
Abstract
Currently, the main hurdle in the tissue engineering field is how to provide sufficient blood supply to grafted tissue substitutes in the early post-transplanted period. For three-dimensional, cell-dense, thick tissues to survive after transplantation, treatments are required for hypoxia, nutrient insufficiency, and the accumulation of waste products. In this study, a biomacromolecular layer-by-layer coating process of chitosan/heparin onto a decellularized extracellular bone matrix was designed to accelerate the blood perfusion and re-endothelialization process. The results of in vitro measurements of the activated partial thromboplastin time supported the theory that the combination of chitosan and heparin could bring both anticoagulation and hemocompatibility to the scaffold. A rabbit bone defect model was established for further evaluation of the application of this kind of surface-modified scaffold in vivo. The final results of computed tomography (CT) perfusion imaging and histological examination proved that this facile coating approach could significantly promote blood perfusion and re-endothelialization in the early post-transplanted period compared with an acellular bone matrix due to its much-improved anticoagulation property.
Introduction
Heparin, the most commonly used anticoagulant reagent, has an incontrovertible effect in suppressing thrombi.13–15 It has already been shown that the layer-by-layer coating of heparin/chitosan (HC) serves as an anticoagulant and antibacterial agent, and it is widely used in drug-eluting stent systems in both animal studies and clinical therapies.16–18 Heparinization of surfaces has been shown to be a successful strategy to prevent thrombus formation and improve the hemocompatibility of blood-contacting biomaterials.19–22
Both naturally derived and artificially synthesized biomaterials play a crucial role in supporting the proliferation and differentiation of seed cells by offering a three-dimensional (3-D) environment.23,24 One of the naturally derived materials with osteoinductive properties, acellular bone matrix (ACBM), has exhibited good biocompatibility and osteoinduction in our previous study. 25 The aim of the present research was to fabricate a HC coating on ACBM and to characterize the HC-ACBM scaffold in vitro. To validate this anticoagulation, oxygen and nutrient diffusion were enhanced, and hemoperfusion was performed on the substrates in vivo.
Materials and Methods
Preparation of the HC-ACBM scaffold
The ACBM was prepared using a porcine trabecular bone using a process previously described. 25 Briefly, cancellous bone was harvested from the femoral head of a white swine from a local slaughterhouse within 6 h after death, transferred to the laboratory in 4°C saline (0.9%), and immediately processed under clean conditions. The samples were cleaned by removing the residual tissues, sectioned into discs (10 mm in diameter and 5 mm in thickness), rinsed, and immersed in distilled water overnight at 4°C. Then, the samples were decellularized by 1% Triton X-100 (Sigma) for 48 h, degreased with methane/methyl alcohol for 24 h, incubated with DNase (Sigma)/RNase (Fluka) at 37°C for 2 h, and then washed in phosphate-buffered saline (PBS) at room temperature under continuous shaking. The scaffolds were immersed in dehydrated alcohol for 4 h to remove the cellular remnants and then washed with a large amount of deionized water for 2 h before being dried.
The scaffolds were then dipped in a 0.05 wt% heparin sodium salt (Sigma) aqueous solution for 15 min and subsequently rinsed with deionized water. The heparinized blocks were then put into a solution including 0.2 wt% acetic acid and 0.1 wt% chitosan (Sigma) with a minimum deacetylation degree of 85% for 15 min, followed by the same rinsing procedures. Several bilayers (1∼8) of HC coated stable supramolecular complex films were prepared by repeating this process (1–8 times) by electrostatic interaction. The blocks were transported to deionized water for 6 h before being dried at 37°C. Finally, the blocks were sterilized by 60Co γ irradiation (2 Mrad) and stored at –80°C before further application.
Characterization of the HC-ACBM scaffold
Surface characterization
The morphology of the HC-ACBM scaffold (the following scaffolds were eight layers except samples used in XPS) and ACBM was visualized under a scanning electron microscope(TESCAN VEAG II,Czech Republic). The elemental compositions of the ACBM surface and (2, 4, 6, and 8 layers, respectively) of heparin-chitosan (HEP-CS)-coated HC-ACBM scaffolds were determined by X-ray photoelectron spectroscopy (XPS, ESCALAB 250, Thermo Scientific). All such spectra were recorded using monochromatic Al-Kα radiation (1486.6 eV), with a pass energy of 30 eV. The shift in binding energy due to relative surface charging was corrected using the C1s level at 285.0 eV as an internal standard. The surface compositions were calculated from the XPS intensities using the relative sensitivity factors provided by the instrument manufacturer. The chemical structure of the coated film was investigated by Fourier transform infrared spectrometry (FTIR).
Mercury intrusion porosimetry
The total pore volume and the median pore size of the HC-ACBM and ACBM scaffolds were determined using a mercury intrusion porosimeter (Micromeritics Autopore III, n=5).
Heparin release from the HC-ACBM scaffolds
The reaction between toluidine blue and heparin allowed for the determination of the heparin content in solution. Briefly, a 0.005% toluidine blue solution was prepared in 0.01 N HCl containing 0.2% NaCl. A standard heparin solution was prepared by dissolving 10 mg of heparin in 100 mL of 0.2% NaCl aqueous solution. Next, 2.5 mL of 0.005% toluidine blue solution was pipetted into test tubes. The test samples, heparin standards (10–70 μg heparin), and with a blank solution (0.2% NaCl) were added and diluted with 0.2% NaCl to a total volume of 5 mL. All the tubes were agitated for 30 s. Hexane (5 mL) was then added to each tube, and the tubes were shaken vigorously for another 30 s to separate the heparin-dye complex. The aqueous layers from all the tubes were removed, and the absorbance was measured at 631 nm within 30 min using a Shimadzu UV-1201 spectrophotometer. The heparinized scaffolds were placed in 15-mL plastic centrifuge tubes containing 10 mL PBS (pH 7.4) or deionized (DI) water in a shaking water bath at 37°C. At appropriate intervals, namely, 1, 3, 7, 14, 21, and 28 d later, 500 μL of the dissolution medium was extracted and assayed for heparin content using the method just described.
Activated partial thromboplastin time (APTT) assay
For the APTT measurement, both the ACBM and HC-ACBM dishes were soaked in PBS (pH 7.4) for 1, 3, 7, 14, 21, and 28 d (n=4). The supernatants of the samples (10 μL) were placed onto a 24-well culture plate. Fresh human platelet poor plasma (200 μL) and actin-activated cephaloplastin reagent (100 μL) were added, followed by the addition of a 0.03 M CaCl2 solution (100 μL) after incubation for 5 min at 37°C. The clotting time of the plasma solution was measured using a coagulometer (Clot 1A, Innova).
Cell attachment and proliferation on the HC-ACBM scaffold in vitro
Isolation and culture of bone marrow stem cells (BMSCs)
Bone marrow (3 mL from each rabbit) was aspirated from the ilium of healthy New Zealand white rabbits (age 3 months and weighing 2–2.5 kg) with a 10-mL syringe containing 1250 units of heparin. The aspirated bone marrow was mixed with an equal volume of PBS and centrifuged on a Percoll gradient (1.077 g/mL, TBD) for 20 min at a relative centrifugal force of 2000×g at 20°C. The BMSCs were isolated from the layer between the Percoll reagent and the blood plasma and washed thrice with PBS. Then, the cells were resuspended in low glucose Dulbecco's modified Eagle's medium (DMEM, Gibco) supplemented with 10% fetal bovine serum (FBS, HyClone), 100 U/mL penicillin (Sigma), and 100 mg/mL streptomycin (Sigma) and cultured in 5% CO2 at 37°C. These cultured cells were referred to as P0 cells. When the cells grew to near confluence, they were washed with PBS and harvested with 0.25% trypsin/1 mM ethylenediaminetetraacetic acid (EDTA). The cells were subcultured when they reached 70%–80% confluence. Cells at passages 3–5 were used for the following studies.
Cell attachment
All disks were attached in 24-well plates, seeded with 1×104 cells per scaffold, and incubated in DMEM with 10% FBS medium at 37°C for 6, 24, and 72 h. The disks were washed thrice in PBS and microscopically observed (Axiover 25, Carl Zeiss). At the same time, the cells on the scaffolds were fixed at room temperature in 3% gluteraldehyde for 1 h. The cell-scaffold constructs were then sequentially dehydrated using an ethanol series (50%, 70%, 80%, 90%, 95%, and 100%) for 10 min each, dried overnight, and coated with gold. The cell attachment was evaluated under scanning electron microscopy (SEM).
Cell culture and proliferation
BMSCs were seeded on the HC-ACBM and ACBM (10 mm in diameter×3 mm in length) at a density of 5×104 cells per scaffold, cultured in DMEM supplemented with 10% FBS and 1% penicillin-streptomycin, and maintained in an incubator at 37°C with 5% CO2 and 95% humidified air for 21 d. Cell proliferation was quantitatively analyzed by mean transit time (MTT) assay. Briefly, the scaffolds were washed with PBS at predetermined time points, and 2 mL of MTT (Sigma) solution (0.5 mg/mL in PBS) was added to each well, followed by 4 h of incubation at 37°C. After the MTT solution had been removed, 5 mL of dimethyl sulfoxide solution (Sigma) was added. The scaffolds were extensively washed by repeatedly pipetting up and down to allow total cell release. Moreover, the solution was centrifuged at 12000×g for 10 min. The supernatant was collected and diluted whenever necessary. The absorbance was read via a spectrophotometer at 490 nm. The growth curves of the BMSCs cultured in all groups were determined.
Perfusion of blood and vascularization in vivo
Surgical procedures
Animal experiments were performed in the Animal Laboratory, Daping Hospital, Third Military Medical University, Chongqing, China. The Institutional Animal Care and Use Committee approved all of the animal experimental protocols. The rabbits were anesthetized by intramuscular injection of ketamine (50 mg/kg body weight), and bilateral surgical procedures were conducted under aseptic conditions. A 2-cm incision was made in the anterior aspect of the upper limb, and the radius was isolated through the interspace of the tendons and the muscles. Then, a complete bone defect of 15 mm, which included the periosteum, was made in the middle segment of the radius. The ulna was left intact for mechanical stability. The implanted materials were inserted into the bone defect and bound to the ulna by thread without other fixation devices. Thirty rabbits were randomized into 6 time groups (1, 3, 7, 14, 21, and 28 d), with five rabbits in each time group. The bone defect in the right radius was implanted with HC-ACBM, and the defect in the left radius was implanted with ACBM material. After implantation, the wounds were carefully washed with physiological saline, and the incisions were sutured in full thickness.
Computed tomography perfusion study of the implanted scaffold
A 64-detector row CT scanner (Philips Brilliance 64, Philips Medical System) was used with the following protocol at the above time points. A first CT scan was obtained without intravenous injection of contrast medium using the following imaging parameters: 120 kV, 100 mA, 0.4-s gantry rotation time, 5-mm collimation, 360-mm field-of-view, and 512-mm matrix. This series helped locate the scaffold and choose an area that encompassed the entire bone defect for the subsequent perfusion imaging. The area was chosen by a radiologist who had 20 years of experience in the field. In the computed tomography perfusion (CTP) study, a pump injector (MEORAO-Stellant, MEORAO Company) was used to inject a 50 mL bolus of iodinated contrast (Ultravist 300, iopamidol) via a pinna vein at a flow rate of 6 mL/s. Repeated spiral scans were then acquired at an interval of 1 s by means of cine-mode acquisition. The following parameters were used: 120 kV, 100 mA, 0.4-s gantry rotation time, 2.5-mm reconstruction width, 150-mm field of view, and 512-mm matrix. Image acquisition started 10 s after the start of the bolus injection, and finally, the CTP images were analyzed with the commercial CTP analysis software ‘Perfusion 3’ (Philips Medical Systems). This technique allows the calculation of parametric maps for regional blood flow (BF), regional blood volume (BV), and regional MTT.
Image analysis was performed by another radiologist with 5 years of experience in interpreting CTP images, who was blinded to the features including animals' groups, time after operation, and the final pathologic results. The blood input was determined by placing a circular region of interest (ROI) on the area. A circular or oval ROI for the calculation of perfusion parameters of the entire scaffold was established around the peripheral margin of the radius. To minimize biases, three sites were randomly measured on each section (from three sections of each scaffold: the middle and two ends). The average value of the measurements was chosen as the perfusion parameter.
Histological analysis
Five rabbits out of each group were euthanized by overdose of anesthesia at 1, 3, 7, 14, 21, and 28 d after implantation. The radii of each rabbit were obtained and fixed in 10% formalin, decalcified by 8% EDTA (Sigma), and embedded in paraffin. Sagittal plane sections (5 μm thick) were prepared and stained with H.E. to assess neovascularization. Three independent observers who had been blinded to the treatment groups counted the microvessels at the implanted site under a light microscope, as previously described. 6 Briefly, five consecutive sections were prepared for every sample. The microvessels of each randomly chosen field were counted by the three independent observers. The mean of the three independent counts by the observers was considered the final value for each counted field. All observers followed the prescheduled rule that, under the microscope, each luminal structure composed of endothelial cells was counted as a vessel.
Statistical analysis
All the data are expressed as mean±SD. Analysis was performed using the Statistical Program for Social Science (SPSS) 13.0 for Windows. Analysis of variance and a paired t-test were used to determine any significant differences among the groups, and p values >0.05 were considered significant.
Results
Figure 1 shows the surface morphology of an ACBM and HC-treated ACBM scaffold. The HC treatment did not change the morphology of the ACBM scaffold (Fig. 1A and B), but the microparticles were found to be evenly distributed and embedded, which made the surface more smooth than that of the ACBM. The total pore volume and the median pore size of the ACBM and HC-ACBM scaffolds are shown in Figure 1 (C and D). The scaffolds of the ACBM had a total pore volume of 69.17%±0.79% and a median pore size of 454.92±107.22 μm, whereas those of the HC-ACBM were 68.93%±0.87% and 447.33±109.89 μm, respectively. There was no statistically significant difference in the aforementioned properties between the two kinds of scaffolds (p=0.068). Thus, the heparinization process did not affect the porous structures of the scaffolds.
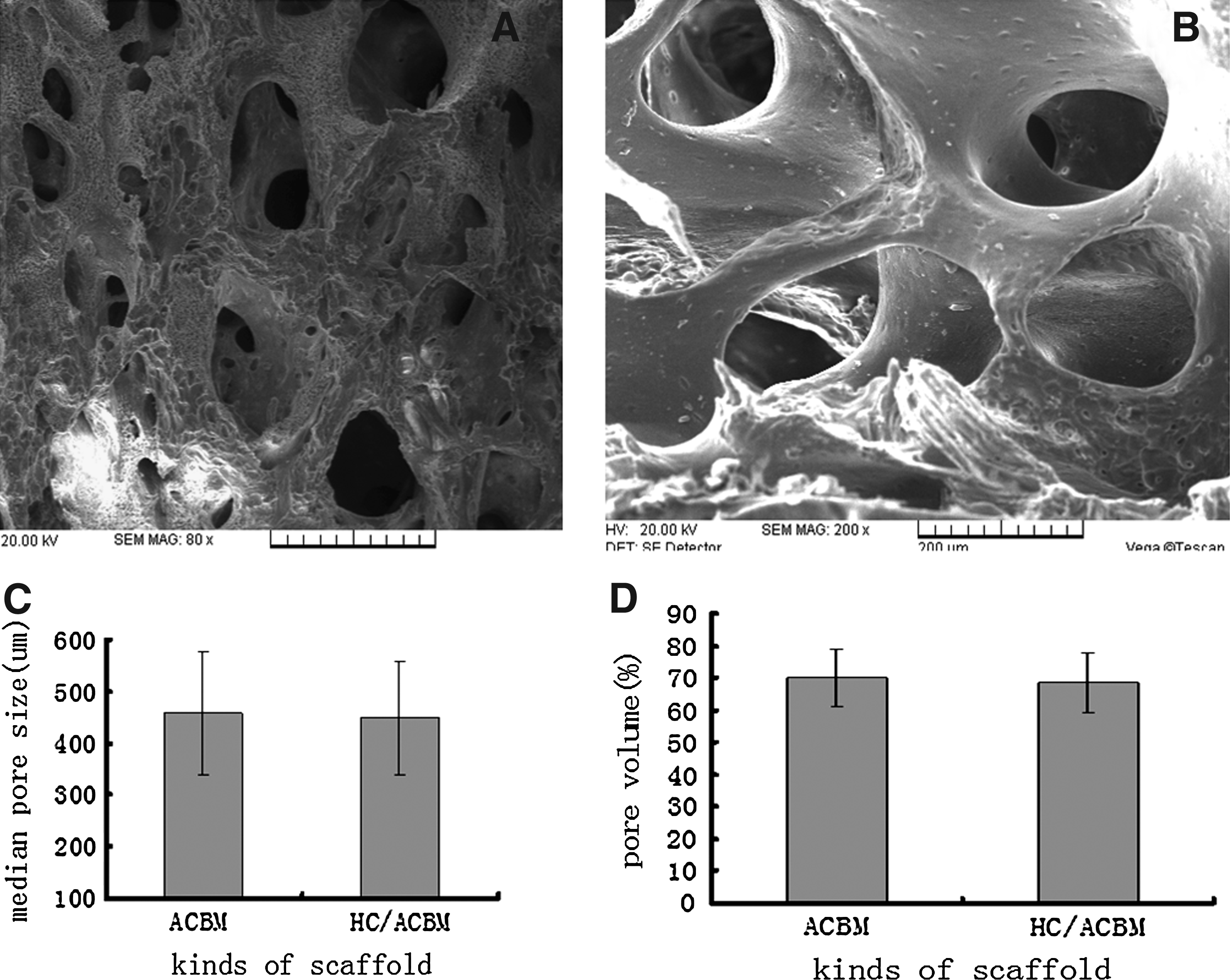
Scanning electron micrographs of ACBM and HC-ACBM scaffold. Structure of cancellous bone was reserved and collagen I exposed on the surface of ACBM scaffolds
The XPS spectrum of the ACBM scaffold showed abundant carbon and oxygen peaks due to both chitosan and ACBM (Fig. 2A). After heparinization, the sulfur (S) peak appeared at the binding energy of 168-170 eV (Fig. 2B), which indicated the presence of heparin on the surface of the heparinized scaffold. The percentage of S on the surface of the HC-ACBM scaffold was further confirmed by XPS, and it increased as the number of heparin layers increased (Fig. 2C).
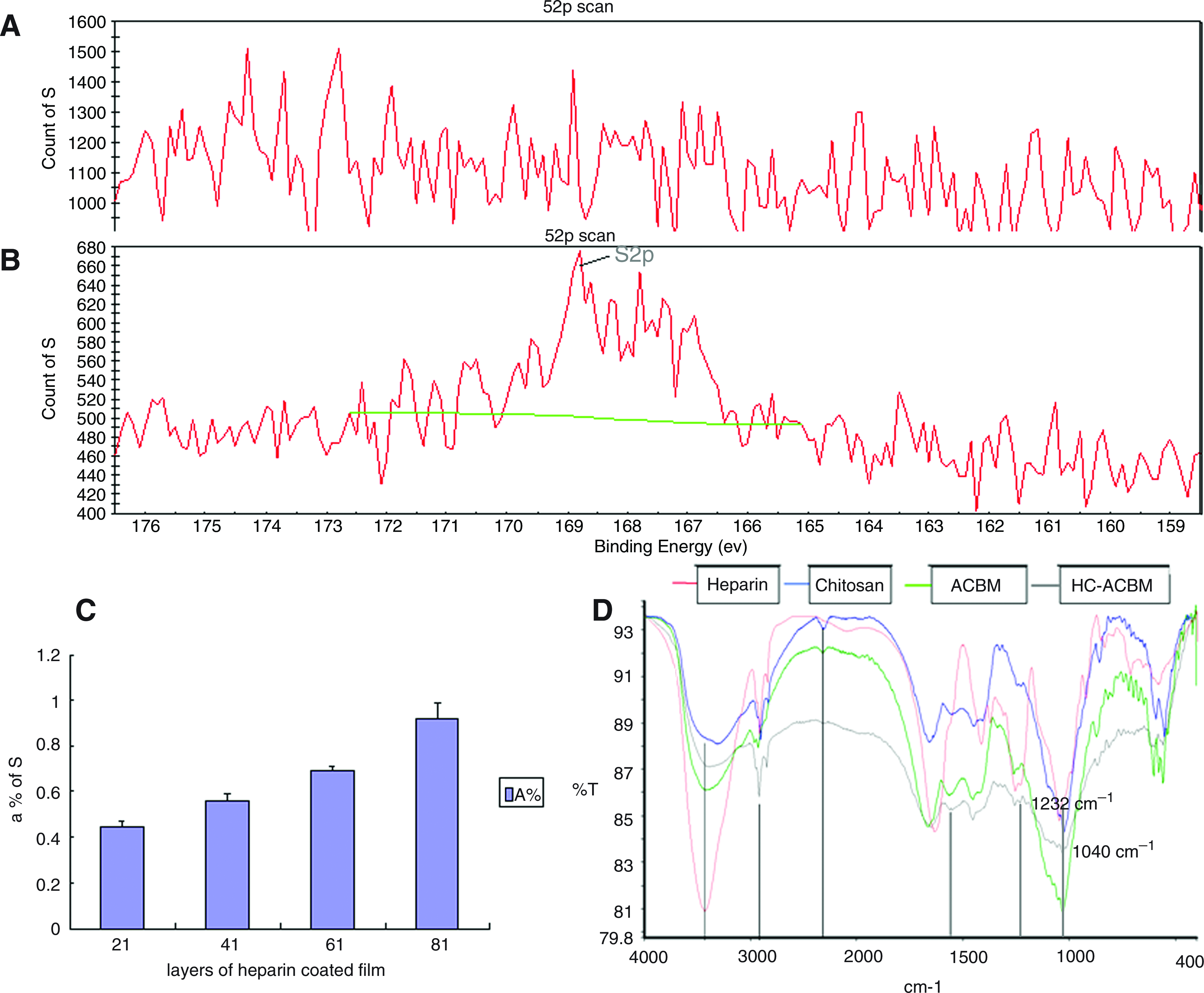
XPS spectra of scaffolds
The FTIR spectrum of chitosan (Fig. 2D) showed a broad peak around 3450 cm−1 related to hydroxyl stretching, a peak at 1638 cm−1 attributed to the C=O (amide I) stretching mode, a peak at 1385 cm−1 related to the–C–O stretching mode of the -CH2–OH group, and a broad peak around 1090 cm−1 related to vibrational C–O stretching. The FTIR spectrum of heparin showed a broad peak centered at 3450 cm−1 assigned to hydroxyl stretching, a peak related to the stretching vibration of C–H bonds at 2942 cm−1, and peaks attributed to asymmetric and symmetric axial deformations of carboxylate anions at 1634 cm−1 and 1429 cm−1, respectively. The absorbances at 1232 cm−1 and 1040 cm−1 were due to–SO3 asymmetric and symmetric stretching, respectively. The formation of chitosan-heparin complexes resulted in an additional shoulder corresponding to the heparin absorbance at 1232 cm−1 and a peak corresponding to the heparin absorbance at 1040 cm−1. Such absorbances were characteristic for the -SO3 groups of heparin.
Periodic release of heparin from HC/ACBM scaffolds (10 mm×5 mm) in PBS and DI is shown in Figure 3A. Within two weeks, the concentration of heparin released in PBS was significantly higher than that in DI (p<0.05). Heparin release decreased gradually in DI after 2 weeks, whereas in PBS, heparin release was negatively correlated with time.
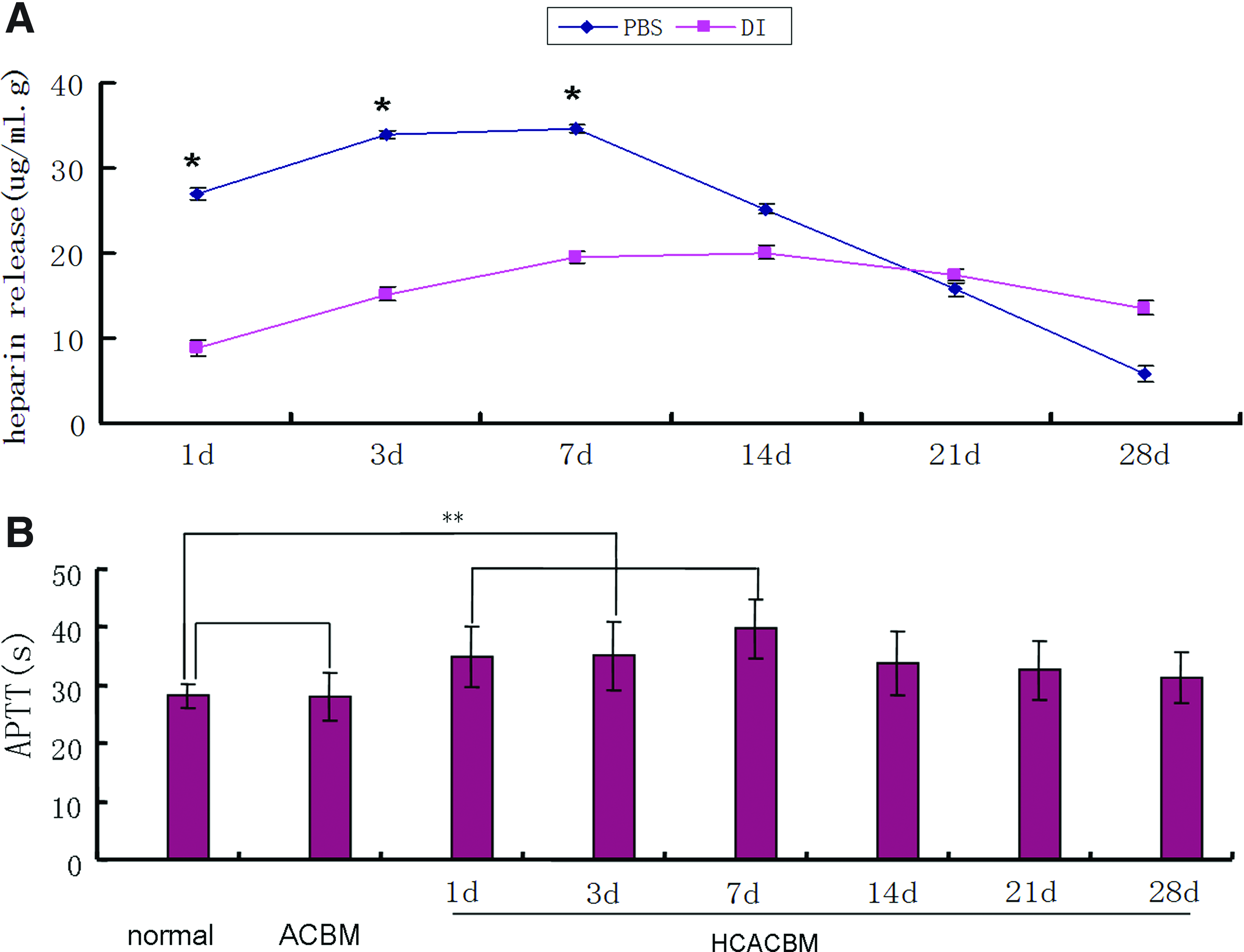
Periodic heparin releases from 8 layers of HC/ACBM scaffolds treated with PBS and DI, respectively, for 28 d
Figure 3B shows the anticoagulation of the samples in vitro. The blood coagulation assay was repeated on the layer-by-layer (LBL)-coated ACBM samples after being soaked in PBS for 1, 3, 7 14 d, 21, and 28 d.
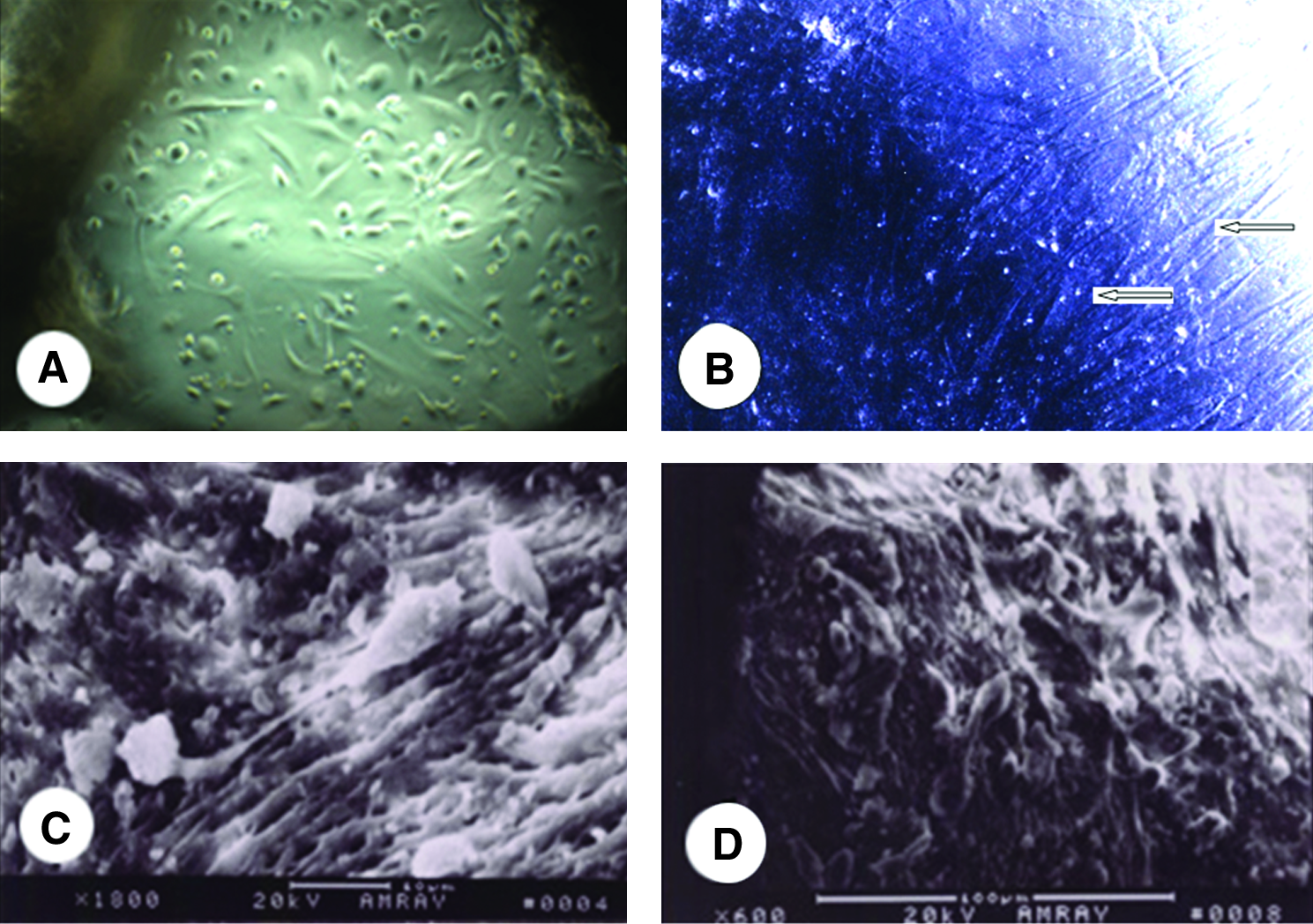
The attachment of mesenchymal stem cells (MSCs) on each scaffold after different time points of culture was measured and normalized to an initial cell seeding density. At the same time, cells seeded on the scaffold were viewed under a light microscope and by SEM (Fig. 4A–D). In general, cell attachment on the HC-ACBM scaffold in the presence of FBS was similar to that of the control ACBM. The cell densities on different scaffolds were also measured to evaluate cell proliferation for up to 3 weeks of culture in the presence of FBS at 37°C. In general, the cell densities reached a peak after 2 weeks and remained at a similar level during the later time periods. The cell densities on the HC-ACBM substrates were similar to the ACBM scaffold, and the maximum density was twice to thrice higher than the initial cell seeding density.
CTP analysis revealed significant differences in BF, BV, and MTT at the various temporal resolutions between the HC-ACBM- and ACBM-implanted groups (Fig. 5C–J). The median BF increased continuously within 2 weeks (Fig. 5K), with the highest values at 2 weeks.
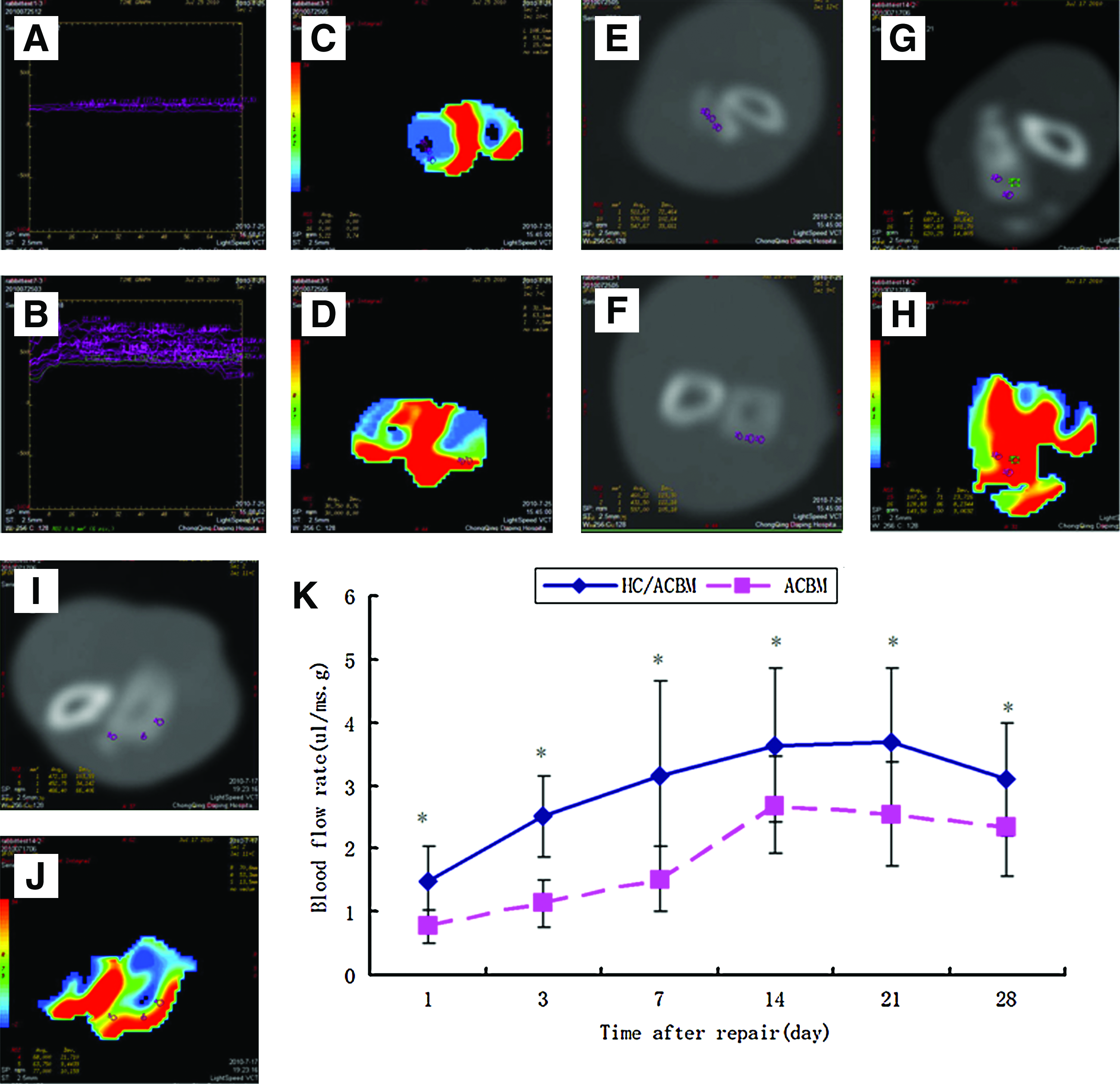
Time density curves of the ACBM
Microvessels at the implant site were easily observed in the bone trabecula by light microscopy at 7 d in the HC-ACBM-implanted group, whereas in the ACBM group, microvessels could only be observed in the surrounding tissues. At 14 and 28 d, the number of microvessels was much higher in the HC-ACBM than in the ACBM group, and new formed bone became obviously around the scaffold. In the ACBM group, only fibrous tissue surround the scaffold instead of new formed bone (Fig. 6).

H&E stained sections of rabbit bone defects after implantation in the ACBM group
Discussion
Blood contacting the surface of a foreign material may result in protein adsorption, activation of the complement system, and the clotting cascade, eventually leading to thrombus formation. 26 The hemocompatibility of a biomaterial is determined by its surface properties; therefore, good surface properties are crucial for the application of biomaterials in vivo. The surface properties are frequently supplemented by the addition of active anticoagulant molecules, such as heparin. Covalently immobilized heparin needs a relatively high surface density and stability to act as a long-term anticoagulant in a clinical situation.27,28
Heparin-based delivery systems have been shown to be capable of serving as reservoirs to store heparin-binding growth factors and enhancing the bioavailability of these factors, such as fibroblast growth factors and bone morphogenetic proteins. 29
Our earlier work has shown that ACBM scaffolds possess excellent mechanical properties, are noncytotoxic, and have low immunogenicity and appropriate porous structures for bone tissue engineering applications. 30 In this study, collagen I was exposed on the surface of ACBM (Fig. 1A). Collagen, like chitosan, has positively charged NH3+ groups. Heparin, on the other hand, has a highly negative charge density and is, thus, capable of interacting with protonated collagen and chitosan. Heparinization of the surfaces has been shown to be a successful strategy to prevent thrombus formation and to improve the hemocompatibility of blood-contacting biomaterials.31–33 In the recent decade, various approaches of surface heparinization have been reported (for example, layer-by-layer coating and covalent immobilization).34,35 In this study, the heparin-chitosan self-assembled ACBM showed the same FTIR spectra as that in a stent, which indicates that certain fragmentation effects occur in the process and that primary amine groups are partially transformed into nitrile, amide, or imine functional groups. 36 Therefore, the results of FTIR combined with SEM indicated the possibility of an electrophoretic deposition of chitosan coatings containing heparin.
The presence of heparin on HC-coated ACBM scaffolds was ascertained through performing XPS on the surface of the scaffolds. The XPS spectrum clearly showed a peak at the binding energy of 168-170 eV, which is characteristic of the 2p electrons of S, although this S peak did not appear on the XPS spectrum of the ACBM scaffolds (Fig. 2A). XPS is a quantitative spectroscopic surface chemistry analysis technique by which S can be quantified. Since the scaffold has a 3-D porous structure, the amount of heparin detected could not stand for the average amount of heparin immobilized on the scaffolds.37,38
Therefore, in this study, a colorimetric assay was adopted to measure the concentration of the heparin solution after heparin treatment. The amount of heparin released periodically from a heparin-coated ACBM was different in the two solutions. As shown in Figure3A, the concentration of heparin bound to the surface is determined by the toluidine blue method after immersion in PBS and DI water for various periods of time to evaluate the stability of covalently immobilized heparin. In their study, Yang et al. 39 observed that the surface concentration of heparin merely reduces a little of the heparin-coated stent after immersion in DI water for days. They proposed that this was mainly due to the excellent stability of the film, which has robust covalent bonding strength. However, in our experiment, the heparin released in DI water was below 20 μg/mL.g, whereas in PBS solution, the amount of heparin released was twice higher than that in DI water in the first week. Therefore, we presume that electrolytes may make the heparin release more easily than that in vivo.
The CS/HEP LBL coating has already been shown to be effective in the anticoagulation of human blood.40–42 It was confirmed that heparin depolymerized by γ-irradiation via mechanisms of radical-induced scission of the glycosidic linkage under a high amount of radiation of 180 kGy. However, the prevalent structure of the parent in the undersulfated heparin region was maintained, which preserved the activty of anticogulation. When sterilized according to ISO standards (below a doses of 25kGy), there was no significant loss of activity in samples.43,44
In our blood coagulation assays, we observed that APTT was remarkably prolonged in the case of LBL-coated samples after 2 weeks compared with that of the normal samples, as shown in Figure 3B. The APTT values of the LBL-coated samples were also found to be extended, with an increase in the number of CS/HEP bilayers (data not shown). Heparin has been shown to contribute predominantly to the anticoagulation property of the CS/HEP LBL membrane and is one important part in this coating system. 45
In nearly all tissues, capillaries precisely organize themselves and support normal organ functions via the supply of oxygen and nutrients as well as the removal of various metabolic wastes. Cells rely on a capillary network within a perimeter of 100–150 μm in living tissues. 46 In the case of cultured cell aggregates in vitro, oxygen transport is limited to a diffusion distance of 150–200 μm from the oxygen source. 19 To date, most of the success in tissue engineering has been limited to avascular tissues and thin tissues such as cartilage, skin, and large-scale vasculature,47–50 that can survive with a supply of oxygen and nutrients by simple diffusion without an additional vascular supply. Insufficient vascularization can lead to improper cell integration or cell death in cell-dense thick tissues. Therefore, the main hurdle of current tissue engineering is how to provide sufficient blood supply to implanted tissue substitutes in the early post-transplanted period.
There are many methods of measuring blood supply in tissues, such as micro-CT, laser Doppler anemometry, SPECT, and MRI; however, there are many problems with micro-CT and laser Doppler, including the need for isotopes as well as subject sacrifice or removal of a piece of bone.51,52 In addition, SPECT and MRI are inaccurate because of interference with surrounding tissues. Thus, we prefer to use CTP technology for non-invasive imaging. CTP can detect blood perfusion in definite tissues, such as lung, brain, bone, and heart. Moreover, it can exclude the interference from areas outside the ROI. Importantly, CTP can detect blood perfusion of engineered bone to provide real-time and reproducible assessments of bone BF.
Due to these characteristics, CTP is used extensively for the observation of angiopoiesis in tumors of the heart or in brain infarctions. Through analyzing the results from CTP with software, quantitative data can be obtained, including BV, BF, and MTT.
In this study, blood infiltrated into the scaffold at its boundary after 24 h of implantation, but the BV and MTT in the HC-ACBM group was much greater than that in the ACBM group. This tendency lasted until 28 d after implantation. In the HC-ACBM group, blood perfusion could enter the center of the scaffold, and this perfusion could be seen histologically, where new blood capillaries were formed starting at 3 d after implantation. On the other hand, in the ACBM scaffold, vascularization only appeared in the surrounding soft tissues.
Conclusions
Heparin released from the HC-coated ACBM scaffold can lengthen the APTT. When implanted into the bone defect, this scaffold can promote blood perfusion and angiopoiesis. CTP as a noninvasive technology for detecting blood supply can be used in tissue engineering in the early post-transplanted period. Although our results showed that HC-ACBM has no influence on the adhesion and proliferation of MSCs, whether the cell differentiation of MSCs in this 3-D scaffold and blood perfusion could be promoted to induce hemokinesis through an interior anticoagulation scaffold and whether this type of blood perfusion could promote cell survival and angiopoiesis need further research.
Footnotes
Acknowledgments
This study was funded by the projects of (CSTC, 2008BC5004, and 2011CB964701).
Disclosure Statement
No competing financial interests exist.