
Abstract
Microfracture of cartilage induces migration of bone-marrow-derived mesenchymal stem cells. However, this treatment often results in fibrocartilage regeneration. Growth factors such as bone morphogenetic protein (BMP)-2 induce the differentiation of bone-marrow-derived mesenchymal stem cells into chondrocytes, which can be used for hyaline cartilage regeneration. Here, we tested the hypothesis that long-term delivery of BMP-2 to cartilage defects subjected to microfracture results in regeneration of high-quality hyaline-like cartilage, as opposed to short-term delivery of BMP-2 or no BMP-2 delivery. Heparin-conjugated fibrin (HCF) and normal fibrin were used as carriers for the long- and short-term delivery of BMP-2, respectively. Rabbit articular cartilage defects were treated with microfracture combined with one of the following: no treatment, fibrin, short-term delivery of BMP-2, HCF, or long-term delivery of BMP-2. Eight weeks after treatment, histological analysis revealed that the long-term delivery of BMP-2 group (microfracture + HCF + BMP-2) showed the most staining with alcian blue. A biochemical assay, real-time polymerase chain reaction assay and Western blot analysis all revealed that the long-term delivery of BMP-2 group had the highest glucosaminoglycan content as well as the highest expression level of collagen type II. Taken together, the long-term delivery of BMP-2 to cartilage defects subjected to microfracture resulted in regeneration of hyaline-like cartilage, as opposed to short-term delivery or no BMP-2 delivery. Therefore, this method could be more convenient for hyaline cartilage regeneration than autologous chondrocyte implantation due to its less invasive nature and lack of cell implantation.
Introduction
One method for articular cartilage repair that does not involve cell implantation is marrow stimulation using subchondral bone. 4 In this procedure, bone-marrow-derived stem cells (BMSCs) are stimulated to migrate from the subchondral bone to the site of cartilage defect. However, microfracture often results in regeneration of fibrocartilage, which contains less proteoglycan and more type I collagen with inferior mechanical properties, rather than the formation of desired hyaline cartilage. 5 Fibrocartilage regeneration by microfracture could be due to failure of chondrogenic differentiation of recruited BMSCs. An appropriate stimulus for the chondrogenic differentiation of recruited BMSCs could induce hyaline cartilage regeneration mediated by microfracture. To enhance the quality of cartilage regenerated by microfracture, hyaluronic acid, which is known to induce chondrogenic differentiation of BMSCs, was applied to the defects. 6 However, this study did not demonstrate statistically significant improvement in the quality of regenerated cartilage. 4 Application of growth factors could also improve the quality of the cartilage regenerated by microfracture. Bone morphogenetic proteins (BMPs), including BMP-2, -4, -6, and -7, have been shown to promote chondrogenic differentiation of BMSCs.7–10 BMP-2 stimulates the in vitro synthesis of chondrocytic matrix components, such as proteoglycans and type II collagen. 11 Delivery of BMPs to BMSCs migrating from bone marrow to cartilage defect sites by microfracture could induce the chondrogenic differentiation of the BMSCs (Fig. 1), resulting in regeneration of hyaline cartilage rather than fibrocartilage. A study showed that BMP-7 improves the histological quality of cartilage regenerated by microfracture 12 but did not show quantitative improvement in the quality of the regenerated cartilage.

A diagram describing a hypothesis of hyaline cartilage regeneration by combined therapy of microfracture and a long-term delivery of bone morphogenetic protein (BMP)-2. Articular cartilage defect is treated with microfracture followed by BMP-2 delivery using heparin-conjugated fibrin (HCF). Bone-marrow-derived stem cells are recruited to the cartilage defect site by microfracture and may be induced to undergo chondrogenic differentiation, produce cartilage extracellular matrices, and regenerate hyaline cartilage. Color images available online at www.liebertonline.com/tea
Despite the chondrogenic efficacy of BMPs, a problem still remains regarding their clinical treatment. Due to their short half-life, BMPs administrated in solution may be decreased in bioactivity over a short period. 13 In the present study, we hypothesized that the sustained delivery of BMP-2 to articular cartilage defects subjected to microfracture would result in more regeneration of hyaline-like cartilage compared to short-term delivery of BMP-2 or no BMP-2 delivery. Heparin-conjugated fibrin (HCF) 14 and normal fibrin were utilized as long-term and short-term delivery vehicles, respectively. Since BMP-2 electrostatically interacts with heparin, HCF would induce sustained release of BMP-2 14 and maintenance of BMP-2 activity. 15 Rabbit articular cartilage defects were subjected to microfracture and one of the following: no treatment, fibrin, short-term delivery of BMP-2, HCF, and long-term delivery of BMP-2. Eight weeks after treatment, qualitative (histological analysis and Western blot assay) and quantitative (biochemical assay and real-time polymerase chain reaction [PCR] assay) evaluations on extracellular matrices of the regenerated cartilage were performed.
Materials and Methods
Preparation and characterization of heparin-conjugated fibrinogen
Heparin-conjugated fibrinogen was prepared using standard carbodiimide chemistry as described previously. 16 Plasminogen-free fibrinogen (Sigma, St. Louis, MO) from pooled human plasma was covalently reacted with heparin (molecular weight=4,000–6,000; Sigma). Heparin (100 mg) was dissolved in a buffer solution (100 mL, pH 6) of 0.05 M 2-morpholinoethanesulfonic acid (Sigma). N-hydroxysuccinimide (0.04 mM; Sigma) and 1-ethyl-3-(3-dimethylaminopropyl)-carbodiimide hydrochloride (0.08 mM; Sigma) were added to the solution to activate the carboxylic acid groups of the heparin. After 12 h of reaction at 4°C, the solution was stirred to obtain a homogeneous solution. The product was precipitated with excess anhydrous acetone and lyophilized. Fibrinogen (100 mg) was dissolved in phosphate-buffered saline (PBS, 20 mL, pH 7.4) without bubbling at 4°C and reacted with the activated carboxyl acid groups of heparin (60 mg) under the same conditions for 3 h. The product was precipitated with a large excess of acetone and lyophilized. The resultant white powder was completely dissolved in PBS and dialyzed through a porous membrane bag (12,000–14,000 Da molecular weight cut-off; Spectrum Lab Inc., Greensboro, NC) to remove residual heparin at 4°C for 24 h. Finally, HCF was lyophilized for 48 h.
The surface charge of HCF and fibrin in PBS solutions were determined using zeta potential analyzer (Zetasizer 3000HS, Malvern, United Kingdom). The amount of heparin conjugated to fibrinogen in HCF was determined with the toluidine blue O method, as previously described. 16 To evaluate in vivo degradation rate of HCF and fibrin, 4-week-old female athymic mice (20–25 g body weight; Orient, Seoul, Korea) were anesthetized with xylazine (10 mg/kg) and ketamine (100 mg/kg), and 200 μL of either HCF or fibrin (n=8 for each group) was implanted into dorsal subcutaneous space of the athymic mice for 9 days.
In vitro BMP-2 release kinetics
The kinetics of BMP-2 release from fibrin or HCF were determined by enzyme-linked immunosorption assay. Normal fibrin containing free heparin was prepared by mixing heparin mixed in normal fibrinogen (100 mg/mL) dissolved in aprotinin (100 KIU/mL) solution and thrombin (500 IU) dissolved in calcium chloride solution (6 mg/mL). HCF was formed by mixing heparin-conjugated fibrinogen (40 mg/mL) and normal fibrinogen (60 mg/mL) dissolved in aprotinin solution and thrombin dissolved in calcium chloride solution (6 mg/mL). Fibrin (250 μL) or heparin-conjugated fibrinogen (250 μL) containing 3 μg of BMP-2 (R&D Systems, Minneapolis, MN) mixed with thrombin (250 μL) for preparation of 500 μL gel. Each delivery system containing BMP-2 (n=5 per group) was immerged in a 2 mL microcentrifuge tube containing 1.5 mL of PBS and then incubated at 37°C with continuous agitation. At various time points, the supernatant was collected, after which the microcentrifuge tubes were replenished with fresh buffer. The amounts of BMP-2 in the supernatants were determined using an enzyme-linked immunosorption assay kit (Human BMP-2 Quantikine®; R&D Systems).
Animal surgery and treatments
New Zealand white rabbits (3–6 months old, body weight 2.5–3.5 kg; Jung-Ang Lab Animal, Seoul, Korea) were anesthetized by intramuscular injection of ketamine hydrochloride (250 mg, Ketara; Yuhan Co., Seoul, Korea), xylazine hydrochloride (35 mg, Rompun; Bayer, Seoul, Korea), and 10 mg of acepromizine (Yuhan Co.). After shaving, disinfection, and draping, the left knee was opened by an anteromedial parapatellar incision and the patella was everted. A full-thickness articular cartilage defect (3×6 mm, 1 mm in depth) was created by corneal trephine in the trochlear groove of the left distal femur (Fig. 2A). Using a sterilized 0.03-inch Kirschner wire (Sanatmetal Co., EGER, Hungary), meticulous subchondral penetration was introduced to the defects (Fig. 2B). Four holes were made in each defect without violation of neighboring holes. The debris was completely removed and hemostasis was achieved. Forty-eight rabbit knee joints were divided into six groups (n=8 per group). Rabbit articular cartilage defects were subjected to microfracture and one of the following: no treatment (MF group), fibrin (F group), BMP-2 delivery using fibrin (MF + F + BMP-2 group), HCF (MF + HCF group), and BMP-2 delivery using HCF (MF + HCF + BMP-2 group). For BMP-2 (3 μg per defect) delivery, either fibrin or HCF containing BMP-2 was mixed with thrombin solution at 1:1 volume ratio. In the no treatment group, cartilage defects were not subjected to microfracture or other treatments. Wound closure was performed in layers. All rabbits were treated with antibiotics (gentamycin) for 3 days postoperatively and then sacrificed by CO2 asphyxiation at 8 weeks for analysis. The repaired tissues were cut in half and used for histological analysis (n=4), glucosaminoglycan (GAG) content analysis (n=4), real-time PCR analysis (n=4), and Western blot analysis (n=4). The animal study was approved by the Institutional Animal Care and Use Committee at Seoul National University (#SNU100607-5).
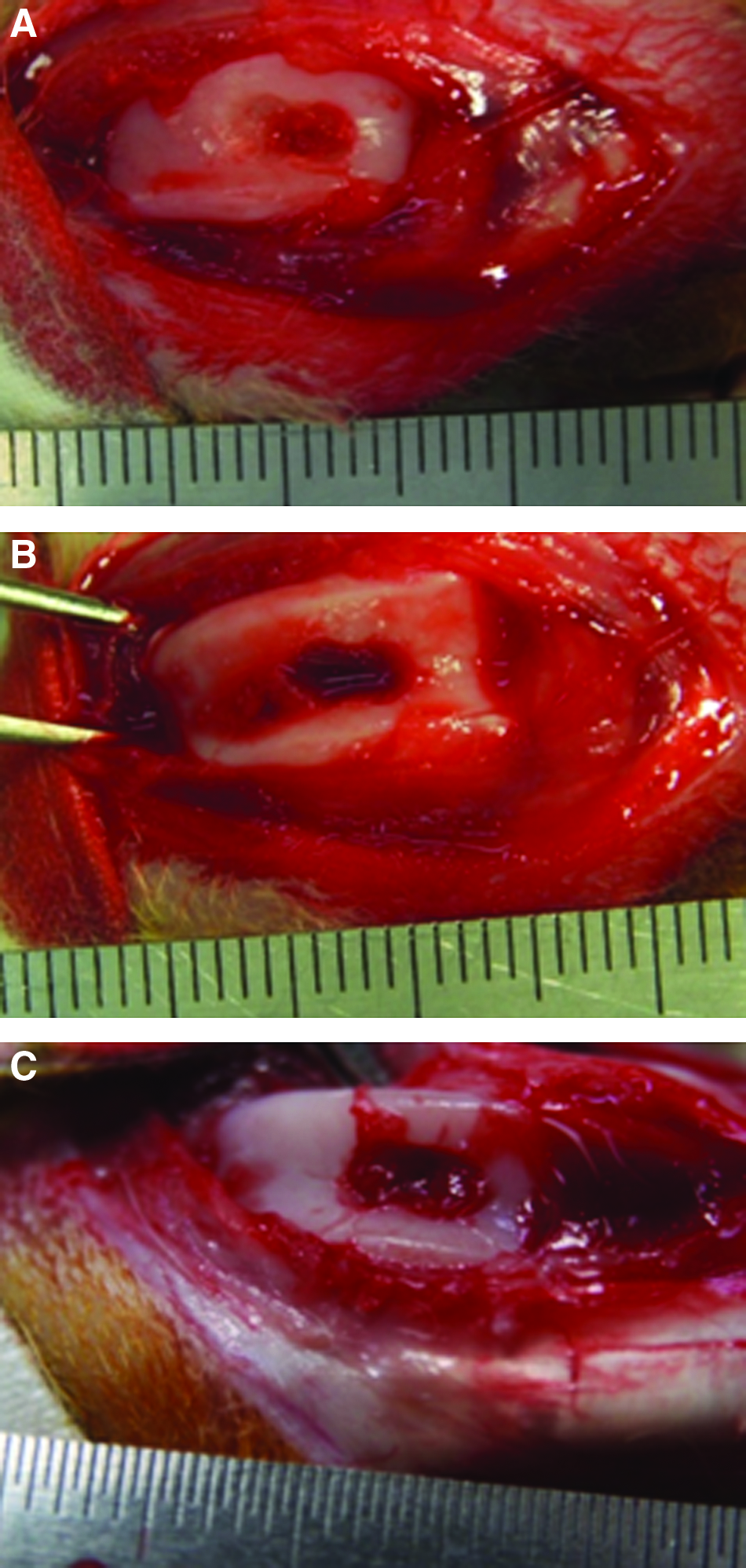
Photographs of rabbit knee articular cartilage defect treatment.
Gross appearance
Eight weeks after treatment, the joint and synovium were examined grossly. The percentage of regenerated surface area was determined with Adobe Photoshop software (Adobe Systems Inc., San Jose, CA). 17 The defect area at the time of surgery (original defect area) as well as the defect area at the time of sacrifice was determined. The percentage of regenerated surface area was calculated using the following equation: percentage of regenerated surface area=[(original defect area) – (defect area at sacrifice)/(original defect area)×100].
Histological analysis
The trochlear grooves were retrieved for analysis. All specimens were fixed in 10% (v/v) buffered formalin for 48 h, decalcified in 10% (v/v) formic acid for 48 h, and then extensively washed in water. The specimens were dehydrated with a graded ethanol series and embedded in paraffin. The midportion of the specimens were sliced into 4-μm-thick sections and stained with alcian blue to evaluate GAG deposition. All samples were examined under histomophometric analysis by observers. For each of the grading scales, all samples were examined three times by the observers. The observers consisted of pathology researchers with different levels of examine and grade the samples according to the grading systems. The scoring systems suggested by O'Driscoll et al. was determined from linear regression analysis of the average scores for each cartilage sample. 18 All samples were presented to the observers in a blinded and random order.
GAG content analysis
The regenerated tissues (n=4) were digested in 1 mL of 0.5% papain in PBS for 1 h at 65°C. An aliquot of the papain digest was assayed for total GAG content by the addition of dimethylmethylene blue dye solution. 19 Briefly, 50 μL of each papain-digested sample was incubated with 5 mL of dimethylmethylene blue dye, and the reaction was observed using a spectrophotometer at 525 nm. The amount of GAG was extrapolated from a standard curve using shark chondroitin sulfate (Sigma).
Real-time PCR and Western blots
Total RNA were extracted from the regenerated tissues obtained from cartilage defect sites (n=4). The expression of collagen type I and collagen type II was measured by quantitative real-time-PCR, which was performed using LightCycler® 1.5 instrument (Roche Diagnostics Co., Indianapolis, IN) with Universal prove library probe (Roche Diagnostics Co.). Each cycle consisted of the following times and temperatures: 94°C for 40 s, 60°C for 30 s, and 72°C for 30 s. Primers specific to rabbit GAPDH were of the following sequences: 5′-CTC TCT CAA GAT TGT CAG CAA C-3′ (forward) and 5′-CAC AAT GCC GAA GTG GTC GT-3′ (reverse). Primers specific for rabbit collagen type I had the following sequences: 5′-AGG GAG AGC CTG GTG ACA A-3′ (forward) and 5′-GAA GAC CTT GCA ATC CGT TG-3′ (reverse). Primers specific to rabbit collagen type II were of the following sequences: 5′-ACA GCA GGT TCA CCT ATA CCG-3′ (forward) and 5′-CCC ACT TAC CGG TGT GTT TC-3′ (reverse). Primers specific to rabbit collagen type X had the following sequences: 5′-CAG GAC CAG CTG GCA TTT-3′ (forward) and 5′-GGG CTC CTG TAA GTC CCT GT-3′ (reverse). Western blot analysis was carried out with 10% sodium dodecyl sulfate–polyacrylamide gel electrophoresis. After proteins were transferred to an Immobilon-P membrane (Millipore Corp., Billerica, MA), they were probed with polyclonal antibodies against collagen type I and II (Abcam, Cambridge, MA), followed by incubation with horseradish peroxidase-conjugated anti-rabbit antibodies (1:5000; Santa Cruz Biotechnology, Santa Cruz, CA) for 1 h at room temperature. The blots were developed using an enhanced chemiluminescence detection method (Amersham Bioscience, Piscataway, NJ).
Statistical analysis
All quantitative data were expressed as the mean±standard deviation. A one-way analysis of variance using the Bonferroni test was performed on samples to determine significant differences. The assumptions for analysis of variance were found to satisfy Levene's test for homogeneity of variance. A value of p<0.05 was considered statistically significant.
Results
Characterization of HCF
Zeta potentials at pH 7.4 of HCF and fibrin were −48.4±2.3 and −32.5±2.1 mV, respectively. The amount of heparin conjugated to fibrinogen in HCF was 42.7 mg/g fibrinogen. The in vivo degradation rate of HCF was significantly slower than that of fibrin (Fig. 3). At various time points, animals were sacrificed, and the implants were retrieved. The volumes of the retrieved implants were measured by immersing the implants in physiological saline in a graded pipette. To minimize possible saline absorption into the implants, the volume change was measured instantly.
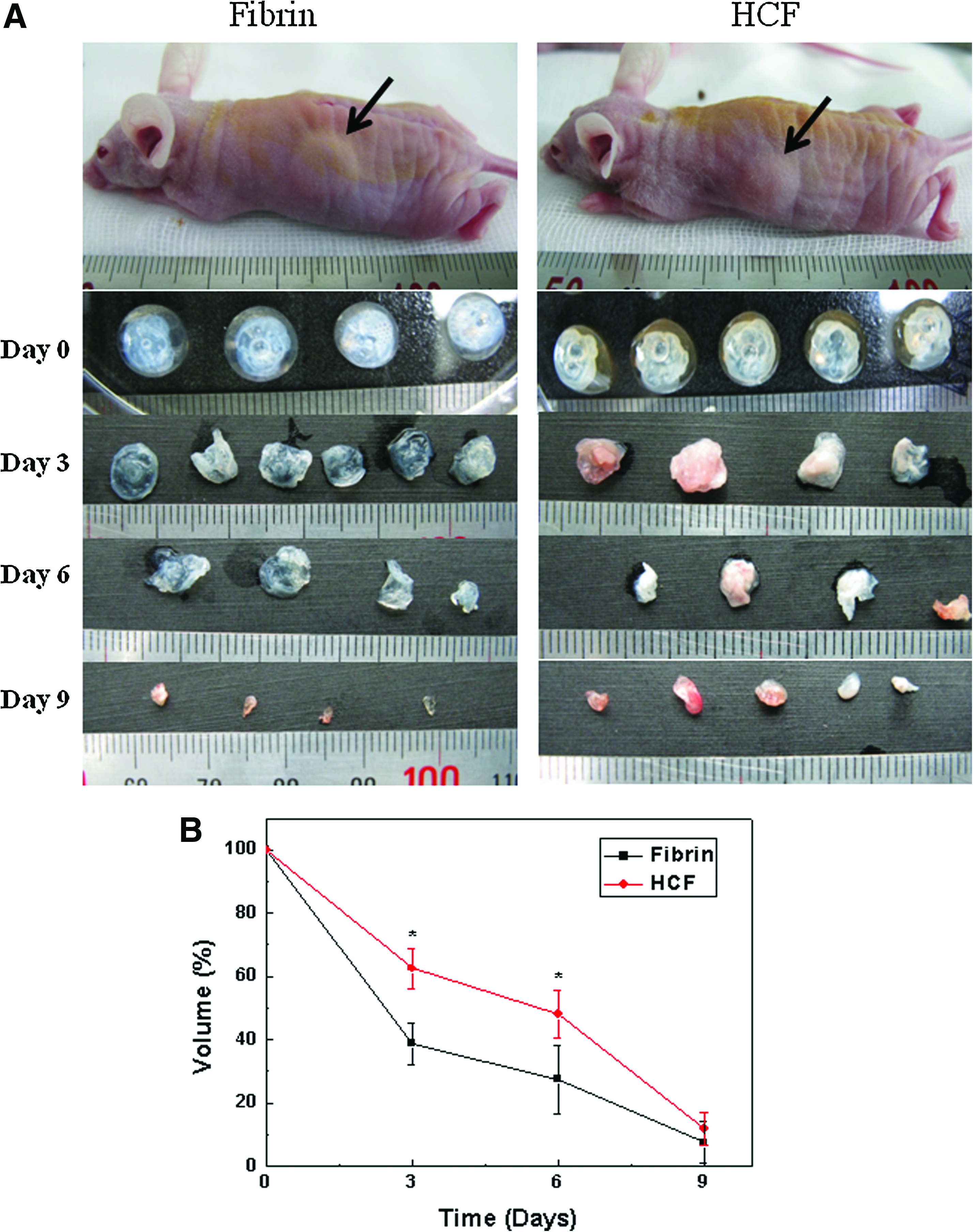
In vivo degradation of HCF and fibrin that were implanted to subcutaneous space of mice for 9 days.
In vitro BMP-2 release kinetics
The in vitro BMP-2 release kinetics for the two delivery systems (fibrin and HCF) were compared. The initial burst release and release period dramatically differed between the two delivery systems (Fig. 4). The initial burst release for the first 12 h from fibrin was 61.1%±5.4%, whereas that from HCF was only 28.6%±6.2%. The percentage of loaded BMP-2 released from fibrin was 87.8%±7.5% during the first 3 days. In contrast, 81.8%±5.4% was released from HCF over 13 days.

Profiles of the amount of BMP-2 remaining in fibrin gel (▪) and HCF (□) (n=5). The values represent mean±standard deviation (n=5). *p<0.05 compared to fibrin gel group.
Gross appearance of repair tissues
Eight weeks after treatment, the repaired tissues in the MF + HCF + BMP-2 group had a morphologically smooth and glistening appearance and exhibited continuity with the surrounding host cartilage (Fig. 5F). The color and glistening appearance of the repaired tissues in the long-term BMP-2 (MF + HCF + BMP-2) delivery group were similar to those manifested by the adjacent host cartilage. In contrast, the groups treated with other methods revealed varying degrees of cartilage resurfacing with whitish regenerative tissue (Fig. 5A–E). The regenerated tissues in the other groups had a rough surface containing fissures. Degenerative changes were not observed in the adjacent articular cartilage of any group. The percentages of regenerated surface area were then compared. The MF + HCF + BMP-2 group showed a significantly higher percentage of regenerated surface area compared to the other groups (Fig. 6).

Photographs of rabbit knee articular cartilage defects 8 weeks after

Percentage of the defect surface area covered with repaired tissue (n=8) 8 weeks after no treatment, microfracture (MF), microfracture + fibrin gel (F), microfracture + fibrin gel + BMP-2, microfracture + HCF, or microfracture + HCF + BMP-2. *p<0.05 compared to no treatment, MF + F + BMP-2, or MF + HCF. **p<0.001 compared to any group.
Histological analysis
Histological analysis showed that the quality of the regenerated tissues differed depending on the treatment (Fig. 7). The histological appearance of the repaired tissue in the MF + HCF + BMP-2 (the long-term delivery of BMP-2) group was improved compared to that of the other groups (Fig. 6). The repaired tissues of the other groups were predominantly fibrous tissues or fibrocartilage, as they were negatively or slightly stained with alcian blue (Fig. 7B–F). In contrast, the MF + HCF + BMP-2 group contained defects filled with hyaline-like cartilage that were stained with alcian blue (Fig. 7G). The thickness of the positively stained tissue was largest in the MF + HCF + BMP-2 group. The MF + HCF + BMP-2 group led to greater chondrocyte cell morphology, Alcian blue staining, structural integrity, thickness, normal cellularity, free from degeneration in adjacent cartilage, and higher total O'Driscoll scores than any other groups except normal group (Table 1).

Alcian blue-stained histological sections of defects 8 weeks after treatments.
p<0.05 compared to any groups except normal group.
BMP, bone morphogenetic protein; HCF, heparin-conjugated fibrin; MF, microfracture; FG, fibrin group.
Extracellular matrix synthesis evaluation
Biochemical assay revealed that the GAG content of the regenerated tissues in the MF + HCF + BMP-2 group was significantly higher than that in the other groups, except for normal cartilage (Fig. 8). There was no significant difference in GAG content between the MF + HCF + BMP-2 group and normal cartilage. The expression of collagen type I mRNA was highest in the short-term BMP-2 (MF + F + BMP-2) delivery group and significantly decreased in the long-term BMP-2 delivery group (Fig. 9A). The long-term delivery of BMP-2 dramatically increased the expression of collagen type II mRNA compared to the other groups, whereas the short-term delivery of BMP-2 did not (Fig. 9B). For the long-term BMP-2 delivery group, the expression of collagen type II protein was highest, whereas that of collagen type I protein was decreased compared to the short-term delivery of BMP-2 (Fig. 10). mRNA expression of type X was not different between the long-term delivery group and the short-term delivery group.

GAG contents of the repaired tissues (n=4). #p<0.001 compared to any group except for the MF + HCF + BMP-2 group. *p<0.001 compared to any group except for normal group. **p<0.05 compared to no treatment, MF, or MF + F group. GAG, glucosaminoglycan.

Quantification of relative expression of extracellular matrices in the repaired tissues 8 weeks after treatment as detected by real-time polymerase chain reaction (n=4).

Representative image of Western blot analysis to evaluate expression of collagen type I and II proteins in the repaired tissues 8 weeks after treatment.
Discussion
Microfracture can regenerate cartilage without cell implantation by inducing migration of BMSCs to cartilage defect sites. However, the treatment often results in regeneration of fibrocartilage rather than hyaline cartilage, 4 which could be due to failed chondrogenic differentiation of the recruited BMSCs. Chondrogenic differentiation of BMSCs can be induced by growth factors such as BMP-2. 20 Therefore, local delivery of BMP-2 to BMSCs recruited to cartilage defect sites by microfracture could induce chondrogenic differentiation of the BMSCs and, in turn, regeneration of hyaline cartilage. This study demonstrates that long-term delivery of BMP-2 to cartilage defects subjected to microfracture induced regeneration of more hyaline-like cartilage compared to short-term delivery or no delivery.
Long-term delivery of BMP-2 to cartilage defect sites was achieved by HCF (Fig. 4). The sustained release of BMP-2 from HCF was likely due to both BMP-2 interactions with heparin and slower degradation of HCF. The inherent capacity of heparin in HCF to bind to BMP-2 via electrostatic interactions between the negatively charged sulfate groups of heparin and the positively charged amino acid residues of BMP-2 enables the long-term delivery of BMP-2.21,22 Several studies have demonstrated long-term delivery of BMP-2 using heparin-conjugated carriers such as fibrin, 14 poly(lactic-co-glycolic acid) scaffold, 23 poly(lactic-co-glycolic acid) nanosphere,24,25 and demineralized bone matrix. 26 Our previous study showed that BMP-2 released from HCF is bioactive. 14 In addition of BMP-2 interaction with heparin in HCF, the slower degradation of HCF (Fig. 4) may contribute to the sustained release of BMP-2. Therefore, local and sustained delivery of BMP-2 to cartilage defect sites could reduce the BMP-2 dosage as well as avoid potential adverse effects.
BMP-2 delivery to cartilage defect sites using HCF has several advantages. Since BMP-2 is loaded into HCF via interaction with heparin, it does not require the use of organic solvents, which are generally utilized in the loading of BMP-2 to a polymeric carrier. This prevents potential loss of BMP-2 bioactivity. Further, the heparin contained in HCF can potentiate BMP-2 bioactivity.21,22,27 In the presence of heparin, degradation of BMP-2 is blocked and the half-life of BMP-2 in culture media is prolonged 20-fold. 22 In addition, HCF is an injectable carrier that can fill irregularly shaped cartilage defects via implantation using minimally invasive surgical procedures. Since a large amount of heparin is conjugated to HCF, this carrier allows for loading of up to 1.7 mg of BMP-2 per milligram of dried HCF. 14
Long-term delivery of BMP-2 to cartilage defects subjected to microfracture resulted in regeneration of more hyaline-like cartilage compared to short-term delivery of BMP-2 (Figs. 6–9). The regeneration of hyaline-like cartilage may be attributed to effective chondrogenic differentiation of the recruited bone-marrow-derived mesenchymal stem cells (BMMSCs) by long-term delivery of BMP-2. Since BMP-2 has a short half-life, 28 BMP-2 should be released over a sufficiently long time period to effectively induce chondrogenic differentiation of the recruited BMMSCs. Indeed, mRNA expression of collagen type II in human BMMSCs was observed after 7 days of BMP-2 treatment. 29 A study showed that long-term delivery of BMP-2 enhances chondrogenic differentiation of murine BMMSCs in vitro. 30
The present study quantitatively demonstrates regeneration of hyaline-like cartilage by long-term delivery of BMP-2 to cartilage defects subjected to microfracture. Analysis of the quantitative (Figs. 8 and 9) as well as qualitative data (Figs. 7 and 10) confirmed that long-term delivery of BMP-2 to cartilage defects subjected to microfracture resulted in regeneration of hyaline-like cartilage compared to short-term delivery of BMP-2. A previous study showed that BMP-7 delivery using a collagen sponge to cartilage defects in rabbits subjected to microfracture results in regeneration of hyaline-like cartilage. 12 However, the collagen sponge mediated short-term delivery of BMP-7 only, and the study did not provide any quantitative data. Another study showed that BMP-2 delivery using hydroxyapatite-polymer composite scaffolds to full-thickness cartilage defects in rabbits likewise results in regeneration of hyaline-like cartilage. 31 However, the composite scaffolds released a majority (96%) of BMP-2 within the first 3 days, and the study also did not provide quantitative data.
Collagen type X is predominantly associated with hypertrophic cartilage and has often been seen as unique to that tissue. 32 Interestingly, at 8 week time point, the in vivo regenerated tissue showed higher expression of collagen type X in both fibrin and HCF treated groups than in no treatment group (MF group) (Fig. 10). This could be due to good entrapment of recruited BMSCs in fibrin or HCF applied to the microfracture sites and subsequent formation of hypertrophic cartilage. In no treatment group (MF group), most of recruited BMSCs may not be localized in the microfracture sites and washed away, resulting in less formation of new tissue and less expression of collagen type X. While BMP-2 is known to stimulate chondrocyte hypertrophy, 33 no additional effect of BMP-2 was found on expression of collagen type X (Fig. 9). The BMP-2 effect on collagen type X expression is seen in vitro.33,34 In vivo, many other types of growth factors and cytokines could be present in cartilage defect site, which might suppress the effect of BMP-2 on collagen type X expression.
Additional studies are necessary to fully evaluate the therapeutic potential of this method. The mechanical properties of the regenerated cartilage should be evaluated, since mechanical function is the major function of cartilage. Cartilage regeneration was evaluated at 8 weeks in this study. Longer-term (i.e., 12–48 weeks) follow-up studies are also necessary since progressive deterioration might be observed after long time periods. A study with rabbit osteochondral defect models showed that degenerative changes in regenerated cartilage increased from 12 to 40 weeks. 35 Additionally, the treatment method of the present study should be evaluated using larger animal models such as dogs, since the canine osteochondral defect model is more closely related to the human clinical setting than the rabbit model with respect to mechanical loading conditions and cartilage thickness. 36 The rabbits used in this study were between 3 and 6 months old, at which rabbits are not skeletally mature. Since the healing capacity of skeletally immature animals is much higher than old ones, the findings of this study must be verified for skeletally mature animals.
Conclusions
The quantitative and qualitative data of this study demonstrate that microfracture combined with long-term delivery of BMP-2 induced regeneration of more hyaline-like cartilage than either microfracture combined with short-term delivery of BMP-2 or microfracture alone. This method is more convenient for hyaline cartilage regeneration than ACI due to its less invasive nature and avoidance of cell implantation. Since BMP-2 and microfracture are currently in use clinically, this approach would be highly feasible. However, examination of the mechanical properties of the regenerated cartilage as well as a longer-term follow-up are necessary to fully evaluate the therapeutic potential of this method. It is also necessary to determine whether recruited BMSCs undergo chondrogenic differentiation and participate in the regeneration of hyaline cartilage.
Footnotes
Acknowledgments
This study was supported by grants (No. 2009-0092213, 2009-0080769) from the National Research Foundation of Korea, a grant (SC 3220) from the Stem cell Research Center of the 21st Century Frontier Program, the Ministry of Education, Science, and Technology, and a grant (A100443) from Ministry of Health and Welfare, Republic of Korea.
Disclosure Statement
No competing financial interests exist.