
Abstract
Background:
Anastomotic leaks after esophagectomy cause significant morbidity and mortality. In addition to their early detection and prompt endoscopic or surgical management, providing adequate antimicrobial agents is a fundamental aspect of therapy. In this study, different types of microbiological samples were analyzed to provide insight into the microbial pathogen spectrum of anastomotic leaks after esophagectomy.
Methods:
We retrospectively reviewed patients who developed anastomotic leak after Ivor–Lewis esophagectomy at a German high-volume center between 2016 and 2018. Results of microbiological cultures from surgical samples, chest tube fluid, endoscopic aspirates, and blood cultures were analyzed to determine species and antimicrobial susceptibility.
Results:
Out of 513 consecutive patients undergoing esophagectomy, 74 developed an anastomotic leak. About 88%–100% of positive samples showed growth of gram-positive bacteria, mainly viridians streptococci but also enterococci. Gram-negative bacteria were found in 48%–82% of positive samples, mainly enterobacterales. Yeasts were found in 43%–64%. The prevalance of multidrug-resistant bacteria was low in our patient population. Expected failure of empiric antibiotic treatment was <10% for piperacillin-tazobactam, meropenem, and tigecycline (each combined with an echinocandin) but not for ampicillin-sulbactam, ceftriaxone plus metronidazole, moxifloxacin, or gentamicine plus clindamycin.
Conclusions:
There is a broad microbial pathogen spectrum in anastomotic leaks after esophagectomy. Implications for empiric antimicrobial treatment arise from enterobacterales, enterococci, and yeasts.
Introduction
Esophagectomy is a complex surgical procedure associated with a significant rate of morbidity and mortality. Anastomotic leaks, in particular, remain a major problem with an incidence up to 22%.1–5 Subsequent mediastinal infection and inflammation can lead to both local complications and sepsis. Anastomotic leakage is therefore associated with increased in-hospital and long-term mortality,5,6 as well as impaired quality of life. 7 It has even been hypothesized that immunological compromise because of anastomotic leakage might promote tumor recurrence. 6
In addition to endoscopic or surgical management of an anastomotic leak, providing adequate antimicrobial agents is a fundamental aspect of therapy. Numerous studies have shown that delayed or inadequate antimicrobial therapy compromises the outcome of patients with severe infections.8,9 Early administration of antimicrobial therapy is therefore a key recommendation in international guidelines, e.g., for the management of sepsis or intra-abdominal infection.10–12 The chosen antimicrobial agents should reliably cover those microorganisms that are usually found at the site of infection.
However, there are very limited data on the microbiota of anastomotic leaks after esophagectomy. 13 Both the underlying disease (most often cancer) and the subsequent therapies (e.g., proton pump inhibition, chemo(radio)therapy, and surgery) might induce a change in the microbiota compared with the usual upper gastrointestinal flora in healthy subjects.14–17 We have therefore analyzed microbiological samples from patients with anastomotic leak after esophagectomy from a German high-volume center.
Materials and Methods
We retrospectively reviewed the records of all consecutive patients who had developed an anastomotic leak after Ivor–Lewis esophagectomy at our institution between 2016 and 2018. Because of the retrospective nature of this study, approval was waived by the Ethics Committee of the Faculty of Medicine of the University of Cologne (waiver no. 23-1410-retro).
Surgical and medical management
All patients had undergone transthoracic esophagectomy with 2-field lymphadenectomy and gastric tube reconstruction (Ivor–Lewis procedure). A single dose of cefazolin was administered prior to incision as perioperative antimicrobial prophylaxis.
If an anastomotic leak was suspected, endoscopy and computed tomography were performed immediately to establish or rule out the diagnosis. If an anastomotic leak was identified, conservative (e.g., nasogastric tube), endoscopic (e.g., endoluminal vacuum therapy and stent placement), or surgical treatment was initiated, as deemed clinically appropriate. Antimicrobial therapy with either piperacillin-tazobactam or meropenem in combination with an echinocandin (caspofungin or anidulafungin) was initiated for 7–10 days. Additional measures during sepsis were taken as needed, e.g., hemodynamic support or mechanical ventilation.
Microbiological samples
Microbiological samples were obtained by the clinicians on duty at their discretion. In general, two pairs of blood cultures were to be collected before starting antimicrobial therapy according to the institutional standard operating procedure. In patients requiring surgical intervention, biopsies or swaps of infected tissues were usually obtained during the procedure. Other methods of sampling included chest tube fluid (in case of bilious or turbid appearance) or endoscopically obtained aspirate (in case of larger defects with adjacent cavities).
For this study, we reviewed results of microbiological cultures from the above-mentioned samples as they were presented by the laboratory. The cultured microorganisms were classified into 13 categories according to microbiological criteria, clinical significance, and implications on antimicrobial therapy:
Staphylococcus aureus (including Staphylococcus lugdunensis), coagulase-negative staphylococci (except Staphylococcus lugdunensis), viridans streptococci, beta-hemolytic streptococci, enterococci, other aerobic gram-positive cocci (mainly Abiotrophia spp., Granulicatella spp., Rothia spp.), anaerobic gram-positive bacteria (mainly Actinomyces spp., Lactobacillus spp., Propionibacterium spp.), enterobacterales, non-fermentative gram-negative bacilli (Pseudomonas spp., Stenotrophomonas spp.) other aerobic gram-negative bacteria (mainly Eikenella spp., Haemophilus spp., Neisseria spp.), anaerobic gram-negative bacteria (mainly Prevotella spp., Veilonella spp.), Candida albicans, non-albicans Candida species.
When growth of normal bacterial skin flora (coagulase-negative staphylococci, Propionibacterium acnes) was obtained in only one out of two or more pairs of blood cultures, these were considered false positives and excluded from the analysis.18–20 We further excluded positive blood cultures of one patient, which were associated with a concurrent urinary tract infection (Proteus mirabilis and Pseudomonas aeruginosa).
Results from in vitro susceptibility testing were used to determine expected failure rates of various hypothetical empiric antibiotic therapies. In this context, growth of coagulase-negative staphylococci (except Staphylococcus lugdunensis) was considered irrelevant. We checked susceptibility for seven antibiotic regimens:
ampicillin-sulbactam, piperacillin-tazobactam, ceftriaxone plus metronidazole, meropenem, moxifloxacin, tigecycline, gentamicin plus clindamycin.
Results
In total, 513 patients underwent esophagectomy at our institution between 2016 and 2018. Seventy-four patients (14%) developed an anastomotic leak and were included in this analysis. Baseline characteristics and outcome data are shown in Table 1.
Characteristics of the Study Population
Age is presented as mean ± standard deviation. Onset of anastomotic leak is presented as median [interquartile range].
Positivity rates of microbiological cultures are shown in Table 2. Surgical samples and endoscopic aspirates yielded positive cultures in almost all patients and chest tube fluid in more than two-thirds of the patients. Blood cultures were positive in 21% of the patients.
Positivity Rates of Microbiological Samples
Regarding blood cultures, 14 samples from 9 patients were excluded from the analysis. See “Materials and methods” section for details.
Microorganisms detected are shown in Figure 1 and in the Supplementary Figures. Gram-positive bacteria were predominant and found in 88%–100% of patients who had positive cultures from surgical, endoscopic, or chest fluid samples. Most prevalent were viridans streptococci, primarily Streptococcus anginosus and Streptococcus oralis. Gram-negative bacteria were found in 48%–82%. Most prevalent were enterobacterales, primarily Escherichia coli. Yeasts were found in 43%–64%. In blood cultures, viridans streptococci and enterobacterales equally predominated, whereas there was no case of fungemia.
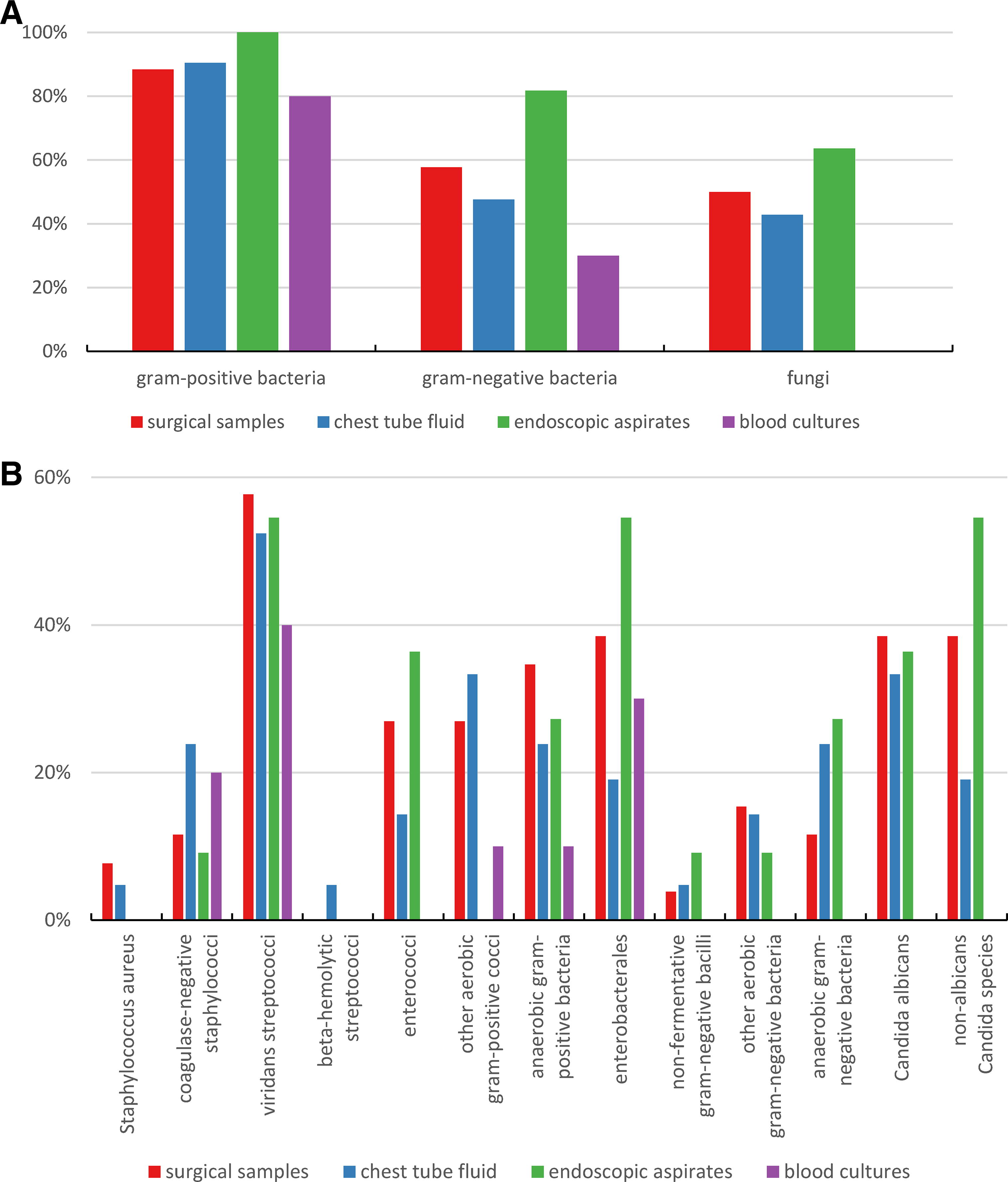
There was a low prevalence of multidrug resistance among cultured bacteria. One patient grew methicillin-resistant staphylococcus aureus, and four patients grew ampC beta-lactamase-producing enterobacterales (Citrobacter freundii, Enterobacter cloacae, and Hafnia alvei). There were no cases of vancomycin-resistant enterococci, extended-spectrum beta-lactamase-producing bacteria, or carbapenemase-producing bacteria.
The expected failure of empiric antibiotic treatment is shown in Figure 2. Rates were <10% with piperacillin-tazobactam, meropenem, and tigecycline. Regarding piperacillin-tazobactam and tigecycline, failure was mainly because of resistant enterobacterales, whereas there was no clear pattern with meropenem. For ceftriaxone/metronidazole and gentamicin/clindamycin, failure was expected in more than 30% of patients, mainly because of the presence of enterococci.

Positive cultures were obtained from three out of six non-surviving patients. These samples yielded bacteria, which were fully susceptible to the empiric regimens used at our institution.
Discussion
To our knowledge, our study is the most comprehensive analysis of microbiota of anastomotic leaks after esophagectomy. Gram-positive bacteria, mainly viridans streptococci, were most abundant in samples from anastomotic leaks. However, enterobacterales, enterococci, and yeasts were also frequently detected. Appropriate antimicrobial therapy must therefore include coverage for this full spectrum of pathogens.
Several studies have analyzed esophageal microbiota from healthy subjects using microbiological culture or genetic sequencing.14,15,21–23 These studies showed a rich flora with the presence of numerous bacterial species, usually with a vast predominance of streptococci. Other commonly found species include anaerobic bacteria such as Prevotella, Veilonella, Fusobacterium, and Lactobacillus spp., the gram-positive cocci Granulicatella and Rothia spp., as well as the gram-negative species Haemophilus and Neisseria spp. Studies in patients with esophageal cancer indicate a less diverse bacterial flora in the upper gastrointestinal tract.14–17 Although our findings are generally in line with these studies, there is a marked difference in the prevalence of enterococci and enterobacterales. Although these species are rarely found in healthy subjects and cancer patients prior to surgery, they grew in abundance in our samples from patients with anastomotic leak after esophagectomy.
To our knowledge, there is only one small study to date addressing the microbiota of anastomotic leaks after esophagectomy. 13 In this study, Erichsen et al. only analyzed endoscopic aspirates from 17 patients. They found enterococci and enterobacterales in a similar percentage (27% and 40%, respectively) as in our patient population.
Regarding the differences in microbiota between patients with adenocarcinoma and squamous cell carcinoma, our samples suggest a shift away from streptococci toward other species in squamous cell carcinoma (Supplementary Fig. S1). Interestingly, the same shift appeared to occur in adenocarcinoma with chemoradiotherapy (Supplementary Fig. S2). Almost all patients with squamous cell carcinoma had undergone chemoradiotherapy prior to surgery. However, because of the small sample size, we refrained from further analysis.
Colonization with Candida spp. is common in esophageal cancer.24,25 Possible mechanisms that may facilitate such colonization include disruption of the mucosa barrier, dysphagia, proton pump inhibitor treatment, and immunosuppression by neoadjuvant therapy. In our study, we found yeasts in more than 40% of positive samples. Other studies in patients undergoing esophagectomy reported an even higher prevalence.13,26
When reviewing microbiological tests, it is imperative to distinguish between mere colonization and true infection. Positive blood culture results (except those contaminated with skin flora) are usually synonymous with infection. However, only a few patients with anastomotic leaks yield positive blood cultures. In our study, 21% of patients had positive blood cultures. This percentage is almost identical to a study of patients with post-operative intra-abdominal infections (19%). 27
Surgical sampling from the site of infection is usually considered a standard procedure and recommended in international guidelines.11–12 In contrast, endoscopic aspirates from the anastomotic leakage, as performed at our center as well as in the study by Erichsen et al., 13 are less common. Determining true infection from these specimens may not always be possible. The same is true for chest tube fluid, which has even further limitations (e.g., false negatives by insufficient connection to the leakage and false positives by biofilm on tube surfaces). In our opinion, despite these limitations, it is important to know the local flora for adequate antimicrobial therapy.
Viridans streptococci were most abundant in all samples investigated in our study, the most common species being Streptococcus anginosus. Although viridans streptococci were once considered harmless commensals, this view has changed in the recent decades. Several virulence factors have been described, which promote tissue adhesion and destruction as well as protection from host response. 28 The high frequency of streptococci within positive blood cultures in our study indicates their clinical significance in anastomotic leakage after esophagectomy. Streptococci are highly susceptible to most antimicrobial regimens, particularly beta-lactam antibiotics. However, we observed clindamycin resistance in 20% of patients, which should be considered when selecting an antibiotic regimen.
Enterococci are not usually expected flora in the healthy esophagus.14,15,21–23 Nevertheless, they were present in 14%–36% of our patients, most frequently in endoscopic aspirates, usually Enterococcus faecalis. Like streptococci, enterococci were previously considered less significant. However, they also possess several virulence factors. 29 It has even been suggested that the presence of enterococci per se promotes the emergence of anastomotic leakage through collagen degradation. 30 A recent meta-analysis of studies on community-acquired intra-abdominal infection showed that empiric anti-enterococcal therapy does not improve outcome. 31 However, the authors argued that the result was because of the low percentage of enterococcal infections in this population and should not be applied to hospital-acquired infections or septic patients. Robust clinical trials in these populations are lacking. Guidelines on intra-abdominal infections do recommend empiric anti-enterococcal therapy in post-operative infections.11–12 The high prevalence of enterococci in our study should therefore discourage the use of regimens such as ceftriaxone/metronidazole or gentamicin/clindamycin in patients with anastomotic leak after Ivor–Lewis esophagectomy.
Yeasts were found in 43%–64% of our patients. Like bacteria, Candida spp. possess multiple virulence factors enabling invasive infection. 32 Retrospective data suggest that growth of Candida spp. in mediastinal or peritoneal samples is associated with increased mortality.33,34 There is an ongoing debate as to whether preemptive antifungal treatment should be started before microbiological evidence of infection is present. 35 However, guidelines on intra-abdominal infection do recommend antifungal treatment when Candida spp. is recovered from microbiological samples, but also in cases when Candida infection is suspected.11–12 Invasive candidiasis is most effectively treated with echinocandins. 36
We investigated the expected failure rates of different empiric antimicrobial regimens. It has been suggested by guidelines that expected failure rates of any empiric therapy should be <10%. 12 In our study, piperacillin-tazobactam, meropenem, and tigecycline fulfill this criterion and are therefore suitable for use in patients with anastomotic leak after esophagectomy. Considering the high prevalence of yeasts, we suggest supplementing the antibiotic therapy with an echinocandin.
We did not analyze whether the results of microbiological samples led to a change in therapy. However, we exclusively used piperacillin-tazobactam or meropenem for empiric treatment, each in combination with an echinocandin. Therefore, necessary changes in antimicrobial therapy should have been minimal. In contrast, in the study by Erichsen et al., different empiric regimens were used. 13 Here, microbiological testing of endoscopic aspirates led to a modification of therapy in all patients, most often because yeasts had not been considered in the initial therapy, followed by enterococci.
The diverse microbiota of anastomotic leaks also impacts antibiotic de-escalation strategies. We suggest that de-escalation should only be considered based on microbiological samples from the immediate leak site, if at all. Blood cultures, in particular, do not reflect the complexity of this polymicrobial infection.
Extrapolation of our findings to different patient populations must be done with caution. In particular, susceptibility rates of enterobacterales vary significantly between different geographic locations. In our study, despite the frequent growth of enterobacterales, the expected failure because of resistant species of enterobacterales was low. This is consistent with the study by Erichsen et al., which investigated patients from another center in Germany. 13 Susceptibility rates among Europe and the United States can be found in surveillance atlases by the European Centre for Disease Prevention and Control and the Centers for Disease Control and Prevention, respectively.37,38 Susceptibility to piperacillin-tazobactam is not included per se. However, considering a number of mutual resistance mechanisms such as extended-spectrum beta-lactamases, it might be extrapolated from susceptibility to third-generation cephalosporins. Regarding Escherichia coli, which was most frequently found in our patients, resistance rates to third-generation cephalosporins in Europe vary between 5% and 40% (Germany: 10%), and in the United States, it varies between 3% and 40%. Resistance rates to carbapenems in Europe vary between 0% and 2% (Germany: 0–0.1%), and in the United States, it varies between 0% and 4%. Resistance in Klebsiella pneumoniae, which was found in two of our patients, can be even higher.
Our study has several limitations. First, we did not obtain a complete set of all four sample types from each patient. Furthermore, we have already discussed the incomplete association between microbiological growth and true infection as well as the limited generalizability to other geographic locations. Finally, the retrospective nature of our study does not allow us to discern whether any antimicrobial regimen will affect patient outcome.
Conclusions
This study demonstrated growth of a broad spectrum of both gram-positive and gram-negative bacteria as well as yeasts in samples from anastomotic leaks after Ivor–Lewis esophagectomy. Viridans streptococci were most abundant. However, implications on empiric antimicrobial therapy arise from enterobacterales, enterococci, and yeasts. In our patient cohort with a low prevalence of multidrug-resistant bacteria, piperacillin-tazobactam, meropenem, or tigecycline, each combined with an echinocandin, proved to be the most suitable treatment options. Local susceptibility rates particularly of enterobacterales must be considered.
Footnotes
Acknowledgment
The authors thank Jose Rafael Valladares Arias, MD, for proofreading the article.
Authors’ Contributions
All named authors took active part in data collection, article writing, and reviewing.
Author Disclosure Statement
The authors have no competing interests to declare that are relevant to the content of this article.
Funding Information
No funding was received for conducting this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.