
Abstract
Tissue reactions against poly-L-lactic acid (PLLA) in engineered cartilage may influence the size or maturity of regenerative tissue. To understand the biological events in these reactions, we subcutaneously transplanted engineered constructs of PLLA scaffolds with or without human chondrocytes or atelocollagen in nude mice and evaluated neovascularization and macrophage activation, which can be assessed even in nude mice. Although not showing cartilage regeneration, PLLA alone demonstrated dense localization of macrophages and blood vessels, as well as a high level of interleukin-1 beta and tissue hemoglobin at 2 and 8 weeks. Otherwise, constructs with PLLA and chondrocytes with or without atelocollagen (PLLA/cell/gel or PLLA/cell) formed mature cartilage by 8 weeks, which was more prominent in PLLA/cell/gel. Although accumulation of macrophages and blood vessels in PLLA/cell/gel and PLLA/cell was comparable with that in PLLA at 2 weeks, that in PLLA/cell/gel markedly decreased by 8 weeks, with blood vessels and macrophages excluded into non-cartilage areas. Macrophage migration inhibitory factor could be involved in these suppressed tissue reactions, because it was expressed in chondrocytes of engineered cartilage. Intense tissue reactions inevitably occurred in biopolymers alone, but it is possible that maturation of engineered cartilage suppressed these reactions, which may contribute to circumventing deformity or malformation of engineered tissues.
Introduction
Recently, several studies have attempted to use PLLA as a scaffold for tissue engineering.5–10 The requirements for scaffolds of engineered tissues are to provide a nano- and micro-structure and to have the ability to retain the embedded cells efficiently with their viability sustained. Because the biodegradable polymers are not only biocompatible, but also easily processed into any desired structure, scaffolds composed of these polymers would meet the requirements mentioned above, being promising candidates as the scaffolds of engineered tissues.
Research on cartilage regenerative medicine is more advanced than that on other tissues. Some protocols have already been applied in clinical settings.11–13 Brittberg et al. 11 performed autologous chondrocyte transplantation on patients with deep cartilage defects in the knee as early as the 1990s. Another group implanted autologous chondrocytes together with serum into a subcutaneous pocket for nasal augmentation and repair. 13 Because these approaches have used chondrocytes suspended in solution or gel, the engineered cartilage produced using these approaches might have limitations in shape or size. To build satisfactory cartilage constructs with proper morphology and hardness, it would be efficient to use a rigid biodegradable scaffold that does not soften even in a humid environment. Because no scaffold with such properties has been applied in clinical settings, we used PLLA, which has enough rigidity and a long history of safe use as a medical material. PLLA is sufficiently rigid for scaffolds and therefore could be advantageous in obtaining the required shape and hardness in engineered constructs. Regarding tissue reactions to PLLA, there was a report on the pathological findings of PLLA screws intraosseously implanted in a sheep model. 14 In that study, macrophages and multinucleated giant cells were shown to appear on the implant surface, followed by a reduction in the polymer mass 1 year after implantation. However, cartilage tissue is avascular and may function as a barrier against the monocyte–macrophage system. If the PLLA constituting engineered cartilage as a scaffold is embedded within cartilage tissue, it may evoke tissue reactions different from those observed when PLLA is intraosseously implanted. Although foreign body reactions caused by PLLA implantation are likely to be within the range of clinical acceptance, tissue reactions against the PLLA scaffolds in engineered constructs remain unknown. Potentially, severe tissue reactions could induce inflammatory cytokines such as interleukin-1 beta (IL-1β) and tumor necrosis factor alpha (TNF-α) and promote the actions of catabolic factors, resulting in deformity or malformation of engineered constructs. Because the lack of clear understanding of the actions of PLLA in engineered constructs hampers its clinical application, the tissue reaction in and around the engineered cartilage based on PLLA scaffolds should be clarified.
To that end, for the present study, we made engineered cartilage constructs consisting of human chondrocytes and PLLA scaffolds and transplanted them into nude mice to assess tissue reactions. We used human auricular chondrocytes instead of mouse chondrocytes, because a substantial number of homogeneous chondrocytes was required for the study, and better understanding of the biological actions of human cells would be beneficial in future clinical application. A mouse subcutaneous model was used as the experimental model for transplantation because of its simplicity. There are two main possible indications for cartilage regeneration: cartilage in the joint area and cartilage of the ear, nose, and trachea in the maxillofacial neck area. Thus, it would be necessary to examine tissue reactions of engineered cartilage in a joint model in addition to a subcutaneous model. However, tissue preparation for histological analysis in a joint model includes invasive processes such as decalcification, which might decrease immunogenic antigens in tissues, resulting in limited efficacy of the analysis of immunohistochemical staining. To avoid such potential inconvenience in a joint model, we used a subcutaneous model in which the experimental procedure was simple. We focused on investigating neovascularization and the participation of macrophages, which have been reported to play central roles in the course of absorption of PLLA screws.14,15 These reactions comprise early-phase inflammation, which can be observed even in nude mice with impaired T cell immune function. Thus, to elucidate the tissue reactions caused by PLLA in engineered cartilage, PLLA scaffolds containing human auricular chondrocytes were transplanted subcutaneously in nude mice, and neovascularization, activation of the macrophage system, and cytokine interactions in the engineered constructs were evaluated morphologically, histologically, and biochemically.
Materials and Methods
Chemicals and antibodies
Dulbecco's modified Eagle medium (DMEM), penicillin–streptomycin solution, and trypsin–ethylenediaminetetraacetic acid solution were purchased from Sigma Chemical Co. (St. Louis, MO). Bullet kit chondrocyte growth medium was obtained from Cambrex Bioscience (Walkersville, MD). Collagenase from Clostridium histolyticum and a hemoglobin assay kit were from Wako Pure Chemical Industries (Osaka, Japan). Other materials were 3% atelocollagen implant from KOKEN Co., Ltd. (Tokyo, Japan), PLLA porous scaffolds from KRI (Kyoto, Japan), anti-type II collagen antibody from LSL (Tokyo, Japan), anti-CD31 antibody (Mec 13.3) from BD Biosciences (San Jose, CA), anti-F4/80 antibody (Cl: A3-1) from BMA (Augst, Switzerland), and anti-macrophage migration inhibitory factor (MIF ) antibody (FL-115) from Santa Cruz Technologies (Santa Cruz, CA). Biotinylated secondary antibody, Vectastain Elite ABC dit, and peroxidase substrate kit diaminobenzidine were all obtained from Vector Laboratories (Burlingame, CA). A Quantikine murine IL-1β kit was bought from R&D Systems (Wiesbaden, Germany). Isogen (Nippongene, Tokyo, Japan), PrimeScript Reverse Transcriptase (Takara Shuzo, Shiga, Japan), Platinum SYBR Green quantitative polymerase chain reaction (qPCR) SuperMix (Invitrogen, Carlsbad, CA), recombinant human bone morphogenetic protein-2 (rh-BMP-2; Kamiya Biomedical Company, Tukwila, WA), rh-insulin (MP Biomedicals, Irvine, CA), and rh-L-3,3′,5′-triiodothyronine (rhT3, EMD Bioscience, Darmstadt, Germany) were also obtained. RAW264 cell line was purchased from Riken Cell Bank (Tsukuba, Japan).
Human chondrocytes
The ethics committee of the University of Tokyo Hospital approved all procedures in the present study (ethics permission #622). Human cartilage was obtained from remnant auricular cartilage of microtia patients who underwent surgery at the University of Tokyo Hospital. After digestion of the cartilage in 0.15% collagenase solution for 24 h, isolated chondrocytes were seeded on a 10-cm plastic tissue culture dish with chondrocyte growth medium, under the condition of 37°C/5% carbon dioxide (CO2). 16 The cells were cultured to passage 3 and collected for transplantation.
Preparation and transplantation of engineered constructs
PLLA scaffolds (KRI) were produced using a sugar-leaching method. The molecular weight of the scaffolds was 200,000, average pore size was 0.3 mm, and average porosity was more than 95%. PLLA scaffolds with a size of 4 × 4 × 3 mm were sterilized in 70% ethanol before use. Then 1% atelocollagen gel diluted from original 3% atelocollagen gel with DMEM was used as a cell suspension buffer to retain the chondrocytes in the scaffolds efficiently. To make engineered constructs, human chondrocytes suspended in 1% atelocollagen gel or human chondrocytes suspended in DMEM (2 × 107 cells/200 μL) were applied to the PLLA scaffolds and incubated at 37°C/5% CO2 for 3 h (PLLA/gel/cell group and PLLA/cell group, n = 3). At the same time, other scaffolds were allowed to absorb 200 μL of DMEM, followed by incubation as described above to make a control group (PLLA group, n = 3). Regarding the transplantation procedure, 6-week-old male BALB/cAJcl-nu/nu mice (Nisseizai, Tokyo, Japan) were anesthetized using an intraperitoneal injection of sodium pentobarbital (50 mg/kg). A small incision was made on the back in the midline, and three types of constructs (PLLA/gel/cell, PLLA/cell, and PLLA) were transplanted subcutaneously in each animal. Two or 8 weeks after the operation, harvested constructs were assessed using histological, immunohistochemical, and biochemical analyses.
Histological study
Each sample was cut into equal parts, and one was frozen in liquid nitrogen and preserved at −80°C for biochemical analysis, whereas the other was fixed in 4% paraformaldehyde for 3 h, embedded in paraffin, and cut into 8-μm sections. The sections were stained with toluidine blue to detect proteoglycan and with hematoxylin and eosin (H-E) staining. We introduced a scoring system for the analysis of cartilage regeneration in toluidine blue–stained sections. The extent of metachromasia was examined under low magnification (original magnification ×15), at which the whole of a construct could be observed in one view. Each section was scored based on the following criteria: 1 = free of metachromasia throughout the construct, 2 = slight metachromasia throughout or in part of the construct, 3 = dense metachromasia accompanied by the formation of chondrocyte lacunae in spotted areas of the construct, and 4 = dense metachromasia accompanied by the formation of chondrocyte lacunae in continuous areas of the construct. In each group, three sections from different animals were used for analysis, and the mean of the three values was used to determine the extent of cartilage regeneration.
Immunohistochemical study
The sections were also used for immunohistochemical staining for type II collagen, vascular endothelial cells, macrophages, and MIF according to previous studies.17–19 Briefly, the sections were deparaffinized in xylene, hydrated with step-down concentrations of ethanol, and quenched in a mixture of 3% hydrogen peroxide in methanol for 15 min at room temperature. After antigen retrieval, the sections were treated with 10% normal serum for 20 min at room temperature to reduce non-specific binding of antibodies. Incubation with primary antibodies (for type II collagen detection, rabbit polyclonal anti-type II collagen, 1:100 dilution; for vascular endothelial cell detection, rat anti-mouse CD31 antibody, 1:100 dilution; for macrophage detection, rat anti-mouse F4/80 antibody, 1:100 dilution; for MIF detection, rabbit polyclonal anti-MIF antibody, 1:100 dilution) was performed for 1 h at 37°C. Then the sections were incubated with biotinylated secondary antibodies (1:200 dilution) for 30 min at room temperature. Consecutive steps for the visualization of positive reactions were conducted using a Vectastain ABC kit and peroxidase substrate kit diaminobenzidine according to the manufacturer's instructions. Subsequently, the sections were counterstained with hematoxylin. Then the number of positive cells in the sections of immunohistochemical staining for F4/80 and MIF was evaluated. Three different fields were randomly selected from each section, and the numbers of positive areas per 0.5 × 0.5 mm were measured. Three sections from different animals were used in each group, and the mean of nine values was used to determine the blood vessel density.
Biochemical study
Samples stored at –80°C for biochemical analysis were cut into small pieces with scissors and suspended in homogenizing buffer. 20 After homogenization at 24,000 rpm for 30 sec, the supernatant was analyzed for the presence of IL-1β protein with a Quantikine murine IL-1β kit according to the manufacturer's instructions. Hemoglobin concentration in the supernatant was determined using a hemoglobin assay kit by measuring the absorbance at 540 nm. 21 Measurements were performed three times, and mean values were used for statistical analysis.
Co-culture and gene expression
We conducted co-culture of human auricular chondrocytes, mouse macrophage cell line RAW264, and PLLA scaffolds in vitro to assess the expression of MIF. The cells from different species were used to clarify the expression of MIF in the chondrocytes using a set of primers specific to human MIF. The chondrocytes and RAW264 were suspended in 1% atelocollagen gel (1 × 107 cells/mL) before seeding into PLLA porous scaffolds in 15-mL conical tubes. After incubation without any medium at 37°C for 2 h for gelation, the constructs were cultured in chondrogenic medium consisting of BMP-2, insulin, and T3 for 1 week. 22 Total RNA was isolated from chondrocytes using Isogen and reverse transcribed with PrimeScript reverse transcriptase and random hexamers. Gene expression was detected using real-time qPCR using the standard SYBR green method with an ABI Prism 7700 sequence detection system (Applied BioSystems, Foster City, CA). Standard templates were produced according to a previous study. 22 Sequences of primers were 5′-GCCCGGACAGGGTCTACA-3′ and 5′-CTTAGGCGAAGGTGGAGTTGTT-3′ for hMIF; 5′-GAAGGTGAAGGTCGGAGTCA-3′ and 5′-GAAGATGGTGATGGGATTTC-3′ for glyceraldehyde-3-phosphate dehydrogenase (GAPDH). All primers have been confirmed to be specific to the human gene. The expression level of MIF was normalized to GAPDH expression.
Statistical analysis
Data are expressed as means ± standard deviations. Statistical significance was evaluated using Tukey-Kramer test for multiple comparisons. P < 0.05 was interpreted to denote statistical significance.
Results
Cartilage regeneration in engineered constructs
We made engineered constructs using PLLA porous scaffolds with or without human chondrocytes or atelocollagen gel and transplanted them into the subcutaneous tissue of the back of nude mice. Because the properties of cell attachment and retention of porous scaffolds are potentially poor, we adopted an additional construct using atelocollagen gel, which served as a binding material of cells. Thus, we conducted our present study with the following three types of constructs; PLLA/cell/gel, PLLA/cell, and PLLA. Even though the same numbers of cell were applied, the PLLA/cell/gel constructs were observed to retain more cells than the PLLA/cell constructs (Fig. 1, before transplant). On gross observation, the constructs maintained the original shapes of the PLLA porous scaffolds in all groups, even after subcutaneous transplantation. The constructs in the PLLA/cell/gel group were whiter than those in the other two groups at 2 and 8 weeks after transplantation (Fig. 1, 2 and 8 weeks). The skin where the constructs were transplanted was smooth, and no marked tissue reaction such as redness, swelling, or exposure of the constructs was apparent after 2 weeks (Fig. 1, 2 weeks).

Gross and histological findings of each construct before and after transplantation. Left: Gross findings and toluidine blue staining of each contruct before transplantation. Right: Toluidine blue staining of each construct before transplantation. Poly-L-lactic acid (PLLA)/cell/gel constructs were observed to retain cells more efficiently and evenly than PLLA/cell constructs. Scale bars: 100 μm. Right: Skin appearance of transplanted site in each group at 2 weeks and gross images of each engineered construct at 2 and 8 weeks after transplantation. Skin of the transplanted site was smooth, and no marked tissue reaction was apparent at 2 weeks. The constructs in the PLLA/cell/gel group were whiter than those in the other two groups. PLLA/gel/cell: constructs with chondrocytes and scaffold consisting of atelocollagen hydrogel and PLLA porous body. PLLA/cell: constructs with chondrocytes and PLLA porous body. PLLA: only PLLA porous body. Color images available online at www.liebertonline.com/ten.
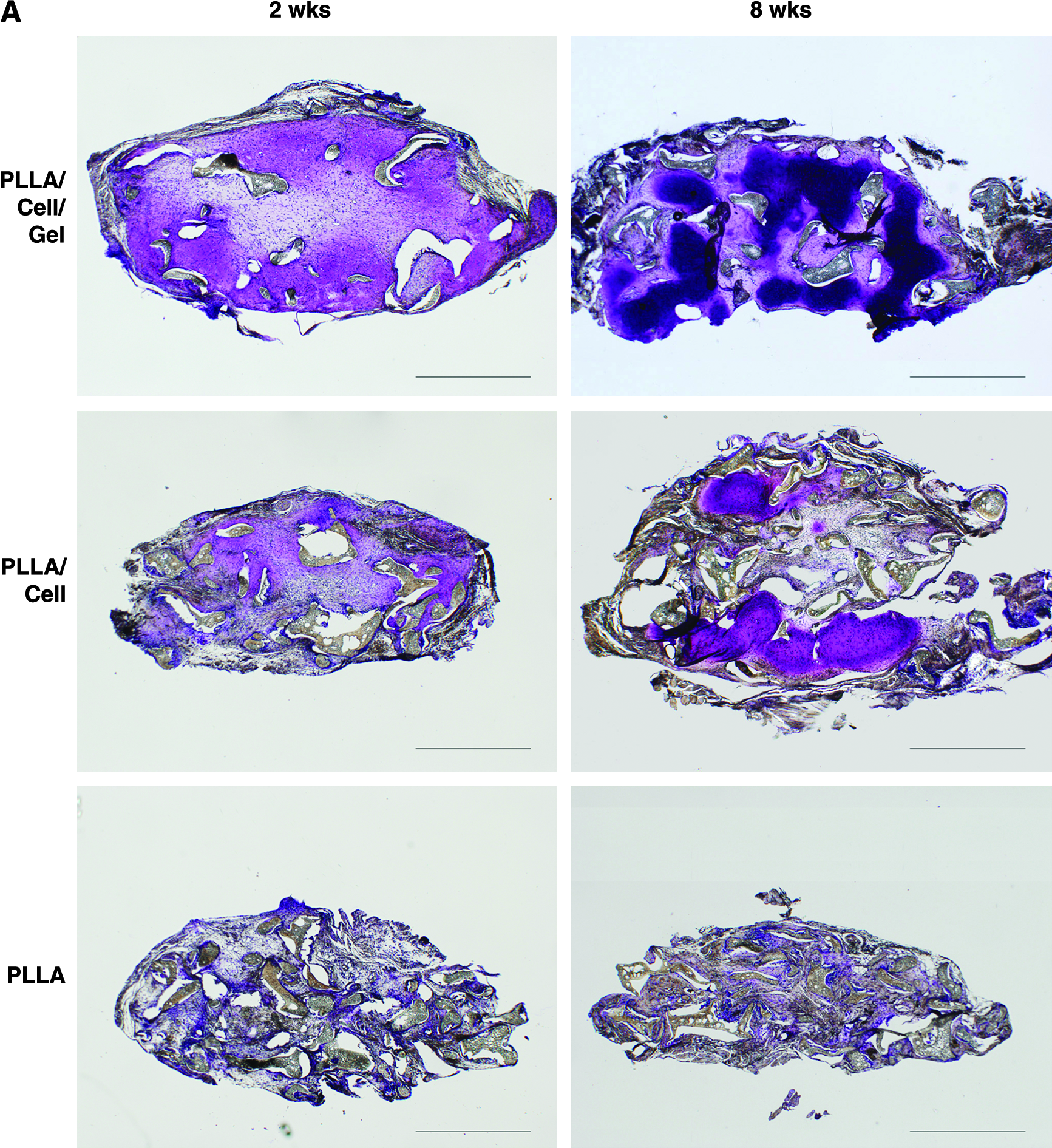
On histological examination, toluidine blue staining in the PLLA/cell/gel group showed increasing metachromasia, which indicates accumulation of proteoglycan in cartilaginous matrix with time, and mature cartilage was observed throughout the engineered tissue by 8 weeks (Fig. 2, PLLA/cell/gel). Although the PLLA/cell construct showed less metachromasia than the PLLA/cell/gel construct, no cartilaginous matrix was recognized in the PLLA group over the observation period (Fig. 2, PLLA/cell and PLLA). Metachromasia score increased with time in the PLLA/cell/gel and PLLA/cell groups, although the PLLA/cell construct had significantly lower scores than the PLLA/cell/gel construct at 2 and 8 weeks after the transplantation (Fig. 2, PLLA/cell and PLLA). H-E staining of the engineered tissues in the PLLA/cell/gel group revealed that myriad cells with round or flattened nuclei and some extracellular matrix surrounded the unstained PLLA at 2 weeks. By 8 weeks, although the PLLA still remained in the constructs, most of the cells had become round, with abundant extracellular matrix around them (Fig. 3, PLLA/cell/gel). These areas were also shown to be immunopositive for a cartilage-specific marker type II collagen, suggesting they could be regarded as regenerative cartilage but not granulation tissue (Fig. 4, PLLA/cell/gel). This alteration was also confirmed in the PLLA/cell group, although the area of cartilage regeneration was smaller (Fig. 3, PLLA/cell). In the constructs in the PLLA group, there were few cells with large cytoplasm and abundant matrix at 2 weeks. At 8 weeks, areas with high cellularity surrounded the PLLA (Fig. 3, PLLA).
(

Histological findings of hematoxylin and eosin staining in each group at 2 and 8 weeks after transplantation. By 8 weeks, cartilage appeared in constructs with chondrocytes and scaffold consisting of the atelocollagen hydrogel (poly-L-lactic acid (PLLA)/gel/cell) and constructs with chondrocytes and PLLA porous body (PLLA/cell), although areas of high cellularity (asterisks) surrounded the PLLA polymers in the constructs only with PLLA porous body (PLLA). Scale bars: 100 μm. Color images available online at www.liebertonline.com/ten.
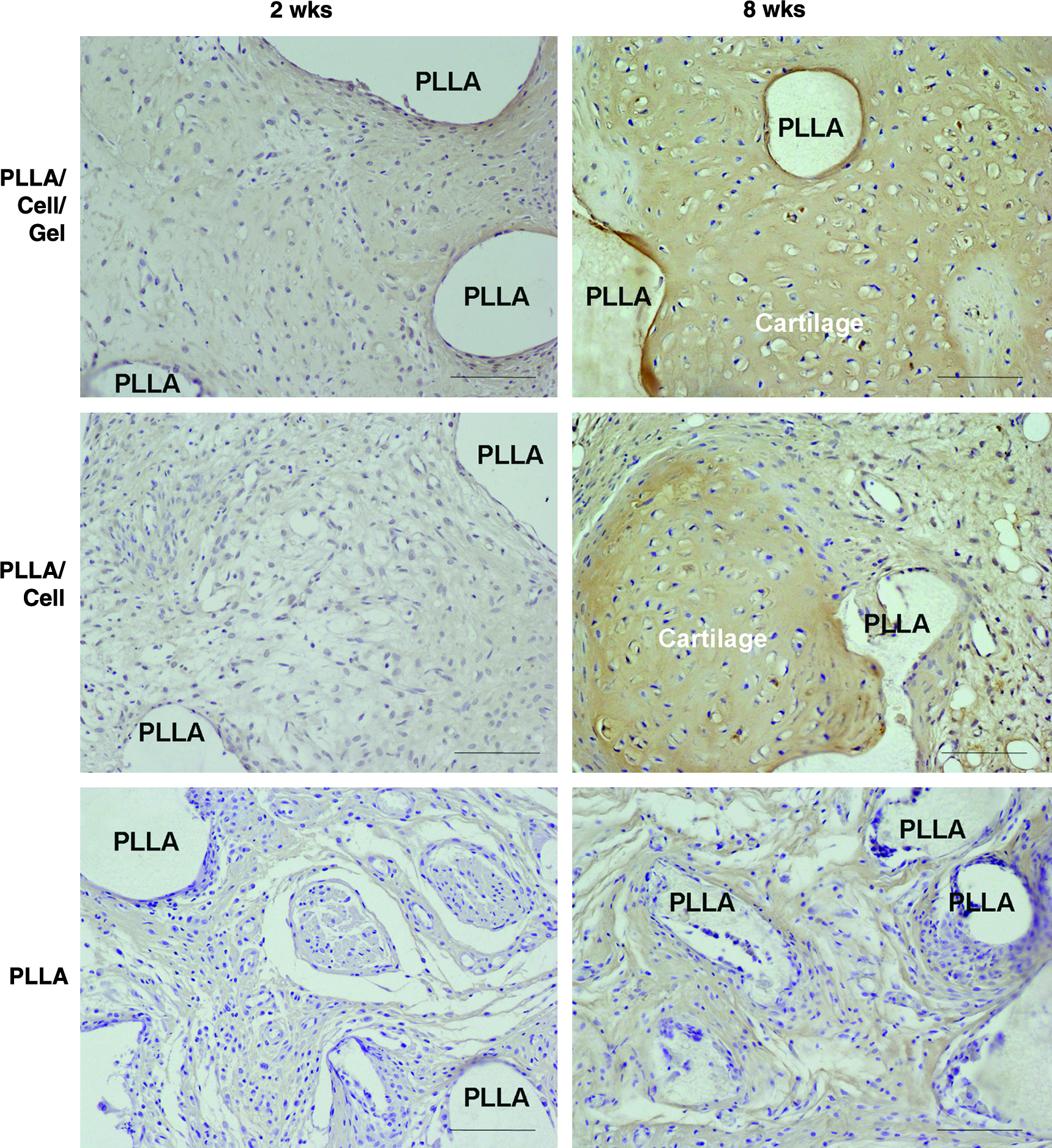
Cartilage regeneration in engineered cartilage constructs 2 and 8 weeks after transplantation. The area of round cells with abundant extracellular matrix was positive for cartilage-specific marker type II collagen in constructs with chondrocytes and scaffold consisting of atelocollagen hydrogel (poly-L-lactic acid (PLLA)/gel/cell) and constructs with chondrocytes and PLLA porous body (PLLA/cell) at 8 weeks. PLLA: only PLLA porous body. Scale bars, 100 μm. Color images available online at www.liebertonline.com/ten.
Tissue reactions against cartilage constructs
We evaluated neovascularization and activation of macrophages as tissue reactions. Immunohistochemical localization of CD31, indicating vascular endothelial cells, was observed in all groups at 2 weeks, suggesting the formation of new blood vessels (Fig. 5, 2 weeks). In the PLLA/cell/gel and PLLA/cell groups, although blood vessels were scattered throughout the engineered tissues at 2 weeks, they decreased in number and showed a change in localization to only non-cartilage areas by 8 weeks (Fig. 5, PLLA/cell/gel and PLLA/cell). Meanwhile, immunopositivity for CD31 was maintained in the PLLA group over time. To support the morphological findings of neovascularization, hemoglobin level in the engineered constructs was biochemically measured using enzyme-linked immunoassay. It showed that, at 2 weeks, the hemoglobin level in the PLLA/cell/gel group was significantly lower than in the PLLA group. By 8 weeks, the PLLA/cell group and the PLLA/cell/gel group also showed a lower hemoglobin level than the PLLA group (Fig. 6, hemoglobin level).

Neovascularization in engineered cartilage constructs 2 and 8 weeks after transplantation. Endothelial cells of blood vessels immunolocalized by CD31 were abundantly found in all groups at 2 weeks, although they decreased in constructs with chondrocytes and scaffold consisting of atelocollagen hydrogel (poly-L-lactic acid (PLLA)/gel/cell) and constructs with chondrocytes and PLLA porous body (PLLA/cell) at 8 weeks. PLLA: only PLLA porous body. Scale bars: 100 μm. Color images available online at www.liebertonline.com/ten.
Biochemical assessment of tissue reactions 2 and 8 weeks after transplantation. Top: Hemoglobin level was measured in constructs with chondrocytes and scaffold consisting of atelocollagen hydrogel (poly-L-lactic acid (PLLA)/gel/cell, n = 3 for each week ), constructs with chondrocytes and PLLA porous body (PLLA/cell, n = 3 for each week ), and constructs only with PLLA porous body (PLLA, n = 3 for each week ). Bottom: IL-1β level in each group (n = 3, respectively) was determined using enzyme-linked immunoassay. Data are expressed as means (bars) ± standard errors (error bars). *p < 0.05, **p < 0.01 vs PLLA.
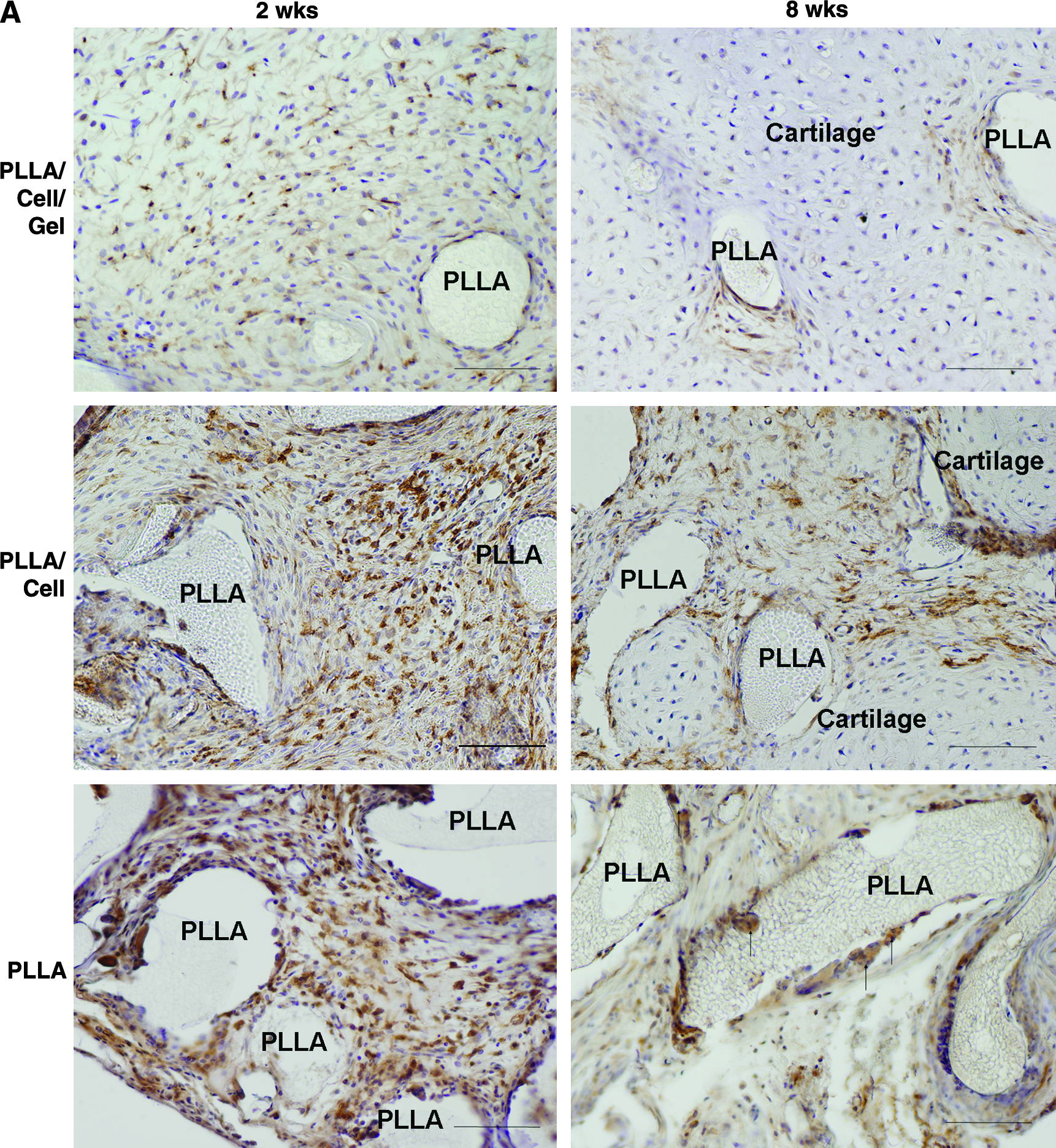
Regarding the activation of macrophages, their localization was shown using immunohistochemical staining for F4/80 antigen. Evenly distributed macrophages were noted in each group at 2 weeks, and their accumulation appeared more intense in the PLLA/cell and PLLA groups than in the PLLA/cell/gel group (Fig. 7, 2 weeks). By 8 weeks, the macrophage localization had become sparse and gradually restricted to non-cartilage areas in the PLLA/cell/gel and PLLA/cell groups (Fig. 7, PLLA/cell/gel and PLLA/cell). In the PLLA group, immunopositive cells were concentrated in the areas around the PLLA, and some of them had fused to form multinucleated giant cells by 8 weeks (Fig. 7, PLLA). The number of macrophages (F4/80-positive cells) was significantly higher in the PLLA constructs than in the PLLA/cell/gel and PLLA/cell constructs throughout the observation period. Furthermore, there was a significant difference in macrophage number between the PLLA/cell/gel constructs and the PLLA/cell constructs at 2 weeks after transplantation. (Fig. 6, macrophage number). Biochemical measurement of IL-1β, which is a major activator of macrophages, was also significantly lower in the PLLA/cell/gel and PLLA/cell groups than in the PLLA group at 2 and 8 weeks (Fig. 6, IL-1β).

(
As the cytological mechanism of regulation of macrophage distribution, we focused on MIF. Immunohistochemical staining for MIF antigen revealed that positive cells were widely observed in the PLLA/cell/gel and PLLA/cell groups at 2 weeks (Fig. 8, 2 weeks). By 8 weeks, immunopositivity was confined to mature cartilage (Fig. 8, 8 weeks). The positivity was significantly higher in the PLLA/cell/gel and PLLA/cell groups than in the PLLA group at 2 and 8 weeks (Fig. 8, MIF-positive cell number). In the PLLA group, no MIF-positive cells were observed at 2 or 8 weeks, suggesting that cartilage regeneration increased in accordance with MIF localization. Then we conducted co-culture of human auricular chondrocytes, mouse macrophage cell line RAW264, and PLLA to assess the expression of MIF in vitro. The results demonstrated that chondrocytes cultured with PLLA scaffolds were MIF positive but that the expression was significantly higher when co-cultured with RAW264 and PLLA scaffolds (Fig. 8, hMIF expression).
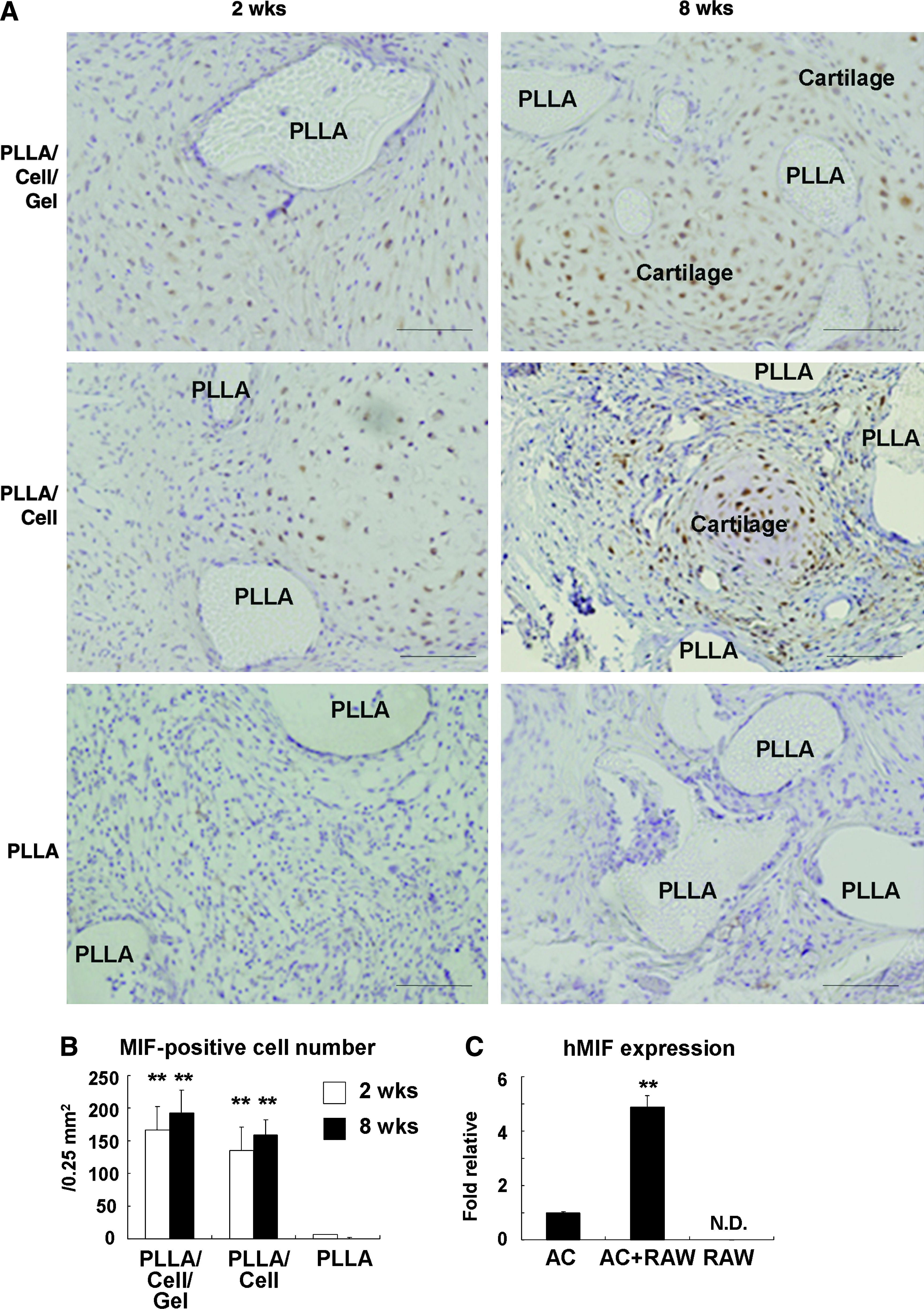
Immunolocalization of macrophage migration inhibitory factor (MIF ) in engineered constructs 2 and 8 weeks after transplantation and MIF expression in vitro. (
Discussion
Similar to previous reports on the intraosseous application of bone screws,14,15 the migration of macrophages and the formation of new blood vessels were observed mostly around the PLLA scaffolds when they were subcutaneously implanted with or without chondrocytes in the present study. These tissue reactions from the surrounding areas can potentially cause deformity of engineered cartilage, because macrophages promote the degradation of PLLA scaffolds,14,15 which would weaken the mechanical support of the engineered constructs. In addition, macrophages secrete catabolic cytokines, including IL-1β, which can make chondrocytes release aggrecanase and matrix metalloproteinases,23,24 causing deterioration of matrix accumulation in engineered cartilage. It is therefore suggested that controlling the early-phase tissue reactions would be of importance in reducing the risk of deformity and malformation of engineered cartilage.
Our study demonstrated that tissue reactions triggered by PLLA could be diminished when the PLLA scaffolds contained chondrocytes. This finding was highly evident in the constructs with cells and atelocollagen, the PLLA/gel/cell group, which showed superior cartilage regeneration to that in the other groups (Fig. 2 and 3). The molecular mechanism mediating suppressed reactions in the PLLA/gel/cell group remains unclear, but three possibilities can be suggested, based on differences in the surrounding environment of PLLA.
The first may be related to mechanical stimulation of the rough surface in PLLA/cell or PLLA constructs. The PLLA/cell group could not retain cells sufficiently or as evenly (Fig. 1, before transplant) as the PLLA/gel/cell group. For that, the cartilage regeneration in the PLLA/cell constructs would be relatively poor, and the surface of the PLLA/cell constructs and the PLLA constructs, therefore, could be rougher (Fig. 1, 2 weeks). However, the difference in the construct surface would not affect the intensity of the tissue reactions, because the engineered constructs became covered with fibrous tissue after transplantation and were not so movable as to stimulate surrounding tissue mechanically. The skin where the constructs were transplanted was smooth, and no intensive tissue reaction such as redness, swelling, or exposure of the constructs was apparent. Thus, we suppose that the stronger tissue reactions in the PLLA or PLLA/cell constructs would be due to biological effects of the engineered cartilage constructs rather than physical stimulation of a rough surface.
The second is that atelocollagen gel in the constructs might act as a physical barrier to the migration of inflammatory cells. As atelocollagen is removed of antigenic telopeptide by pepsin treatment, it possesses negligible immunogenicity and angiogenesis induction.25,26 Thus, engineered constructs containing atelocollagen might show less tissue reactions. However, because suppression of tissue reactions was also observed in the PLLA/cell group that did not contain atelocollagen, even if to a lesser degree, its mechanism could not be confined to the effects of atelocollagen.
The last possible reason for the limited tissue reactions in the engineered cartilage could be related to biological factors secreted from the chondrocytes in the constructs. Factors secreted from chondrocytes may bring about a situation similar to immune privilege. Immune privilege was originally shown in particular organs, such as the anterior chamber of the eye, brain, and placenta, where antigens do not cause inflammation. 27 This natural immune privilege is considered to be due to the need for these tissues to be protected from excessive tissue reactions. 28 Several factors have been indicated as being responsible for immune privilege in normal aqueous humor in the anterior chamber of the eye, including MIF.29–31 MIF exerts its function by directly abolishing the actions of macrophages and natural killer (NK) cells.31,32 We speculated that chondrocytes might produce these factors to protect themselves and thus investigated the expression of MIF in vitro and in engineered constructs. The present study revealed the presence of MIF-positive cells in chondrocytes cultured with PLLA as well as in the engineered cartilage. Although chondrocytes cultured with PLLA scaffolds in vitro were MIF positive, the expression of MIF in chondrocytes became significantly higher when co-cultured with RAW264 and PLLA scaffolds. In the engineered cartilage, MIF-positive cells were scattered at 2 weeks, when the formation of cartilage was not yet apparent (Fig. 8). During the subsequent process of cartilage maturation, macrophages were observed to converge in non-cartilage areas, whereas MIF-positive cells were located in cartilage areas, indicating that chondrocytes, and not macrophages, were MIF positive.
In addition to its function in immune privilege, it has been recently reported that MIF acts as a pro-inflammatory factor in several inflammatory diseases, such as rheumatoid arthritis, 33 atherosclerosis, 34 and others.35,36 Considering the MIF positivity of chondrocytes in the engineered cartilage, it could be speculated that MIF secreted from chondrocytes would principally maintain immune privilege around the engineered cartilage but may regionally promote the absorption of foreign materials in non-cartilage areas, such as PLLA, contributing to the formation of homogeneous cartilage in the engineered constructs.
The present study revealed that PLLA in the transplanted constructs remained, regardless of the experimental group, even at 8 weeks after transplantation. Because it was not feasible to measure the areas of remaining PLLA in histological sections precisely, we could not quantify the PLLA degradation in the engineered constructs. However, histological images at 8 weeks demonstrated that macrophages and multinucleated cells surrounded the remaining PLLA, indicating biological degradation of PLLA in the engineered constructs, although in a gradual manner. Relatively prolonged degradation of PLLA has been reported, and Walton et al. 14 demonstrated that PLLA orthopedic implants remained for more than 3 years in sheep. Although the slow degradation rate of PLLA could be convenient to secure sufficient time for the maturation of engineered cartilage, the period of scaffold degradation should be ideally in accordance with that of tissue formation. Further elaboration would be required to obtain such scaffolds.
In summary, the present study suggests that intense tissue reactions inevitably occurred in biopolymers alone, but it is possible that the maturation of engineered cartilage suppressed these reactions, which PLLA caused. Sufficient cartilage formation may contribute to circumventing deformation or malformation of engineered tissues by regulating tissue reactions.
Footnotes
Acknowledgments
This work was supported by Grants-in-Aid for Scientific Research (C) from the Ministry of Education, Culture, Sports, Science and Technology of Japan (No. 19592283), Establishment of Evaluation Method for Tissue Engineering, the Japan Science and Technology Agency, and Research and Development Programs for Three-dimensional Complex Organ Structures from the New Energy and Industrial Technology Development Organization.
Disclosure Statement
No competing financial interests exist.