
Abstract
Abstract
Artificial dermis (AD) has been used to regenerate dermis-like tissues in the treatment of full-thickness skin defects, but it takes 2 or 3 weeks to complete dermal regeneration. Our previous study demonstrated that injection of basic fibroblast growth factor (bFGF)–impregnated gelatin microspheres (MS) into the AD accelerates the regeneration of dermis-like tissue. However, injection of gelatin MS before clinical use is complicated and time consuming. This study investigated a new scaffold, in which collagen and gelatin are integrated, and which is capable of sustained bFGF release. We produced collagen/gelatin sponges with a gelatin concentration of 0wt%, 10wt%, 30wt%, and 50wt%. The mean pore size in each sponge decreased with the gelatin concentration. In an in vitro study, proliferation of fibroblasts in each sponge was not significantly different over 7 days of culture. As for in vivo sustained release of bFGF, a radioisotope study demonstrated that retention of bFGF in gelatin 10wt% and 30wt% sponges was significantly larger than that in gelatin 0wt% sponge. The collagen/gelatin sponges were grafted on full-thickness skin defects created on a rabbit ear, and we evaluated regeneration of dermis-like tissue by measuring the amount of hemoglobin and size of dermis-like tissue on histological sections. Seven days after implantation, the amount of hemoglobin in dermis-like tissue in gelatin 10wt% sponge was significantly larger than those in control and gelatin 50wt% sponge. Twenty-eight days after implantation, the area of dermis-like tissue in gelatin 10wt% sponge was significantly larger than those in the other specimens. We conclude that the collagen sponge integrated with 10wt% gelatin has the most potential for sustained release of bFGF and that the combination of collagen/gelatin 10wt% sponge and bFGF is a promising therapeutic modality for the treatment of full-thickness skin defects.
Introduction
AD is composed of an outer silicone membrane and an inner collagen sponge, which functions as a scaffold. When it is grafted on a full-thickness skin defect, fibroblasts and capillaries infiltrate the pores of the inner collagen sponge from the lower layer. Then these fibroblasts and capillaries further spread throughout the sponge. The proliferating fibroblasts synthesize new collagen fibers, and at the same time the original collagen sponge is absorbed. The collagen sponge spontaneously turns into regenerated connective tissue, the so-called dermis-like tissue in 2 or 3 weeks. Then, the silicone membrane is peeled off and a secondary split-thickness graft is grafted onto the dermis-like tissue. The skin graft takes easily, and post-operative graft contraction is minimal. During the period till the vascular network is formed, however, the collagen sponge carries a high risk of infection. 8 So we would like to design the AD that can be applied to a wound bed with poor blood supply. Some authors have reported that basic fibroblast growth factor (bFGF) accelerates wound healing.9–16 We previously reported the sustained release of biologically active bFGF from gelatin microspheres (MS).17–20 In addition, we demonstrated acceleration of tissue regeneration through incorporation of bFGF-impregnated gelatin MS into the AD. 21 However, injection of MS into AD just before clinical use is complicated and time consuming.
Therefore, we attempted to produce a new scaffold in which collagen and gelatin are integrated by adding gelatin during the manufacturing of the collagen sponge. Dehydrothermally cross-linked composites of fibrillar and denatured collagen were also developed and used for covering skin defects.22,23 However, these were not intended to facilitate the addition of bFGF. Then we manufactured collagen/gelatin sponges containing various percentage of gelatin (collagen/gelatin sponge) and investigated in vitro cell proliferation, in vivo release of bFGF, and in vivo tissue generation.
Materials and Methods
Animals and operations
Animals were maintained in the Institute of Laboratory Animals, Graduate School of Medicine, Kyoto University. The number of animals used in this study was kept to a minimum, and all possible efforts were made to reduce suffering in compliance with protocols established by the Animal Research Committee of Kyoto University.
Experimental materials
An aqueous solution of human recombinant bFGF with an isoelectric point (IEP) of 9.6 (10 mg/mL) was supplied by Kaken Pharmaceutical, Tokyo, Japan. We used gelatin isolated from pig dermis with an IEP of 5.0 and a molecular weight of 99,000 (Nippi, Osaka, Japan) and atelocollagen isolated from pig tendon with an IEP of 8.5 and a molecular weight of 300,000 (Nitta Gelatin, Osaka, Japan). Dulbecco's modified Eagle's medium (DMEM; Sigma, Tokyo, Japan) and fetal bovine serum (FBS; Gibco, Osaka, Japan) were used for fibroblast culture. Other chemicals were purchased from Wako Pure Chemical Industries (Kyoto, Japan) and used without further purification.
Preparation of collagen/gelatin sponge
Table 1 summarizes the method of producing collagen/gelatin sponges as scaffold. Collagen/gelatin sponges at gelatin concentrations of 0wt%, 10wt%, 30wt%, and 50wt% of the total solute were prepared by mixing 3wt% gelatin solution into 0.3wt% collagen solution. Each sponge was examined by scanning electron microscopy (SEM, S-4800 Type I; Hitachi, Tokyo, Japan), and the mean pore size was measured by calculating the dots of each pore (n = 6) from the image. Further, we produced other collagen/gelatin sponges using rhodamine 6G isothiocyanate (RITC) as fluorescent signal indications for gelatin. RITC-labeled gelatin was prepared by the same method as used for fluorescence-labeled dextran and human growth hormone. 24 Briefly, 1.5 mg of RITC dissolved in 0.5 mL of dimethyl sulfoxide was slowly added in aliquot volumes of 2 μL to 4 mg of IEP gelatin dissolved in 2 mL of 0.1 M Na2CO3. After an incubation period of 8 h at 4°C, the coupling reaction was stopped by the addition of 50 mM NH4Cl and agitation for 2 h at 4°C. Excess RITC was separated on a Sephadex® G15 column. The RITC–gelatin conjugate was frozen in liquid nitrogen, lyophilized as described above, and stored at 4°C in the dark until further use. We produced collagen/gelatin sponges in which the concentration of fluorescence-labeled gelatin was 10wt%, 30wt%, and 50wt%. And we observed the distribution of gelatin in collagen/gelatin sponge using a fluorescence microscope (Eclipse 80i; Nikon, Tokyo, Japan).
In vitro cell proliferation in collagen/gelatin sponge
In a 96-well plate, 1 × 105 fibroblasts (Clonetics, Walkersville, MD) were seeded onto each well, and DMEM with 10% FBS was added. Fibroblasts were then incubated in CO2 incubator and became attached to the bottom of the plate. After incubation for 24 h, media were exchanged and sponges that had been soaked in media for 24 h were placed on the fibroblasts in each well. Samples were incubated in a CO2 incubator. After culturing for 1, 3, 5, and 7 days, the number of fibroblasts in each sponge was assessed by measuring the amount of DNA by Hoechst 33258. 25 Briefly, each sponge was rinsed with phosphate-buffered solution (PBS) three times and minced by scissors. The fragments of sponge were digested with collagenase (2 mg/mL) at 37°C for 1 h with occasional mixing. After confirming the absence of fragments, fibroblasts were collected by centrifuging at 1000 rpm for 5 min at room temperature. Then fibroblasts were washed with PBS twice and stored at −30°C until assay. After thawing, the samples were added to 1 mL of mixed solution containing sodium dodecyl sulfate (SDS, 0.2 mg/mL) and 30 mM saline-sodium citrate (SSC) and incubated for 1 h at 37°C with occasional mixing. Sample solution (100 μL) was mixed with a dye solution (100 μL) containing 30 mM SSC and Hoechst 33258 dye (1 μg/mL). The fluorescence intensity of the mixed solution was determined with a fluorescence spectrophotometer (F-2000; Hitachi) at excitation and emission wavelengths of 355 and 460 nm. The cell number was calculated from the calibration curve between cell number and fluorescence intensity prepared using known numbers of fibroblasts.
In vivo bFGF release from collagen/gelatin sponge
In vivo release of bFGF was tested using 125I-labeled bFGF. 26 Basic FGF was radioiodinated with chloramine-T according to the method described by Greenwood et al. 27 Briefly, 5 μL of Na125I was added to 200 μL of 0.5 mg/mL bFGF solution in 0.5 M potassium PBS (pH 7.5) containing 0.5 M sodium chloride. Then 0.2 mg/mL of chloramine-T in 0.5 M potassium PBS (pH 7.5) containing 0.5 M sodium chloride (100 μL) was added to the solution mixture. After agitation at room temperature for 2 min, 100 μL solution containing 0.4 mg of sodium metabisulfate was added to the reaction solution to stop the radioiodination. The reaction mixture was passed through an anionic-exchange column to remove the uncoupled, free 125I molecules from the 125I-labeled bFGF.
The collagen/gelatin sponge (15 mm in diameter) was impregnated with the 125I-labeled bFGF solution and left overnight at 4°C.
Eight-week-old female ddY mice (Shimizu Laboratory Animal Supply, Kyoto, Japan) were anesthetized by intraperitoneal injection of Pentobarbital (2.25 mg/45 μL/mouse). After shaving, a full-thickness skin defect (15 mm in diameter) was made on the back of each mouse. Each sponge was implanted onto the skin defect and sutured to the wound edge with a 5-0 nylon monofilament. At 3, 7, and 10 days after implantation, mice were sacrificed (5 mice/sponge/day), and the remaining radioactivity in each sponge was measured with a gamma ray counter (AUTO WELL GAMMA SYSTEM; Aloka, Tokyo, Japan).
Implantation of collagen/gelatin sponge
Before implantation, collagen/gelatin sponges (8 mm in diameter) were impregnated with the bFGF solution (20 μg/cm2) and left overnight at 4°C. Gelatin 0wt% sponge with normal saline solution was used as a control in this study.
Ten-week-old male rabbits (Shimizu Laboratory Animal Supply) were anesthetized by intramuscular injection of Medetomidine (100 μL/kg), Midazolam (500 μL/kg), and Butophanol (100 μL/kg). Three full-thickness skin defects (8 mm in diameter) were made on the rabbit ear, at 2 cm intervals from the base of the ear. Each sponge was implanted onto the skin defect (Fig. 1) and sutured to the wound edge with a 5-0 nylon monofilament. Three sponges we grafted on each rabbit ear include the same gelatin concentration. Seven days after implantation, all sutures were removed and dermis-like tissue was covered with another silicone sealant that was sutured outside of the dermis-like tissue using a 5-0 nylon monofilament in order to prevent suture notch.
Skin defects in the rabbit ear. Color images available online at www.liebertonline.com/ten.
Assessment of dermis-like tissue
At 3, 7, 10, 14, and 28 days after implantation, the rabbits were sacrificed. The implanted sponges were harvested using a dermal biopsy punch (Kai Medical, Gifu, Japan) 8 mm in diameter. The specimens at 3, 7, 10, and 14 days after implantation were minced with scissors and stored at −30°C. The amount of hemoglobin was measured using a Hemoglobin B-test Wako. Briefly, after thawing, minced tissues were treated in 1 mL hemolytic buffer and mixed at 4°C for 24 h to hemolyze the tissue. Hemolytic buffer was produced by mixing 1.21 g of tris-hydrochloride, 0.744 g of ethylenediaminetetraacetate (EDTA), and 0.1 g of 0.1wt% Triton® X-100; a volume of 100 mL was achieved by adding double-distilled water, and then 1 N hydrochloric acid was added in order to adjust the pH to 7.8. After confirming that the specimens had whitened, 500 μL of supernatant was taken and centrifuged at 15,000 rpm for 15 min at 4°C. Supernatant after centrifuging (100 μL) was mixed with 100 μL of coloration liquid. The fluorescence intensity of the mixed solution was measured with F-2000 at excitation and emission wavelengths of 546 and 660 nm.
The specimens obtained 28 and 90 days after implantation were fixed in 10% neutral-buffered formalin solution, embedded in paraffin wax, sectioned, and stained with hematoxylin and eosin. The histological area of regenerated dermis-like tissue in each section was measured using Image J 1.36b (Wayne Rasband, National Institutes of Health, Bethesda, Maryland).
Statistical analysis
All data were analyzed by Fisher's test and expressed as a mean + standard deviation (SD). A value of p < 0.05 was accepted as significant.
Results
Mean pore size in each sponge
An SEM image of each sponge is shown in Figure 2. Figure 3 shows the mean pore size in each sponge. The mean pore sizes in gelatin 0wt%, 10wt%, 30wt%, and 50wt% were 102.67, 76.67, 66.67, and 58.00 μm, respectively. Significant differences were detected between gelatin 0wt% and each of the other specimens and between gelatin 10wt% and gelatin 50wt%.
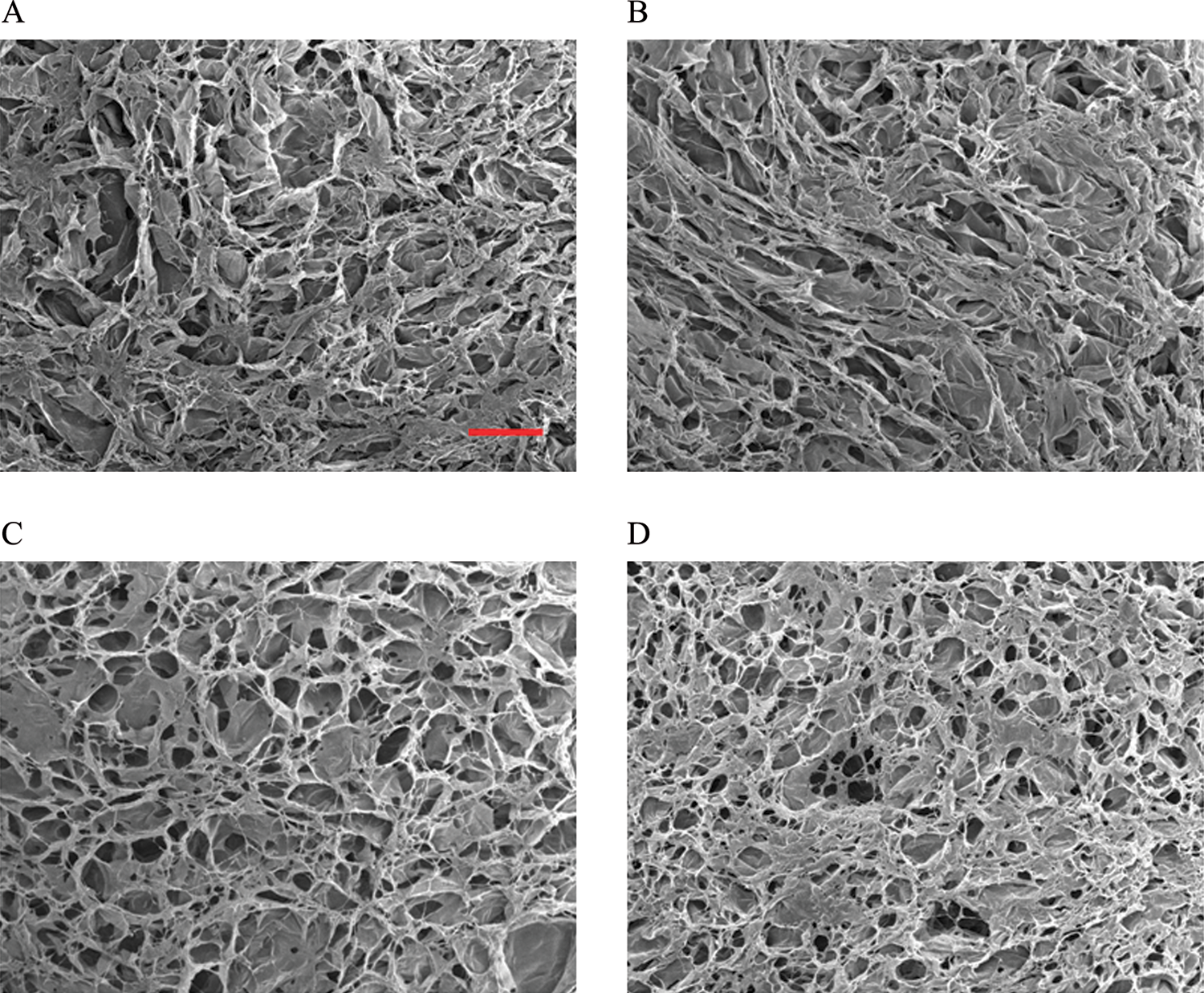
SEM view of each sponge. Gelatin 0wt% (
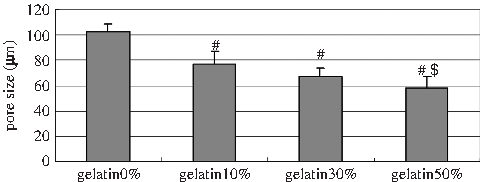
Comparison of mean pore size in each sponge. Data are presented as mean + SE (n = 6), and statistical analysis was performed by Fisher's test. #p < 0.01 compared with gelatin 0wt%; #$p < 0.01 compared with gelatin 10wt%.
Distribution of gelatin in collagen/gelatin sponge
RITC-labeled gelatin was distributed homogeneously; in proportion to gelatin concentration, the luminance of the collagen/gelatin sponge increased. We did not detect RITC in the image of gelatin 0wt% sponge (Fig. 4).

Fluorescent view of each image. Gelatin 0wt% (
Cell proliferation in collagen/gelatin sponge
Figure 5 shows the number of fibroblasts in collagen/gelatin sponges. The number of fibroblasts in each sponge increased similarly over time.

Time course of the proliferation of fibroblasts in each sponge by DNA assay. Number of fibroblasts in the collagen/gelatin sponge (gelatin 0wt% [•], 10wt% [▪], 30wt% [▴], and 50wt% [×]). Data are presented as mean + SE (n = 3), and statistical analysis was performed by Fisher's test. There was no significant difference.
Basic FGF release from collagen/gelatin sponge
Figure 6 shows the remaining radioactivity of bFGF in the sponge. The remaining percentages of bFGF in gelatin 10wt% and 30wt% sponges were significantly higher than those in gelatin 0wt% and 50wt% sponges throughout the time period studied. In gelatin 50wt% sponge, the remaining percentages were higher than those in gelatin 0wt% at 3 and 7 days after implantation.

Time course of bFGF release from collagen/gelatin sponge. Residual bFGF in gelatin 0wt% (•), 10wt% (▪), 30wt% (▴), and 50wt% (×). Data are presented as mean + SE (n = 3–6), and statistical analysis was performed by Fisher's test. #p < 0.05 compared with gelatin 0wt%; #$p < 0.05 compared with gelatin 50wt%.
Hemoglobin assay
Seven days after implantation, the amount of hemoglobin in dermis-like tissue using gelatin 10wt% sponge was significantly larger than that in controls or using gelatin 50wt% sponge (Fig. 7). There were no significant differences at other time points.
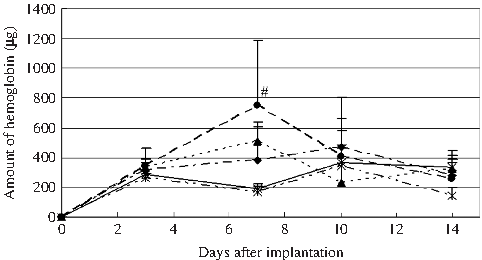
Time course of the amount of hemoglobin in dermis-like tissues regenerated by gelatin 0wt% (•), 10wt% (▪), 30wt% (▴), and 50wt% (×) and control (*). Data are presented as mean + SE (n = 3), and statistical analysis was done by Fisher's test. #p < 0.05 compared with control and gelatin 50wt%.
Area of dermis-like tissue
Figure 8 shows the image of hematoxylin and eosin stain 28 days after implantation. The area of the histological section of dermis-like tissue obtained using gelatin 10wt% sponge was significantly larger than those using sponges with other gelatin weights (Fig. 9). As for the area of dermis-like tissue 90 days after implantation, control is significantly smaller than each of the other specimens (Fig. 10).
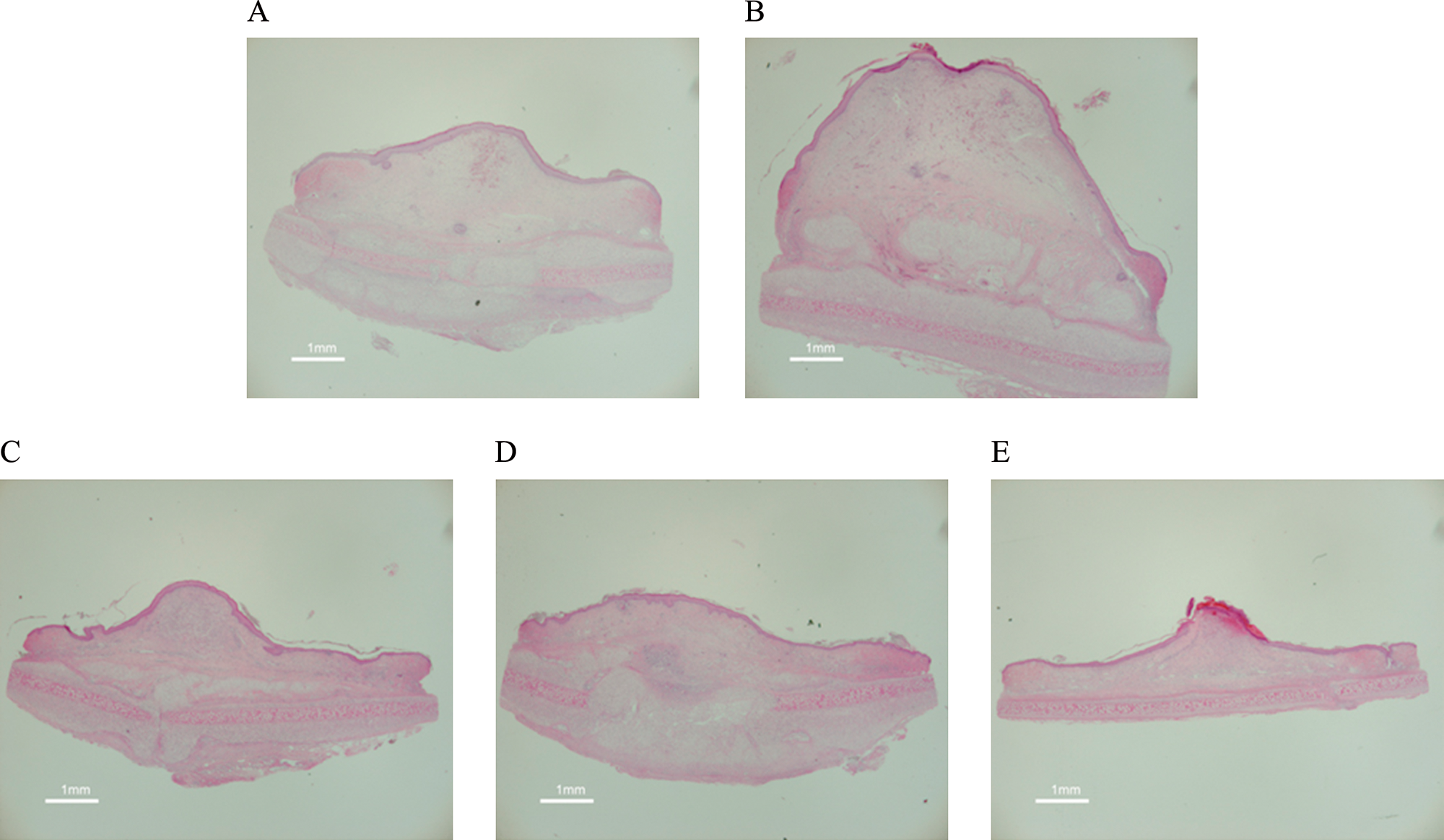
Histological sections of collagen/gelatin sponge 28 days after implantation. Gelatin 0wt% (
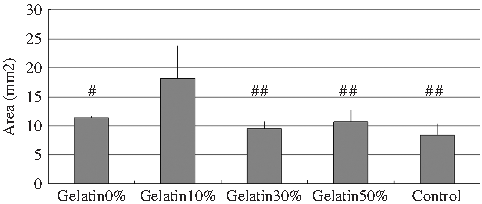
Comparison of the size of each section 28 days after implantation. Data are presented as mean + SE (n = 3), and statistical analysis was performed by Fisher's test. #p < 0.05 and ##p < 0.01 compared with gelatin 10wt%.
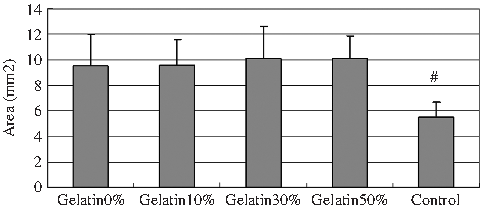
Comparison of the size of each section 90 days after implantation. Data are presented as mean + SE (n = 3), and statistical analysis was performed by Fisher's test. #p < 0.05 compared with others.
Discussion
In 1974, bFGF in bovine pituitary was identified by Gospodarowicz as having potent mitogenic activity on fibroblasts. 28 Basic FGF has already been described as a growth factor involved in various biological activities29–38 and is one of the most potent angiogenic factors.39–41 In 1986, Abraham reported the possibility of using recombinant bFGF, 42 and in Japan a bFGF spray has been commercially available since 2001 and has been widely used for an effective treatment for refractory skin ulcers, such as leg ulcers, as well as for deep wounds with exposed bone.43,44 Further, the combination of bFGF and conventional collagen sponge has been reported as a treatment of refractory skin ulcers, such as diabetic foot ulcer or burn ulcer.45,46 Ito et al. reported that AD was grafted on diabetic foot wound and then bFGF was applied topically twice a week for more than 6 weeks to regenerate dermis-like tissue. 45 Muneuchi et al. reported that AD was grafted on burn ulcer, and then bFGF was injected into the collagen layer of AD once daily for 2 weeks. 46 In these reports, bFGF was applied multiple times during the course of one treatment. As its half-time is very short in vivo, bFGF in free form cannot remain bioactive over a prolonged period, but sustained release systems have been developed to prolong the bioactivity of bFGF. Polymer matrices such as ethylene-vinyl acetate copolymer,47,48 alginate,49–51 collagen, 52 and gelatin17–21 have been reported as carriers of bFGF.
Kawai et al. reported sustained release of bFGF using gelatin MS accelerated tissue regeneration in conventional collagen sponge. 21 However, injection of gelatin MS before clinical application is very complicated and time consuming. Therefore, we devised a method of applying bFGF simply and easily.
In this study, we used gelatin as a carrier of bFGF and evaluated whether incorporation of bFGF into collagen/gelatin sponge affected the regeneration of dermis-like tissues. Preliminarily, Suzuki et al. 53 reported that the collagen sponge was useful as a scaffold, but the sponge of 100% gelatin was not, because fibroblasts did not infiltrate inside the gelatin sponges. Therefore, we produced sponges that integrated varying proportions of collagen and gelatin in this study.
On SEM image, there was a significant difference in mean pore size between collagen sponge and collagen/gelatin sponge and between gelatin 10wt% and gelatin 50wt%. The mean pore size of collagen/gelatin sponges was smaller than that of collagen sponge in proportion to gelatin concentration, but maintained the size measuring more than approximately 60 μm. The difference in sizes might be ascribed to the small molecular weight of gelatin. Gelatin was produced by dissolving collagen. As the gelatin concentration was increased, the spaces in a collagen molecule were gradually filled in by gelatin. Dawlee et al. reported that there is no significant difference in the cell infiltration into the sponge with pore sizes ranging 50–200 μm. 54 From this perspective, the pore size of our collagen/gelatin sponge is accommodative.
Indeed, on in vitro DNA assay, the number of fibroblasts that proliferated into sponges did not significantly differ among collagen sponge and the three kinds of collagen/gelatin sponges. This indicates that the differences in pore sizes among these sponges with pore larger than approximately 60 μm did not influence cell infiltration.
In vivo radioisotope study, the collagen/gelatin sponge was impregnated with the 125I-labeled bFGF solution. Tabata et al. reported that the hydrogel of gelatin with an IEP of 5.0 could immobilize about 70% of bFGF added initially. 55 Further, the bFGF remaining in vivo was closely correlated with the residual gelatin by radiotracing experiments. 56 As the same gelatin hydrogel was used in this study, it is supposed that the gelatin integrated into the sponge can also immobilize about 70% of bFGF, and the remaining radioactivity scientifically demonstrates the amount of residual bFGF in the scaffold.
Gelatin 10wt% and 30wt% sponges retained bFGF throughout the time period studied. These findings indicate that gelatin 10wt% and 30wt% sponges function as scaffolds that can provide the sustained release of bFGF.
To evaluate dermis-like tissue, we grafted sponges that incorporated bFGF on the ears of a rabbit. As wounds on rabbit ears do not contract during the healing process, 57 we could eliminate that bias. As the same kind of sponge was implanted on each ear, we could offset the difference in the location. The results of hemoglobin assay indicate that combined use of gelatin 10wt% sponge and bFGF accelerated angiogenesis. Further, the size of dermis-like tissue obtained using gelatin 10wt% sponge was significantly larger than those obtained using sponges with other gelatin weights 28 days after implantation. We regard the so-called dermis-like tissue as highly vascularized granulation tissue. Figure 11 shows gelatin 10wt% sponge produces much more new capillaries than control. These findings indicate that bFGF-impregnated gelatin 10wt% sponge induces tissue regeneration. The amount of hemoglobin in gelatin 10wt% sponge gradually increased until 7 days after implantation. Increased blood supply during the early stage of the repair process, especially within the initial 7 days, promotes the early formation of granulation tissue. 58 Kawai et al. reported that accelerated fibroblast proliferation and capillary formation reduced infection in AD. 59 Since the sponge matrix often carries a high risk of infection, it is important to induce vascularization as soon as possible to diminish the risk.
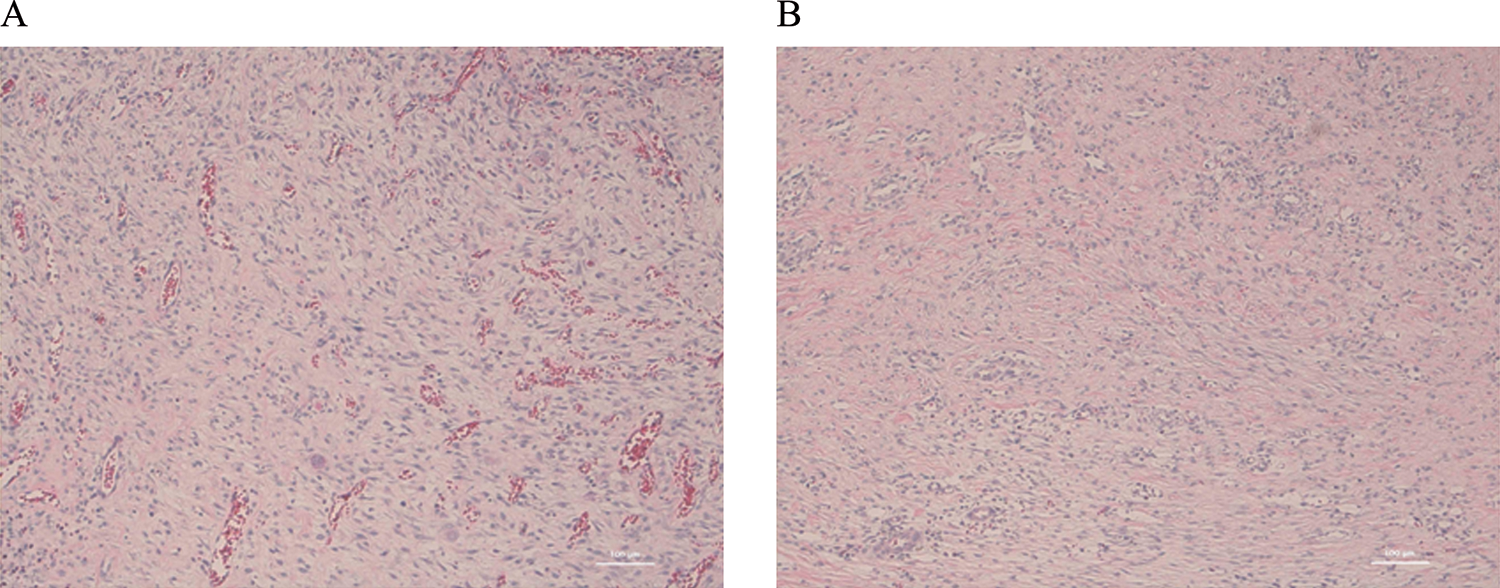
Histological sections of collagen/gelatin sponge 28 days after implantation. Gelatin 10wt% (
In the long-term results, dermis-like tissue in using bFGF was larger than control. As bFGF has efficiency even on single application, 21 we think that the obtained results show it.
In summary, the collagen/gelatin sponge with 10wt% gelatin shows the effect of bFGF in early stage and keeps it in the long term. This new AD seems very attractive and promising, allowing simple and immediate applications without injuring other sites on the patient. It might be possible to use other growth factors such as platelet-derived growth factor instead of bFGF. Further experiments would be needed to clarify that issue.
Conclusions
The collagen/gelatin sponge with 10wt% gelatin has the potential for sustained release of bFGF and acceleration of tissue regeneration with combined use of bFGF. The collagen/gelatin sponge is very promising for the next generation of AD.