
Abstract
Previous studies have shown that synthetic octacalcium phosphate (OCP) facilitates in vitro osteoblastic cell differentiation in an OCP dose–dependent manner and that a complex of OCP and collagen (OCP/collagen) enhances critical-sized rat calvaria defects more than OCP alone. The present study was designed to investigate whether the bone regenerative properties of OCP/collagen are augmented in an OCP dose–dependent manner, thereby establishing a suitable composition of this composite as a bone substitute material. OCP/collagens with a wide range of mixing ratios from 23:77 to 83:17, including the previously examined composition (77:23), were prepared by blending granules of OCP with atelocollagen and molded into a disk as an implant. A critical-sized defect was made in rat calvaria, and each disk was implanted into the defect for 4 or 12 weeks and then examined radiographically, histologically, and histomorphometrically. Mouse bone marrow–derived stromal ST-2 cells were cultured in dishes pre-coated with OCP/collagen or OCP alone with different OCP contents to determine the capacity of cell attachment and proliferation up to 14 days. Histological and radiographic examinations showed that newly formed bone was observed in relation to OCP granules within the collagen matrix. Histomorphometric analysis confirmed that increasing the amount of OCP in collagen matrices resulted in progressive enhancement of bone regeneration and that the ratio 83:17 generated the maximum repair level of approximately 64% of the defect at 12 weeks. OCP/collagen promoted the proliferation and attachment of ST-2 cells more than OCP alone regardless of OCP content. Fourier transform infrared spectroscopy analysis of the coatings after the incubation indicated that OCP tended to convert to apatite regardless of the presence of collagen. The present study demonstrated that the osteoconductive characteristics of OCP/collagen can be displayed in an OCP dose–dependent manner. The results suggest that collagen promotes the proliferation and attachment of host osteoblastic cells on OCP/collagen composite implants.
Introduction
Recently, the importance of synthetic OCP as a bone substitute material was further recognized in the field of tissue engineering for bone regeneration.7- 9 Much attention has been paid to the use of synthetic OCP with the expectation of it acting as potential loci for the nucleation of bone induction in orthotopic sites, which could be replaced with a significantly higher volume of newly formed bone than the other calcium phosphate phases such as HA 10 or amorphous carbonated apatite. 11 The osteoconductivity of OCP was first found in a granule form when implanted in the subperiosteal region of mouse calvaria.12–14 The biological responses to OCP have also been investigated in the forms of coatings on metallic implants,7,8,15 with osteoblastic cell proliferation, 15 or by implantation into subcutaneous tissue or bone defects.7,9,11,16,17 Moreover, recent studies have found that OCP facilitates in vitro osteoblastic cell differentiation.17–19 We further found that bone regeneration and in vitro osteoblastic cell differentiation are enhanced when OCP is converted into HA 17 and that osteoblastic cell differentiation is significantly facilitated in an OCP dose–dependent manner. 20
OCP cannot be molded using sintering processes, unlike bioceramics such as HA or beta-tricalcium phosphate (β-Ca3(PO4)2; β-TCP) because of the intrinsic crystal structure of OCP, including a large number of water molecules within the layered HA structure. 1 Previous studies clarified that combining OCP with collagen (OCP/collagen) not only overcomes this poor moldability, but also improves the osteoconductivity of OCP in critical-sized rat calvaria defects. 21 However, it is still unclear whether the composition of OCP/collagen is optimized with regard to osteoconductive characteristics in the light of the recent finding that OCP stimulates its own osteogenic capability in an OCP dose–dependent manner in vitro. 20 We hypothesized that OCP provides loci to initiate bone formation within OCP/collagen, as proposed in the physiological mineralization mechanism, 6 and that increasing the OCP content in this composite results in increments of nucleation that lead to enhanced bone regeneration. The present study was designed to test this hypothesis and establish a suitable composition of OCP/collagen to most effectively repair critical-sized rat calvaria defects.
Materials and Methods
Preparation of octacalcium phosphate, collagen, and composites of OCP/collagen
OCP was prepared by mixing calcium and phosphate solutions as described previously.12,22 Sieved OCP granules (particle sizes 300–500 μm) obtained from the dried OCP were sterilized by heating at 120°C for 2 h. Our previous study showed that such heating does not affect such physical properties as the crystalline structure or specific surface area of OCP granules,13,23 although it was reported that increasing the temperature above 100°C induced the collapse of the OCP structure because of dehydration.24,25 Collagen was prepared from NMP collagen PS (Nippon Meat Packers, Tsukuba, Ibaraki, Japan), a lyophilized powder of pepsin-digested atelocollagen isolated from porcine dermis. NMP collagen PS was dissolved in distilled water and adjusted to a final concentration of 3% at pH 7.4. The concentrated collagen was lyophilized, and a disk was molded (9 mm diameter, 1 mm thick). OCP/collagen was prepared from NMP collagen PS and OCP granules. OCP was added to the concentrated collagen and mixed. The weight percentages of OCP in OCP/collagen were 23%, 50%, 77%, and 83% (OCP23/collagen, OCP50/collagen, OCP77/collagen, and OCP83/collagen). These OCP/collagen mixtures were then lyophilized, and disks were molded (9 mm diameter, 1 mm thick). The molded OCP/collagen and collagen underwent dehydrothermal treatment (150°C, 24 h) in a vacuum drying oven (DP32, Yamato Scientific, Tokyo, Japan) and sterilized using electron beam irradiation (5 kGy).
Animals
Twelve-week-old male Wistar rats (SLC, Hamamatsu, Shizuoka, Japan) were used. The principles of laboratory animal care were followed, as well as national laws. The Animal Research Committee of Tohoku University approved all procedures.
Implantation procedure
The experimental rats were anesthetized using intraperitoneal sodium pentobarbital (50 mg/kg) supplemented by ether inhalation. A skin incision was made aseptically along the bilateral temporal line and the middle of the forehead, and the dissection was continued to the calvarium. The periosteum of the calvarium was ablated, and a full-thickness standardized trephine defect, 9 mm in diameter, was made in the calvarium under continuous saline buffer irrigation. Extreme care was exercised to avoid injury to the midsagittal blood sinus and dura mater. OCP/collagen or collagen was implanted into the trephine defect. As a negative control, untreated animals were processed in the same way except that nothing was implanted after the defects were created. After the defects were treated, the ablated periosteum and skin were repositioned and sutured, respectively. The calvarial tissue of five rats in each of OCP/collagen, collagen, and untreated groups were fixed at 4 and 12 weeks after implantation.
Radiographic analysis
The rats were anesthetized using intraperitoneal sodium pentobarbital (50 mg/kg) and then the tissues were fixed with 4% paraformaldehyde in 0.1 M phosphate buffered saline (PBS, pH 7.4) by perfusion through the aorta. The implants were resected together with the surrounding bones and tissues and kept in the same fixative overnight at 4°C. The skulls were radiographed using a microradiography unit (Softex CMR Unit, Softex, Tokyo, Japan) with X-ray film (FR; Fuji Photo Film, Tokyo, Japan) under standardized conditions (16 KV, 5 mA, 1 min) under which OCP showed no radiopacity.
Tissue preparation
After the radiographs were taken, the samples were decalcified in 10% ethylenediaminetetraacetic acid in 0.01 M phosphate buffer, pH 7.4, for 2 to 4 weeks at 4°C. The samples were dehydrated in a graded series of ethanol and embedded in paraffin. The center of the defect was extracted and sectioned coronally at a thickness of 5 μm. The sections were stained with hematoxylin and eosin, and photographs were taken using a photomicroscope (Leica DFC300 FX, Leica Microsystems Japan, Tokyo, Japan).
Quantitative micrograph analysis
Light micrographs of the sections stained with hematoxylin and eosin were used for histomorphometric measurements. Photographs projecting the overall defect were taken from each specimen. The percentage of newly formed bone in the defect (n-Bone%) was calculated as area of newly formed bone per area of the defect originally created busingy trephination × 100. n-Bone% was quantified on a computer using Scion Image public domain software (Scion Corporation, Frederick, MD).
Coating of OCP and OCP/collagen onto plates for culture
OCP granules were ground using a pestle and mortar and then passed through a USA standard testing sieve (270 mesh, 53 μm pore size). The sieved OCP was suspended in water for OCP coating and in a solution of 0.16% collagen with 0.013 M 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) buffer for OCP/collagen coating and then dropped onto each well of a 48-well plate (Corning Inc., Corning, NY) using a pipette. The quantity of OCP was adjusted to 0.0 (collagen itself), 0.3, 1.5, and 3.0 mg/well (weight%, 0, 38, 75, and 90). The plates were placed in an oven at 37°C for drying overnight, allowing the suspension to dry for sufficient adherence to the plate during incubation. Then plates were sterilized through irradiation using an ultraviolet linker (FS-1500, FUNAKOSHI, Tokyo, Japan). A coating-free plate (plastic) was prepared as a control.
Cell culture
Mouse bone marrow stromal ST-2 cells were obtained from RIKEN Cell Bank (Tsukuba Science City, Ibaraki, Japan). Cells were maintained in alpha-minimal essential medium (α-MEM) containing 10% fetal bovine serum (FBS; Sigma-Aldrich, St. Louis, MO) and 1% penicillin/streptomycin (Invitrogen-Gibco, Carlsbad, CA) at 37°C in a 5% carbon dioxide environment.
Attachment of ST-2 cells on OCP or OCP/collagen
ST-2 cells (5 × 104) suspended in 250 μL of α-MEM (containing 10% FBS) were seeded into each well of a 48-well tissue culture plate pre-coated with OCP, OCP/collagen, or no coating. The plates were incubated for 10 h. After washing the wells and adding fresh medium, the cell numbers on the coating plates were determined by measuring living cells using the WST-8 assay. The attachment was calculated as the number of cells on the coating of OCP, OCP/collagen, or collagen per the number of cell on the control coating (plastic) ×100.
Observation of cell morphology
The morphology of ST-2 cells attached to OCP and OCP/collagen was observed using a scanning electron microscope (SEM, MARUTO Instrument Co. Ltd., TOKYO, Japan). After 1 day of incubation, the adherent cells on the substrates were fixed with 2% glutaraldehyde (Sigma-Aldrich) in PBS for 2 h at room temperature. After thorough washing with PBS, the cells on the surfaces were dehydrated in a graded series of ethanol (50%, 70%, 90%, 95%, and 100%) for 10 min each and immersed in tert-butyl alcohol (Wako Pure Chemical Industries, Ltd, Osaka, Japan) for 10 min, followed by drying under vacuum. Au-Pd was sputtered onto the samples before SEM observation.
Proliferation of ST-2 cells on OCP or OCP/collagen
ST-2 cells (3 × 104) suspended in 250 μL of α-MEM (containing 10% FBS) were seeded into each well of a 48-well tissue culture plate pre-coated with OCP, OCP/collagen, or no coating. The plates were incubated for 3, 7, and 14 days. For prolonged incubation, the culture medium was replaced with fresh medium every 3 days. The proliferation of cells on the coating plates was determined by measuring living cells using a WST-8 assay (Cell Counting Kit-8, DOJINDO MOLECULAR TECHNOLOGIES Inc., Tokyo, Japan).
Analysis of the crystal structure conversion of OCP or OCP/collagen
The sieved OCP (4.5 mg) was suspended in 150 μL of water for OCP coating and in 150 μL of 0.16% collagen with HEPES buffer for OCP/collagen coating, and then the OCP or OCP/collagen solution was coated onto a dish (35 mm diameter, 14 mm height, SUMITOMO BAKELITE CO., Ltd, Tokyo, Japan). The dishes were placed in an oven overnight at 60°C to coat OCP or at 37°C to coat OCP/collagen for drying, allowing the suspension to dry for sufficient adherence to the plate during incubation. Then the dishes were sterilized using irradiation in an ultraviolet linker. OCP and OCP/collagen were maintained in α-MEM. For prolonged incubation, the culture medium was replaced with fresh medium every 3 days. The dishes were incubated for 3, 7, and 14 days, and the dishes were washed in PBS and placed at room temperature for drying overnight. Fourier transform infrared spectroscopy (FTIR) was used to analyze the crystal structures of OCP and OCP/collagen. After incubation, the samples were washed with PBS, dried at 37°C, and collected from the dishes for FTIR. FTIR spectra of OCP and OCP/collagen were obtained using a HORITA FTIR FREEXACT-2 (HORIBA, Kyoto, Japan), with the sample diluted with KBr, over the range of 4000 to 400 cm−1 with 4 cm−1 resolution.
Statistical analysis
Histomorphometric data were analyzed using Excel v.X, (Microsoft Co., Redmond, WA). All values were reported as means ± standard deviations (SD). Statistical analysis was performed for all of the cellular and histomorphometric experiments. One-way analysis of variance (ANOVA) was used to compare the means between groups. If the ANOVA was significant, Tukey's multiple comparison analysis was used as a post hoc test.
Results
Radiographic examination
The results of the radiographic examination are shown in Figure 1. It was confirmed that OCP/collagen was not radiopaque before implantation. At week 4, there was little radiopacity in the defect implanted with OCP23/collagen. In OCP50/collagen, the radiopacity was greater than in OCP23/collagen, but the area of radiopacity was smaller than the defect. In OCP77/collagen, a larger area of thorn-like radiopacity amalgamated and condensed, and the radiopacity of OCP83/collagen was greater. In collagen, isolated pudgy radiopacities were scattered throughout the defect. In untreated defects, radiopacity was observed along the defect margins. By week 12, in OCP23/collagen and OCP50/collagen, the radiopacities became larger, but the defects were not fully filled. In OCP77/collagen, the amalgamated radiopacity was more condensed and became larger, and in OCP83/collagen, the radiopacity was larger than that of OCP77/collagen. With collagen, the radiopacity became slightly larger, and in the untreated defect, radiopacity was observed only along the defect margins.
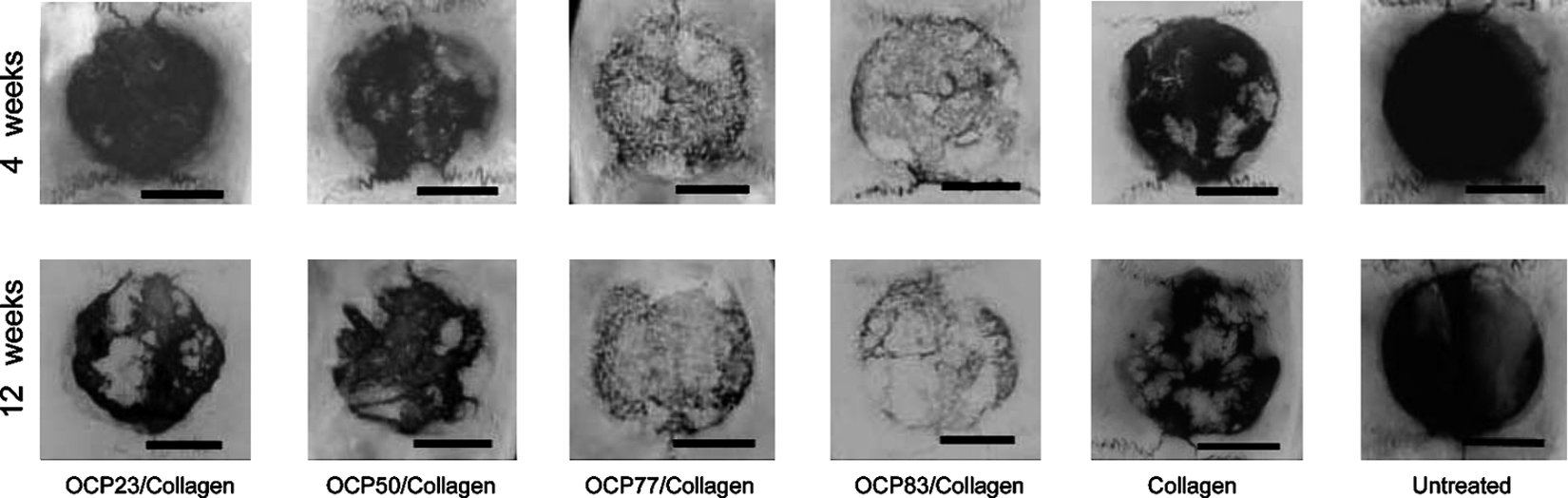
Radiographic examination of the implants. The area of radiopacity increased with increasing amount of OCP in OCP/collagen at weeks 4 and 12. The area of radiopacity at week 12 was larger than at week 4 in each OCP/collagen formulation. In collagen, isolated pudgy radiopacities were observed at week 4, and the radiopacities became larger at week 12. In untreated defects, radiopacity was observed along the defect margins. Bars = 4 mm.
Histological examination
An overview of histological sections at week 12 is shown in Figure 2, and detailed histological examination at week 12 is shown in Figure 3. Newly formed bone was observed sporadically in the defect in OCP23/collagen, and there was no remaining OCP. In OCP50/collagen, newly formed bone was observed sporadically in the defect, with a small amount of remaining OCP that was slightly bigger than in the case of OCP23/collagen. In OCP77/collagen, newly formed bone was observed throughout the defect and surrounding the remaining OCP. In OCP83/collagen, newly formed bone was observed in the same way as with OCP77/collagen, but the area of newly formed bone was larger than with OCP77/collagen. Multinucleated giant cells surrounded some of the OCP granules within OCP/collagen. Inflammatory cell infiltration was not observed at the implantation site. In collagen, bone formation was observed sporadically in the collagen sponge, and bone regeneration in the untreated control was restricted to the defect margin.
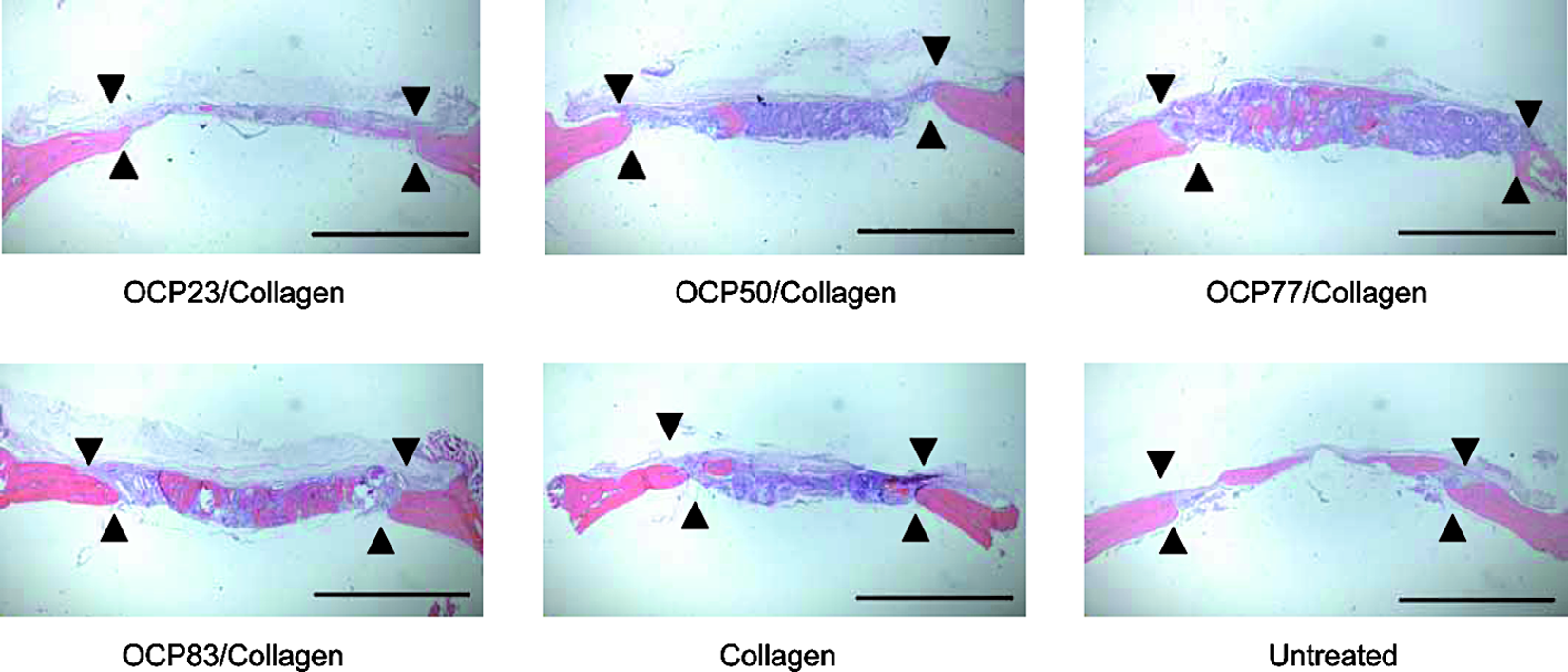
Overview of histological sections in the defects. An overview of the histological sections at week 12 shows that newly formed bone is regenerated throughout the defect in an octacalcium phosphate–collagen mix with 77% collagen (OCP77/collagen) and OCP83/collagen. Concentrical bone formation around OCP or sporadic bone formation in OCP23/collagen, OCP50/collagen, and collagen was observed, whereas bone regeneration was restricted to the defect margin in untreated animals. Bars = 4 mm, ▼; defect margin. Color images available online at www.liebertonline.com/ten.
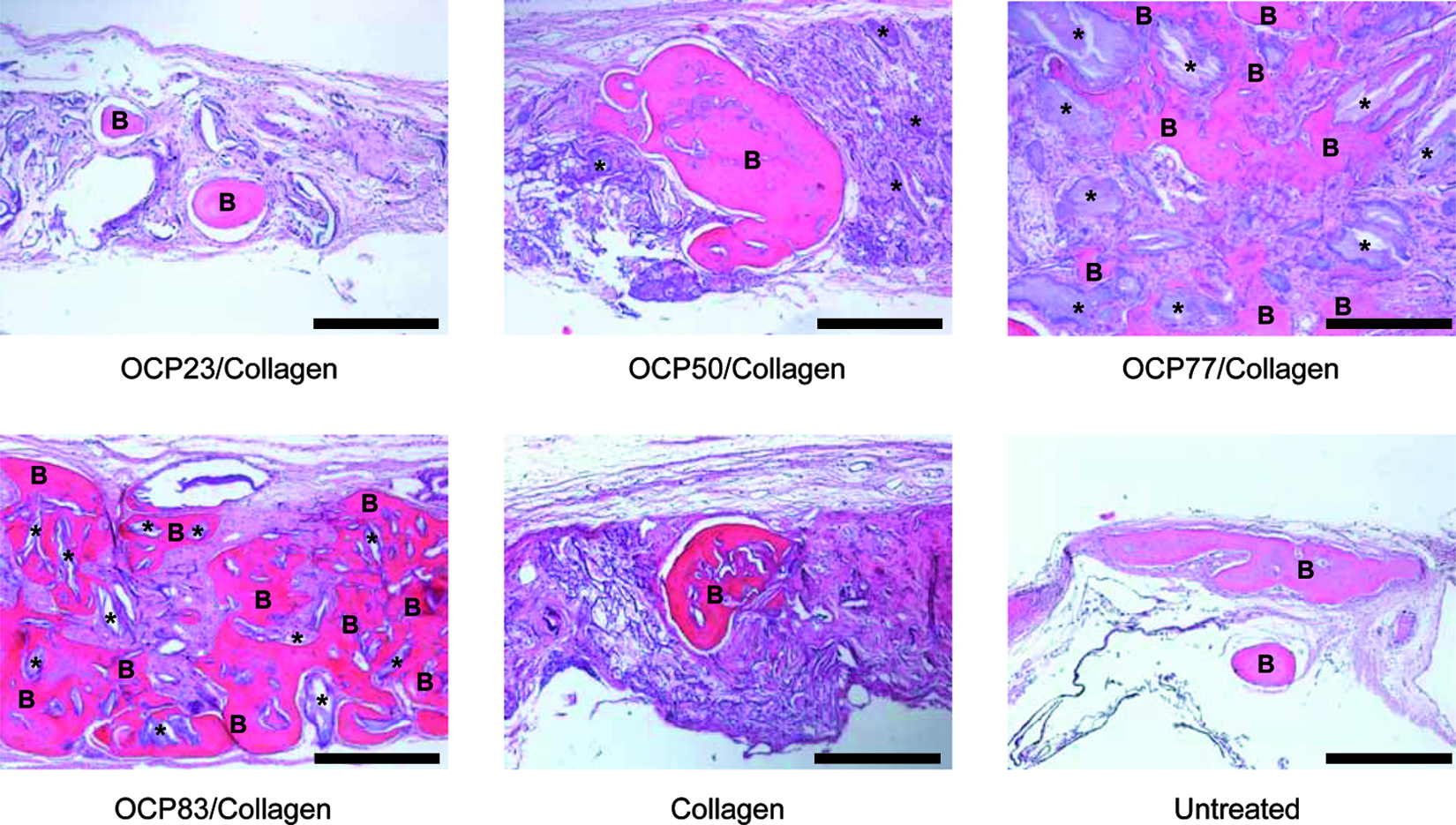
Histological examination of each OCP/collagen, collagen, and untreated (control) group at week 12. The area of newly formed bone (B) seemed to increase in an OCP dose–dependent manner. Newly formed bone surrounded the remaining OCP (asterisks). Multinucleated giant cells surrounded some implanted OCP in OCP/collagen. Inflammatory cell infiltration was not observed at the implantation site. Bars = 400 μm. Color images available online at www.liebertonline.com/ten.
Histomorphometric examination
Histomorphometric findings regarding n-Bone% are shown in Figure 4. By week 4, mean n-Bone% ± SD in OCP23/collagen, OCP50/collagen, OCP77/collagen, OCP83/collagen, collagen, and untreated was 7.94 ± 2.45, 10.79 ± 3.53, 15.32 ± 3.83, 17.07 ± 4.94, 9.97 ± 3.80, and 4.93 ± 1.75, respectively. An increase in n-Bone% with increasing OCP concentration in collagen was seen. A significant difference was observed between OCP23/collagen and OCP83/collagen. By week 12, n-Bone% ± SD in OCP23/collagen, OCP50/collagen, OCP77/collagen, OCP83/collagen, collagen, and untreated was 19.02 ± 6.41, 30.64 ± 2.67, 53.16 ± 5.42, 63.71 ± 7.53, 30.29 ± 2.98, and 26.80 ± 5.03, respectively. A significant difference was seen between OCP/collagen composites. However, when OCP23/collagen was implanted, the amount of the newly formed bone was less than that of the untreated sample. When OCP50/collagen was implanted, the amount of newly formed bone was almost equal to that of collagen.
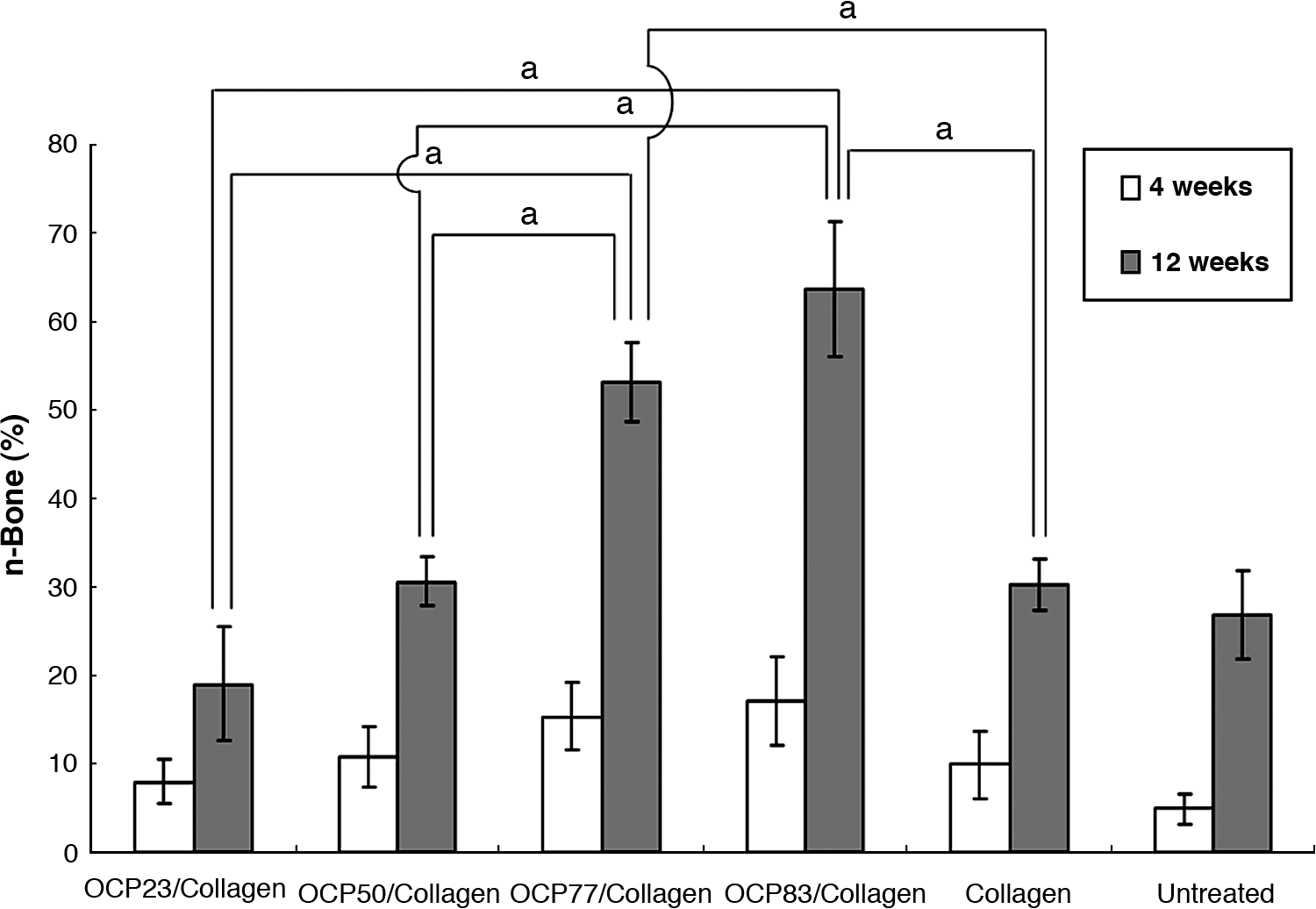
Quantitative analysis of newly formed bone in the defects. The percentage of new bone in the defect (n-Bone %) ± standard deviation in OCP/collagen, collagen, and untreated groups is shown. At week 4, a tendency that newly formed bone increased with increasing amount of OCP in OCP/collagen was shown. Significant differences were observed between an octacalcium phosphate–collagen mix with 23% collagen (OCP23/collagen) and OCP83/collagen (p < 0.05), OCP77/collagen and untreated (P < 0.05), and OCP83/collagen and untreated (p < 0.01). At week 12, a significant difference was seen between each OCP/collagen implant. ap < 0.01.
Cell attachment
Cell attachment to the OCP, OCP/collagen, and collagen surfaces was measured after 10 h of incubation. Figure 5 shows the number of cells attached to each substrate as a percentage of the number of cells on the plastic tissue culture plate (control). There were fewer cells on OCP than on OCP/collagen for each amount of OCP, than on collagen, and than on the control. There were more cells on OCP/collagen than on the control.
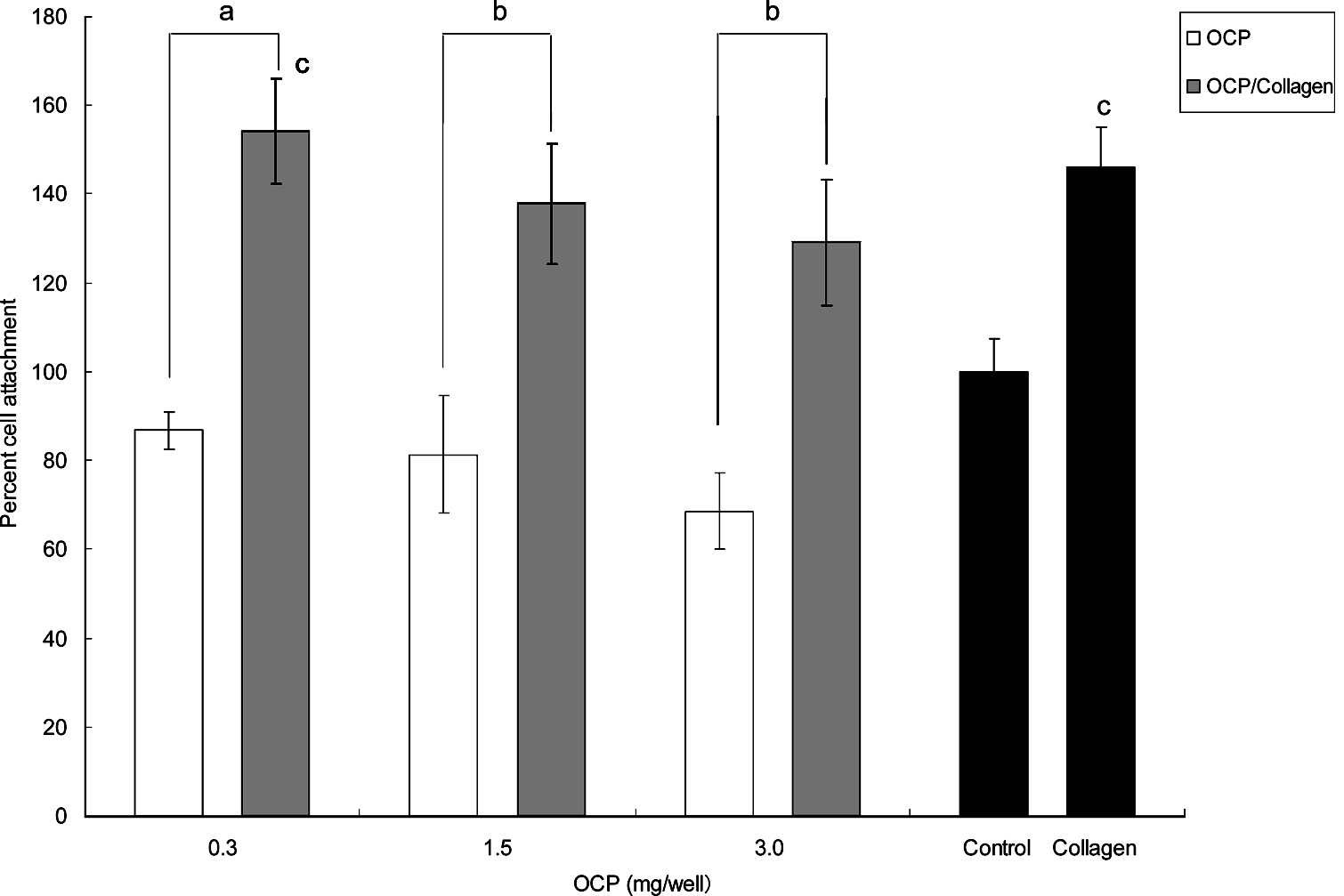
Cell attachment to OCP, OCP/collagen, collagen, and the plastic plate (control). The adhesion is indicated as the percentage of the number of cells attached to the control after 10 h of incubation. Data are mean values ± standard deviations (n = 3). Attachment on OCP was inferior to that on OCP/collagen for each amount of OCP. The attachment capacity decreased depending upon the amount of OCP in the initial stage of the culture in OCP and OCP/collagen. ap < 0.05, bp < 0.01 (c, versus control).
Morphology analysis
An analysis of cellular morphology on OCP and OCP/collagen was performed using SEM (Fig. 6). ST-2 cells on OCP showed a spindle shape with a long filopodia-like structure (Fig. 6A). ST-2 cells on OCP/collagen showed a flat polygonal shape in multiple directions (Fig. 6B). The cells cultured on OCP/collagen were more spread out than on OCP.
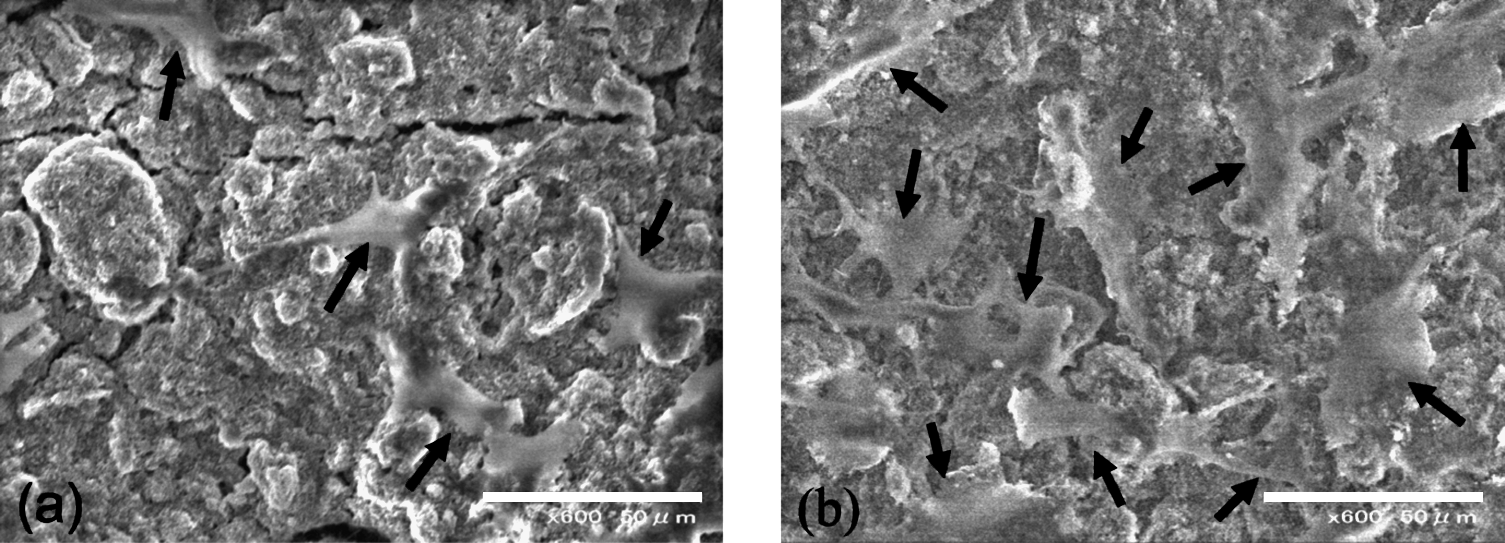
Scanning electron microscopy images of ST-2 cells adhering to OCP (
Proliferation of ST-2 cells cultured on OCP and OCP/collagen
ST-2 cell proliferation is shown in Figure 7. The presence of OCP and OCP/collagen resulted in a significantly lower rate of cell proliferation, which depended on the amount of coating in the initial stage of the culture. The inhibitory capacity of OCP was stronger than that of OCP/collagen. Consequently, the cells on OCP/collagen proliferated to a confluent state more rapidly than those on OCP.
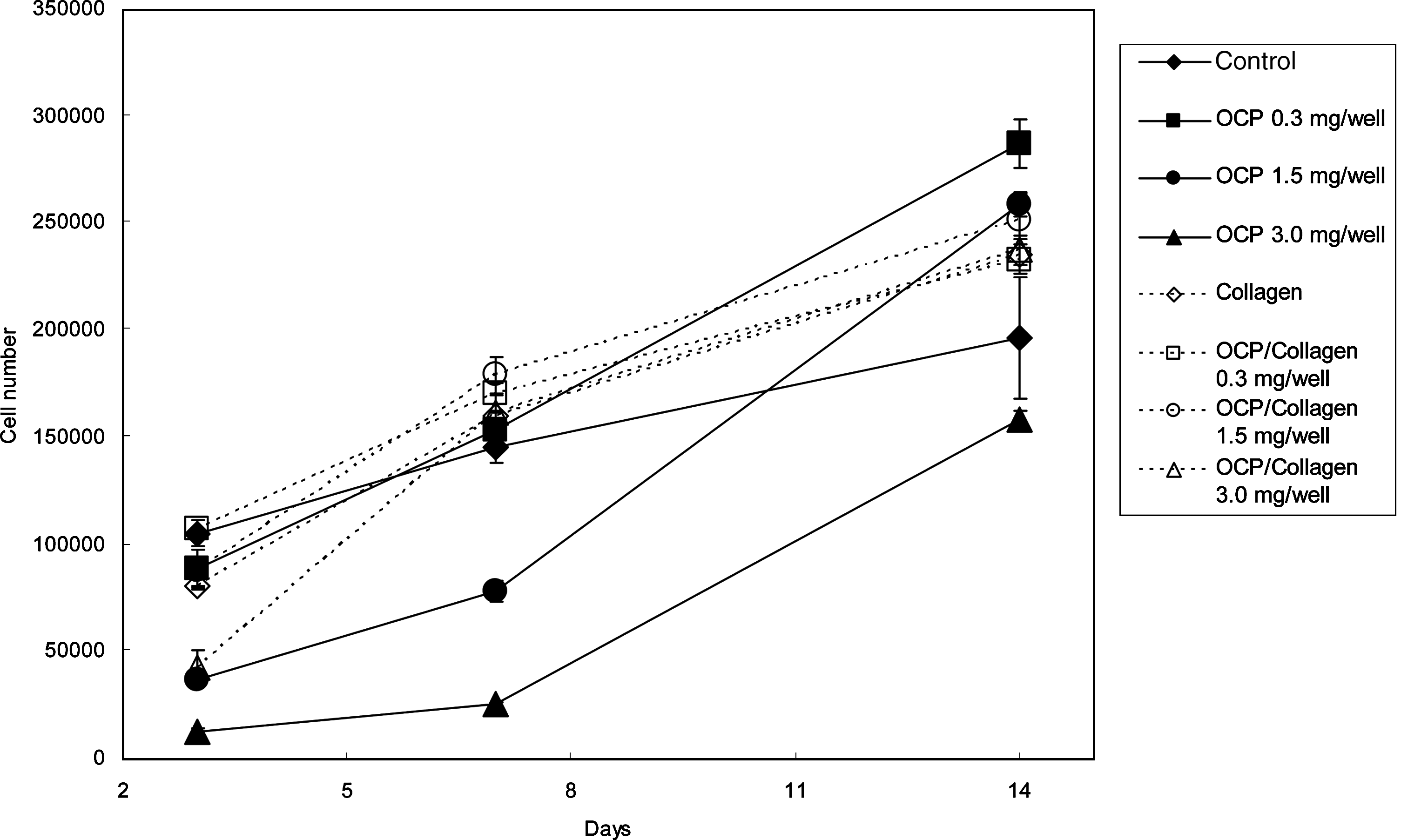
Cell proliferation of ST-2 cells on OCP, OCP/collagen, collagen, and the plastic plate (control). Data are the mean values ± standard deviations (n = 3). Proliferation of ST-2 cells on OCP coatings was more inhibited in the initial stage of culture than on OCP/collagen coatings containing the same amount of OCP.
Conversion of the crystal structure of OCP and OCP/collagen
Figure 8 shows FTIR spectra of OCP and OCP/collagen before and after incubation for 14 days. The FTIR spectrum of the original OCP or OCP in OCP/collagen composite corresponded well with that reported previously. 24 The three distinct bands originating from ν3 P-O in the orthophosphate stretch absorption or approximately 1030 to 1130 cm−1 tended to obscure the splitting peaks at 1119 cm−1 and 1124 cm−1 (indicated by arrows in Fig. 8) with the progression of OCP-apatite conversion. This change has been ascribed to the conversion of OCP to HA.17,26 Two sharp absorption bands of ν4 phosphate at 560 to 600 cm−1 remained constant, which was ascribed to crystalline calcium phosphate.
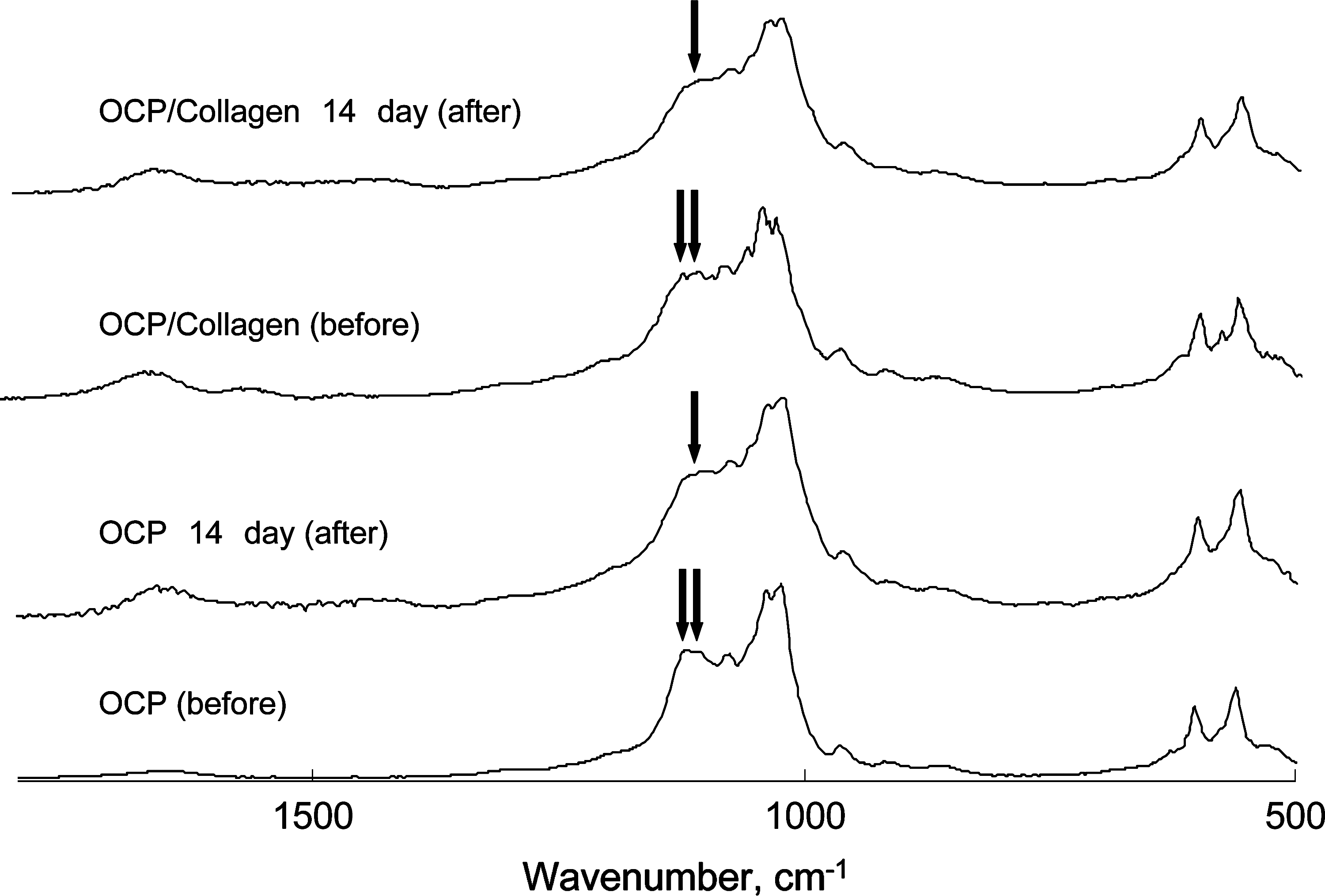
Fourier transform infrared spectroscopy spectra of OCP and OCP/collagen before and after incubation for 14 days. Infrared spectral bands around 1030 to 1130 cm−1 became obscured by day 14, indicating a tendency of conversion from OCP to hydroxyapatite.
Discussion
The present study provided evidence that bone regeneration in OCP/collagen is facilitated in an OCP dose–dependent manner. OCP/collagen promoted osteoblastic cell proliferation and attachment in vitro better than OCP alone. Our previous study found that OCP stimulates in vitro osteoblastic cell differentiation in an OCP dose–dependent manner, accompanied by marked greater expression of osteoblast-related gene, such as Osterix, collagen I, and alkaline phosphatase. 20 A method to combine OCP with collagen has been reported to enhance bone regeneration in rat bone marrow 27 and in critical-sized rat calvaria defects. 21 The present results suggest that the bone regenerative property of OCP/collagen can be controlled using the content of OCP and displayed according to the intrinsic osteogenic property of OCP in concert with collagen matrix.
It was apparent that the attachment and proliferation of ST-2 cells were inhibited on coatings of OCP with increasing OCP concentration, whereas they were restored when OCP was combined with collagen. The previous study showed that the proliferation of rat bone marrow stromal cells on three-dimensional OCP crystal assemblies, in the absence of collagen, was compatible with that of the control culture plate even in the presence of osteogenic medium. 18 On the contrary, it has been shown that the surface area of the OCP crystal assemblies affected the proliferation of bone marrow stromal cells, although OCP consisted of a mixture of OCP and HA as a second crystalline phase. 19 Another study showed that the proliferation of ST-2 cells or mouse calvaria primary osteoblastic cells on an OCP coating was inhibited in the early stage of culture but became compatible at a later stage, at which point OCP tended to be converted to an apatitic crystalline phase. 17 Studies of the physicochemical reactions of OCP showed that phosphate ion release and calcium ion uptake under physiological conditions16,28 and in culture media 20 accompanies the process of conversion from OCP to HA. It is widely accepted that calcium ions play an important role in cell adhesion29,30 and proliferation. 31 It has recently been found that phosphate ions play multiple roles in maintaining osteoblast-like cells. 32 Previous studies have revealed that phosphate ions can diffuse in collagen membranes. 33 Collagen is known to promote specific cell interactions, such as cell-recognition signals and cell adhesion.34,35 In the current study, FTIR analysis confirmed that OCP tended to convert to HA regardless of the presence of collagen in the culture medium. It seems likely that calcium and phosphate ions derived from OCP affect osteoblastic cell attachment and proliferation on OCP/collagen in vitro.
Synthetic OCP has also been shown to convert to apatite when implanted in various sites, including muscle pouches, 36 subperiosteal region of calvaria,12,13 and subcutaneous regions in mice 13 and critical-sized calvarial bone defects 17 in rats. This was the same bone defect as analyzed in the present study. OCP can be converted into HA in simulated body fluid. 37 The conversion from OCP to HA is faster in the presence of collagen. 38 It is well accepted that osteoconductivity of bone substitute materials could be acquired by forming bone-like apatite on their material surfaces. 39 This may explain that the observed enhancement of bone regeneration with increasing OCP content within collagen is induced by the formation of bone-like apatite through OCP-HA conversion. However, a comparative study using synthetic OCP and bone-like apatite (obtained via OCP by hydrolysis) suggested that a process of OCP-HA conversion itself stimulates bone formation. 17 Synthetic OCP can be topotaxially converted to HA when implanted in the subperiosteal region of mouse calvaria while retaining its original plate-like morphology, suggesting that OCP may provide a scaffold to host osteoblastic cell attachment and proliferation because of the suitable solubility in OCP as a bone regenerative material. 28 Enhanced bone formation has also been reported on the OCP-coated surface of a titanium implant, which accompanied the partial dissolution of OCP and conversion into carbonate apatite. 11 Such a stimulatory capacity of OCP should contribute to the enhanced bone regeneration observed in the present OCP/collagen.
OCP is brittle in nature and cannot be molded using sintering processes used for HA and β-TCP ceramics because of the dehydration of water molecules in the hydrated layer of the OCP structure.24,25 Combining OCP with a collagen matrix allowed OCP to be molded without losing the osteoconductivity of OCP,21,27 as observed in HA/collagen 40 and β-TCP/collagen composites. 41 The present study demonstrated that greater OCP content in the collagen matrix enhances bone regeneration in a dose-dependent manner. The inclusion of 83% OCP within collagen attained approximately 64% of bone regeneration in critical sized-defects of rat calvaria after 12 weeks. The optimized combination of OCP and collagen may lead to the development of bone substitute materials compatible with autogenous bone.
Conclusion
The present study demonstrated that bone regeneration using a composite of OCP and collagen was significantly facilitated in an OCP dose–dependent manner in a collagen matrix. The results suggest that the intrinsic bone regenerative properties of OCP can display the osteoconductive characteristics of OCP/collagen and that the highest content of OCP (83% OCP) was the best candidate for substituting autogenous bone grafts. Because OCP is thought to be a precursor of biological apatite crystals in bones and teeth, studies of the mechanism of bone formation using synthetic OCP implantation may lead to the elucidation of the mechanism of biomineralization during bone formation, in addition to the understanding of OCP as a bone substitute material in the field of orthopedic and oral surgery.
Footnotes
Acknowledgments
This study was supported in part by Grants in Aid (17076001, 19390490, 19750134, 20659304) from the Ministry of Education, Science, Sports and Culture of Japan.