
Abstract
Conventional clinical therapies are unable to resolve osteochondral defects adequately; hence, tissue engineering solutions are sought to address the challenge. A biphasic implant that was seeded with mesenchymal stem cells (MSCs) and coupled with an electrospun membrane was evaluated as an alternative. This dual phase construct comprised of a polycaprolactone (PCL) cartilage scaffold and a PCL–tricalcium phosphate osseous matrix. Autologous MSCs were seeded into the entire implant via fibrin and the construct was inserted into critically sized osteochondral defects located at the medial condyle and patellar groove of pigs. The defect was resurfaced with a PCL–collagen electrospun mesh, which served as a substitute for periosteal flap in preventing cell leakage. Controls without either implanted MSCs or resurfacing membrane were included. After 6 months, cartilaginous repair was observed with a low occurrence of fibrocartilage at the medial condyle. Osteochondral repair was promoted and host cartilage degeneration was arrested as shown by superior glycosaminoglycan maintenance. This positive morphological outcome was supported by a higher relative Young's modulus, which indicated functional cartilage restoration. Bone ingrowth and remodeling occurred in all groups, with a higher degree of mineralization in the experimental group. Tissue repair was compromised in the absence of the implanted cells or the resurfacing membrane. Moreover, healing was inferior at the patellar groove when compared with the medial condyle and this was attributed to the native biomechanical features.
Introduction
Cell implantation procedures at the cartilage site are frequently accompanied by a periosteal flap as it fulfills various biomechanical and biological functions. 20 First, it seals the defect and prevents the leakage of the implanted cells. Moreover, the residing periosteal cells stimulate cartilage repair via secretion of cytokines and they can also differentiate into chondroblasts, which populate the defect site. 21 However, there were several disadvantages associated with the graft. It was discovered that a staggering 36.4% of the patients who received the periosteal patch during autologous chondrocyte implantation experienced cartilage hypertrophy. 22 Similar studies in sheep have shown a 45–70% increase in the density of the subchondral bone. 23 This occurred because the periosteal patch stimulated bone remodeling and the stiffening would lead to the degeneration of the overlying cartilage via a build up of stresses. This response was attributed to the expression of vascular endothelial growth factor (VEGF) by the periosteum. 24 VEGF induces vasculature invasion, which encourages bone development. 24 In addition, Kajitani et al. questioned the efficacy of the periosteal cells as there was no difference in the outcome of the cartilage defects that were resurfaced with either fresh or frozen periosteum grafts. 25 Moreover, the quality of the natural graft is influenced by the patient's age and surgical harvesting technique.26,27 Graft harvesting also inflicts donor-site morbidity and scarring. In view of these concerns, a tissue-engineered alternative was sought.
The author proposed a large animal study (Fig. 1) so as to evaluate the efficacy of a biphasic osteochondral implant coupled with an electrospun membrane in the repair of critically sized defects at different sites in the knee joint. The implant would comprise of a polycaprolactone (PCL) cartilage scaffold and a PCL–tricalcium phosphate (TCP) matrix, which served as the bone substratum. These rapid prototyped matrices were mechanically competent and porous, and hence, they would shield growing tissues from excessive stresses while facilitating tissue ingrowth and nutrient exchange. Autologous MSCs were seeded into the biphasic implant via fibrin glue so as to promote cartilage and bone regeneration. These biological constructs would be implanted into critically sized osteochondral defects located at the medial condyle and patellar groove of pigs. The defect was subsequently resurfaced with an electrospun PCL–collagen 20% membrane, which served as a synthetic substitute for the periosteal patch, whose use was associated with undesirable side effects such as cartilage hypertrophy and subchondral bone sclerosis.22,23 This permeable mesh would arrest the leakage of the implanted cells while facilitating nutrient exchange from the synovial fluid to the repair site. Further, prior in vitro trials on the synthetic patch demonstrated the absence of tissue hypertrophy (unpublished data). Adolescent pigs were used in this investigation. This experimental model was adopted by Chang et al., Jiang et al., Pulliainen et al., Li et al., and Zhou et al., who used 2–9-month-old pigs for osteochondral regenerative studies.2,5,10,16,28 These pigs were skeletally immature because growth plate fusion was absent at 8 months.5,28 The common use of the immature animal for cartilage regenerative studies was rationalized by the unsatisfactory spontaneous repair. Chang et al. observed tissue deterioration over a period of 6 months in the untreated osteochondral defects (8 mm in diameter, 5 mm in depth) of 4–8-month-old pigs. 2 Seamless self-repair in young animals is unlikely, except for fetal lambs. 29 Moreover, immature pigs have been used to model the condition osteochondritis dissecans, which is more prevalent among the young than the elderly. 30 Although natural growth did not exert a significant influence on healing in the model of Chang et al., 2 the effect was accounted for through the use of 6-month-old pigs across the different treatment groups in this investigation. The reparative outcome was subsequently compared after 6 months via microcomputed tomography (micro-CT) scans, mechanical testing, and histological analysis. Results from the experimental group were compared against controls without implanted MSCs or electrospun mesh.
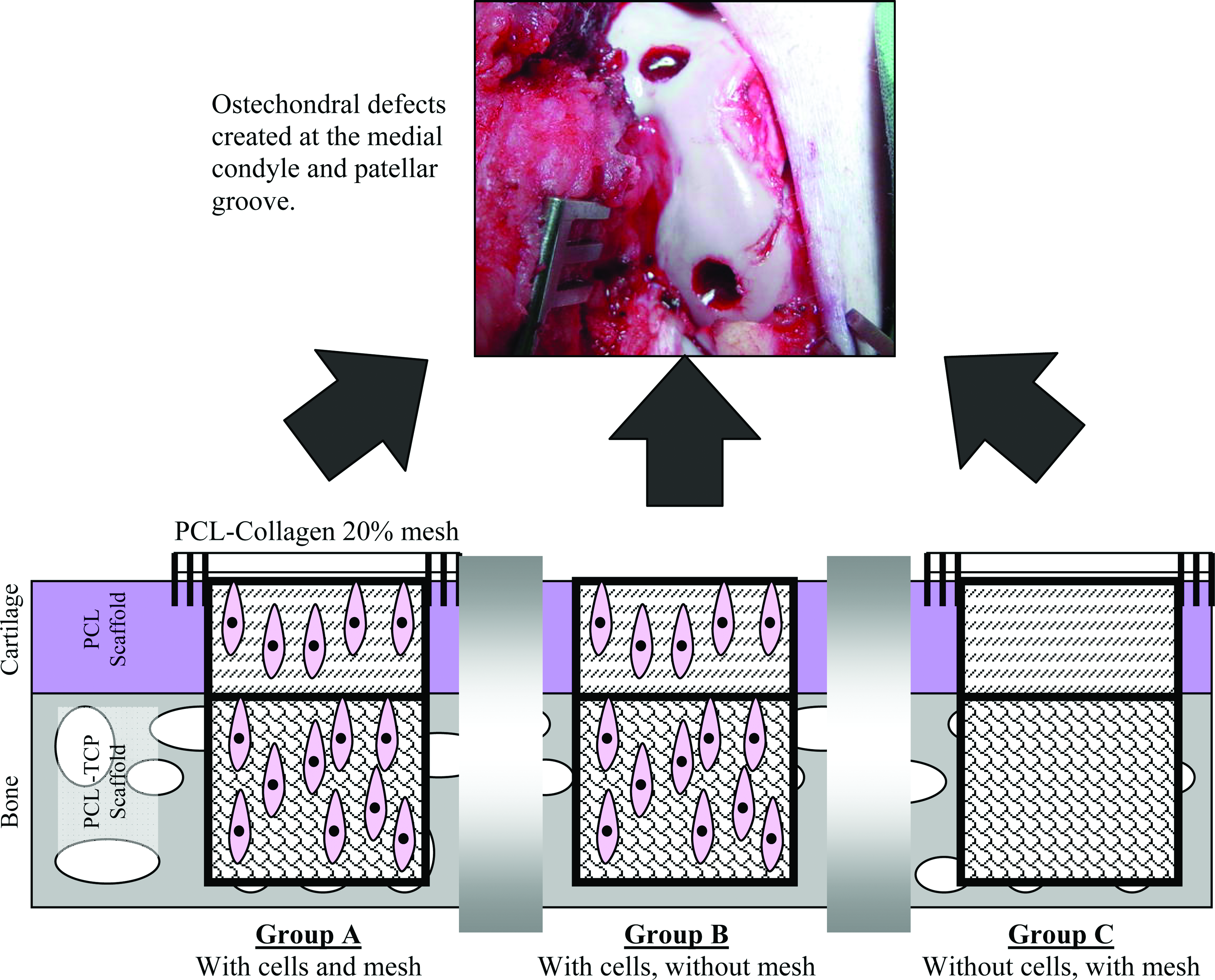
A schematic diagram of the experimental layout. Three groups of biphasic constructs were evaluated: Group A: with cells and mesh; Group B: with cells and without mesh; Group C: without cells and with mesh. These were implanted into critically sized osteochondral defects located at the medial condyle and patellar groove in the pig model. PCL, polycaprolactone; TCP, tricalcium phosphate. Color images available online at www.liebertonline.com/ten.
Materials and Methods
Reagents and chemicals
Unless otherwise stated, all reagents used in this study were purchased from Sigma Aldrich (St. Louis, MO). Low-glucose Dulbecco's modified Eagle's medium was purchased from Gibco BRL (Grand Islands, NY). All labware consumables were purchased from Becton-Dickinson (Franklin Lakes, NJ).
Scaffold fabrication
The PCL and PCL–TCP (Osteopore, Singapore, Singapore) scaffolds were built using the Fused Deposition Modeling 3000 setup (Stratasys, Eden Prairie, MN). PCL (Mw of 139,300) was acquired from Birimingham Polymers (Pelham, AL) and TCP was purchased from Shanghai Rebone Biomaterials (Shanghai, China). TCP powder (density of 3.14 g/cm3) was sieved through a 60-μm sieve and analyzed with Coulter Laser Diffraction LS100Q particle size analyzer (working range: 0.4–1000 μm). Ninety percent, 75%, 50%, 25%, and 10% volumes of the sieved ceramic fell below particle diameters of 63, 34, 15, 5, and 2 μm, respectively. TCP was blended with PCL at a ratio of 1:4. The laydown patterns of the PCL and PCL–TCP scaffolds were 0°/90°/180° and 0°/60°/120°, respectively. The PCL scaffold has a porosity of 77% and it was cut into 8-mm-diameter discs with a thickness of 2.5 mm. The compressive Young's modulus and yield strength of the PCL scaffold were 15.7 MPa and 2.12 MPa, respectively. The porosity of the PCL–TCP scaffold was 56% and it was sectioned into 8-mm-diameter discs with a thickness of 5.5 mm. The PCL–TCP scaffold has a stiffness of 124 MPa and yield strength of 4.2 MPa. Prior to use, both scaffolds were rendered hydrophilic through a 3-h treatment in 5 M NaOH at 37°C. Sterilization was achieved with 70% ethanol treatment and UV irradiation.
Fabrication of the PCL–Collagen 20% electrospun mesh
PCL collagen composite was prepared by dissolving PCL (Mw of 139,300) and bovine collagen type I (Symatase, Chaponost, France) in 1,1,1,3,3,3-fluoro-2-propanol (HFP; Fluka, Buchs, Switzerland). PCL (0.1 g) and collagen (0.025 g) were added into 1 mL of HFP so as to constitute the PCL–collagen 20% mix. The solution was subsequently loaded into a syringe positioned on a pump and discharged through a metallic needle at a flow rate of 0.75 mL/h with a potential of 10 kV. The resultant fibers were collected onto an earthed aluminum foil placed 15 cm below the discharge point. Once completed, the electrospun sheets were dried in a desiccator. Ten-millimeter-diameter patches were cut from the sheet. Prior to use, the patches were sterilized via 70% ethanol treatment with UV irradiation.
Bone marrow aspiration, MSC isolation, and culturing
Approval for the animal work was granted by the Institutional Animal Care and Use Committee of the Singapore General Hospital. Six-month-old Yorkshire Duroc pigs were procured for the procedure. The animals were anesthetized and scrubbed prior to bone marrow aspiration from the iliac crest region. Upon collection, the bone marrow was inoculated into 300-cm2 flasks containing low-glucose Dulbecco's modified Eagle's medium, 10% fetal bovine serum (Invitrogen, Carlsbad, CA), and 100 U/mL penicillin–streptomycin (Invitrogen) and incubated at 37°C in 5% CO2, 95% air, and 99% relative humidity. The unattached cells were removed via repeated phosphate-buffered saline washings after 24 h. The adherent MSCs were cultured with media changes on every third day. When the cultures were at 75% confluence, they were passaged with 0.25% trypsin (Invitrogen). The enzymatic treatment was quenched in the presence of fetal bovine serum and cell count was done using a hemocytometer. Only passage 1 MSCs were used in the experiment.
Fibrin encapsulation of MSC within the biphasic osteochondral construct
Passage 1 MSCs were mixed in fibrin and pipetted into sterile PCL and PCL–TCP scaffolds, and gel polymerization was subsequently achieved with the addition of thrombin. The final concentrations of fibrin and thrombin of the encapsulation matrix were 30 mg/mL and 5 U/mL, respectively. Five million MSCs were entrapped in the PCL cartilage scaffold, whereas 2 million MSCs were seeded into the PCL–TCP matrix. The cartilage and bone constructs were maintained in the MSC expansion media prior to implantation.
Surgical implantation
Six-month-old pigs were anesthetized and maintained in dorsal recumbency. The skin of the right hind knee joint was scrubbed and disinfected. Following that, a medial stifle arthrotomy was carried out to expose the distal femur and a manual hand drill was used to core out defects measuring 8 mm diameter and 8 mm depth at the medial condyle and the patellar groove. The biphasic osteochondral implant was inserted into the defect, secured through interference fit, and flushed to the articulating surface. A PCL–collagen patch was used to resurface the cartilage defect in groups A and C. The patch was sutured down onto the surrounding cartilage and secured with the application of fibrin glue at the periphery. Wound closure was accomplished with bioabsorbable sutures, and the animal was returned to the enclosure and monitored till full recovery. The pigs were allowed to move freely without constraints within the pens. After 6 months, the animals were euthanized with an overdose of barbiturates. Medial condyle and patellar groove regions of the operated joints were excised and kept for analysis. Native samples were also taken from the unoperated left limb of each animal. At the point of euthanasia, an average weight gain of 111.7% was noted for every animal.
Gross morphology and histology
The harvested samples were photographed and fixed in 10% neutral buffered formalin. Decalcification in 30% formic acid, ethanol dehydration, and paraffin embedding followed. Five-micrometer sections were taken from the center of the defect site and stained for cartilaginous matrix using 1% toluidine blue and 0.1% safranin O fast green. Morphological details were observed via hematoxylin–eosin and Masson's trichrome staining. The stained sections were scored under blinded conditions by three examiners using a modified O'Driscoll's score (Table 1). 31 The specimens were graded for hyaline cartilage formation, structural characteristics, and tissue morphology. In addition, immunohistology was conducted using collagen I (dilution factor 1:500), collagen II (dilution factor 1:500; Chemicon, Temecula, CA), and isotype (Dakocytomation, Glostrup, Denmark) antibodies. Endogenous peroxidase was blocked with hydrogen peroxide and antigen retrieval was performed by treating the sections with pepsin (Labvision, Fremont, CA) for 20 min. Biotinylated goat anti-mouse antibodies were used as the secondary antibodies (Labvision) for a 30-min reaction at room temperature. Streptavidin peroxidase was administered for 45 min, using 3,3′ diaminobenzidine as a chromogenic agent. Counterstaining was done with Gill's hematoxylin, after which the sections were dehydrated before being coverslipped.
Compared with the adjacent normal cartilage thickness. The total score is 26 points.
Micro-CT
The osteochondral samples were loaded onto a Skyscan in vivo microtomograph 1076 scanner (Skyscan, Kontich, Belgium) for micro-CT analysis. The data were acquired at a resolution of 35 μm and reconstructed using a modified Feldkamp algorithm as provided by Skyscan. Visualization and analysis were carried out with MIMICS (Materialize, Leuven, Belgium). A threshold of −175 to 1370 HU was used to differentiate growing bone within the bone scaffold from the surrounding tissue. As the boundaries of the original bone defect were highly visible from the scans, the defect site was isolated out via the positioning of a cylindrical region of interest (ROI) measuring 8 mm in diameter. As the pigs were still growing with the enlargement of the joints, bone growth occurred over the top of the bone implant (Fig. 2). This region was also examined via micro-CT. Volumetric measurements of bone growth were compared against that of the unoperated knee joint in the same animal at a similar site and they were expressed as the degree of mineralization.

Spatial changes at the implant site due to joint enlargement, which led to the evaluation of the two region of interests in the micro-CT model. The bone growth above (gray) and within (yellow) the bone implant are shown. The host bone is denoted pink. micro-CT, microcomputed tomography. Color images available online at www.liebertonline.com/ten.
Indentation of the repaired cartilage
The Young's modulus of the repaired and native cartilage was measured via indentation tests that were conducted with an Instron 5848 microtester (Norwood, MA). Thawed samples were positioned in a custom-made rotatable holder that allowed perpendicular alignment of the cartilage surface to a 1.6-mm-diameter, porous, plane-ended indenter (Captan Permaflow, Gardena, CA). After a tare load, five stepwise consecutive 10 μm displacements were compressed into the cartilage at a rate of 1 μm/s. Data were recorded at each step over a period of 150–300 s. Once full relaxation occurred (load fluctuations <0.005 N over the final 60 s) during equilibrium, the load was recorded. The cartilage thickness at the test site was measured with a customized needle probe system. A fine needle was lowered into the cartilage at a constant rate and the applied load jumped when the needle contacted the subchondral bone. Cartilage thickness was read off from the displacement versus load graph. Four sets of readings were recorded for each sample. The Young's modulus (E) of the cartilage was calculated from the following equation taken from Hayes et al.,
32
with a Poisson ratio of 0.35 adopted for pig cartilage:
33
where P = equilibrium load, ν = Poisson ratio (0.35), a =radius of indenter, u = applied displacement, κ = theoretical scaling factor, dependent on ν and a/hc, and hc = thickness of cartilage.
Statistical analysis
The experimental procedure was repeated for six pigs in each group. The results were expressed in mean ± standard deviation and compared using Student's t-test. The difference was considered significant when p < 0.05.
Results
Cartilage repair
The animals grew over the 6-month period and gained an average of 111.7% in body weight. When the samples were extracted, the distal femur enlarged by 31.5% and 22.3% in the width of the medial condyle and patellar groove, respectively (Fig. 3). In groups A and C, only remnants of the electrospun mesh were found with the remains of the sutures that secured the membranes.

The enlargement of the distant femur over a period of 6 months. The weight of the pigs, width of the medial condyle, and width of the patellar groove were increased by an average of 111.7%, 31.5%, and 22.3%, respectively. Color images available online at www.liebertonline.com/ten.
A smooth articulating surface was restored in all groups as shown by the gross inspection of the medial condyle (Fig. 4). There was varying degrees of integration between the repair tissue and the host cartilage, with occasional fissures on the articulating surface (Fig. 4G, K). As the repair tissue was immature, it did not resemble the native hyaline cartilage with a regular cell orientation and the characteristic glass-like appearance of the mature hyaline extracellular matrix. The presence of glycosaminoglycan (GAG) in the neocartilage was detected via toluidine blue and a fully restored tidemark was found in only a few of group A and C samples but none in group B (Table 2). Both toluidine blue and safrannin O detect the presence of GAG, but the latter stained negatively at low GAG levels. 34 The surface of the neocartilage in C contained low levels of GAG and this observation was more predominant than in the other groups (Fig. 4S). Further, there was also an unexpected GAG reduction in the surrounding cartilage (five out of six group C samples). The development of fibrocartilage was accompanied by the deposition of collagen I and this protein was mainly detected in groups B and C (two and three out of six samples, respectively). Group A has the least fibrocartilage. The neocartilage stained positively for collagen II in all groups (Fig. 4U2–W2) and the repair cartilage bridged across the medial condyle defect for all samples.
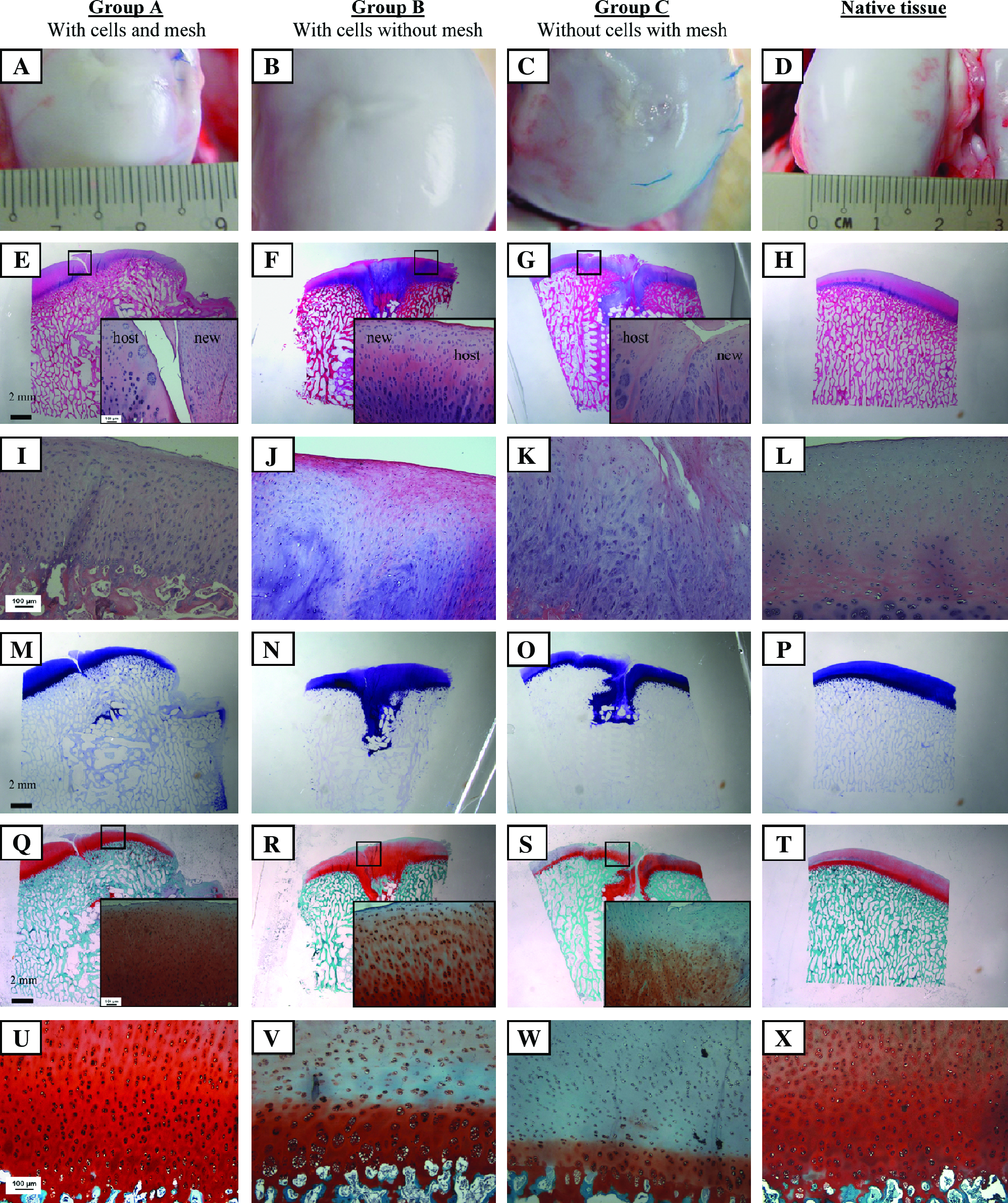
Cartilage repair at the medial condyle, 6 months postimplantation. Gross morphology (
GAG, glycosaminoglycan.
The patellar groove defect was barely distinguishable from the surrounding cartilage in group A as it was resurfaced by a smooth layer of reparative tissue (Fig. 5A). When the sections were examined, a mix of hyaline, fibrocartilage, and fibrous tissue was observed in all the three groups (Fig 5E–G). Surface restoration varied within each group as smooth and fibrillated morphologies were found (Fig. 5I–K). The cell orientation in the neocartilage differed from that of the native tissue and the repair at the defect periphery was better than that at the center where fibrous tissues would usually reside. This observation was supported by the poor toluidine blue staining, especially in groups B and C (Fig. 5M–O). GAG concentration in the neocartilage was lower than that in the native tissue for all samples (Fig. 5Q–S); moreover, it was depleted in the surrounding cartilage in B and C (three out of six for both groups), thus indicating degenerative changes. Collagen I and II were detected in all the specimens except for one group-A sample that stained negatively for collagen I (Fig. 5U1–W1). A complete bridging of the patellar groove defect as shown by the toluidine blue and collagen II stains was only accomplished for two out of six group-A samples but none for the other groups.
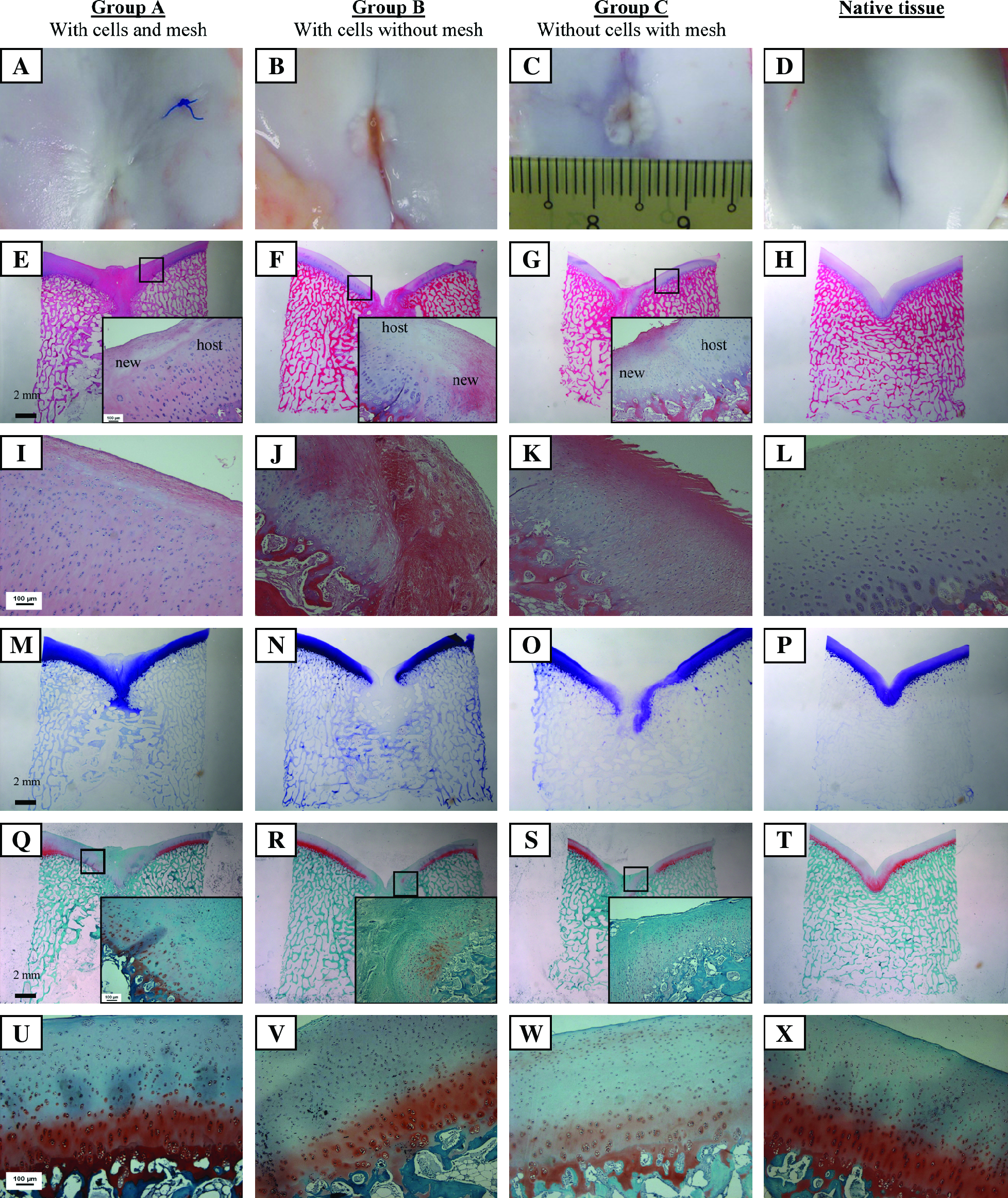
Cartilage repair at the patellar groove, 6 months postimplantation. Gross morphology (
Differences were noted in the cartilage repair between the two sites. This was validated by the significantly higher scores at the medial condyle when compared with the patellar groove (Fig. 6) and it was evident in terms of the hyaline content, cell morphology in the repair cartilage, and cartilage thickness. Moreover, there was no tidemark reconstitution in all the patellar groove defects (Table 2). When the three groups were compared, A tended to register a higher total score particularly so at the medial condyle. Further, the enhanced repair is mirrored by the superior scores for the hyaline content and the tissue morphology. This observation was supported by the key observations as tabulated in Table 2, which point to an improved outcome in A with a lower incident of fibrocartilage and better GAG maintenance in the host cartilage.

Mechanical evaluation and histological scoring of the repair cartilage. The relative Young's modulus and total O'Driscoll's histological scores are shown in (
The functionality of the regenerated cartilage was reflected by its Young's modulus. The relative Young's moduli of A and B at the medial condyle were significantly higher than that of C (Fig. 6). Further, the measured A and B values were approximately 70% of the Young's modulus of the native cartilage. At the patellar groove, A seemed to have a higher relative Young's modulus when compared with B and C. But there was an absence of statistical difference because of the considerable variation within each group. A comparison of the two anatomical sites revealed better functional restoration at the medial condyle and this was likely attributed to the unique biomechanical cues that stimulated tissue repair.
Cartilage healing was enhanced in the critically sized osteochondral defects through the use of the implanted MSCs and electrospun mesh. Group A exhibited a reduced occurrence of fibrocartilage with minimal GAG depletion in the surrounding cartilage when compared with B and C. Moreover, the patellar groove defect could only be bridged in A (two out of six samples), whereas gaps persisted in B and C. Tissue repair in C was solely dependent on the native progenitor cells, but unfortunately the quantity of these cells was insufficient to support an adequate repair as shown by the inferior morphological features and mechanical properties. To achieve optimal results, MSC implantation must be complemented by a resurfacing membrane as indicated by the improved outcomes in A when compared with B (Table 2). The mesh did not induce cartilage hypertrophy. Moreover, cell loss in the absence of the patch led to an inferior outcome in group B when compared with A. This was indicated by the prevalence of fibrocartilage and lower GAG distribution in B. However, a complete loss of the implanted MSCs was not proven in the absence of cell-tracking assays. Healing is not only dependent on the implant features but also on the intrinsic biomechanical interactions at the defect site. This was shown by the better regeneration at the medial condyle when compared with the patellar groove in all the groups, with an obvious discrepancy in the general histological features, scores, and indentation results.
Bone repair
Bone cavities were found in the region above the bone implant as shown in the micro-CT models, these were directly located beneath the cartilage zone and a visual assessment suggested larger cavities at the patellar groove (Fig. 7). Histological evaluation of the bone implants indicated bone ingrowth within the pores of the PCL–TCP scaffold, with dense bone infiltration in groups A and B, but it was notably reduced at the patellar groove when compared with the medial condyle. This was because the native trabeculae networks were denser at the medial condyle when compared with the patellar groove; hence, quantification with respect to the native site was required. Fibrous tissue was occasionally found in the implants, especially for group C (Fig. 7K, K1). In addition to the hematoxylin–eosin stain, Masson's trichrome was included for an indepth assessment of bone growth as it was able to differentiate old (red) from new bone (green). A mixture of old and new tissues suggested bone remodeling within the implant and this was observed for all the samples (Fig. 7M–O, M1–O1). The turnover process mirrored bone maturation as shown by the lamella rings. It appeared that the bone formation in A and B at both locations was accompanied by a higher proportion of old bone. When the native osteochondral tissues were examined (Fig. 7L, L1), skeletal growth was evident at both sites, given the remodeling was happening, particularly beneath the cartilage zone.
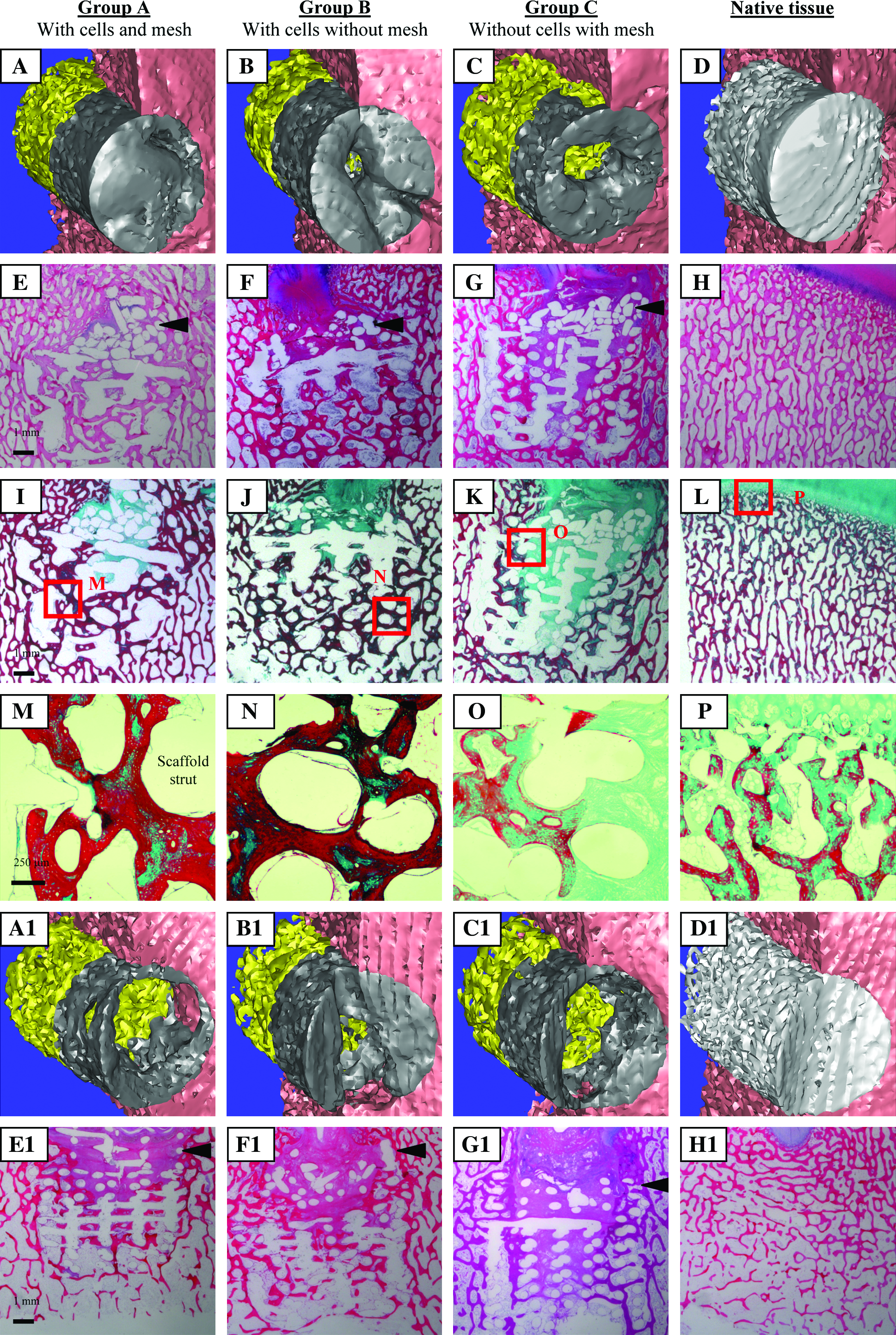
Bone repair at the medial condyle (
The nondestructive micro-CT evaluation of the bone defects was aided by the measurement of the degree of mineralization relative to the native bone volume fraction (88.6% and 47.3% at the medial condyle and patellar groove, respectively). When the three groups were compared, A and B were found to be more mineralized than C, above and within the bone implants and at both sites (Fig. 8). Bone repair in the absence of the implanted MSCs was unsatisfactory as the native cells were inadequate to support the healing at the critically sized bone defects. Group A generally have a higher degree of mineralization with respect to B, and thus it was probable that the electrospun mesh had helped to retain the implanted cells at the location where they were required for the reparative process. Mineralization above the bone implant was directly correlated to cavity size; hence, a lower value in C would imply a larger bone cavity when compared with the other groups. Similarly, the craters were larger at the patellar groove when compared with the medial condyle for all groups. Hence, the in vivo conditions at the patellar groove were adverse not only to cartilage repair but also to bone healing.
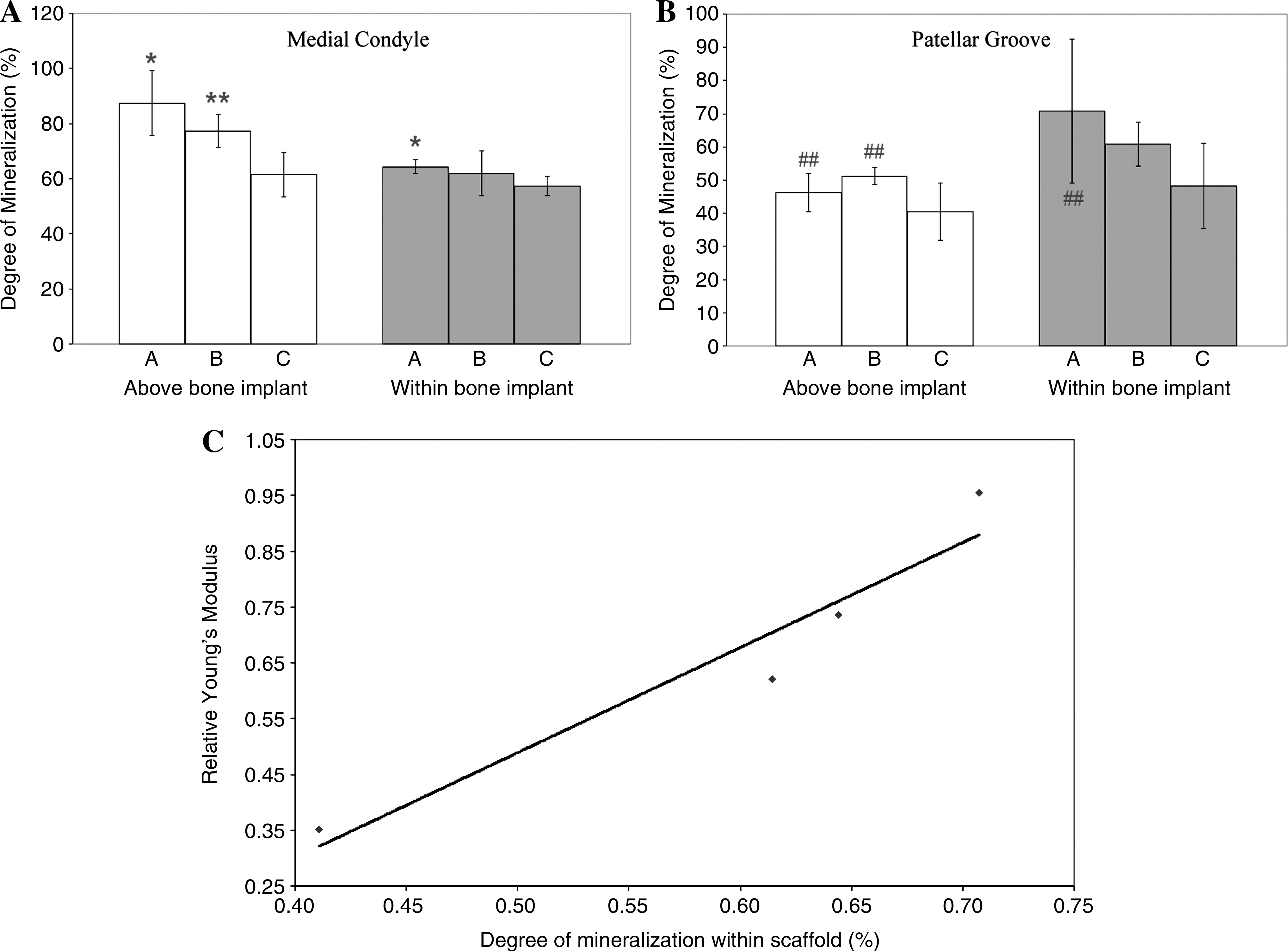
Bone mineralization and correlation with cartilage repair. The degree of mineralization was measured at the medial condyle (
A graphical plot between the degree of mineralization within the bone implant and the relative Young's modulus of the overlying cartilage revealed a positive correlation for all groups implanted at both locations (Fig. 8 and Table 3). This validated the long-held assumption that there was a close interaction in the healing of both tissues as cartilage repair was dependent on the underlying bone for support.
The results were not statistically significant (p > 0.05) as n = 4 was small.
Discussion
The implanted MSCs exerted a restorative effect at the osteochondral site. At the medial condyle of group C where these cells were omitted, a high incidence of fibrocartilage was found with the positive staining of collagen I and it was accompanied by GAG depletion at both the repair and surrounding cartilage. These anomalies led to a lower relative Young's modulus, thus compromising the load-bearing function of the new cartilage. The implantation of MSCs with the electrospun mesh supported cartilage repair in A. GAG loss in the host cartilage was minimized and more importantly the patellar groove defect was bridged by the repair cartilage for two out of six group-A specimens but not in B and C. The enhanced cartilage healing also meant better functional restoration as shown by the higher relative Young's modulus. The implanted MSCs have promoted bone regeneration. In their absence, large bone craters above the PCL–TCP implant were found in C at both sites as shown by the lower degree of mineralization. In addition, there was limited bone ingrowth within the bone construct as indicated by the histological and radiographical evidence. To realize the full restorative potential of the implanted MSCs, an adequate cell number must be maintained at the site, and this was achieved with the electrospun mesh, which prevented cell leakage. When cartilage regeneration was compared in A and B, the outcome in B was inferior given the prevalence of fibrocartilage and lower GAG distribution within and beyond the defect. Interestingly, these morphological observations at the patellar groove were similar for B and C despite the presence of implanted cells in the former (Table 2). Thus it was probable that cartilage regeneration at the patellar groove was difficult and a high cell number was crucial for effective healing, but this was hampered by the loss of seeded cells due to the omission of the electrospun mesh. These findings were reiterated at the bone region, as the degree of mineralization in A was generally higher than B. Hence, the electrospun mesh was deemed as a promising substitute for the periosteal graft. Although the natural graft was a source of cartilage and bone progenitor cells,35–37 donor-site morbidity and age-dependent quality were concerns. Graft harvesting entails extra incision, which inflicts scarring. But the main drawback of the periosteal patch was the high incidence of cartilage hypertrophy. This was likely due to the expression of VEGF, which induced vascularization and bone growth.22,24 Hence, a tissue-engineered alternative was proposed and a more stringent model was adopted by replacing the periosteal graft with an acellular electrospun PCL–collagen membrane. This permeable mesh facilitates nutrient exchange from the synovial space while preventing cell leakage and it did not provoke a hypertrophic reaction in the cartilage region. It was probable that the membrane could have hampered the migration of native reparative cells from the joint space. One of which is the synovial cells as observed by Hunziker et al. 38 Conversely, Hunziker et al. also acknowledged that synovial cells were unable to promote adequate cartilage repair unless stimulated by growth factors. 39 Synovial cell migration could have occurred in the absence of the electrospun membrane for group B, but the leakage of the implanted MSCs seemed to have outweighed the migration of these native cells, resulting in an insufficient number of reparative cells. This eventually led to the inferior outcome in B when compared with A.
The significance of cellular therapy toward osteochondral repair is fast gaining recognition. When cell-free implants were evaluated in the goat model, Kangarlu et al. discovered fibrous ingrowth at the defect site. 40 The results were improved in the pig model when Gotterbarm et al. added a growth factor cocktail to the cell-free construct. 41 Bone repair was satisfactory but the neocartilage exhibited a reduction in mechanical properties. 41 The experiment was repeated by Zhou et al. with chondrogenic induced MSCs. The seeded implant promoted both cartilage and bone repair when compared with the controls without cells that were invaded with fibrotic tissue. 5 These findings were also reported in other large animal models. Yamazoe et al. found that the implantation of MSCs with atelocollagen assisted bone repair in the canine osteochondral defect, 42 while Guo et al. reported that MSCs seeded within a TCP scaffold were able to promote cartilage growth with high GAG content in an ovine model. 43 The application of MSCs in musculoskeletal medicine is gaining popularity, given the inherent advantages. Bone marrow rich in MSCs could be obtained via a simple operative procedure, and subsequent expansion to achieve significant cell numbers for therapeutic use can be accomplished via monolayer culturing. Moreover, the differentiation potential of these cells, which includes osteogenic and chondrogenic lineages, is maintained during the expansion process. 44 Comparative studies between mature chondrocytes and MSCs have suggested a predominant fibrocartilage repair with chondrocytes but hyaline regeneration and improved host cartilage integration with MSCs.16,45 Wakitani et al. reasoned that during an osteochondral injury, potent cytokines were released and they primarily target the MSCs but not chondrocytes. 46 Their opinion was based on the poor response of chondrocytes, especially at the bone region where bone substitution was slow.46–49 Conversely, MSCs were able to assist bone healing by progressing rapidly through the chondrogenic lineage to hypertrophy and subsequently the hypertrophic tissue was vascularized and remodeled. 50
Osteochondral defects enlarge progressively into the surrounding tissue when they fail to heal. 51 When an injury disrupts the normal stress distribution at the cartilage zone, an elevation in compressive strains and loads occurs in the surrounding tissue, triggering a change in chondrocyte metabolism and eventual deterioration as indicated by the loss of GAG.52–54 Sams et al. discovered a 42% decline in the GAG content of the host cartilage when equine chondral defects were left to heal on their own. 55 But this loss was promptly reversed with cell implantation and the observation was similar to the current findings. It was interesting to note that severe cellular aberrations were hardly observed despite the reduced safranin O stain, which hinted of GAG depletion. A probable explanation would be that the loss of this key cartilage marker preceded critical abnormalities. To ensure normal load bearing at the defect site, GAG maintenance must occur with host tissue integration so as to prevent micro- and macromotion that disrupt the neotissue. 56 Cartilage integration was inconsistent in group A, which might be attributed to the limited involvement of the native chondrocytes during the repair phase. 57 But bonding can be improved with an enzymatic treatment of the defect site prior to implant placement.38,58
The histological scores did not indicate a significantly superior cartilage repair for any one group at both sites, although outstanding trends were highlighted by key observations (Table 2). This was attributed to several reasons. First, differences based on the scoring criteria were hardly noticeable between the groups as the repair was barely complete because tissue maturation was reported to last 6 months to 2 years.59–61 This was reinforced by the observation that the repair tissue resembled partially differentiated mesenchyme, which differed from mature hyaline cartilage that was characterized by a homogeneous extracellular matrix. 62 Additional complications arose when tissue regeneration was found to vary within and between the animals despite identical treatment. This fluctuation was noted in the cell morphology, host tissue integration, and surface and structural integrity of the repair cartilage at both sites.
The present implant was designed as a biphasic system consisting of a cartilage PCL scaffold and an osseous PCL–TCP matrix. Both phases were engineered with various mechanical, structural, and material considerations. The compressive Young's modulus and yield strength of the PCL cartilage scaffold were 15.7 and 2.12 MPa, respectively, whereas the PCL–TCP bone matrix has a stiffness of 124 MPa and a yield strength of 4.2 MPa. The stiffness of these scaffolds approximated to that of the respective tissues. The PCL–TCP matrix was implanted in the subchondral trabecular region and the yield strength was within that of the trabecular bone (0.85–13 MPa). 9 A mechanical comparison with cortical bone was omitted as the PCL–TCP scaffold was implanted in trabecular bone. Although the yield strength of the PCL scaffold was below that of cartilage, both were of the same order of magnitude and would suffice under contact stresses of 0.3–4.47 MPa as observed at the human knee joint.63,64 Besides biomechanical competence, scaffold porosity is crucial as it facilitated tissue repair. When the osteochondral defect was first created, a hematoma formed, which was entrapped within the pores of the matrices. The presence of growth factors within the clot would signal for the migration of the native progenitor cells required for tissue regeneration. Moreover, the fibrin matrix encapsulated within the polymeric scaffolds would also exert a reparative effect as witnessed by Paletta et al. 65 However, the inferior results in group C suggested that the native cells were insufficient for an effective repair, and hence, MSC implantation was necessary. The main advantage of the biphasic design would be the tailoring of the specific phases so as to cater to the regenerative needs of the different tissues located within the osteochondral defect. This was accomplished by using PCL-based materials. PCL demonstrated potential in cartilage and bone tissue engineering as it is a slow-degrading polymer that is able to provide prolong mechanical support at the load-bearing site.51,66 This support is critical during the remodeling and maturation of neotissues.67,68 The cartilage phase of the biphasic implant comprised of a PCL scaffold with the incorporation of TCP at the bone region. This bioactive ceramic was included as it not only enhanced the osteoconductivity and osteoinductivity of the bone matrix,69–71 but it also improved the stiffness of the scaffold. 68 Byrne et al. monitored the effects of scaffold stiffness (800–1200 MPa) on bone formation via computational simulation, and bone ingrowth was found to peak for the scaffold with the highest Young's modulus. The estimation was based on several assumptions, but it validated a positive correlation between bone regeneration and scaffold stiffness. 72 The observation was further reinforced when higher levels of alkaline phosphatase, osteocalcin, and bone sialoprotein were expressed by MC 3T3-E1 preosteoblastic cells that were cultured on a stiffer substrate (0.4 MPa) when compared with a similar material with a reduced stiffness of 0.01 MPa. 73 Substrate stiffness modulated osteogenic differentiation. 73 These in silico and in vitro evidences were reiterated in the experiment of subchondral bone matrices by Schlichting et al. 74 PLGA calcium sulfate scaffolds with a Young's modulus of either 95 or 150 MPa were implanted in sheep. 74 Different outcomes were observed, although the values were within the range of trabecular bone stiffness (4.4–229 MPa).8,9 Sclerotic bone enveloped the 95 MPa scaffold, whereas a higher Young's modulus was observed for the repair cartilage located above the 150 MPa matrix. The stiffer scaffold served as a stable substratum for cartilage repair while mechanical support was compromised by the reduction in scaffold stiffness, thus inducing bone sclerosis. 74 In the light of these biomechanical findings, bone regeneration was promoted by the addition of the TCP ceramic as it conferred an increase in the stiffness of PCL–TCP when compared with PCL. 68 Moreover, the positive correlation between the degree of mineralization within the bone scaffold and the relative Young's modulus of the overlying cartilage suggested that the optimal design of the bone matrix encouraged bone repair, which in turn promoted cartilage restoration. 57
Implant degradation occurred in the in vivo environment over 6 months. The electrospun mesh was completely degraded for most specimens while the structure of the PCL scaffold collapsed in several samples. The electrospun mesh served the intended function during the initial phase, given the improved results in group A over B, but joint articulation would have worn out over time. Although mechanically resilient, 68 cyclic compressive loading would have induced fatigue damage and microcracks, which accelerated the degradation of the cartilage PCL scaffold.75,76 The PCL–TCP scaffold appeared to be intact but scaffold degradation would certainly have occurred. A 33% degradation of a similar PCL–TCP scaffold was observed when it was implanted into a canine mandible defect for 6–9 months. 77 Polymer breakdown proceeded via hydrolytic surface erosion and enzymatic pathways. Further, the cyclic physiological loads would have hastened the process as a lower scaffold mass loss was observed at a subcutaneous site over a similar time frame. 78
Young pigs were selected for the study, as spontaneous healing was reported to be inadequate. Chang et al. noted the collapse of adjacent cartilage with the formation of subchondral cyst when osteochondral defects were left unattended in 4–8-month-old pigs. 2 Moreover, a seamless self-repair has not been reported even in young animals except for fetal lambs. 29 With this in mind, the experimentation of adult animals would only be warranted when preliminary findings were promising in young animals. 62 Moreover, the use of young animals in osteochondral regenerative studies modeled the condition osteochondritis dissecans, which is more prevalent among the adolescent than the elderly. 30 However, the use of skeletally immature pigs has drawbacks. In this study, the entire biphasic implant was embedded in the subchondral bone after 6 months as the joints enlarged during natural growth. Siegling et al. has reported in his landmark study that the growth of the epiphysis was initiated by cell proliferation in the articular cartilage and it was followed by endochondral ossification at the tidemark region. 79 Thus bone growth advanced beyond the PCL–TCP scaffold into the cartilage PCL matrix. As a result, the PCL scaffold was not integrated into the newly formed cartilage but it supported its development by acting as a cellular delivery vehicle.
Osteochondral restoration at the patellar groove was deficient when compared with the medial condyle as shown by the lower relative Young's modulus, histological scores, and the absence of tidemark. Further, all the medial condyle cartilage defects were bridged by the repair tissue, whereas osteochondral healing took place in only two group-A patellar groove samples. The degree of mineralization above the bone implant was generally poorer at the patellar groove and it implied a large bone crevice beneath the cartilage zone. The unsatisfactory osteochondral healing at the patellar groove could be attributed to the unfavorable in vivo loading conditions. When the human knee joint was examined during the walking gait, compressive loads measuring 0.2–0.4 times the body weight were observed at the patellar groove. However, the force increases to three and eight times the body weight during stairs ascent and squatting, respectively.80,81 On the other hand, the loading was more consistent at the medial condyle as it ranged from 2.4 to 3.4 times the body weight throughout the same set of activities.82,83 This constant moderate loading might have favored osteochondral repair but the fluctuating stresses at the patellar groove could have been detrimental. The prevalence of fibrocartilage and fibrous tissue hinted of high distortional shear stresses at the patellar groove, which stimulated the fibroblastic differentiation of MSCs. 84 Carter et al. have also highlighted that a low compression, high shear stress environment would predispose pluripotent cells to differentiate into fibrous tissue. Conversely, high compression and low shear encouraged cartilaginous development. 85 Hence, these in vivo biomechanical conditions might adversely affect the healing at the patellar groove and this might explain the discrepancy in osteochondral regeneration between the medial condyle and the patellar groove in pig, monkey, and goat as reported by other researchers.14,86,87 However, such findings were absent in the rabbit model because of the predominant squatting position.62,88
This work was a follow-up from a rabbit study. In the rabbit model, it was discovered that bone regeneration was equivalent with or without MSC implantation at 6 months. 89 Neither a PCL–collagen membrane nor a periosteal flap was used in this rabbit study. In the pig model, the implanted MSCs exerted a notable effect as the degree of bone mineralization was higher in group A when compared with C. Such differences would caution the translation of small animal modeling to clinical applications. The loss of seeded cells from the defect site could be prevented by a tissue-engineered patch that assisted both the cartilage and bone regeneration. By evaluating the two sites in the pig model, healing was not only dependent on exogenous factors but also on endogenous features such as the physiological loads at the defect site.
Conclusion
The tissue engineering of an osteochondral implant with a biphasic construct was investigated in the pig model and healing was found to be enhanced with seeded MSCs. The electrospun mesh also assisted tissue regeneration by preventing cell leakage. Favorable outcomes in the cartilage region were noted with the reduced incidence of fibrocartilage and improved GAG content when both the implanted cells and mesh were used. The bone phase also experienced a higher degree of mineralization, which facilitated the functional restoration of the overlying cartilage. However, osteochondral healing was not just dependent on the implant design but also on the in vivo conditions at the defect site as shown by the differing outcomes at the medial condyle and patellar groove.
Footnotes
Acknowledgments
The work was funded by A*star BMRC (grant R-397-000-038-305). The authors thank Yong Soon Chiong and Julee from the Department of Orthopaedics NUS, Song In Chin and Kiong Chin Yong from the Department of Experimental Surgery, Singapore General Hospital (SGH), for their valuable contributions.
Author Contribution
All authors have made substantial contributions to all of the following: (1) the conception and design of the study, acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; and (3) approval of the final version to be submitted.
Disclosure Statement
Each author confirms that neither this manuscript nor one with substantially similar content has been submitted, accepted, or published elsewhere (except as an abstract). There were no financial and personal relationships with other people or organizations that could inappropriately influence (bias) their work, and no potential conflicts of interest, including employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, and grants or other funding.