
Abstract
Abstract
Macrophage phenotype can be characterized as proinflammatory (M1) or immunomodulatory and tissue remodeling (M2). The present study used a rat model to determine the macrophage phenotype at the site of implantation of two biologic scaffolds that were derived from porcine small intestinal submucosa (SIS) and that differed mainly according to their method of processing: the Restore device (SIS) and the CuffPatch device (carbodiimide crosslinked form of porcine-derived SIS (CDI-SIS)). An autologous tissue graft was used as a control implant. Immunohistologic methods were used to identify macrophage surface markers CD68 (pan macrophages), CD80 and CCR7 (M1 profile), and CD163 (M2 profile) during the remodeling process. All graft sites were characterized by the dense population of CD68+ mononuclear cells present during the first 4 weeks. The SIS device elicited a predominantly CD163+ response (M2 profile, p < 0.001) and showed constructive remodeling at 16 weeks. The CDI-SIS device showed a predominately CD80+ and CCR7+ response (M1 profile, p < 0.03), and at 16 weeks was characterized by chronic inflammation. The autologous tissue graft showed a predominately CD163+ response (M2) at 1 week, with a dual M1/M2 population (CD80+, CCR7+, and CD163+) by 2 and 4 weeks and moderately well organized connective tissue by 16 weeks. The processing methods used during the manufacturing of a biologic scaffold can have a profound influence upon the macrophage phenotype profile and downstream remodeling events. Routine histologic examination alone is inadequate to determine the phenotype of mononuclear cells that participate in the host response to the scaffold.
Introduction
The presence of large numbers of tissue macrophages and their multinucleate giant-cell counterpart is one of the hallmarks of chronic inflammation. Typically, the host inflammatory response to an implanted biomaterial follows a predictable sequence of events, with downstream consequences of foreign-body giant-cell formation and fibrosis at the host–implant interface. 2 However, phenotypic and functional polarization of the mononuclear phagocyte cell population has recently been described,3–6 which is similar to the Th1/Th2 polarization scheme of lymphocytes. 7 The pro-inflammatory, cytotoxic macrophage phenotype, signified as M1, is characterized by cells that promote pathogen killing and is associated with classic signs of inflammation, especially chronic inflammation. The anti-inflammatory macrophage phenotype, signified as M2, promotes immunoregulation, tissue repair, and constructive tissue remodeling. Although morphologically indistinguishable using routine methods of examination, mononuclear macrophages from these two pathways can be identified and distinguished according to their cell surface markers and their cytokine and gene expression profiles.6,8,9 To our knowledge, the effect of these two macrophage phenotypes upon biologic scaffold remodeling, especially in the context of tissue engineering and regenerative medicine, has not been previously considered.
The objectives of the present study were to examine the association between macrophage phenotype response and tissue remodeling in a rodent model of body wall repair and to determine the effect of ECM processing methods, most notably chemical cross-linking, upon the phenotype of responding macrophages (e.g., polarization profile). The two ECM scaffolds used in the present study were similar in all aspects except for one variable: the use of carbodiimide during the processing of the materials for human clinical use.
Materials and Methods
Overview
Thirty-six rats were randomly divided into three equal groups of 12 each. A 1.0-cm2 partial-thickness defect was created in the ventrolateral abdominal wall of each animal. The defect was repaired with one of three different materials: an ECM biologic scaffold composed of porcine-derived small intestinal submucosa (SIS), a carbodiimide crosslinked form of porcine-derived SIS (CDI-SIS), or autologous body wall tissue. Three animals in each group were sacrificed at 1, 2, 4, or 16 weeks after surgery. The explanted tissues were examined using standard histologic methods and immunohistochemical methods for cell surface markers representative of an M1 (CD80+ or CCR7+) or M2 profile (CD163+). All procedures were performed in accordance with the National Institutes of Health guidelines for care and use of laboratory animals and with approval of the Institutional Animal Care and Use Committee at the University of Pittsburgh.
Test articles
The biologic scaffolds used in this study were the Restore device (Depuy Orthopaedics, Warsaw, IN), a 10-layer configuration of porcine SIS that is maintained in its native state (i.e., not chemically modified) after decellularization (SIS); CuffPatch (Arthrotek, Warsaw, IN), an eight-layer configuration of the same porcine SIS ECM that is cross-linked with carbodiimide after decellularization (CDI-SIS); and autologous body wall tissue. The Food and Drug Administration has approved the first two devices for musculotendinous soft tissue repair where weakness exists. Both of these biologic scaffold materials were purchased from the manufacturer and were handled according to product specifications as detailed in the package insert.
Experimental animals
Sprague-Dawley rats weighing 300 to 500 g were purchased from Charles River Laboratory (Wilmington, MA). Each animal was fed a diet of Purina Iso Pro and housed individually in an environment maintained at 68° to 76°C for 24 h a day and with a light:dark cycle of 12:12 hours.
Surgical procedure
The abdominal wall defect model has been previously described.1,10 Surgical plane anesthesia in each animal was induced and maintained with 2% isoflurane in oxygen. The ventral abdomen was shaved and prepared for surgery in sterile fashion. A midline incision was made, and the underlying muscle tissue lateral to the linea alba was separated from the skin and subcutaneous tissues. A 1.0-cm2 partial-thickness abdominal wall segment was excised and replaced with a size-matched graft of the SIS device, the CDI-SIS device, or the autologous excised abdominal wall tissue. The underlying transversalis fascia and peritoneum were left intact; therefore, the abdominal cavity was not entered. The grafts were sutured in place at each corner with 4-0 Prolene to secure and demarcate the boundaries of the device. The incision was then closed with a subcuticular stitch using 4-0 Vicryl. The animals recovered from anesthesia on a heating pad and were returned to the housing unit.
Buprenex (0.02 mg) and gentamicin (2.0 mg) were administered by subcutaneous injection after surgery and for 2 additional days. The surgical site was evaluated daily for signs of swelling, infection, or discoloration, and the findings were recorded. The dietary habits and general health of each animal were recorded daily.
Euthanasia and specimen harvest
At the predetermined time, the animals were anesthetized with 5% isoflurane and euthanized using an intracardiac bolus injection of potassium chloride to induce cardiac arrest. The grafts were harvested with an equal amount of adjacent native abdominal wall tissue. The specimens were fixed in 10% neutral buffered formalin, trimmed, and embedded in paraffin.
Histology and immunohistochemistry
Serial sections of the embedded tissue specimens were then cut at 6-μm intervals. The tissue sections were stained with hematoxylin and eosin or Masson's trichrome, and representative sections were prepared for immunohistochemical staining by deparaffinization with xylene and rehydration through a graded ethanol series. A heat-mediated antigen-retrieval technique that included a 20-min boil in 0.01 M citrate buffer, pH 6.0 (Spectrum, New Brunswick, NJ) was used. After cooling, two separate 5-min washes in Tris buffered saline (TBS)/Tween20, pH 7.4, followed by one wash in phosphate buffered saline (PBS) were performed.
The primary antibodies used for immunohistochemical staining were mouse anti-rat CD68 (Serotec, Raleigh, NC) at 1:50 dilution in PBS, mouse anti-rat CD80 (Serotec) at 1:10 dilution, mouse anti-rat CD163 (Serotec) at 1:50 dilution, rabbit anti-CCR7 (Cell Applications, Inc., San Diego, CA) at 1:100 dilution, and mouse immunoglobulin (Ig)G1 isotype, rat absorbed (Serotec) at 1:10 dilution. CD80 and CCR7 are surface markers indicative of an M1 phenotype, and CD163 is a surface marker representative of an M2 phenotype. 9 A preliminary study in our laboratory showed that the expression of CD80 and CCR7 in populations of rat tissue macrophages was equivalent. The secondary antibody used was biotinylated anti-mouse IgG (Vector, Burlingham, CA) at 1:200 dilution for CD68, CD80, and CD163 and biotinylated anti-rabbit IgG (Vector) for CCR7. Formalin-fixed rat spleen served as the positive control tissue for all immunohistochemical procedures.
To prevent non-specific antibody binding, the slides were incubated for 30 min with 2% normal horse serum (Vector) at room temperature. The slides were incubated with 3% hydrogen peroxide (Spectrum) in methanol for 30 min at room temperature to inhibit endogenous peroxidase activity. The slides were incubated with secondary antibody for 30 min at room temperature, followed by horseradish peroxidase solution (Vector) for 30 min at 37ºC. Diaminobenzidine (Vector) was applied to detect positive staining cells, and the slides were counterstained with hematoxylin.
Analysis
Two investigators who were blinded to the identity of the tissue specimen and to the antigen being positively identified in each specimen independently conducted quantitative analysis. Immunopositive cells were counted for each specimen in six matched microscope fields at 400× magnification. The percentage of cells expressing an M1 phenotype was calculated by dividing the number of CD80+ cells or CCR7+ cells by the number of CD68+ cells in each field. The percentage of cells expressing an M2 phenotype was determined by dividing the number of CD163+ cells by the number of CD68+ cells in each field. The mean value for the percentage of cells showing an M1 and M2 phenotype was then calculated by obtaining the average of the six fields for each specimen at each timepoint. An M1/M2 ratio was then calculated for each specimen at each timepoint. The presence of the CD68 surface marker indicated a macrophage phenotype. Not all macrophages showed differentiation markers to an M1 or M2 state, which accounted for the total number of M1 plus M2 macrophages not necessarily equaling the number of CD68+ cells. 11
Statistical analysis
The data were analyzed using a two-way analysis of variance. The factors analyzed were devices with three levels (SIS, CDI-SIS, and autologous tissue control) and time in weeks with four levels (1, 2, 4, and 16 weeks), with a statistically significant interaction between device and time. Comparisons were made between the three devices at each timepoint. Therefore, a total of 12 comparisons were made for each outcome variable. Bonferroni corrections for the multiple comparisons were used to control the error rate, with an overall error rate of 0.05.
Results
No complications occurred during the surgical procedures or post-operative period for any animals in this study. Immunohistochemical staining showed that all harvested tissue samples at the 1-, 2-, 4-, and 16-week timepoints contained CD68+ mononuclear cells (Table 1). For each of the outcome variables (M1 percentage and M2 percentage), the interaction between device and time was statistically significant.
Values represent the mean ± standard error of six microscope fields at 400× magnification for each specimen, for a total of 18 fields per graft type.
p < 0.05, ‡small intestinal submucosa (SIS) vs autologous, #SIS vs carbodiimide crosslinked SIS (CDI-SIS), **CDI-SIS vs autologous; statistical analysis according to Student t-test.
Immunohistochemical comparison of the local tissue macrophage population at the 2-week timepoint is shown in Figure 1. The SIS device was associated with a dominant M2 response, and the CDI-SIS device and autologous graft showed dual expression of M1 and M2 markers.

Photomicrographs at 2 weeks for each graft type at matched sites. Histologic sections stained with Masson's trichrome showed that the M1 and M2 macrophages were indistinguishable. The macrophage phenotype within each section was identified using immunohistochemical staining for CD68 (pan macrophages), CD80 (M1 macrophages), and CD163 (M2 macrophages). CD68+ cells were present in all grafts. CD80+ cells were present in the carbodiimide crosslinked small intestinal submucosa (CDI-SIS) and autologous tissue grafts and in much smaller numbers in the SIS graft. CD163+ cells were present in large numbers in the SIS graft and in much smaller numbers in the CDI-SIS and autologous tissue grafts. Scale bar = 50 μm.
SIS device
The surgical sites in which the native SIS device was placed showed an intense mononuclear cell response at 1, 2, and 4 weeks, with infiltration of these cells between the individual layers of the multi-laminate SIS device. These mononuclear cells were predominantly of an M2 phenotype (i.e., CD163+) at all timepoints (p < 0.001). By 4 weeks, only remnants of the SIS device could be identified. By 16 weeks, there was no histologic evidence of the SIS device, and the surgical site was characterized by organized collagenous connective tissue, skeletal muscle tissue, and occasional CD163+ mononuclear cells (Fig. 2A).
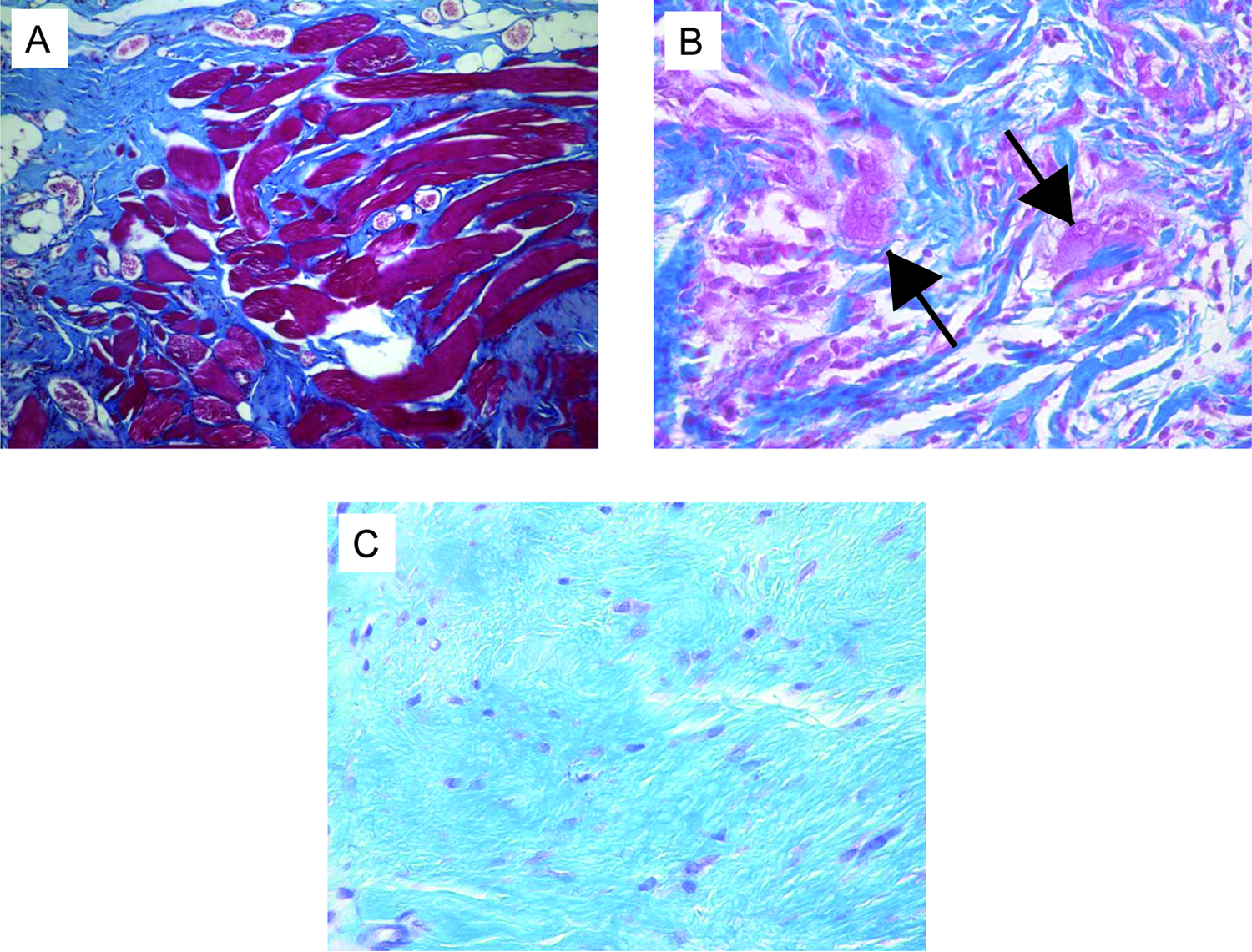
Masson's trichrome staining at 16 weeks post-surgery for each graft type. (
CDI-SIS device
The surgical sites in which the CDI-SIS was placed showed an intense mononuclear cell and polymorphonuclear cell response at 1 and 2 weeks. These cells surrounded but did not infiltrate the device and the mononuclear macrophages were characterized by an equal number of CD163+, CD80+, and CCR7+ cells. The 4-week results show a predominantly M1 profile (p < 0.03), and these M1 cells were located primarily at the edges of the scaffold. At 16 weeks, mononuclear cells and multinucleate giant cells were present and were associated with fibrosis around the scaffold material (Fig. 2B).
Autologous tissue graft
The surgical sites at which the autologous tissue was placed showed a dense infiltration of neutrophils and CD68+ mononuclear cells, with necrosis of muscle fiber bundles at 1 and 2 weeks post-surgery. The mononuclear cell population showed a predominantly M2 phenotype at 1 week (p < 0.001). By 2 weeks and all timepoints thereafter, approximately equal numbers of CD163+, CD80+, and CCR7+ cells were present. There was a deposition of moderately well-organized collagenous connective tissue present at 4 weeks. By 16 weeks, poorly organized fibrous connective tissue had replaced the autologous tissue graft (Fig. 2C).
A bar graph of the phenotypic profile for each device at each timepoint is shown in Figure 3. The M1:M2 ratio for all timepoints for all grafts is shown in Figure 4. In general, a dominant M2 response characterized the SIS device. A mixed response characterized the CDI-SIS device during the first 2 weeks, with a dominant M1 response at the later timepoints. The autologous tissue graft showed a dominant M2 phenotype at 1 week and a duality of M1 and M2 phenotypic macrophages at the remaining timepoints.

The macrophage polarization percentages for (
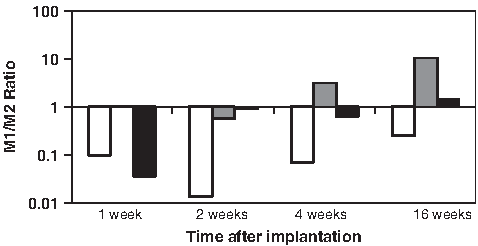
The ratios of M1:M2 percentages are illustrated for each device: small intestinal submucosa (SIS; Restore) white bars, carbodiimide crosslinked SIS (CDI-SIS; CuffPatch) gray bars, and autologous grafts black bars at each timepoint after implantation. The SIS device showed consistent values of less than 1.0 (predominant M2 response). The CDI-SIS showed values greater than 1.0 at the later timepoints (predominant M1 response).
Discussion
Biologic scaffolds are now commonly used to promote the repair and restoration of functional tissue.1,12–15 Although most if not all of these scaffold materials are composed of ECM or components of ECM, the clinical and tissue remodeling outcomes differ greatly. The present study showed that the phenotype of mononuclear macrophages that participate in the host response to biologic scaffold materials can differ markedly and that the method of material processing was an important variable.
Mononuclear cells are commonly observed and are expected participants in the host response to biomaterials, including those that are used as scaffolds for tissue reconstruction. The term “mononuclear cell” is a generic morphologic description for a population of cells with a single nucleus, a round or oblong shape, and variable amounts of cytoplasm. Mononuclear cells in tissue are usually considered to have phagocytic or macrophage capability; possess cytoplasmic lysosomes laden with proteolytic enzymes; and express CD13, CD14, CD68, and CD115 membrane antigens. 16 The classic interpretation of large numbers of mononuclear cells surrounding an implanted biomaterial is that of a chronic inflammatory reaction with downstream consequences of necrosis, fibrosis with encapsulation, some degree of scar tissue formation, or a combination of the three.17–19 It is now recognized that a variety of cell types, including progenitor cells (e.g., vascular endothelial progenitor cells),20–23 circulating fibrocytes,24–26 blood monocytes, 27 and other cell types28–30 are virtually indistinguishable upon routine examination of peripheral blood or tissue sections and that all satisfy the morphologic description of a mononuclear cell.
The proposed paradigm for M1 and M2 macrophage differentiation is based upon observations of differential cytokine expression profiles and cell surface markers. 9 M1 macrophages are characterized by expression of CD68, CD80, and CCR7 cell surface markers in rats (species differences exist); the production of large amounts of nitric oxide and other reactive oxygen intermediates; and copious amounts of pro-inflammatory cytokines 9 such as interleukin (IL)-12, IL-6, and tumor necrosis factor alpha. Conversely, M2 macrophages produce high levels of IL-10 and transforming growth factor beta expression, produce large amounts of arginase, inhibit the release of pro-inflammatory cytokines, 31 scavenge debris, promote angiogenesis, and recruit cells involved in constructive tissue remodeling.9,32 M2 macrophages express CD68 and CD163 surface markers in rats, but again, species differences exist.
The present study characterized the macrophage population that participated in the remodeling response as a function of the M1 and M2 polarization schemes in a rat model. The sum of M1 and M2 immunopositive cells did not always equal the number of CD68 immunopositive cells. 11 CD68+ macrophages that were not yet determined to be an M1 or M2 phenotype would remain negative for the respective markers.
The host tissue response to a biomaterial is, by definition, the central factor in the eventual remodeling outcome. Naturally occurring and synthetic materials are commonly used in tissue engineering and regenerative medicine strategies for tissue and organ replacement. Collagen constitutes approximately 90% of the total protein content in many biologic scaffolds used in tissue engineering and regenerative medicine, including SIS ECM. Cross-linking agents, such as carbodiimide, are often included in the processing of biologic materials to impart added strength and to slow the degradation rate. Collagen materials subjected to carbodiimide treatment show intra- and inter-helical crosslinks of the tropocollagen molecules, which would logically change the surface architecture on a molecular level. 33 The surface topology and molecular organization of biomaterials clearly affect macrophages, and the cell–surface interaction can change the quantity and identity of secreted proinflammatory cytokines and chemokines, 34 the gene expression pattern, 35 and downstream remodeling events.36,37 Chemical cross-linking can also lead to “frustrated phagocytosis” 2 by macrophages, which will affect their M1/M2 phenotype. In the current study, chemical cross-linking of the SIS scaffold with carbodiimide resulted in a switch from an M2-dominant profile to an M1-dominant profile and a change in the long-term (16 week) remodeling outcome from constructive remodeling to chronic inflammation. The M2 response was associated with an organized, site-appropriate tissue-remodeling outcome and an absence of persistent inflammation. Carbodiimide cross-linking was associated with an M1 response, long-term inflammation, and the formation of multinucleate giant cells and scar tissue. The specific ligand-receptor interactions between macrophages and the scaffold surfaces are not currently known and are beyond the scope of this study.
There were several limitations in the present study. First, the determination of M1 versus M2 phenotype was based upon a limited number of cell surface markers. Although many markers exist to differentiate between M1 and M2 macrophages for murine and human tissues, most of these same markers are not available for the analysis of rat tissue, especially formalin-fixed tissue. CD68 identifies cells from the monocyte-macrophage lineage, including activated monocytes, resting-tissue macrophages, and activated macrophages; CD80 and CCR7 identify M1-activated cells; and CD163 shows high expression in M2-activated macrophages. 38 Although the results of the study and the staining affinities of the two macrophage populations were distinct, many other functional criteria of cells could have been examined, including cytokine expression profiles. Cytokine tissue levels were not determined in the present study. One would expect proinflammatory cytokines to be present within and surrounding the implants that showed a dominant M1 profile.
It is unknown whether macrophages that were not committed to the M1 or M2 phenotype were recruited to the site of scaffold remodeling and then stimulated to differentiate locally or whether phenotype-committed macrophages were selectively recruited to sites of remodeling depending upon the antigens or substrates that were present. In either case, the present study would suggest that strategies for tissue engineering and regenerative medicine that promote an M2 response are associated with a favorable remodeling response.
The present study represents the first attempt to link macrophage phenotype to scaffold remodeling in the context of tissue engineering and regenerative medicine. The study was limited to a single form of biologic scaffold material (SIS-ECM), but the principles may also be applied to all scaffold materials, including synthetic and biologic materials.
Footnotes
Acknowledgments
Funding for this study was provided through a grant from the National Institutes of Health (R01 AR054940-01).
Disclosure Statement
The authors have no professional or financial affiliations that would have biased this manuscript.