
Abstract
Transplantation of embryonic stem cells (ESCs) can improve cardiac function in treatment of myocardial infarction. The low rate of cell retention and survival within the ischemic tissues makes the application of cell transplantation techniques difficult. In this study, we used a temperature-responsive chitosan hydrogel (as scaffold) combined with ESCs to maintain viable cells in the infarcted tissue. Temperature-responsive chitosan hydrogel was prepared and injected into the infarcted heart wall of rat infarction models alone or together with mouse ESCs. The result showed that the 24-h cell retention and 4 week graft size of both groups was significantly greater than with a phosphate buffered saline control. After 4 weeks of implantation, heart function, wall thickness, and microvessel densities within the infarct area improved in the chitosan + ESC, chitosan, and ESC group more than the PBS control. Of the three groups, the chitosan + ESC performed best. Results of this study indicate that temperature-responsive chitosan hydrogel is an injectable scaffold that can be used to deliver stem cells to infarcted myocardium. It can also increase cell retention and graft size. Cardiac function is well preserved, too.
Introduction
Despite this progress in cell transplantation, unsatisfactory cell retention and transplant survival plague this technique.17–20 It is reported that, when delivered to the heart through a needle, approximately 90% of cells are lost to the circulation or leak out of the injection site. 21 In the cells that successfully enter the heart, almost 90% die within the first week.17,18 The basic protocol for cell grafting may need further optimization to avoid cell loss. 20
The emerging field of tissue engineering may offer promising alternatives. Tissue-engineering approaches are designed to repair lost or damaged tissues using cellular transplantation and biomaterial scaffolds. Strategies of cardiac tissue engineering can be classified as the construction of a cardiac patch and the engineering of injectable cardiac tissues. In the former approach, cells are seeded in a polymer scaffold to construct a patch in vitro before being implanted into an infarcted heart.21,22 However, this approach fails to deliver viable cells into the infarct wall. Moreover, lacking vascularization, these cultured implants are not thick enough to produce an optimal outcome. The latter approach uses an injectable biopolymeric scaffold to deliver cells directly into the infarct wall, which is a novel approach developed in recent years for heart repairs. The injectable scaffolds used include fibrin glue,23–25 matrigel, 26 and self-assembling peptides. 27 Notwithstanding that fibrin glue can improve cell survival and preserve cardiac function and wall thickness after acute ischemic myocardial injury, its degradation time in vivo is too short to support long-term secretion of extracellular matrix. Matrigel-based liquid can restore injured myocardium without distorting its geometry, but it remains unpopulated and nonvascularized in vivo. The self-assembling peptides can create microenvironments to promote vascular cell recruitment, but there is no report on their use as an injectable scaffold for MI treatment.
Chitosan is a biocompatible and biodegradable cationic polymer. Being a linear polysaccharide, it is composed of glucosamine and N-acetyl glucosamine units linked by β (1–4) glycosidic bonds. Its final degradation products are biocompatible chitosan oligosaccharides of variable length. As an ideal scaffold, chitosan has been widely used in the tissue engineering of skin, bone, cartilage, liver, nerve, and blood vessel in the past 25 years. 28 Derivatives of chitosan vary, with different applications in tissue engineering, such as porous structures, 29 chitosan-based nanofibrous structures, 30 and chitosan hydrogel.31–34 The injectable chitosan hydrogel has many advantages, Liquid gels are available to any space of a defect site, living cells and therapeutic agents could be incorporated in the hydrogel before injection, and the hydrogel can be injected into the site without surgery. Chitosan hydrogel responds to a variety of external stimuli such as light 31 and temperature.32–34 The temperature-responsive chitosan hydrogel has a wide array of applications. The temperature-responsive chitosan–glycerol phosphate (GP) hydrogels are attractive because bioactive factors (such as growth factors, genes, and supportive cells relevant for the repair and regeneration of the tissue) can be easily incorporated into the polymer solution. Once exposed to body temperature, the polymer solution can polymerize rapidly in situ within a short time, trapping and aiding in the retention of these factors within the injected area. This ability for in situ gelation makes chitosan a useful scaffold of injectable biological materials. The degree of deacetylation is the key factor in controlling the degradation rate. It can be adjusted to optimize the degradation rate to match the growth rate of tissue. 34 The biocompatibility of chitosan has been investigated in many cell types. Chitosan has been used in cartilage and bone tissue engineering.35,36 Until now, there has been no report about its use as carrier to deliver ESCs for the treatment of MI.
In this study, temperature-responsive chitosan hydrogel was used as an injectable scaffold to improve implanted ESC retention and survival within the ischemic myocardium. We evaluated the effect of the engineered grafts in improving cardiac cell survival and regeneration using histopathology and immunohistochemical staining for cell development and echocardiography for cardiac function.
Methods
Cell culture
The mouse ES-D3 cell line was maintained on mitotic inactive mouse embryonic fibroblast feeder cells. The ESCs culture medium was Dulbecco's modified Eagle medium (DMEM; Invitrogen, Carlsbad, CA) containing 15% bovine serum albumin (BSA; Hyclone, Logan, UT), 0.1 mM β-mercaptoethanol (Sigma, St. Louis, MO), 2 mM L-glutamine (Chemicon, Temecula, CA), 1% non-essential amino acids (Chemicon), and 103 units/mL of leukemia inhibitory factor (Chemicon).
For the determination of cell retention after 24 h of implantation, mouse ESCs (mESCs) were labeled with PKH26 fluorescent cell linker dyes (Sigma) after cell culture before injection. For the identification of mESCs after 4 weeks of implantation, mESCs were labeled with 4',6-diamidino-2-phenylindole (DAPI; Sigma) before injection.
Preparation of temperature-responsive chitosan hydrogel
The temperature-responsive chitosan hydrogel was prepared according to Hoemann CD et al. 37 Briefly, Chitosan (200 mg) (Oslo, Norway, Product No. UP CL 113, 84% degree of deacetylation, 16% hydrochloric acid) was dissolved in 10 mL of distilled water to obtain a 2% chitosan solution and sterilized using regular liquid autoclaving. Then 1.15 g of β-GP (Sigma) was dissolved in 10 mL of distilled water to obtain 11.5% β-GP solution and filter sterilized. Temperature-responsive chitosan hydrogel was formed by mixing 8 mL of chitosan and 2 mL of GP solution with 2.5 mL of 2.5% (w/v in DMEM) filter-sterilized hydroxyethyl cellulose (Fluka, St. Louis, MO) and incubating at 37°C.
Culture of ESCs in temperature-responsive chitosan hydrogel in vitro
ESCs were suspended in chitosan–GP solution at an initial concentration of 107 cells/mL, and the hydroxyethyl cellulose was added and mixed quickly. The mixture was poured into 24-well plates and allowed to gel at 37°C. After solidification, ESC culture medium (DMEM containing 15% BSA, 0.1 mM β-mercaptoethanol, 2 mM L-glutamine, and 1% non-essential amino acids) was added and incubated at 37°C in a humidified 5% carbon dioxide incubator. Cell viability in the hydrogel was assessed using acridine orange–propidium iodide (AO/PI) staining. Briefly, the stock solution (AO: 670 μmol/L, PI: 750 μmol/L) was prepared with Dulbecco's solution and kept in the dark at 4°C. Just before using, 0.01 mL of AO and 1.0 mL of PI were mixed, diluted 10 times with Dulbecco's solution, and passed through a 0.22-μm filter membrane. The hydrogels containing ESCs were incubated with AO/PI mixture for 10 min and observed under a fluorescence microscope. Live cells were stained in green (AO) and dead cells in red (PI).
MI model
Female Sprague-Dawley (SD) rats were purchased from the Experimental Animal Center, Academy of Military Medical Science (Beijing, PRC). The Institutional Animal Care and Use Committee (IACUC) of the Chinese Academy of Military Medical Science, Beijing, China, approved all experiments in this study. Every effort was made to minimize animal suffering and the number of animals used. Animals were individually housed in cages maintained at a temperature of 24 ± 2°C with a normal day–night cycle with free access to water and food.
An ischemia model described by Miyahara1 was used in this study. 38 Briefly, female SD rats were anesthetized with sodium pentobarbital (30 mg/kg, intraperitoneal.); limb-lead electrocardiography was performed, and the animals were then incubated and ventilated using a volume-regulated respirator for the entire length in the procedure. The surgical approach involved a left lateral thoracotomy, pericardectomy, and identification of the left anterior descending coronary artery for ligation. The left coronary artery was ligated with a 6-0 Prolene suture 2 to 3 mm from its origin between the pulmonary artery conus and the left atrium. After that, the infarcted area of the left ventricle (LV) paled immediately and beat weakly, and the electrocardiography showed typical MI waves. Then the chest was closed. Using this method, there is 25% to 35% mortality within the first 24 h after occlusion. Surviving rats were maintained on standard rat chow and water ad libitum. The laboratory has done extensive experiments with this model, and the histological observation showed that this technique resulted in an acute infarct size of approximately 40% to 60% of the LV.25,38
Injection surgeries
Injection surgeries were performed 1 week after MI. Rats were anesthetized with sodium pentobarbital (30 mg/kg) the second time, and the hearts were exposed for injection. Concomitantly, 1 × 107 mESCs suspended in 100 μL if PBS (n = 20; half for 24-h cell retention observation) or in temperature-responsive chitosan solution (n = 20, half for 24-h cell retention observation) were injected along the border zone of the infarcted area at three different locations (below the left atrium, in the middle portion of the LV, and at the apex) using a 28 gauge needle. PBS only (n = 10) or chitosan only (n = 10) without cells were also injected as control groups. The ischemic area was identified according to a darker region of the LV with a weak heart beat. Injections were made at an angle so as not to inject into the lumen of the LV. Injections were verified according to a slight lightening in color of the myocardium as the solutions entered the infarct wall.
Four weeks later, animals were anesthetized with sodium pentobarbital (30 mg/kg) for function detection with echocardiography (14.0 MHz, Sequoia 512; Acuson, München, Germany). Parasternal short axis views with M-mode were acquired at the ventricular base immediately distal to the mitral valve. LV end-systolic diameter (ESD) and LV end-diastolic diameter (EDD) were measured, and LV fractional shortening (FS) and LV ejection fraction (EF) were calculated as follows: FS (%) = [(EDD–ESD)/EDD] × 100; EF (%) =[(EDD3–ESD3)/EDD3] × 100. The animals were euthanized after functional measurements using an overdose of sodium pentobarbital in compliance with the above guidelines.
Histopathology
The hearts were rapidly excised and freshly frozen in optimal cutting temperature freezing medium. We stained sections (5 μm) with hematoxylin and eosin (HE) and Masson trichrome.
Five sections, equally distributed through the infarct area, were taken from each heart as representative samples and measured for the presence of PKH26-labeled transplanted cells in 24-h post-injection hearts. To measure cell retention within the myocardium, the area covered by the PKH26-labeled mESCs was traced using a fluorescent microscope (Olympus BX51, Olympus, Tokyo, Japan). The area covered by PKH26-labeled cells was measured by using RS Image Pro (version 4.5; Media Cybernetics, Inc., Trenton, NJ). Cell retention was reported as a percentage of PKH26-labeling area in infarct area.
The fraction of the LV that was infarcted and infarct size in 4-week injection hearts was calculated according to Pfeffer et al. 39 The fraction of the LV that was infarcted was calculated from photographs of gross heart slices by measuring the length of the infarcted endocardial circumference and the entire endocardial circumference. Infarct size was reported as percentage of length of the infarcted endocardial circumference in the length of the entire endocardial circumference. All HE-stained sections also were examined for possible evidence of an immune reaction.
Immunofluorescent and immunohistochemical staining
Immunofluorescent and immunohistochemical staining were performed to identify myocardium, ESC-derived cardiomyocytes, and blood vessels using sarcomeric actin, cardiac troponin T (cTnT), and factor VIII-related antigen antibody, respectively.
Cryosections were fixed with acetone, and endogenous peroxide activity was quenched with 3% hydrogen peroxide. After being blocked with 2% normal goat serum, sections were incubated with the primary antibodies diluted to working solutions (sarcomeric actin, 1:200, Sigma; cTnT, 1:200, Sigma; factor VIII–related antigen, 1:200, Zymed, South San Francisco, California) at 4°C overnight. For immunofluorescence, Cy3-conjugated immunoglobulin G (1:100, Sigma) were added and incubated for 1 h at room temperature before being observed under an Olympus FV1000S confocal laser microscope. For immunohistochemical staining, sections were incubated with peroxidase-conjugated streptavidin and stained with diaminbenzidine (DAB).
Graft size in the specimens after 4 weeks of implantation was determined according to a procedure described by Christman. 22 The area covered by DAPI-labeled cells was measured using RS Image Pro. Graft size was reported as percentage of DAPI-labeled area in infarct area.
The density of microvessels was determined in the sections immunohistochemically stained with factor VIII–related antigen antibody. Microvessels in each section were quantified using the following criteria: positive for vessel endothelium labeling, within the infarct scar, having a visible lumen, and having a diameter between 10 and 100 μm.
Statistical analysis
Cell retention data was compared using the Student t test. Analysis of variance and Tukey's multiple comparison tests were used to analyze the data about cardiac function, wall thickness, infarct size, and vessel density. Statistical analyses were performed with SPSS 11.0 (SPSS, Inc., Chicago, IL). Significance was accepted at p < 0.05. Results are reported as means ± standard deviations.
Results
Ninety rats were used in this study; 28 died during or immediately after the infarct surgery, and two rats died during the injection surgery (cells in the chitosan group). After the injection surgery, there was 100% survival in all groups.
In vitro survival of ESCs in temperature-responsive chitosan
The temperature-responsive chitosan hydrogel we prepared is in a liquid state at 4°C. It becomes more and more viscous with increasing temperature. When the temperature reaches 37°C, it turns into a solid within 10 to 15 min.
ESCs survived well in the chitosan hydrogel. After 24 h of culture, ESCs proliferated and aggregated. The AO/PI staining (Fig. 1) showed that cell death rarely occurs owing to the hydrogel.
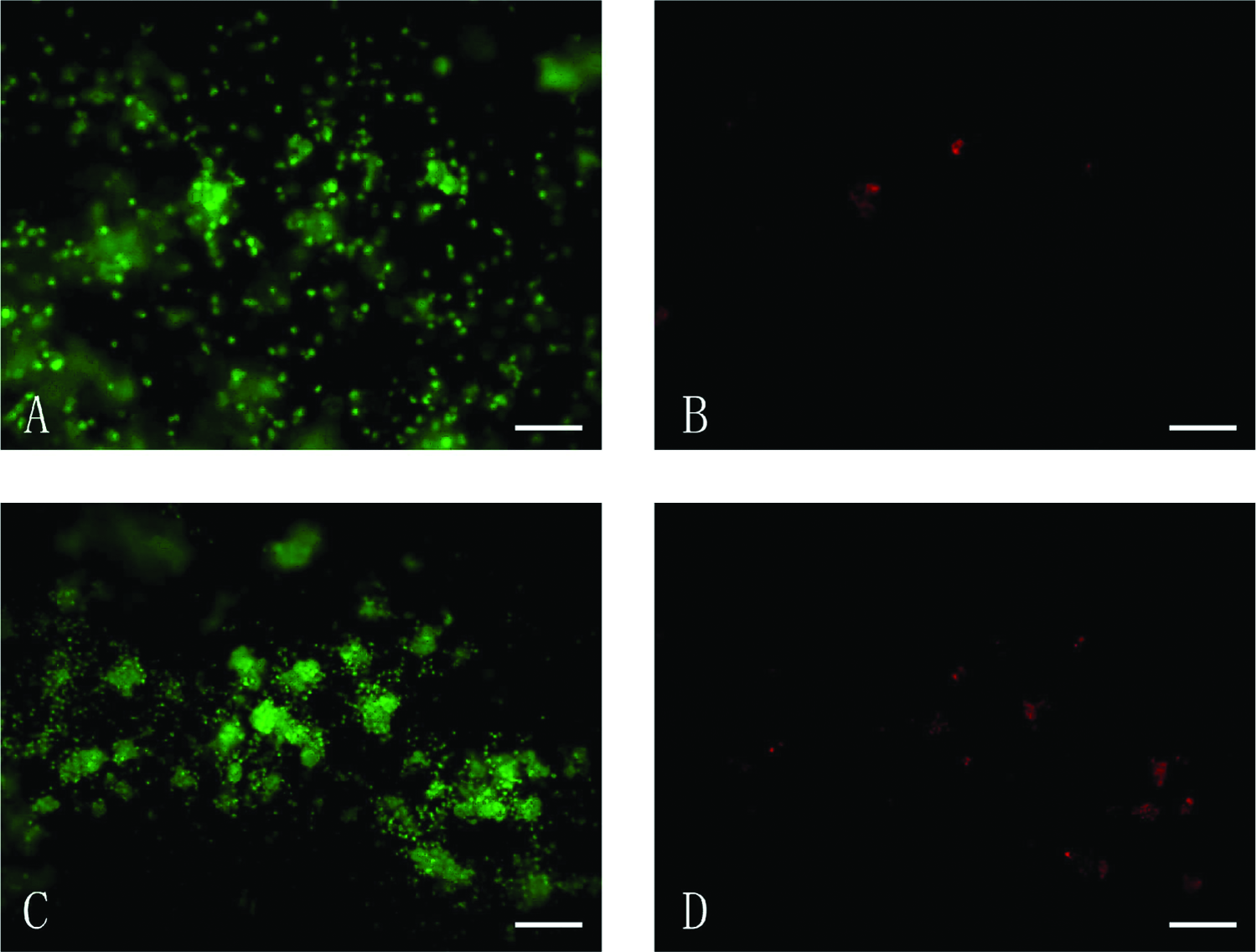
Acridine orange and propidium iodide staining of mouse embryonic stem cells (mESCs) seeded in chitosan hydrogel after solidification (
Cell retention and graft size
Twenty-four h after injection, mESCs injected in PBS only covered 9.91 ± 1.80% of the infarct area (Fig. 2A), whereas mESCs injected in chitosan covered 17.48 ± 3.30% (Fig. 2B) (p < 0.01).
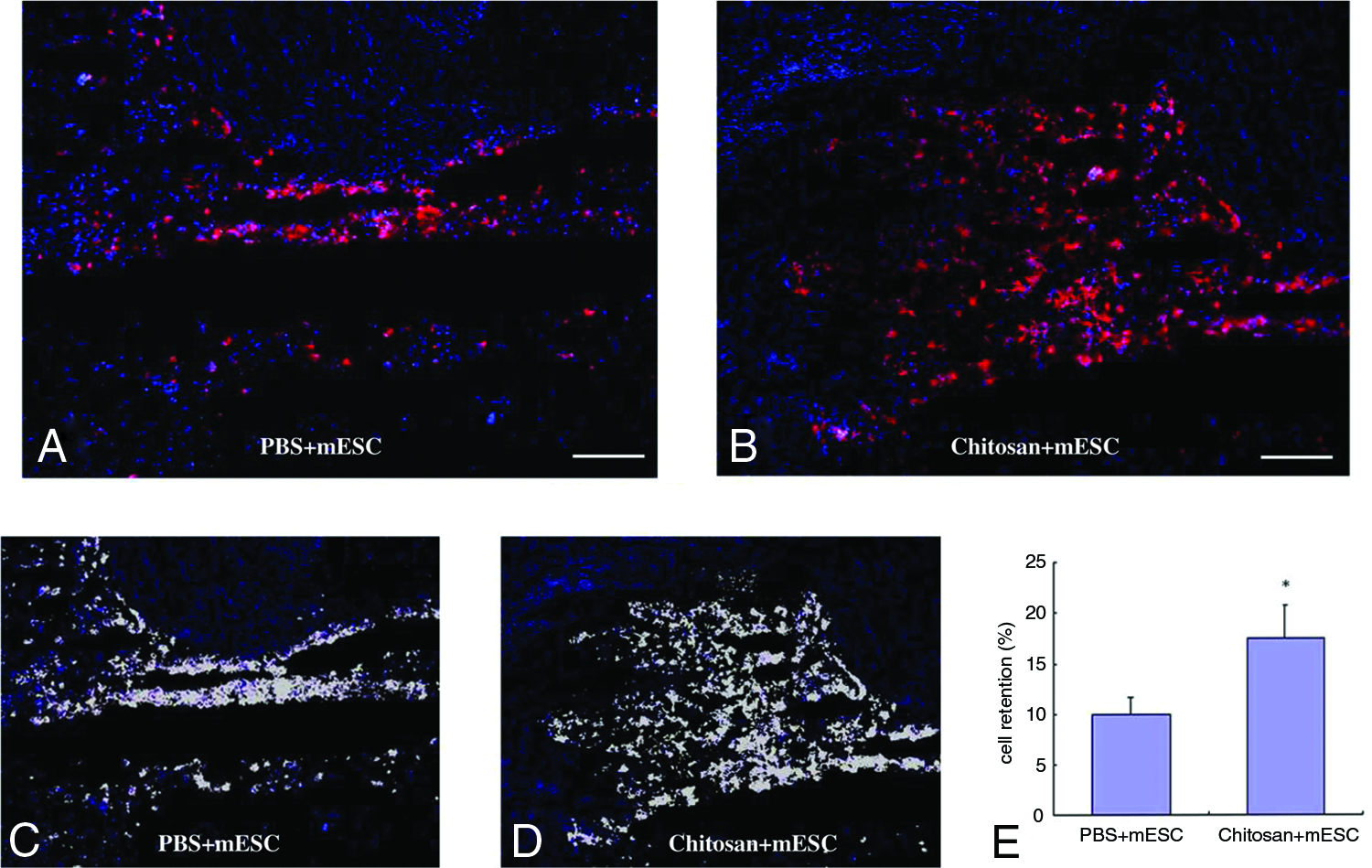
Distribution of PKH26-labeled mouse embryonic stem cells (mESCs) in infarct area 24 h after injection. Red fluorescence showed PKH26-labeled mESCs injected in phosphate buffered saline (PBS) (
After 4 weeks of implantation, when the cells were injected with chitosan, the mESCs in the infarct area significantly outnumbered those injected with PBS (p < 0.01) (Fig. 3). Cells injected in chitosan covered 12.93 ± 1.90% (Fig. 3A) of the infarct area, compared with 6.41 ± 1.15% (Fig. 3B) when injected in PBS. These results indicated that the chitosan hydrogel increased cell retention and graft size in an ischemic heart. In contrast, transplanted mESCs injected in PBS were frequently found scattered in the infarct areas, whereas those injected in chitosan were mainly in aggregates.
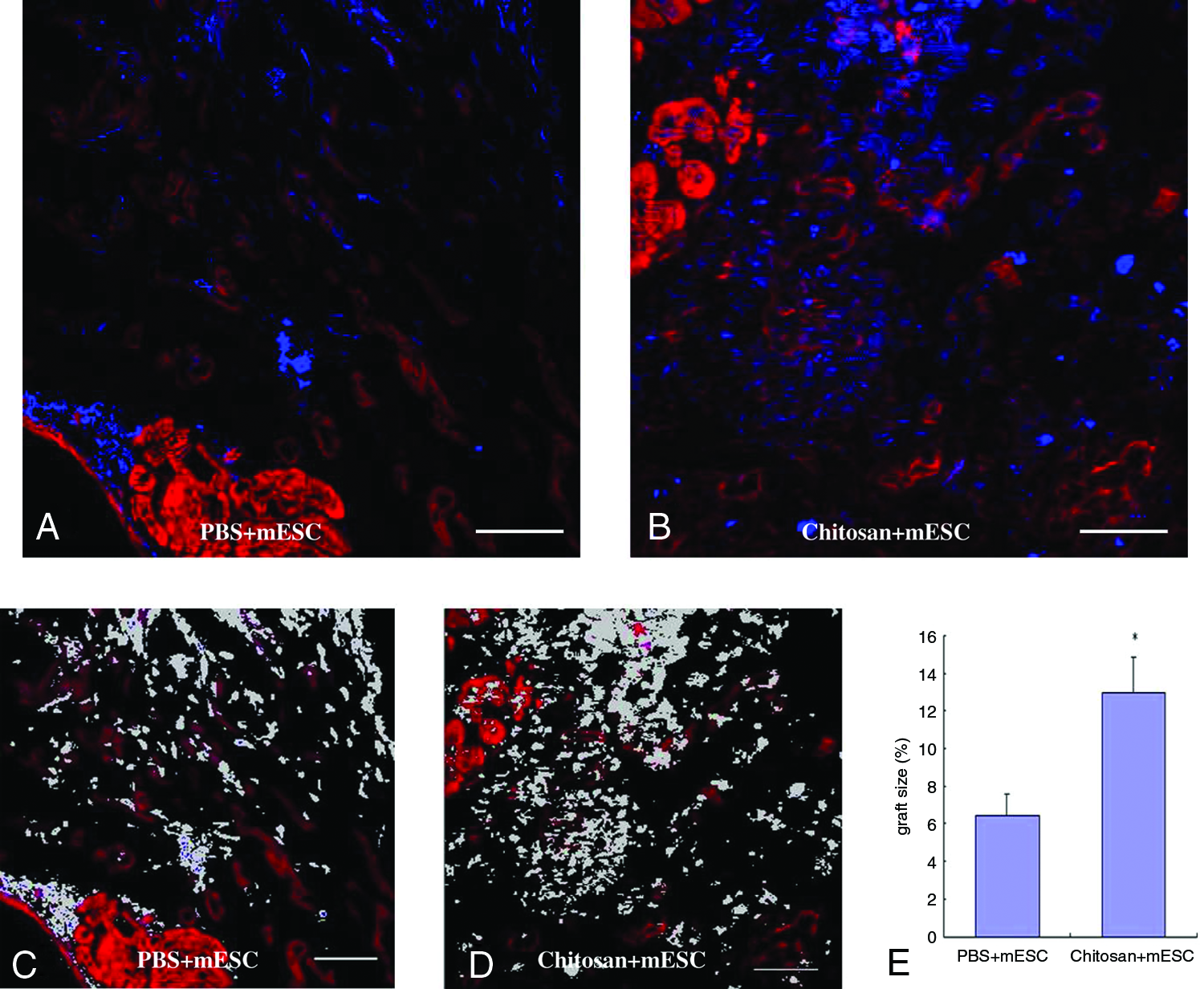
4',6-diamidino-2-phenylindole
Differentiation of mESC in infarcted heart
The cTnT immunofluorescence staining of DAPI-labeled mESCs after 4 weeks of transplantation showed that DAPI-positive and cTnT-positive cells existed in the infarct area (Fig. 4, white arrows). There were also some DAPI-positive but cTnT-negative (non-cardiac) graft cells in the infarct area (Fig. 4, yellow arrows).
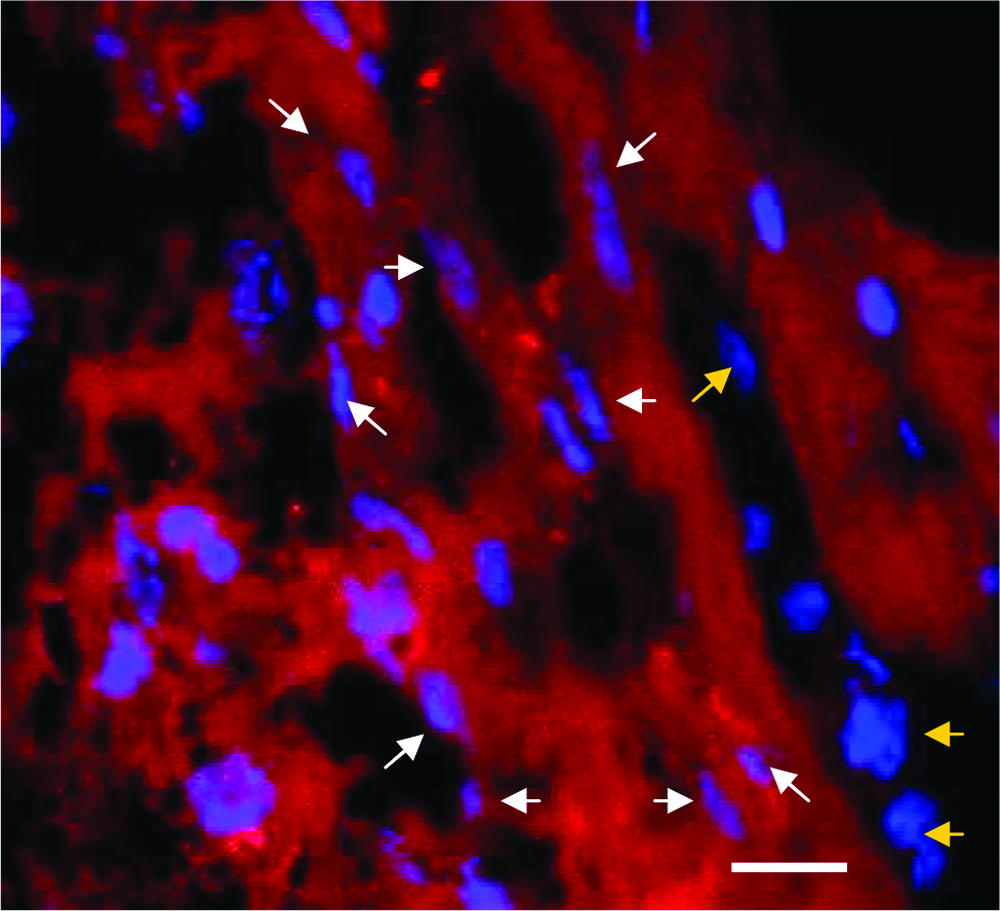
Differentiation of mouse embryonic stem cells (mESCs) in an infarcted heart. The cardiac troponin T (cTnT) immunofluorescence staining of 4',6-diamidino-2-phenylindole (DAPI)-labeled mESCs after 4 weeks of transplantation showed DAPI-positive and cTnT-positive cells in the infarct area (white arrows) and that there were also some DAPI-positive but cTnT-negative (non-cardiac) graft cells in the infarct area (yellow arrows). Bar = 50 μm. Color images available online at www.liebertonline.com/ten.
Cardiac function
Echocardiography revealed better heart function in the rats treated with chitosan only, PBS + mESC, and chitosan + mESC than the control (PBS only) in ESD (Fig. 5A), EDD (Fig. 5B), EF (Fig. 5C), and FS (Fig. 5D) (p < 0.01). The group treated with chitosan + mESCs also demonstrated a significantly higher heart function than the one receiving chitosan only and PBS + mESCs (p < 0.01) in ESD, EDD, EF, and FS. The group treated with chitosan only exhibited the same heart function as the one receiving PBS + mESCs (p > 0.05) in ESD, EDD, EF, and FS.
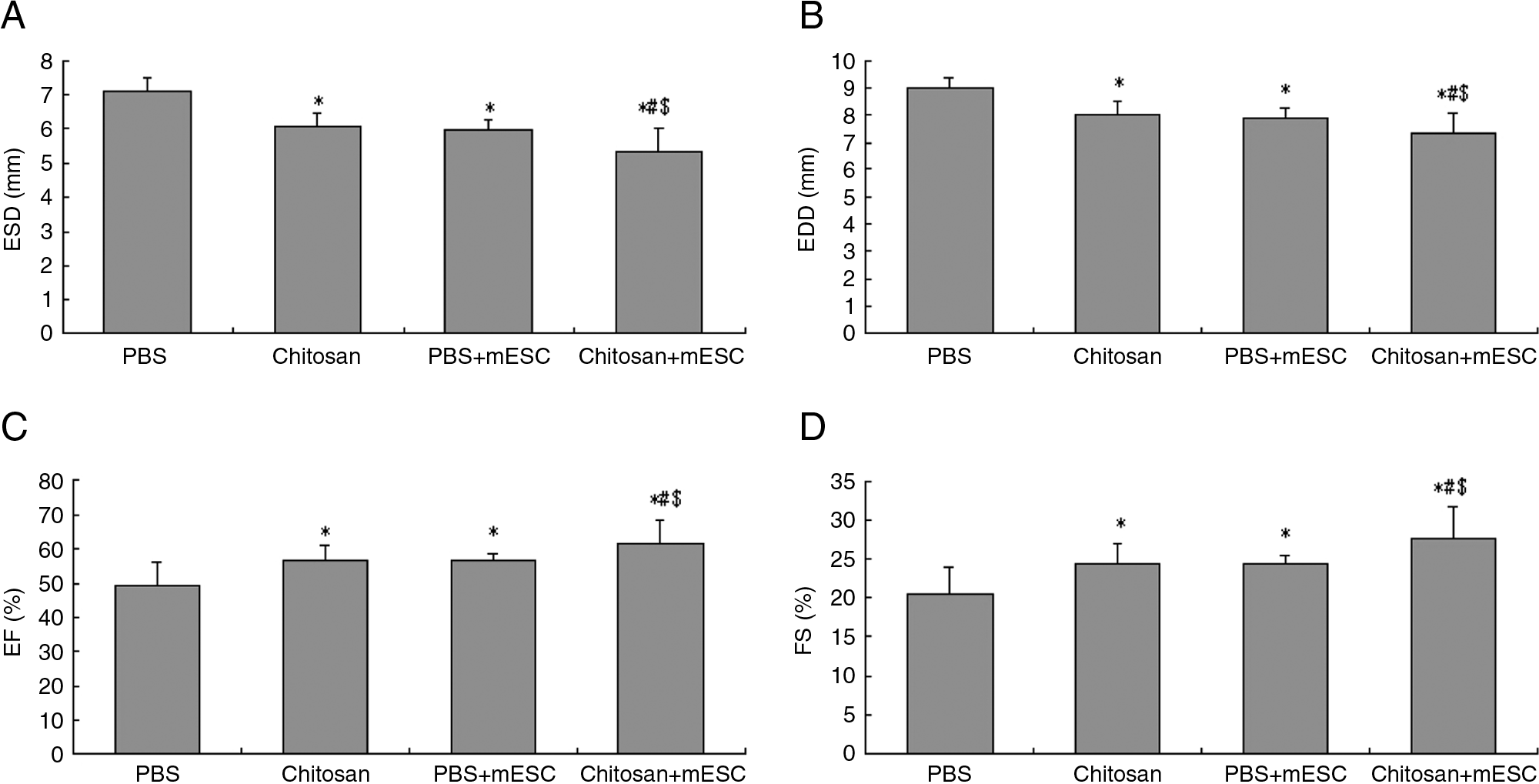
Echocardiography. (
Histopathology
Infarct area and wall thickness
The infarct size was 51.7 ± 2.3% of entire endocardial circumference in the PBS-only group (Fig. 6A), 33.1 ± 2.5% in the chitosan-only group (Fig. 6B). The infarct size was 35.9 ± 3.6% when mESCs were injected in PBS (Fig. 6C), and 22.9 ± 3.5% in chitosan hydrogel (Fig. 6D). These treatments all resulted in significantly smaller infarct sizes than in the PBS control group (p < 0.01). The group treated with chitosan + mESCs also had a significantly smaller infarct size than the group with chitosan only and the group that received PBS + mESCs (p < 0.01). There was no significant difference between chitosan only and PBS + mESCs (p > 0.05) (Fig. 6E).
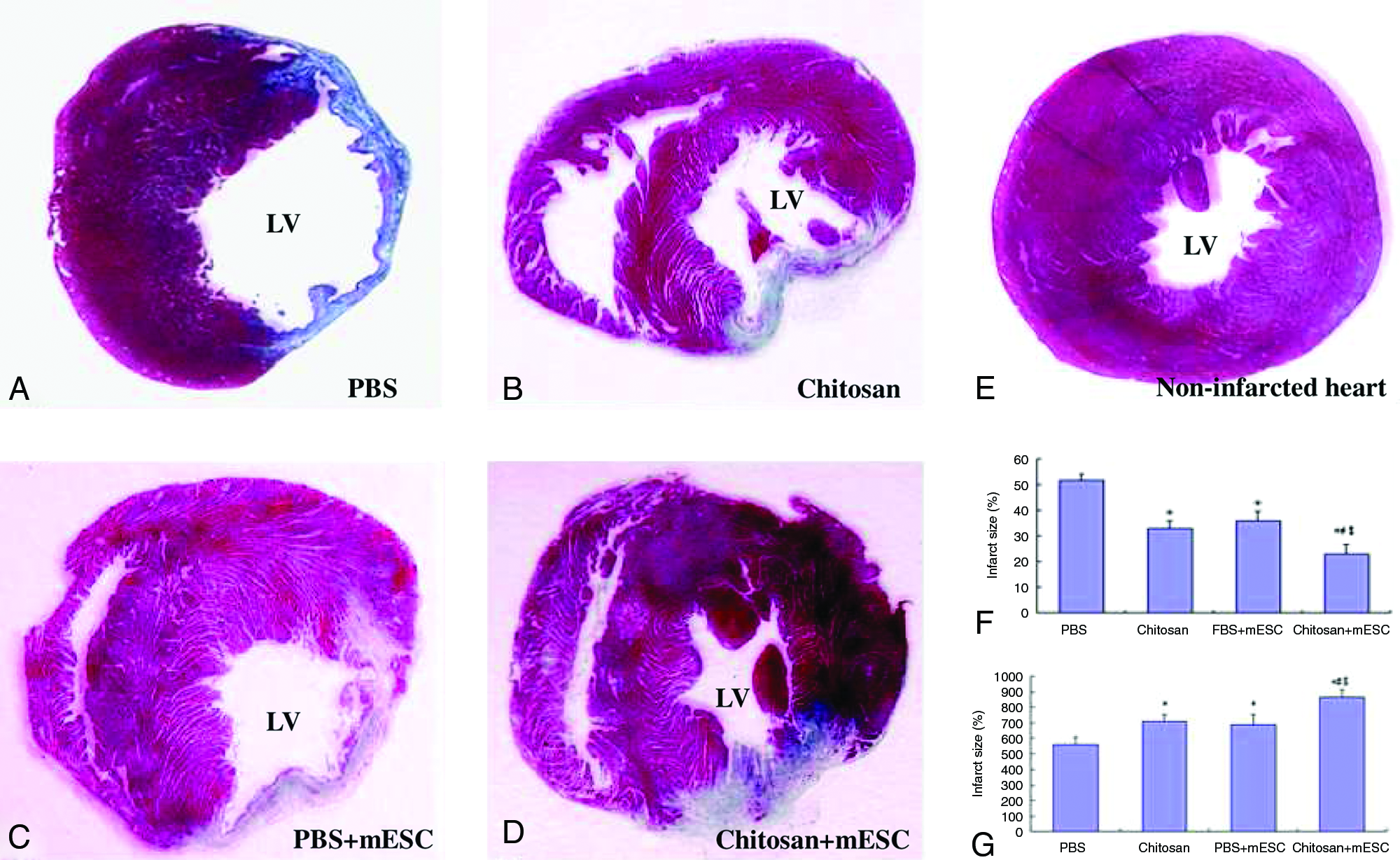
Infarct size and infarct wall thickness. (
The ventricular wall thickness in the central area of the MI after 4 weeks of implantation was as follows: 559.2 ± 44.4 μm in the PBS-only group, 705.1 ± 44.0 μm in the chitosan-only group, 687.6 ± 62.3 μm in the PBS + mESC group, and 861.4 ± 50.1 μm in the chitosan + mESC group. The thickness of the three experimental groups was all significantly higher than of the PBS-only group (p < 0.01, respectively). The group treated with chitosan + mESCs also preserved the thickness significantly compared with the group with chitosan only and the group that received PBS + mESCs (p < 0.01, respectively). There was no significant difference between the chitosan-only and PBS +mESC groups (p > 0.05) (Fig. 6G).
The degradation of chitosan in the infarcted heart
HE staining showed that there was a lot of chitosan in the infarct area after 24 h of transplantation (Fig. 7A), whereas there was little chitosan in the infarct area after 4 weeks of transplantation (Fig. 7B). The chitosan degraded completely after 6 weeks.
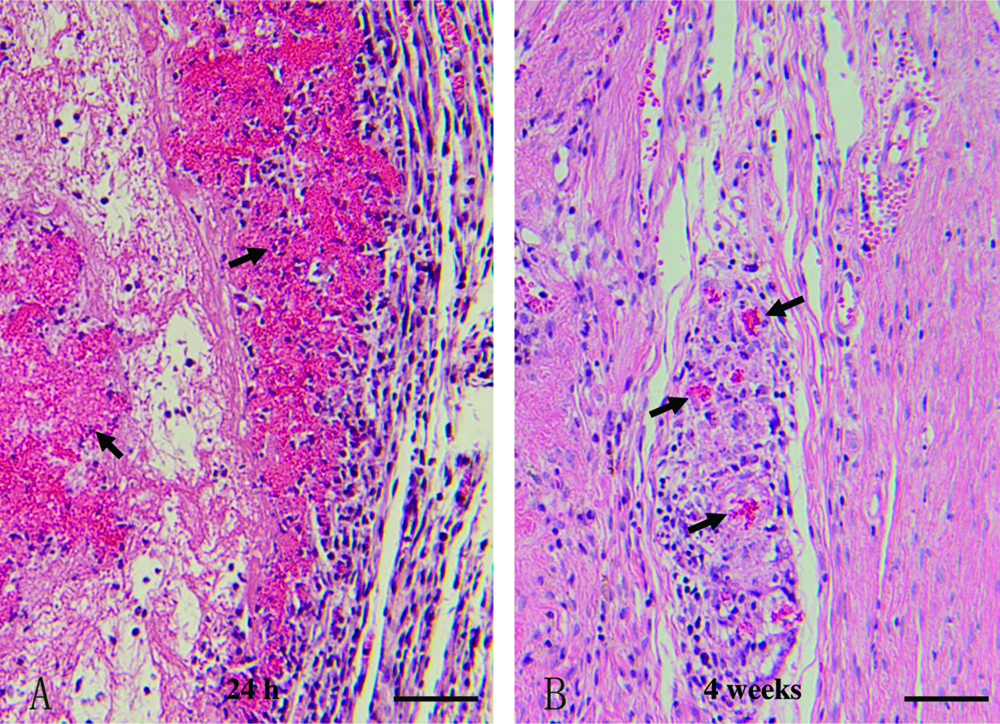
Degradation of chitosan in the infarcted heart. Hematoxylin and eosin staining showed that there was a lot of chitosan in the infarct area after 24 h of transplantation (
Neovasculature formation
Neovasculature formation potential was assessed in the sections immunohistochemically stained with factor VIII–related antigen. Because collateral arterioles are often observed bordering the scar after MI, we counted vessels within the infarct to assess the neovascular effect of the different treatments. The results showed that chitosan only (Fig. 8B), PBS + mESCs (Fig. 8C), and chitosan + mESCs (Fig. 8D) all resulted in better microvessel density in scar areas than PBS only (Fig. 8A) (p < 0.01). The microvessel density of the chitosan combined with mESCs was the highest (p < 0.01, respectively). There was no significant difference between the chitosan-only and PBS + mESC groups (p > 0.05) (Fig. 8E).
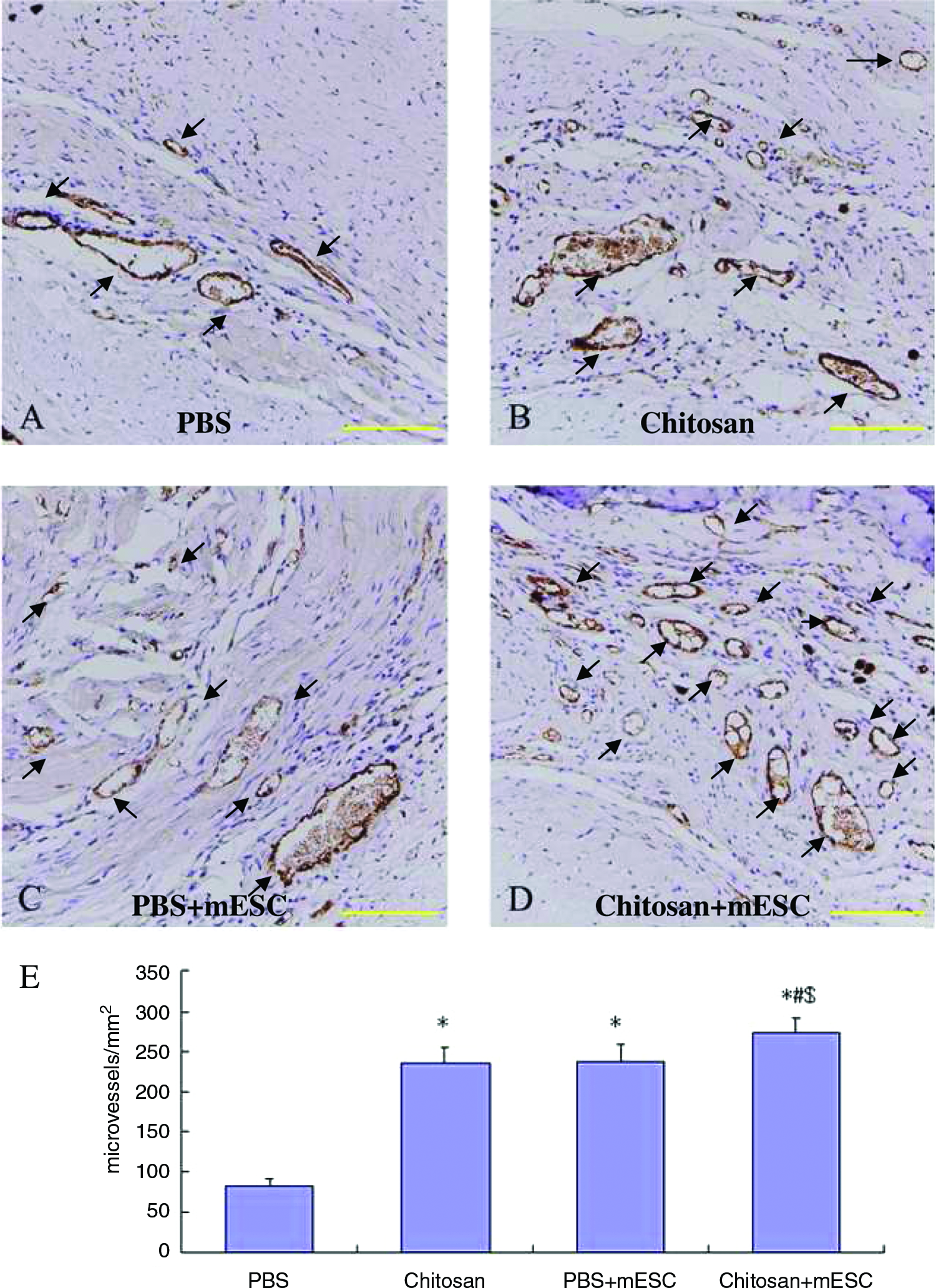
Microvessel density in the myocardial infarction sites 4 weeks after injection. (
Discussion
Low cell retention, cell death, and lack of modulate of proliferation after transplantation has frustrated cell transplantation therapy in the infarcted heart.17–20 Transplanting the cell with biomaterial is effective for improving such therapy. In this study, temperature-responsive chitosan hydrogel as a delivery scaffold for mESC transplantation facilitated cell retention. It also improved the microenvironment of the infarcted area, thus improving the heart function. Our findings showed that 24-h cell retention and 4-week graft size was significantly better with chitosan hydrogel than with using PBS control. The 24-h retention of the chitosan hydrogel group was 17.48 ± 3.30%, whereas that of the PBS group was 9.91 ± 1.80%. Heart function, wall thickness, and microvessel density within the infarct area after 4 weeks of implantation was better in the chitosan + mESC group than in the other three groups. These results suggest that the temperature-responsive chitosan hydrogel is a promising vehicle to deliver ESCs to infarcted heart wall.
ESCs have many potential advantages over other cell types for cardiac repair. They have a high capacity for self-renewal and an ability to differentiate into functional cardiomyocytes in vitro.10,11,14 Such grafts could integrate with the host myocardium electromechanically. So ESC transplantation has emerged as a new approach for repairing damaged myocardium in recent years. Our data show that there were 12.93 ± 1.90% transplanted ESCs in the infarct heart 4 weeks after transplantation. We have also identified the cTnT-positive cells that were derived from the ESCs in the infarcted heart. Heart function, wall thickness, and microvessel density within the infarcted area 4 weeks after implantation was greater in the ESC-only group than in the PBS group. Our results demonstrate that undifferentiated mESCs can be differentiated to a cardiac lineage under the local environmental of an infarcted heart. The injection of mESCs contributed to the recovery of infarcted heart function.
In this study, we evaluated the potential of temperature-responsive chitosan hydrogel as an injectable scaffold for the delivery of ESCs to the infarcted myocardium. Chitosan varies in its form for broad application.32–37 There has been no report of its application in cardiac cell therapy until now. Herein, we formulated chitosan with two other ingredients to form a temperature-responsive chitosan hydrogel that would turn into a solid within 10 to 15 min at 37°C. Biocompatibility was determined in cardiomyocytes (data not shown) and ESCs. Because minimal cytotoxicity was seen in cell cultures with chitosan solutions, it evidenced the good biocompatibility of temperature-responsive chitosan hydrogel. It is consistent with the cytotoxicity evaluation of other forms of chitosan. 40 The degradation time of temperature-responsive chitosan hydrogel in myocardium is 4 to 6 weeks. It is more suitable for the implanted cells to generate new tissues and secrete their own matrix. Moreover, because of the longer degradation time of chitosan hydrogel in vivo, bioactive factors can be incorporated to regulate further proliferation and differentiation after implantation. Therefore, temperature-responsive chitosan hydrogel is a promising delivery vehicle for ESCs to infarcted heart wall. Our data showed that chitosan alone could improve infarcted heart function. The following mechanism accounts for this. Chitosan-induced neovasculature formation in ischemic myocardium resulted in a better microenvironment. Chitosan can provide a three-dimensional space for the migration of cells around an ischemic myocardium, such as cardiocytes, endothelial cells, and stem cells. Chitosan can support the ventricular wall to a certain extent.
The microenvironment is pivotal to the viability and function of transplanted cells. Our results showed that the injection of chitosan alone or together with ESCs increased the microvessel density significantly within the infarct scar. An increase in blood supply would provide a more favorable microenvironment for the cells to thrive. It has been previously reported that the injection of cells into vascularized myocardium resulted in better cell survival than injection into an ischemic myocardium. 18 Chitosan increased vessel density and therefore improved the living condition of transplanted cells. Then the improved living condition helped improve cardiac function. Chitosan-induced neovasculature formation had been found in the healing process of wounds. It was observed that the typical course of healing was the formation of normal granulation tissue, often with accelerated angiogenesis. 41 Chupa et al. indicated that chitosan materials could be used to modulate the proliferation of vascular cells in vitro and in vivo. 42 Ishishara suggested that chitosan could promote the migration of vascular endothelial cells directly to facilitate angiogenesis in the healing process of wounds. The attraction of small chitosan oligosaccharides particles might cause these kinds of migration.43,44 Angiogenesis induced by chitosan in an infarcted heart was found in our study for the first time. The mechanism needs further investigation.
The immunological rejection evoked by stem cell xenotransplantation is an important scientific issue. From the recent reports on the basic studies of ESC immunology or in vivo transplantation, it is still controversial whether ESC xenotransplantation evokes immunological rejection. Many ESC transplantation studies have demonstrated that ESCs could avoid being attacked by the immune system of the host and could survive in the MI model for a long time after implantation.45,46 Basic studies of ESC immunology have showed that lack of major histocompatibility complex expression might be a potential mechanism underlying the weak immune responses towards ESC. 47 However, there are other reports have also claimed that ESC transplantation may evoke a strong immunological rejection. 48 In our study, we observed surviving ESCs after 4 weeks of transplantation, and heart function improved significantly in the group co-injected with chitosan hydrogel and ESCs, which confirmed the contribution of transplanted ESCs. These results indicated that the immunological rejection was at least not strong enough to result in a high mortality rate of the transplanted ESC within 4 weeks. However, the xenotransplantation model has its own limitations and cannot predict the response of allogeneic or isogenic transplantation. The DAPI tracing also need to be revised, with a more-advanced tracing system to make a conclusion. Therefore, this study did not attempt to end the controversy about the immunological rejection of ESC xenotransplantation but focused on the capability of chitosan to carry ESCs to an infarcted heart for repair.
In summary, the results of this study indicate that temperature-responsive chitosan hydrogel is a potential injectable scaffold that can be used to deliver stem cells to an infarcted myocardium. It can increase cell retention and microvascular density and preserve cardiac function after MI.
Footnotes
Acknowledgments
This work was supported by National High Technology Research and Development Program of China (2006AA02A105), Nature Science Foundation of China (30530220), and Beijing Nature Science Foundation of China (7062053). We thank S. Liu for technical assistance in histological preparation and staining.
Disclosure Statement
No competing financial interests exist.