
Abstract

To the Editor:
Salmonella enterica is a gram-negative rod bacterium that typically produces self-limited gastrointestinal infection. Furthermore, it may occasionally lead to bacteremia. The primary risk factor for Salmonella enterica bacteremia is immunocompromised diseases such as human immunodeficiency virus infection, 1 which is also the major cause of the spread of Salmonella enterica to different sites. 2 Here, we report a case of Salmonella enterica-related chest wall abscess in patient with AIDS.
A 51-year-old male presented to our department with left anterior chest wall pain. He received a diagnosis of AIDS 2 months ago. He possessed no prior occurrences of bug bites or localized trauma. On physical examination, localized swelling near the sternum on the affected side, with normal local skin temperature, no fluctuation, and tenderness upon palpation. Laboratory results indicated that white blood cells and neutrophil count were normal, and C-reactive protein was 96.30 mg/L (reference range: 0–0.50 mg/L), and procalcitonin was 0.36 ug/L (0–0.05 ug/L). Computed tomography revealed a mass soft tissue swelling on the left chest wall, characterized by heterogeneous soft tissue density (Fig. 1A). Ultrasound showed a low echo with a range of about 7.80 cm × 3.50 cm, and a weak echo flow could be observed inside (Fig. 1B). Tuberculosis and fungal examination results were negative. He was treated empirically by using amoxicillin clavulanate potassium. Nevertheless, the local infection gradually worsened, and ultrasound indicated the formation of an abscess (Fig. 1C).
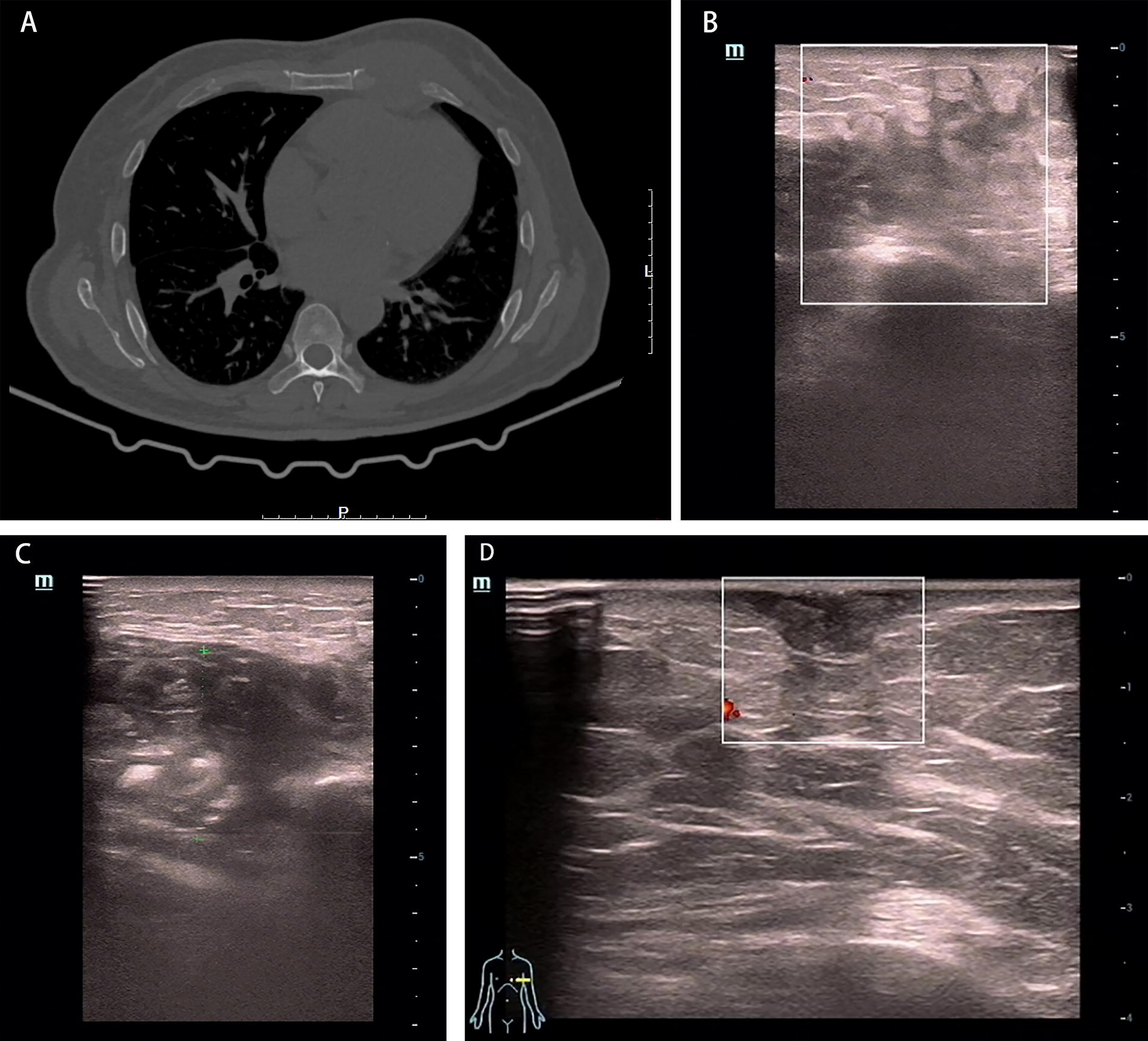
Subsequently, an operation puncturing an abscess was performed. The punctured object consisted of tissue and pus. The histopathology findings indicated granulomatous inflammation, and the metagenomics next-generation sequencing (mNGS) of tissue detected Salmonella enterica; the pus culture was negative. Antibiotic treatment was then switched to combine ceftriaxone and levofloxacin, and the abscess was persistently drainage. Following three weeks of treatment, the abscess was gradually diminished. After discharge, oral levofloxacin and cefixime were used for treatment. Follow-up two weeks later, procalcitonin and C-reactive protein were normal, and ultrasound revealed that the abscess was completely absorbed (Fig. 1D).
The predominant pathogenic microorganisms associated with skin and soft tissue abscesses are Staphylococcus aureus and Streptococcus from the skin surface, 3 whereas Salmonella enterica is relatively rare. The empirical management of typical skin abscesses is ineffective against Salmonella enterica. The patient recalled that he had experienced once severe diarrhea in three months ago and recovered after therapy, it was hypothesized that the individual may have become a carrier from a prior infection, subsequently allowing the bacteria to disseminate through the blood stream to the skin, where it formed an abscess. Regrettably, the patient did not receive pathogen culture of blood upon initial admission. Thus, in clinical practice, particular attention should be given to determining whether a patient has a Salmonella enterica infection when they have an abscess and prodromal gastrointestinal symptoms, particularly if they have a weakened immune system. There were no positive results of the patient’s pus culture and the histopathologic examination, but we conducted an mNGS detection that successfully identified pathogenic bacteria, underscoring the substantial utility of mNGS technology in diagnosing clinically challenging infections.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.