
Abstract
Tissue engineering approaches have been successfully used in repairing bone defects and have become a viable alternative to autologous bone. The aim of the present study was to investigate if a construct of porous beta-tricalcium phosphate (β-TCP) combined with osteogenically induced bone marrow stromal cells (bMSCs) could repair alveolar cleft, and allow for subsequent orthodontic tooth movement in a canine model. Twelve alveolar osteotomy surgeries in six animals were made bilaterally and randomly implanted by (1) tissue-engineered bone complex of bMSCs/β-TCP (group A, n=4), (2) β-TCP alone (group B, n=4), and (3) autologous bone obtained from iliac bone (group C, n=4). Contralateral alveolar defects were created in one animal and left untreated to serve as blank control to observe spontaneous healing of the defects. Sequential fluorescent labeling and radiographic observation was used to evaluate new bone formation and mineralization in each defect. Orthodontic tooth movement was initiated 8 weeks after surgical operation for 12 weeks, and then the dogs were sacrificed for histological and histomorphometric analysis. Results indicated that the tissue-engineered complex with bMSCs/β-TCP dramatically promoted new bone formation and mineralization and achieved a favorable height of the repaired alveolar when compared with β-TCP alone, which absorbed severely. The overall effect of the tissue-engineered bone was equivalent to autologous bone; the physiological function of the alveolar bone was restored by allowing the adjacent teeth to move into the newly formed bone in the grafted region. This study demonstrated that the tissue engineering bone from the combination of β-TCP and bMSCs is a feasible clinical approach for patients with alveolar cleft and the subsequent orthodontic tooth movement.
Introduction
Contemporary treatments of alveolar cleft defects involve surgical techniques that implant autologous bone grafts into the defect site. 7 Particulate cancellous bone harvested from the anterior iliac crest is most widely used for treating alveolar cleft and considered as the gold standard because of its osteoconductive, osteoinductive, and nonimmunogenic property.8,9 This technique, however, has several disadvantages, including early complications such as pain, bleeding, wound infection at the harvest site, as well as poor mobility, and the possibility of a fracture. Late complications, including chronic pain, and unaesthetic scarring at the harvest site, as well as gait disturbance, and paresthesia.10,11 Further, the autologous bone grafting has 15% or higher failure rates (depending on evaluation criteria),12,13 and increases the burden both for the patients and the healthcare system.
Tremendous efforts have been made to explore substitutes for autologous bone grafting. Numerous substitutes have been investigated, including the naturally derived biomaterials such as hyaluronic acid, and synthetic biomaterials such as hydroxyapatite (HA), beta-tricalcium phosphate (β-TCP), calcium phosphate ceramic, poly[D,L-(lactide-co-glycolide)], and collagen/HA composites.14–18 These substitutes may possess favorable osteoconductive characteristics (i.e., stimulation of endogenous osteoblasts and/or progenitor cells to migrate into defect region), but their limitation is intrinsic osteogenesis ability that compromises the desired clinical outcome for repairing bone defects. 12 Bone marrow stromal cells (bMSCs), which can be isolated from bone marrow, have the ability to differentiate into osteoblasts and form new bone.19,20 More importantly, it has been reported that bMSCs combined with scaffolds could repair bone defects in numerous animal models, including oral and maxillofacial defects.21–23 As an alternative strategy to improve the final outcome of patients with cleft alveolar, a tissue engineering approach in which the biomaterial substitutes are combined with osteogenic cells is presented in this study. A few case reports have been reported to date using tissue engineering techniques for repairing alveolar cleft.10,24,25 However, no adequate comparison of tissue engineering bone to autologous bone grafting was performed with regard to functional outcomes, such as moving of adjacent teeth to the grafted area to correctly line up the teeth. It is imperative to assess whether the newly formed bone would support the adjacent teeth beside the cleft to facilitate the orthodontic treatment. Thus, sequential systemic investigations are needed in preclinical models to explore if the newly formed bone could maintain the normal alveolar function.
In this study, we investigated the ability of a tissue-engineered bone. The tissue-engineered bone was fabricated by combining porous particulate β-TCP and autologous osteogenically induced bMSCs. We specifically explored if tissue-engineered bone in the alveolar cleft could function similarly to autologous bone grafting in terms of supporting the teeth movement adjacent to the cleft as a follow-up orthodontic procedure.
Materials and Methods
Animals
Seven 24-week-old male beagle dogs (weighing 8.0–9.5 kg) were used in this study. Twelve alveolar bone graft surgeries in six animals were made bilaterally and repaired randomly by the following three groups of materials—group A: tissue-engineered bone complex of bMSCs/β-TCP (n=4); group B: β-TCP alone (n=4); group C: autologous bone obtained from iliac bone (n=4). Bilateral alveolar defects in the rest of the animal were created and served as a blank control to observe if they could heal spontaneously during the experiment period. The experimental protocol was approved by the Animal Care and Experiment Committee of Ninth People's Hospital affiliated to Shanghai Jiao Tong University, School of Medicine.
Cell culture and osteogenic induction
Under general anesthesia with intramuscular ketamine (10 mg/kg), 3 mL of autologous bone marrow aspirate was obtained from the iliac crests of each dog with a heparinized 16 G biopsy needle and transferred into a sterile centrifuge tube. After washed with phosphate buffered saline (PBS) containing of 100 U/mL penicillin and 100 U/mL streptomycin, bone marrow samples were centrifuged at 1800 rpm for 10 min. Nucleated cells were seeded in 100 mm dishes in Dulbecco's modified Eagle's medium (Gibco) containing 10% (v/v) fetal bovine serum (FBS; Gibco), 100 U/mL penicillin, and 100 U/mL streptomycin, which was acted as a growth medium in present study, and incubated at 37°C under 95% humidity with 5% CO2. Nonadherent cells were removed from the culture during the medium changes twice every week. When cell colonies reached 70%–80% confluence, cells were detached with 0.25% trypsin/ethylenediaminetetraacetic acid and passaged. From passage 1, cells for osteogenic induction were cultured in the osteogenic medium (Dulbecco's modified Eagle's medium supplemented with 10% FBS, 10−8 M dexamethasone, 10 mM β-phosphoglycerol, and 50 mM L-2-ascorbic acid; Sigma). The cells after second passages were used for the following studies.
Osteogenic differentiation of bMSCs cultured in the osteogenic medium
Alkaline phosphatase (ALP) staining was tested after 7 days of culture in the osteogenic medium. The cells were fixed for 10 min at 4°C and then incubated with a mixture of naphthol AS–MX phosphate and fast blue BB salt (ALP kit; Hongqiao) according to Zhao et al. 26 The alizarin red staining was performed after 21 days of culture under the osteogenic medium. The cells were fixed with 10% formalin and stained with 40 mM alizarin red solution for 30 min at 37°C.
For assessment of quantitative ALP activity, the assay was conducted after 4 and 7 days of culture in either the growth medium or the osteogenic medium.27,28 Briefly, bMSCs in 24-well plates were washed twice with PBS and suspended in lysis buffer with 0.1 mL of 0.2% NP-40, and then the cells were mixed with 0.1 mL of 1 mg/mL p-nitrophenyl phosphate (Sigma) in 1 M diethanolamine buffer. After incubation at 37°C for 15 min, the reaction was stopped by the addition of 3 N NaOH. Enzyme activity was quantified by absorbance at 405 nm. Total protein content was determined with the Bradford method by using the Bio-Rad protein assay kit (Bio-Rad), and a series of bovine serum standards. ALP activity was normalized by the protein content and expressed as Abs/mg protein.
To detect mineralization, bMSCs on days 14 and 21 were washed five times in PBS and fixed in cold 70% ethanol for 1 h. The cells were washed three times with dH2O and stained with 40 mM alizarin red solution for 20 min at room temperature, and then the stain was desorbed with 10% cetylpyridinium chloride (Sigma) for 1 h. Finally, the dye was collected and mineralization was quantified by absorbance at 590 nm (Elx800; Bio-Tek) as described in previous study. 29 All experiments were done in triplicate.
Quantitative real-time polymerase chain reaction (PCR) assay was performed for osteoblast gene expression by using bMSCs cultured in either the growth medium or the osteogenic medium. Total RNA was isolated from cells at days 4 and 7, by using Trizol reagent (Invitrogen) according to the manufacturer's instruction. The RNA was used for synthesizing complementary DNA (cDNA) with PrimeScript 1st Strand cDNA Synthesis kit (TaKaRa). Real-time PCR analysis was performed with Bio-Rad real-time PCR system (MyiQ™; Bio-Rad) on markers of runt-related transcription factor 2 (Runx2), osteopontin (OPN), bone sialoprotein (BSP), and osteocalcin (OCN), with glyceraldehyde-3-phosphate dehydrogenase (GADPH) as the house-keeping gene for normalization. Primer sequences for Runx2, OPN, BSP, OCN, and GAPDH are listed in Table 1. All experiments were done in triplicate. The bMSCs cultured with the growth medium was used as a control.
BSP, bone sialoprotein; GAPDH, glyceraldehyde-3-phosphate dehydrogenase; OCN, osteocalcin; OPN, osteopontin; Runx2, runt-related transcription factor 2.
Cell seeding and osteogenic differentiation of bMSCs on β-TCP scaffolds
Sterilized particulate porous β-TCP with a diameter of 1.5–2.5 mm (Shanghai Bio-Lu Biomaterials Co. Ltd.) was used as scaffold. Cells cultured in either the growth medium or the osteogenic medium were detached from culture dishes using 0.25% trypsin/ethylenediaminetetraacetic acid, centrifuged, and then re-suspended in the medium without FBS at a density of 2×107 cells/mL, and then bMSCs suspension was dropped onto the β-TCP by means of the pipetting technique and incubated in the 24-well plate at 37°C for 4 h as previously described. 30 The bMSCs/β-TCP constructs were then cultured in the growth medium or osteogenic medium, correspondingly. Cell spreading on the scaffolds was detected under scanning electron microscopy (SEM; Philips SEM XL-30) at 4 days after cell seeding. While the osteogenic differentiation of bMSCs on β-TCP scaffolds was analyzed with ALP activity assay, quantitative alizarin red mineralization analysis, and quantitative real-time PCR analysis on the osteogenic marker of Runx2, OPN, BSP, and OCN as previously described. The tissue-engineered bone constructing with osteogenically induced bMSCs and β-TCP scaffolds was used for grafting in surgically created alveolar cleft sites.
Surgical procedure
The maxillary third incisors were extracted bilaterally for all animals under general anesthesia through intramuscular injection of ketamine (10 mg/kg), whereas a standard monitoring of general anesthesia was performed, and anesthesia was maintained with intravenous administration of ketamine during the entire course of surgery. Vertical incisions about 15 mm were made on the labial gingiva and mucous between the mesial of the second incisor and the distal of the canine. Full-thickness mucoperiosteal flaps of the labial and palatal were elevated to expose the alveolar crests bone. Alveolar defects (10×5×15 mm) extending to the nasal floor were made bilaterally by a round carbide bur with physiologic saline cooling between the second incisor and canine (Fig. 1). Great care was taken to avoid penetrations to the nasal floor and injuries to the second incisors. Grafts from different groups were transplanted to repair the alveolar defects. For the autologous bone grafts, an incision of 5 cm was made on top of the anterior iliac crest and cortico-cancellus bone blocks were harvested. Then, the wound was closed in layers. The animals were injected with penicillin for 1 week and kept on a soft diet during the study.

Surgically created alveolar cleft model in dogs was illustrated. Scheme was drawn to show the size and shape of the surgically created alveolar cleft
Orthodontic tooth movement and measurement of the tooth movement
Orthodontic tooth movement (distal movement of the first lateral incisor) was initiated 8 weeks after surgical operation using a segmental arch wire (0.018×0.025 inch rectangular stainless steel; 3M Unitek) with a nickel–titanium closed coil spring between the first lateral incisor and the canine. The canine was banded and a buccal tube was welded to the band, and the first lateral incisor was bonded with a 0.022×0.028 inch slot bracket (Fig. 2A). An applied force of 50 g was used and every 2 weeks the appliances were adjusted to avoid arch wire distortion to maintain the set force level. To eliminate occlusal interference, the height of the mandibular incisors and canines were reduced by a trepan bar. Orthodontic tooth movement was lasted for another 12 weeks and the dogs were sacrificed at 20 weeks after surgical operation. The orthodontic tooth movement was recorded with a dental model and measured by using a three-dimensional laser scanner (Laser-RE600; SEREIN). Briefly, the scanned models (before and after orthodontic tooth movement) were aligned on the same plane that was determined by the mesial cusps of the second premolas and the cutting edge of the central incisors. Based on this plane, a coordinate was created using the midline of the palate as X-axis and the line through the mesial cusps of the second premolas as Y-axis. The distance of the first lateral incisor before and after orthodontic tooth movement to the X-axis and Y-axis was measured and recorded as (Dx, Dy) and (Dx′, Dy′) (Fig. 2C1, C2). The tooth displacement was calculated using the formula as follows: D=√(Dx′ – Dx) 2 + (Dy – Dy′) 2 and compared.

Photograph of orthodontic tooth movement appliances. Orthodontic tooth movement was initiated 8 weeks after operation and the view immediately after bonding of the appliance was shown
Radiographic observation
Maxillary occlusal films were obtained with a dental X-ray machine (Trophy) under general anesthesia with ketamine as described previously, immediately after bone graft implantation, or at 4, 8, and 20 weeks after implantation, from a distance of 7 cm with an exposure time of 0.28 s (230 V, 8 mA). The height of the alveolar crest from each group was evaluated. Briefly, root length (from the enamelo-cemental junction to root apex) of the first lateral incisors in the occlusal films immediately after surgery and 20 weeks after implantation was measured, respectively, and recorded (L0, L1). L0/L1 ratio was calculated and adopted for the comparison to correct any possible projected deviations. Then, a circle was drawn with the anterior point of the apertura piriformis as the center with an image analysis system (Image-Pro Plus™; Media Cybernetic). The circle was tangent to the lowest point of the alveolar crest. The radius of the circle in the occlusal films at the time immediately after bone graft implantation and 20 weeks later was measured and recorded as the height of the alveolar crest (R0, R1). The ratio (R) of the maintained height of the residual alveolar crest compared with the height immediately after implantation surgery was calculated using the formula: R=(R1×L0/L1)/R0. A scheme was drawn to illustrate this method (Fig. 5E).
The method was adopted to reduce the interindividual angle deviations and avoid distortions possibly presented in radiographic photos.
Sequential fluorescent labeling
To observe the time course of new bone formation and mineralization, the animals were intraperitoneally injected with 25 mg/kg tetracycline (TE) hydrochloride (Sigma) at 4 weeks and 20 mg/kg calcein (CA; Sigma) at 12 weeks after the operation. Finally, 30 mg/kg alizarin red S (AL; Sigma) was administered 3 days before the animals were sacrificed at week 20 as previously described by Wang et al. 31
Sample preparation and histological and histomorphometric observation
The dogs were sacrificed at 20 weeks after implantation and the premaxillas were harvested and fixed in 4% buffered paraformaldehyde (pH 7.4) for 4 days. The central parts of the samples containing the first lateral incisor and the canine were dehydrated in ascending concentrations of alcohols from 75% to 100%. Finally, the samples were embedded in polymethylmethacrylate (Sigma) for 14 days before polymerization. The specimens were cut into 150-μm-thick sections using diamond-coated internal-hole saw microtome (Leica SP1600), and were subsequently ground and polished to a final thickness of about 50 μm for the observation of fluorescent labeling using a confocal laser scanning microscope (Leica TCS Sp2 AOBS). Excitation/emission wavelengths were used as follows: 405/580 nm (TE, yellow), 488/517 nm (CA, green), and 543/617 nm (AL, red). 32
To quantitate the bone formation and mineralization in the grafted alveolar, the fluorochrome staining of the same three locations, the top, middle, bottom of the central grafted area between the canine and the second incisor, were scanned, respectively. Five photographs were taken from the same area for each of the three positions: three fluorescence microscopy images including the fluorochromes TE, CA, and AL; one merging image of three fluorescent labeling to analyze mineralization of elevated alveolar ridge; and one image using transmission light microscopy without a specific filter combining the former merging image. Digital images of the microscope were stored and evaluated histomorphometrically using a picture-analysis system (Image-Pro Plus; Media Cybernetic). Using this system, the number of pixels labeled with each fluorochrome in each image was measured as a percentage of the mineralization area. This was done separately for yellow (TE), green (CA), and red (AL) and represented the bone formation and mineralization at the time 4, 12, and 20 weeks, postoperatively.
The undecalcified sections were further stained with Van Gieson's picro fuchsin for histological observation after fluorescent analysis. Three randomly selected sections from the serial mesio-distal sections of each sample were evaluated using image analysis system (Image-Pro Plus; Media Cybernetic). The percentage of newly formed bone and the residual β-TCP scaffold in the remaining grafted area was calculated at low magnification (12.5×).
Statistical analysis
All the data are presented as mean±standard deviation. Statistical analysis for osteogenic differentiation was performed by independent-samples t-tests, whereas the differences between groups A, B, and C were analyzed by analysis of variance and Student-Newman-Keuls (SNK) post hoc or Kruskal–Wallis nonparametric procedure followed by Mann–Whitney U-test for multiple comparisons based on the normal distribution and equal variance assumption test, at a significance level of p<0.05. Statistical analysis was performed using SPSS v.10.1 software (SPSS Inc.).
Results
Cell culture and osteogenic differentiation
Scattered bMSC colonies were observed after 5–7 days of culture after initial seeding, and the cells became confluent after ∼10–12 days. Cells were then passaged and cultured in the growth medium or osteogenic medium. The cells cultured in the osteogenic medium demonstrated stronger ALP staining at 7 days (Fig. 3A, B), and more pronounced alizarin red staining (Fig. 3C, D) at 21 days than the cells cultured in the growth medium. The quantitative analysis of ALP activity and mineralization also indicated an increase over time with higher values under the osteogenic medium (p<0.05; Fig. 3E, F). The real-time PCR results showed increased expression of osteogenic genes (Runx2, OPN, BSP, and OCN), at days 4 and 7 when cells were cultured in the osteogenic medium compared to those cultured in the growth medium (p<0.05; Fig. 3G–J).
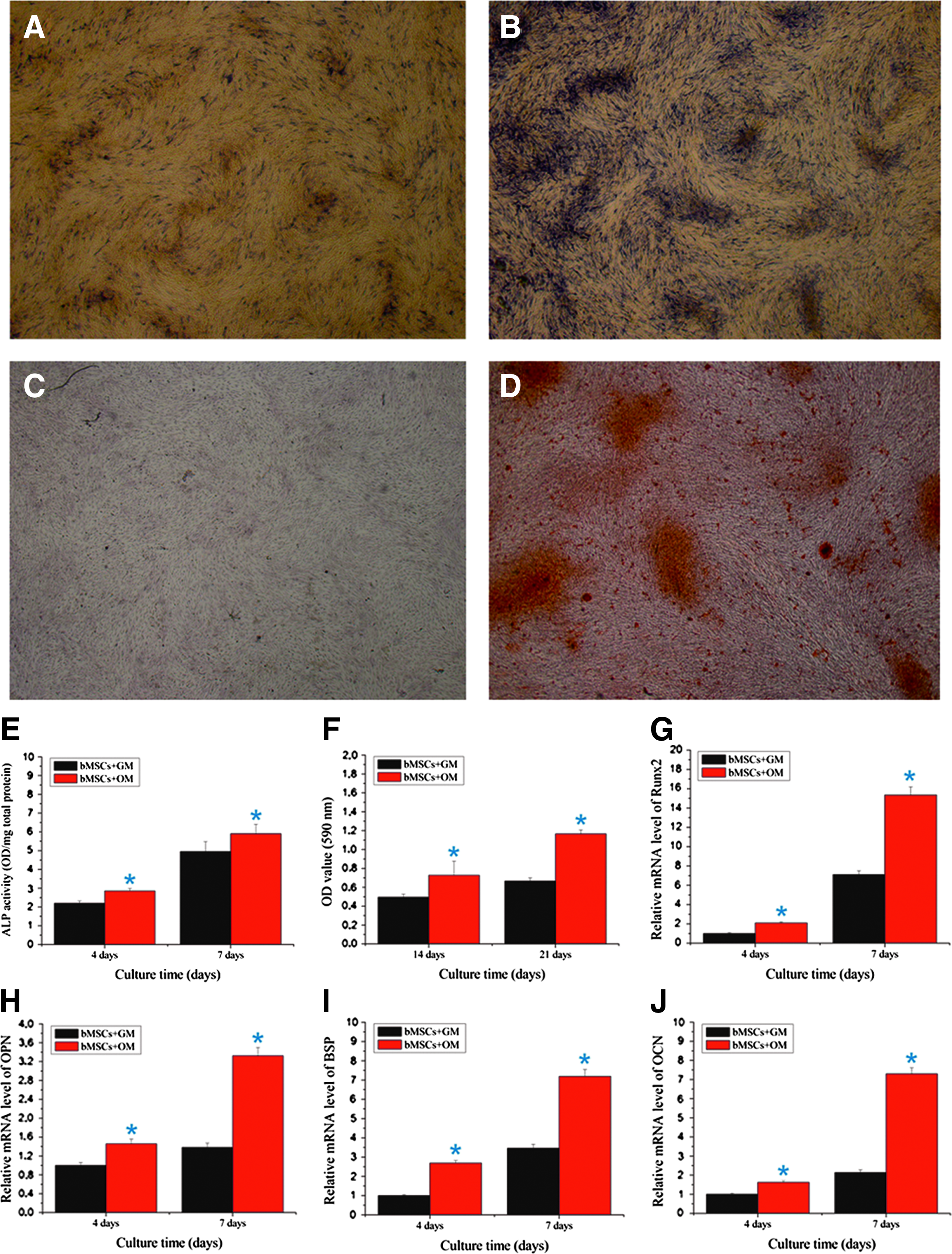
Osteogenic differentiation of bone marrow stromal cells (bMSCs) cultured in the growth medium (GM) or osteogenic medium (OM).
Cell seeding and osteogenic differentiation on β-TCP scaffolds
The interconnected porosity was evaluated using the SEM. The scaffolds had volume porosity of ∼70% with average pore diameter of 450±50 μm. The bMSCs could be seen spreading well on the inner surface of the scaffold in vitro 4 days after cell seeding (Fig. 4A, B). The results from the ALP activity assay, quantitative alizarin red mineralization, and quantitative real-time PCR analysis showed that the osteogenic differentiation of bMSCs on β-TCP scaffolds was significantly enhanced in the osteogenic medium as compared to the cells cultured in the growth medium. This better differentiation of bMSCs on β-TCP scaffolds under the osteogenic medium was consistent with the bMSCs cultured on Petri dishes (Fig. 4C–H). These results suggested that the biomaterial possessed favorable properties for cell attachment and differentiation and was suitable for further studies.

Spreading and osteogenic differentiation of bMSCs on beta-tricalcium phosphate (β-TCP).

Sequential occlusal radiographic findings of the repaired alveolar cleft, the images of
Gross observations and measurement of orthodontic tooth movement
All dogs heal uneventfully after surgery without infections and dehiscence of the grafted bone. There was only slight edema in the soft tissue but disappeared 2–3 days postsurgery. When orthodontic tooth movement initiated 8 weeks after surgery, spotted ulceration can be observed on the buccal mucosa due to friction with the bonded tooth movement appliances.
The first lateral incisors moved distally with a distance of 5.345±0.936, 6.986±1.412, and 4.665±0.483 mm in groups A, B, and C, respectively. There was a significant difference between group B versus group A or C (p<0.05), but no difference between group A and group C. This indicated that porous β-TCP with or without bMSCs did allow as much movement of the adjacent teeth into the repaired defects as the autologous bone.
Radiographic analyses
All the experimental areas in alveolar bone in the presurgery occlusal radiographs were uniform without missing teeth or pathological manifestations (Fig. 5A-1–D-1). In groups A and B, the alveolar defects were filled with radio-opaque particle materials immediately after implantation. The radiographic density of the graft sites was higher than the normal alveolar bone due to the radiopaque properties of β-TCP scaffold (Fig. 5A-2, B-2). At 4 weeks after implantation, the degradation of the grafted materials was evident, and the radio-density in the groups A and B is lower than the normal alveolar bone, indicating the resorption of the scaffolds (Fig. 5A-3, B-3). At 8 weeks, the radio-density of the grafted area was similar to the normal alveolar bone and the contour of the surgical created defect became distinguishable in group A (Fig. 5A-4). This was indicative of the new bone formation and remolding in this defect. Only a small radiopaque area could be observed in group B, and the radio-density of the grafted area was very low compared to the group A as well as the surrounding normal alveolar bone. The contours of the defect were clearly evident at that time (Fig. 5B-4). At 20 weeks, the first lateral incisor has been moved into the grafted area in group A. The periodontium of the tooth was considered well neither with periodontium hypertrophy nor sclerosis. There was complete bridging in the alveolar defect in this group. Cortical bone and cancellouse bone could also been seen in the defect area, making it indistinguishable from surrounding alveolar bone adjacent to the cleft (Fig. 5A-5). Although the tooth in group B has been also moved into the defect, there was not as much bone support for the tooth in the distal direction. The radio-density of the grated area remained relatively low, making the defect distinct from the surrounding alveolar bone (Fig. 5B-5).
In group C, the density of the grafted autologous bone was lower than that of groups A and B immediately after implantation, and the texture of the grafted bone was homogenous. The radio-density increased overtime, whereas the vertical height of the alveolar bone decreased. At 8 weeks, the grafted bone possessed normal architectures of the alveolar bone and it was difficult to discriminate the implant from the defect site (Fig. 5, C). In the blank control group, there was still a highly radiolucent area with a clear contour even 20 weeks after operation (Fig. 5, D).
The ratio of the residual alveolar height was calculated using the method described above, and the value was 73.60%±6.51%, 56.31%±7.72%, and 72.42%±8.72% for groups A, B, and C, respectively. The rate was significantly (p<0.05) lower in group B than in groups A and C. There was no significant difference between groups A and C, indicating that the tissue-engineered bone constructing with bMSCs/β-TCP could achieve an equivalent effect on maintaining alveolar height as the autologous bone.
Fluorochrome labeling analysis
New bone formation and mineralization at different time periods were analyzed by measuring different fluorescent labeling area. At 4 weeks after implantation, the percentage of TE labeling (yellow) in group A was 2.45%±0.82%, which was significant higher than that in group B at 1.43%±0.51% (Fig. 6A1–C1), but no significant difference was observed with group C at 1.98%±0.68% (Fig. 6D). There was also no significant difference between groups B and C (Fig. 6D). At 12 weeks, the percentage of CA labeling (green) was 2.27%±0.75%, 1.33%±0.56%, and 1.83%±0.83% for groups A, B, and C, respectively (Fig. 6A2–C2). There was significant difference between groups A and B, but no significant difference between groups A and C, or groups B and C (Fig. 6D). At 20 weeks, the percentage of AL labeling (red) was 1.66%±0.60%, 0.64%±0.39%, and 0.36%±0.11%, for groups A, B, and C, respectively (Fig. 6A3–C3). There was significant difference between groups A and B, or groups A and C, but no significant difference between groups B and C (Fig. 6D). These data indicated that when bMSCs were combined with β-TCP scaffold, there was a sustained bone formation and mineralization that was higher than the β-TCP scaffold alone throughout the experimental period. The autologous iliac bone remodeled significantly at an earlier stage; as evident from the fluorescent area and intensity at the graft area, the fluorescent labeling (red) was very little at 20 weeks after implantation, indicating low bone deposition at a later period.

Sequential fluorescent labeling of tetracycline (TE), calcein (CA), and AL administered at 4, 12, and 20 weeks separately was used to determine the rate of bone formation and mineralization. The images of
Histological and histomorphometric findings
Based on the light microscopy analysis of undecalcified specimens stained with Van Gieson's picro fuchsin, residual β-TCP was seen surrounded by the newly formed bone in the grafted region in groups A and B (Fig. 7A1, A2, B1, B2, C1, C2). The percentage of newly formed bone between the canine and the second lateral incisor was 54.98%±9.22% in group B, which was significantly lower than that in group A (70.79%±7.02%) and group C (78.68%±4.91%). There was no significant difference between groups A and C (Fig. 7D). The percentage of residual β-TCP in the remaining grafted region was 5.47%±1.32% in group A, and 5.17%±1.61% in group B; there was no significant difference between the two groups (Fig. 7E).

Microscopic view of bone formation in the grafted area from nondecalcified slices. The images of the representative slices surrounding the orthodontic moved first lateral incisor of three groups: groups A, B, and C
Discussion
This study was aimed at exploring whether a tissue-engineered bone from biodegradable β-TCP and bMSCs could be grafted in alveolar cleft and be as effective as a autologous bone graft for sequent orthodontic tooth movement.
Tissue engineering aims at developing substitutes for biological grafts by using scaffolds and seed cells. In the present study, bMSCs were selected as the cell source because they can be easily isolated from bone marrow aspirated from iliac crest and expanded, making large quantities available for transplantation. More importantly, based on the results of several assays intended for osteogenesis assessment (ALP activity, mineralization, and gene expression by PCR), bMSCs cultured in the osteogenic medium possessed the desired osteoblastic phenotypes, which ideally required for cells in bone regeneration.
The application of β-TCP as a clinical scaffold in repairing bone defects was well explored in recent years. Numerous studies have reported that the biocompatible and osteoconductive β-TCP scaffolds could support the attachment, proliferation, and differentiation of osteogenic cells (such as osteoblasts and bMSCs).27,33–36 In agreement with these literatures, the microscopy analysis of the bMSCs/β-TCP constructs in this study also showed that the cells could adhere to the surface of the scaffold, spread, and proliferate. As in regular culture on tissue culture plastic, the bMSCs cultured on β-TCP scaffold displayed the expected osteogenic activity when cultured in the osteogenic medium. This was evident on all of the parameters investigated (i.e., ALP activity, mineralization, and osteogenic gene expression), and suggested that β-TCP scaffold could act as a suitable three-dimensional matrix. The β-TCP was also reported to exhibit the appropriate strength to resist complicated pressures in the oral cavity, making β-TCP a good choice for the filling of bone defects in the alveolar region.15,31,37 Through this study, we extended the therapeutic applications of β-TCP and osteoinduced bMSCs in repairing bone defects such as alveolar cleft, specifically in supporting tooth movement in defect sites, which was attributed to the appropriate degradation of the scaffold to match with the new bone formation.
Beagle dogs were selected for this study since their periodontal structures and healing mechanisms are similar to those of humans.16,38 It was a prerequisite that the surgically created defects in this study (10×5×15 mm, extending to the nasal floor) would not heal spontaneously during the study period. This model was initially adopted previously by Hossain et al. 39 This study also confirmed the presence of highly radiolucent areas and bone discontinuity at the untreated blank controls until the end of the experiment (20 weeks), so that the defects were considered critical-sized.
In the case of alveolar cleft, an interteeth space exists between the central incisor and the canine after bone grafting so that orthodontic closure of the space is recommended for a better prognosis compared with prosthetic treatment. 13 However, orthodontic tooth movement can be performed to move the adjacent tooth into the cleft area to achieve occlusal reconstruction with patient's own teeth. Schultze-Mosgau et al. even reported significant lower resorption rates after bone grafting with subsequent orthodontic gap closures in comparison with gap openings (prosthodontic treatment), which suggested more favorable results for an orthodontic correction of the dental arch. 13 Some researches on orthodontic tooth movement after scaffold implantation was conducted previously.25,39 However, those studies did not specify the reasons for the timing of orthodontic tooth movement. The previous literatures stated that orthodontic manipulation should be done 3–6 months postoperatively when the graft had already well degraded, and there was no worry for any harmful effect to the root for the moved teeth.40,41 Based on the radiography findings in this study, most of the grafted materials already absorbed at 4 weeks after implantation, followed by obvious bone formation at 8 weeks in the tissue-engineered bone group. We therefore initiated orthodontic tooth movement at this point. The timing for initiating orthodontic tooth movement might be crucial to minimize any harm to the roots at early time points. 42 On the other hand, a late movement might cause less than desired bone formation to maintain the height of the repaired alveolar.43,44 Whether a movement earlier than the 4 weeks (significant β-TCP degradation was noticed) might be more beneficial needs exploration in the future.
Many controversies regarding the force magnitude and duration for tooth movement are hotly debated nowadays. 45 Researchers are now inclined to accept the view that the light and continuous force was appropriate for tooth movement and periodontal health. 46 In present study, the 50 g orthodontic force generated by nickel–titanium coil was considered continuous and relatively light for tooth movement. After 12 weeks of orthodontic tooth movement, the first lateral incisors were moved into the defect areas in all groups without obvious root resorption or other side effects. To determine the height of the grafted alveolar, multiple clinical and radiological schemes have been proposed.47–51 In this study, the vertex of apertura piriformis was used as a criterion to evaluate the lowest point of the alveolar so as to establish a reproducible quantitative standard, making comparison consistent, since apertura piriformis is a relative stable anatomical landmark.
The study showed that in β-TCP group after 4 weeks, significant resorption was underwent based on the appearance of radiolucent area inside the graft. This phenomenon continued at 8 weeks with a decreased density of the grafted area. Till 20 weeks, there was only small amount augmented alveolar ridge remained with a lower radiopacity. In the tissue-engineered bone group, the resorption of the scaffold was also evident at 4 weeks; however, the radiopacity of the grafted region began to increase from week 8, and the augmented alveolar ridge maximally maintained the original height with a higher radiopacity at week 20, which was comparable to autologous bone. Although the orthodontic tooth movement was quicker in group B than in group A or C, the occlusal radiograph and sequential fluorescent labeling findings demonstrated a lower rate of bone formation and mineralization in group B than in group A, which has further led to a smaller percentage of bone area and less alveolar support to the teeth adjacent to the cleft. Since the percentage of the remaining β-TCP scaffold was similar in groups A and B, the faster tooth movement in group B was most likely due to the lower resistance with less bony support inside the defects. Unfortunately, less alveolar support in the long-term will have serious adverse effects on teeth stability in the maxillary segment.43,47 However, β-TCP could serve as an suitable scaffold for bMSCs seeding, and the rate of bone formation and mineralization increased substantially with the incorporation of osteoinduced bMSCs. Further research is still needed to improve the effects of alveolar cleft repairing. Suitable solutions for grafting include combinations with biological molecules (i.e., bone morphogenetic proteins) to boost osteogenesis and osteoinduction in the repaired region. In addition, scaffolds that can provide more controllable degradation kinetics, such as β-TCP/HA or organic/inorganic composites, which led to better repair of alveolar cleft and improved tooth movement, might be explored in further study. As for an orthodontist, the optimal timing for orthodontic tooth movement after bone graft implantation to achieve better effect in patients with alveolar cleft is also important, since appropriate initial functional stimulation might be vital for the success of implanted bone graft. 43
Conclusion
This study demonstrated the feasibility of using tissue-engineered bone constructs with β-TCP and bMSCs to repair alveolar cleft. The construct dramatically promoted new bone formation and mineralization, and achieved a favorable height of the repaired alveolar when compared with β-TCP implants alone, which resorbed severely during the 20-week study period. The functional effects of the tissue-engineered bone were equivalent to autologous bone and the induced tissue could support the physiological function of the alveolar by allowing the adjacent teeth to move into the newly formed bone in the grafted region. This study demonstrated that the tissue-engineered bone combining with β-TCP and bMSCs might be a feasible clinical approach as a substitute for bone grafts for patients with alveolar cleft and consequently orthodontic teeth movement.
Footnotes
Acknowledgments
This work was supported by National Science Foundation of China (30772431 and 30973324); Program for New Century Excellent Talents in University (NCET-08-0353); Science and Technology Commission of Shanghai Municipality (08QH14017, 08410706400, 0952nm04000, 10430710900, and 10DZ2211600); and Shanghai Education Committee (07SG19).
Disclosure Statement
No competing financial interests exist.