
Abstract

To the Editor:
Although colorectal cancer (CRC) is a common tumor of the elderly, its occurrence in children is extremely rare, with an annual incidence of one case per million children. 1 While some pre-disposing diseases, such as Peutz–Jeghers syndrome and familial adenomatous polyposis, are found in 10% of children, the majority of pediatric CRC are sporadic. 2 At the time of presentation, pediatric patients with CRC are likely to have late-stage disease with a high rate of adverse pathology, resulting in a poor outcome compared with to adults. 3 Surgery plays a key role in the management of children with CRC. However, these patients are at increased risk of post-operative sepsis and sepsis-related mortality.4,5
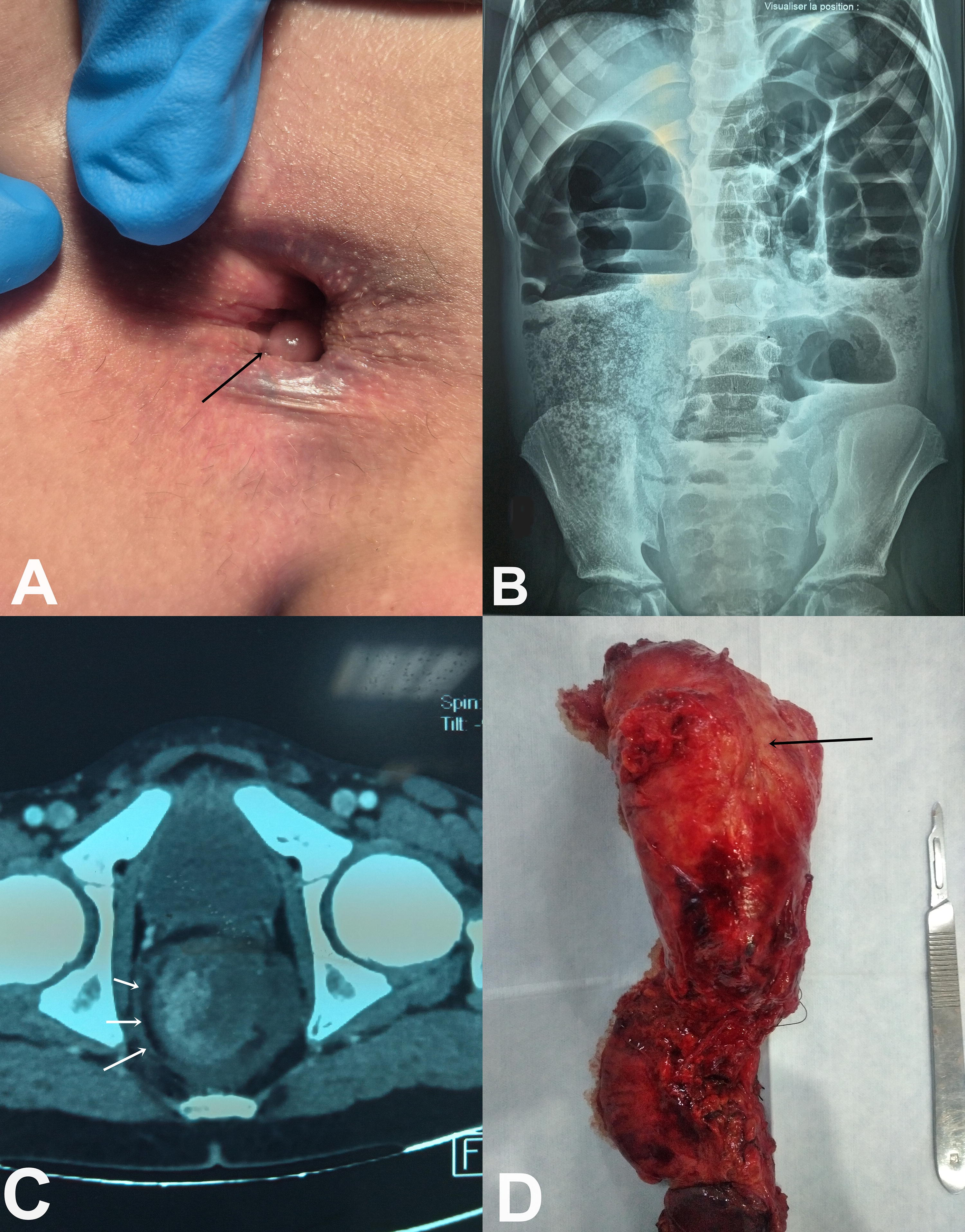
An 11-year-old boy presented to the hospital after 2 days of diarrhea, abdominal pain, and vomiting. The child was not living with his parents, who were not sure whether he had a recent history of trauma or abuse. There was no family history of genetic syndromes pre-disposing to malignant diseases. Examination of the anal area revealed several anorectal polyps (Fig. 1A). There was no fever. Laboratory tests revealed leukocytosis of 13.2 × 109/L, hemoglobin of 14 g/dL, and C-reactive protein of 2 mg/L. Plain abdominal X-ray showed numerous air-fluid levels (Fig. 1B). Computed tomography revealed irregular wall thickening with contrast enhancement and perirectal extraluminal gas suggestive of rectal perforation (Fig. 1C). An emergency laparotomy was performed with closure of an upper rectal perforation, creation of a sigmoid colostomy and excision of an anal polyp. The post-operative course was straightforward, and the child was discharged on post-operative day 7. Pathological findings showed an inflammatory pseudopolyp. One month later, the patient returned to the emergency department with bleeding. This bleeding was both per rectal and through the distal colostomy and was continuous. Hemoglobin level was 8.2 g/dL. Colonoscopy revealed a mass in the lower and middle rectum with active bleeding. After transfusion, the patient underwent emergency laparotomy with resection of the colon downstream of the stoma and removal of the rectal mass (Fig. 1D). Twelve hours after surgery, the child developed multiple organ failure in relation to post-operative sepsis and died. Histological investigation identified a mucinous, low-differentiated adenocarcinoma with tumoral invasion of the visceral peritoneum.
CRC is a rare malignant disease in children, and even rarer is its association with gastrointestinal perforation resulting in peritonitis, abdominal abscess, and sepsis. Despite progress in understanding infection-related complications in children with cancer, septic shock remains a leading cause of mortality, especially in resource-limited settings.4,5
Although rectal malignant diseases are extremely rare in children, a non-traumatic rectal perforation in a child should first point to rectal cancer.
Footnotes
Authors’ Contributions
M.Z. was responsible for conceptualization, project administration, writing (original draft), and writing (review). M.B., R.Z., W.B., and N.B.K. contributed to data curation and methodology. M.B.D. and R.M. performed supervision and validation. M.Z. is the guarantor.
Consent Statement
Informed consent was obtained from the patient’s guardian.
Author Disclosure Statement
The authors have no financial or personal relationships with other people or organizations that could potentially and inappropriately influence our work and conclusions.
Funding Information
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.