe a case of SGI caused by B. cepacia complex after multiple surgical interventions because of an injury from a fall. The successful management encompassed thoracic endovascular aortic repair, antibiotic agents, device removal, and ADAB.
Conclusion:
Our report highlights the ADAB technique in addressing the progression of infection after multiple minimally invasive thoracic procedures for emergent thoracic trauma. The ADAB technique could be considered a viable option in certain clinical scenarios in SGI.
Long-term mortality and morbidity and persistent infection rate of stent graft infection (SGI) remain high. 1 After stabilization with thoracic endovascular aortic repair (TEVAR), some patients might still require open surgical repair (OSR).
SGI caused by the Burkholderia cepacia complex following TEVAR for traumatic events is rare. Herein, we present the case of a patient with SGI caused by the B. cepacia complex, followed by its subsequent management. The Institutional Review Board (IRB) of the Chang Gung Memorial Hospital approved the study protocol and publication of data. The patient provided informed written consent for the publication of the study data (IRB approval number: 202300942B0; Approval date: July 4, 2023).
Report
The patient was a 41-year-old male active triathlete without noteworthy medical history before an injury from a fall. His multiple traumatic injuries included left lung contusion and hemopneumothorax, right lung pneumothorax, traumatic aortic injury grade III (pseudoaneurysm) at the lesser curvature of aorta zone 3 without evidence of dissection or extravasation, 1st to 12th rib fracture, left clavicle fracture, grade I liver laceration on left liver, right pubic ramus fracture, right sacral ala fracture, left iliac wing fracture, right L5 transverse process fracture, left facial bone, skull and skull base fracture, and left orbital wall fracture.
After resuscitation, the patient underwent emergent thoracoscopic partial lung resection with chest tube insertion for massive hemothorax. Ceftriaxone was prescribed to cover the progressing pneumonia resulting from multiple thoracic insults; metronidazole aimed to provide sufficient coverage of suspected peritoneal contamination by the probable traumatic intra-abdominal injury and delayed perforation of the intestine. After respiratory function stabilized, we performed TEVAR landing from zone 3 to T7. Five days later, his blood culture at the initial counter came with a positive B. cepacia complex. His antibiotic agents were shifted to oral clavulanic acid plus amoxycillin. After his clinical condition stabilized, he was discharged with close outpatient follow-up.
Four months later, the patient was admitted to our hospital for hemoptysis. Imaging studies revealed a ruptured pseudoaneurysm at the greater curvature of aorta zone 3, which prompted us to perform a second TEVAR with zone 2 landing, left subclavian artery embolization, and a left-to-right subclavian artery bypass. Blood culture results indicated the presence of the B. cepacia complex. We therefore administered ceftriaxone and vancomycin for six weeks, ertapenem and daptomycin for two weeks, and daptomycin and meropenem for four weeks. He remained afebrile during this hospitalization, and the level of serum C-reactive protein was managed to less than 5 mg/L in the last week. As his clinical conditions stabilized, the patient was discharged with an eight-day course of oral linezolid and levofloxacin. He was scheduled for routine outpatient follow-up.
The patient had bacteremia (B. cepacia complex) even after four months of treatment. Imaging studies (Fig. 1A, B) revealed persistent infection and a stent-induced new entry tear (SINE). Consequently, he was readmitted for operation under cardiopulmonary bypass and cardioplegia with the following procedures:
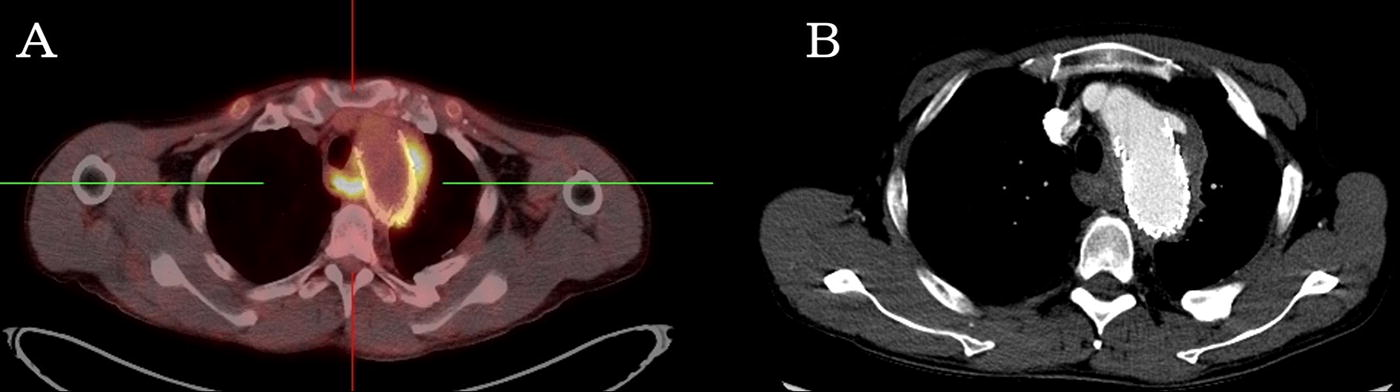
Positron emission tomography–computed tomography
The infected aorta was resected from zone 1 to T8, the infected stent was removed, and primary closure of the aortic arch at zone 1 was performed.
Ascending-to-descending aortic bypass (ADAB) was performed with an 18-mm Gelsoft graft (Terumo, Japan) end-to-side anastomosed to the ascending aorta. The graft extended caudally, passed adjacent to the right atrium, traversed between the right ventricle and the diaphragm, and posteriorly passed through the posterior pericardium. Subsequently, it was anastomosed to the thoracic descending aorta (Fig. 2A, B).
The left carotid artery was debranched with an 8-mm Gelsoft graft connected to the 18-mm Gelsoft graft.
The final reconstructed three-dimensional image is presented in Figure 2C and Supplementary Video SV1. Follow-up examinations revealed no signs of residual infection. The patient recovered with no complications.
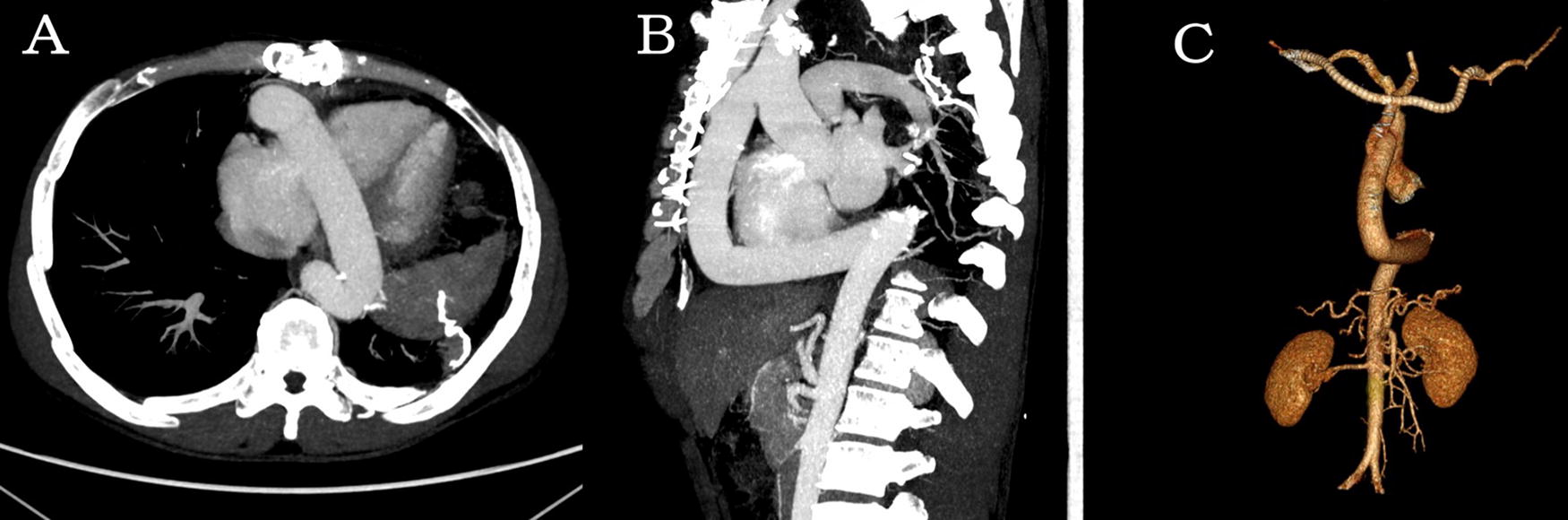
Surgical procedures included the resection of the infected aorta spanning from zone 1 to T8, removal of the infected stent, and primary closure of the aortic arch at zone 1. Subsequently, the graft extended caudally, following a course toward the right atrium, passing between the right ventricle and the diaphragm, traversing posteriorly through the posterior pericardium, and finally being anastomosed to the descending thoracic aorta. Additionally, the left carotid artery was debranched using an 8-mm Gelsoft graft for anastomosis to the 18-mm Gelsoft graft
Comment
The most common pathogens associated with infected aortic aneurysm (IAA) are Salmonella spp., Staphylococcus spp., and Streptococcus spp, accounting for 60% of IAA cases. 2 The B. cepacia complex, a group of gram-negative bacilli and opportunistic pathogens, has been implicated in health-care–associated nosocomial infection outbreaks in the last decade. 3 This complex may be transmitted through contaminated healthcare devices 4 or from pre-transplant colonization in donor lungs to immunosuppressed recipients.
Our patient was not immunocompromised nor a lung transplant recipient. Therefore, his presentation of post-TEVAR IAA and SGI caused by the B. cepacia complex is uncommon. With the increasing TEVAR and thoracoscopic procedures for thoracic trauma, similar cases may be encountered in the future, particularly in patients with trauma with concurrent transient bacteremia.
Long-term mortality and morbidity and persistent infection rate remain high in patients with SGI without device explantation. 1 For these patients, OSR is the preferred approach, with TEVAR often serving as transient stabilization. 1
Current literature does not indicate a clear preference for ADAB or in situ reconstruction (ISR) for patients with thoracic SGI. However, ISR is commonly performed because of its technical feasibility. ADAB is more commonly used to treat recurrent aortic coarctation, though its successful usage in SGI has also been reported. 5
For our patient, ADAB was chosen over ISR because after thoracotomy the progression of infection in the descending aorta, presence of frank pus and tissue adhesion, occurrence of a SINE, history of multiple thoracic interventions, and diffuse oozing from the surgical field were profound.
B. cepacia complex in patients with SGI and IAA should raise concerns, particularly in the multiple thoracic procedures in emergent thoracic trauma cases. In such scenarios, a comprehensive approach involving SGI debridement and ADAB can be considered addressing the persistently compromised SGI-affected area.
Footnotes
Data Availability
The data in this article are available from the corresponding author upon reasonable request.
Authors’ Contributions
T.H.C. drafted the article. S.W.C., Y.T.C., and T.H.C. contributed to the study’s conception and design. S.Y.C. contributed to medical image extraction and reconstruction. All authors participated in article revision and approved the submitted version.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.