
Abstract
Tissue-engineered myocardial patches could be useful in the repair of myocardial injuries. The aim of the present study was to evaluate a collagen targeting delivery system for myocardial repair. A specific peptide collagen-binding domain (CBD) was fused to human vascular endothelial growth factor (VEGF) to enhance the binding of VEGF to collagen. In this study, collagen membranes loaded with CBD-VEGF, natural VEGF, or phosphate-buffered saline are used as cardiac patches to repair the infarcted myocardium in a rabbit model. CBD-VEGF/collagen group could effectively induce more cells to penetrate into the collagen membrane after 4 weeks and promote more vascularization in infarcted myocardium after 12 weeks compared with the other two control groups. Echocardiography and hemodynamic studies both show cardiac function improvement in the CBD-VEGF/collagen group. These results reveal that implantation of CBD-VEGF collagen membrane patch into the infarcted myocardium could effectively improve left ventricle cardiac function and increase the vascular density.
Introduction
Vascular endothelial growth factor (VEGF) is critical to the migration and proliferation of endothelial cells (ECs) and the formation of new vessels. In ischemic heart disease therapy, VEGF specially stimulates angiogenesis and enhances collateral blood flow after myocardial infarction.3,4 Direct addition of VEGF to the scaffold is expected to result in its elution by blood flow and body fluid. As a result, the remaining VEGF will be decreased and repeated injections or higher dose is needed to maintain the effective concentration. However, large amount of VEGF could lead to high cost and certain side effects, for example, the formation of abnormal blood vessel and hemangioma. 5
Biological scaffold materials have been used in a variety of tissue regeneration applications. They provide scaffolds to promote site-specific, constructive remodeling. In cardiac tissue engineering, biomaterials are being used as cardiac patches to improve the cardiac function and have emerged as substitute for heart transplantation for the treatment of damaged myocardium.6,7 Recently, extracellular matrix (ECM) derived from the basement membrane and lamina propria layers of the porcine urinary bladder has been used commonly and has been shown to enhance mechanical function. Although the necessary mechanical support and adhesion sites are provided by many biomaterials, still they could not actively guide cells. 8
Collagen is the main component of the cardiac ECM; about 85% of the total collagen is type I. Collagen is known for its weak antigenicity, excellent biocompatibility, and biodegradability in the tissue engineering research field.9,10 It has been shown that collagen has an important role during wound repair, because it can provide a three-dimensional scaffold for cell adhesion, migration, and differentiation.11,12 In our previous study, we developed a collagen-based VEGF targeting delivery system by combining collagen-binding domain (CBD) and VEGF. When injected to the myocardial infarction site, CBD-VEGF could be retained in the cardiac ECM and stimulate angiogenesis effectively. 13
In this study, CBD-VEGF was used to prolong the presence of VEGF in the collagen membrane and activate the collagen membrane. The purpose of this work was to evaluate the effect of the collagen scaffold loaded with CBD-VEGF as a patch for myocardial ischemia repair as well as cardiac function improvement.
Materials and Methods
Collagen membrane preparation and surface morphologic analysis
Collagen membranes were obtained by Zhenghai Biotechnology and had a porous stereoscopic structure as previously reported. 14 They were derived from bovine skin and 99% of the ingredients were collagen type I and type III. The collagen membranes used throughout this study were cut into 1-cm squares with thickness of 0.8 mm and sterilized by 12 kGy Co60 irradiation (Fig. 1C). The surface morphology of collagen membranes was analyzed by a scanning electron microscope (SEM; Model S-2500; Hitachi).
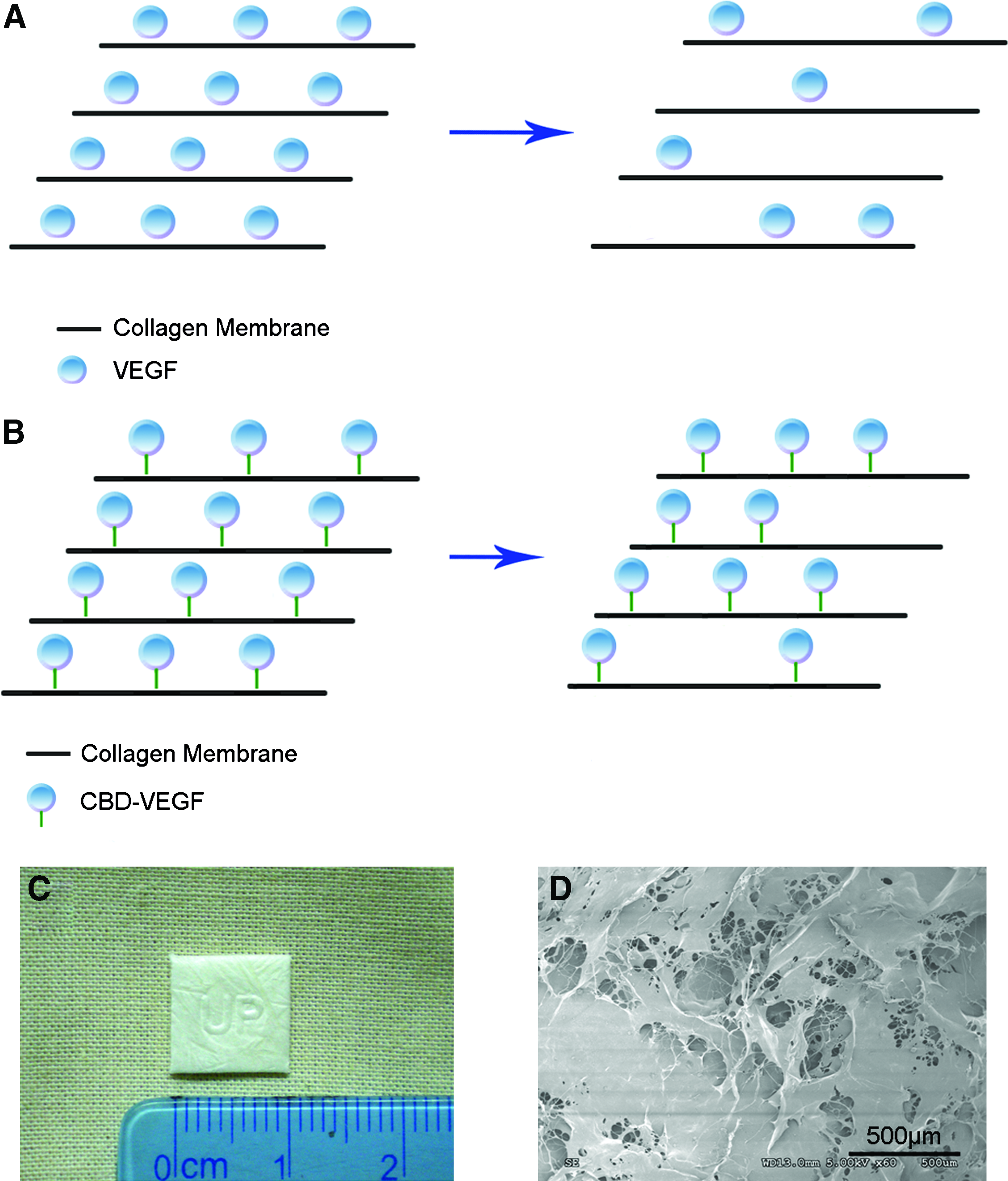
Diagram of the CBD-VEGF delivery system and appearance of collagen scaffold used for myocardial regeneration.
VEGF and CBD-VEGF preparation
VEGF and CBD-VEGF were prepared as previously described.
13
Briefly, VEGF and CBD-VEGF expression vectors were transformed into the BL21 (DE3) strain of Escherichia coli. Protein expression was induced by isopropyl β-
Experimental animals
Adult male New Zealand white rabbits weighing 1.8–2.2 kg were used in this study. All experimental procedures were conducted according to local guidelines on the ethical use of animals and the National Institutes of Health “Guide for the Care and Use of Laboratory Animals” (NIH publication 85-23, revised 1996), and all protocols were approved by the Animal Care and Use Committee of Chinese Academy of Medical Sciences.
Surgical procedure
Experimental myocardial infarction was induced by the ligation of left anterior descending coronary artery as previously described with minor modification. 15 Briefly, 36 male New Zealand White rabbits were used in the experiments. They were randomly divided into two groups: 15 of the rabbits were kept for 4 weeks after the surgery and 21 of the rabbits for 12 weeks. In each group, the rabbits were equally divided into three subgroups, including collagen membrane/CBD-VEGF (0.56 nmol), collagen membrane/VEGF (0.56 nmol), and collagen membrane/phosphate-buffered saline (PBS) groups. The rabbits were anesthetized with pentobarbital sodium (40 mg/kg) by intravenous administration, then placed in the supine position, and subjected to a median sternotomy. The pericardium was incised to expose the anterior surface or the heart and the left anterior descending artery was ligated at the midpoint between the starting point and the cardiac apex with a 6-0 polypropylene suture (Fig. 2B). Correct position of the ligation was confirmed by ST-segment elevation on the ECG and regional cyanosis of the myocardial surface. One side of the collagen membrane loaded with different samples was sewed on the ischemic left ventricular free wall (Fig. 2C). Under the collagen membrane, a square incision of size 1 cm×1 cm×2 mm was made by arteriotome. Within the square incision, about 2-mm-thick myocardium was excised by curved scissors. Only part of the ventricular myocardium was cut off (Fig. 2A). Then the other side of the collagen membrane was sewed on the remaining myocardium to cover the incision (Fig. 2D). The chest was closed and all animals received intramuscular ampicillin for 3 days after surgery.
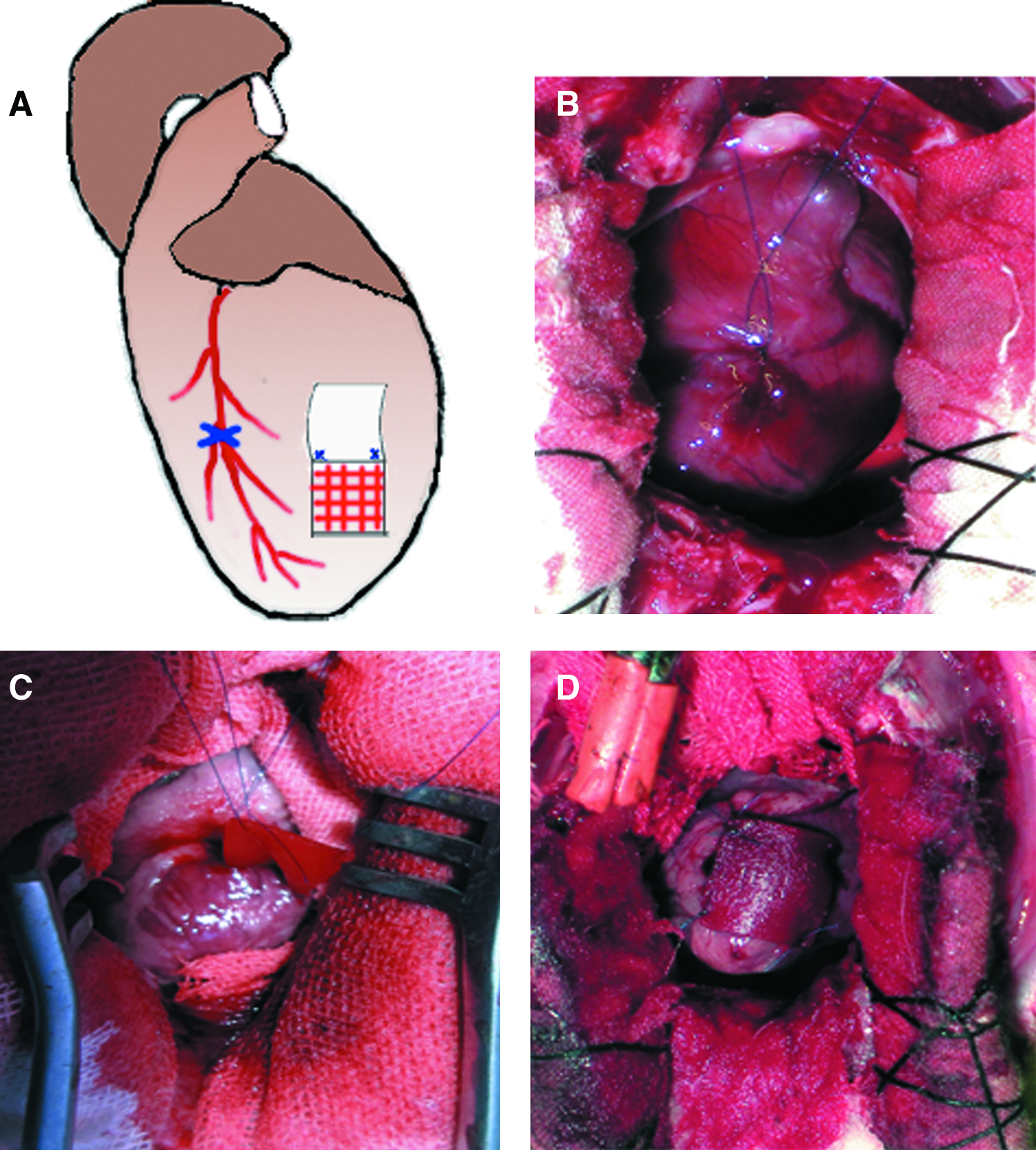
The surgical procedure of rabbit heart injury model.
Functional assessment by echocardiography
Four weeks and 12 weeks after the surgery, echocardiography was performed to evaluate the left ventricle function. The rabbit was placed in the left lateral decubitus position. Standard two-dimensional and M-mode transthoracic images were recorded at the level of the papillary muscles using S8-3 linear transducer (IE33; Philip). Left ventricular (LV) end-systolic dimension (LVDs) and end-diastolic dimension (LVDd) were measured in the M-mode tracings at the midpapillary level. Percentage of LV fractional shortening (%FS) was calculated as %FS=(LVDd − LVDs)/LVDd×100%. 16
Cardiac hemodynamic studies
After echocardiography, rabbits were cannulated with a carotid arterial catheter that had been advanced into the LV from the isolated right carotid artery. The measurements were obtained using a pressure transducer (MP150; Biopac Systems) connected with the catheter. LV systolic pressure, end-diastolic pressure, maximal rise in pressure during systole (+dp/dt), and minimal decrease in pressure in diastole (−dp/dt) were averaged on five consecutive cardiac cycles.
Histological analysis
After hemodynamic measurements, the heart was rapidly excised and sliced into four segments from apex to base. The segments with materials were fixed in 10% formalin for 48 h and embedded in paraffin. Then the samples were cut into 5-μm-thick slices and stained with hematoxylin and eosin (H&E). The slices were scanned with LEICASCN400 to get the general morphology. The cell numbers in the collagen membrane at 4 weeks after the operation were calculated under a 400×microscope field using a Nikon calibrated lens microscope (Nihon Kogaku Co.). Photographs of the remaining collagen membrane at six random locations were taken, and then the cells on each photograph were counted and the average cell number in the six photographs of the same sample was calculated. The average cell number per field in the three groups was calculated respectively. 17
Immunohistological examination was performed using smooth muscle anti-actin antibody (ZM-0003; ZSGB-BIO). 18 The capillary density was counted 12 weeks after the operation. At least six photographs in the infarcted myocardium under the collagen membrane were randomly selected under a 400×microscope field. The number of capillaries with a diameter under 20 μm in each field was counted and the average number per field in the six photographs of the same sample was calculated. The average capillary density in the three groups was counted respectively.
Results
Porous collage membranes degraded after implanted into the infarcted heart
The porous structure of collagen was scanned by SEM (Model S-2500; Hitachi) (Fig. 1D). The pore size ranged from 200 to 500 μm and was suitable for the invasion and penetration of cells and new blood vessels.
We examined collagen membrane degradation by the general morphology of the rabbit heart at 4 and 12 weeks after the surgery (Figs. 3 and 4). The collagen membrane was integrated with myocardium at 4 and 12 weeks. The collagen membrane degraded over time and almost totally degraded at the end of 12 weeks.
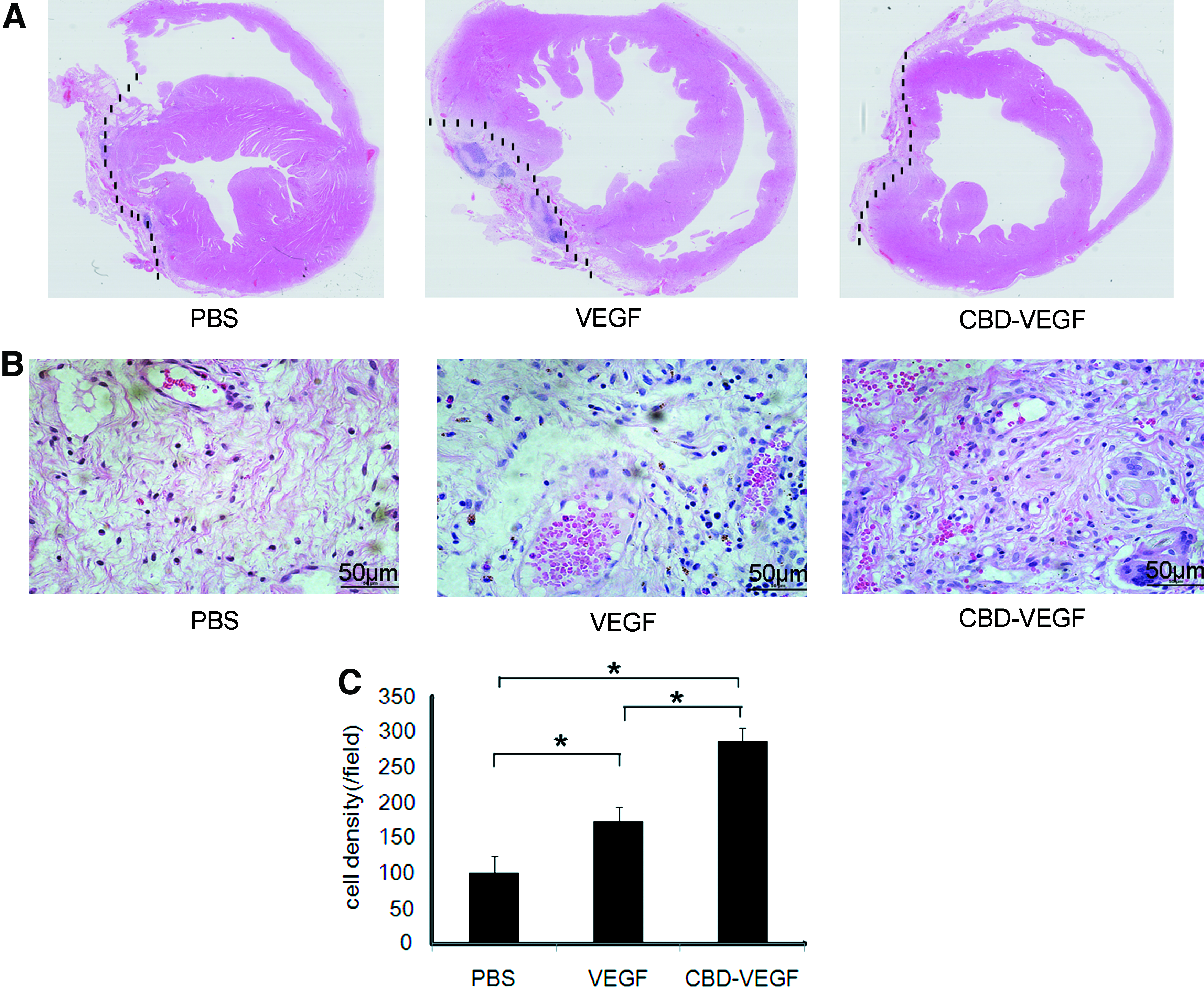
Histological analysis of hearts at 4 weeks after myocardial injuries.
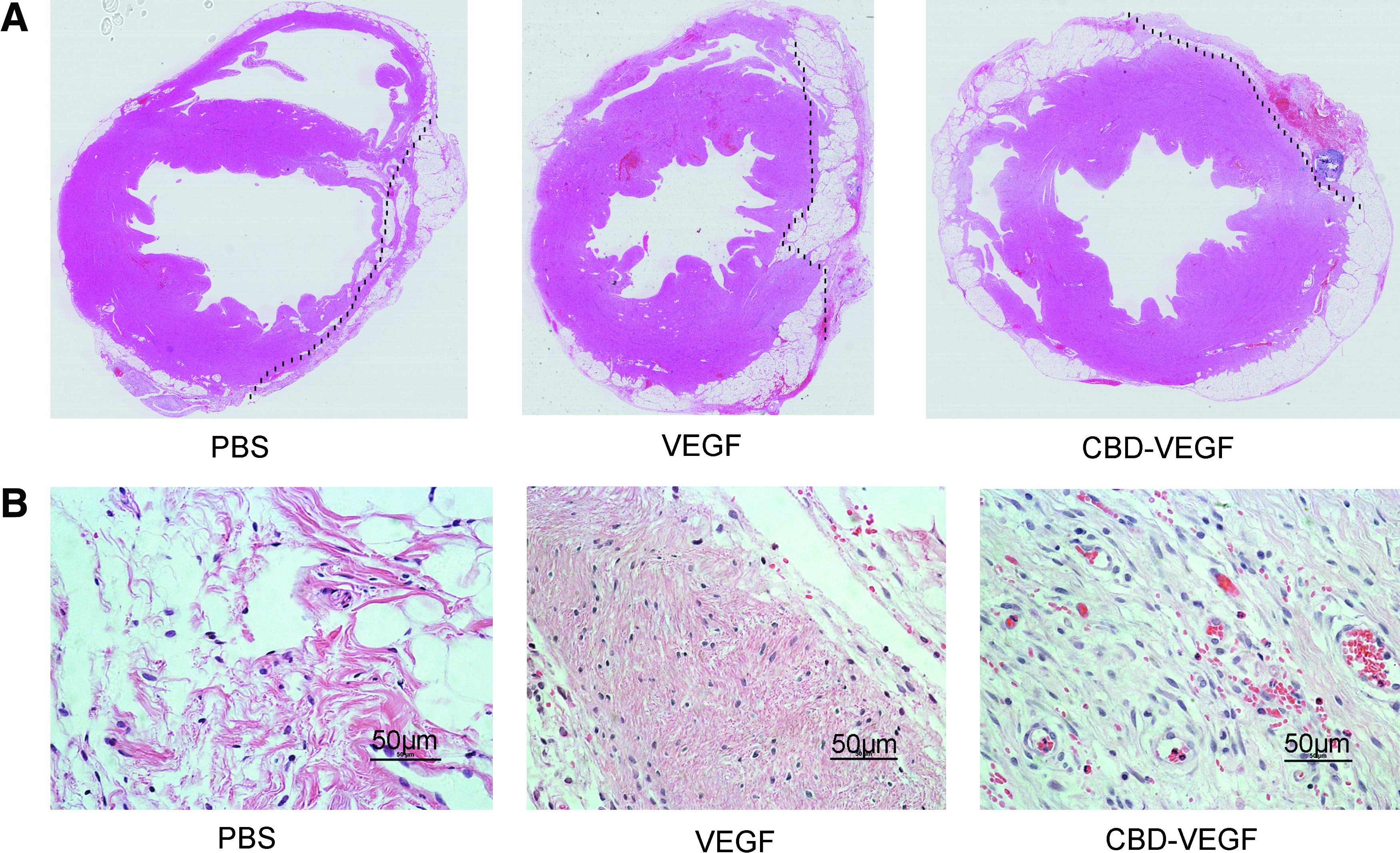
Histological analysis of hearts at 12 weeks after myocardial injuries.
CBD-VEGF/collagen improved cardiac function
The cardiac function was measured by echocardiography and hemodynamics at 4 or 12 weeks after the operation. The results presented in Table 1 summarize the data obtained from echocardiography at 4 and 12 weeks, respectively. The 4-week echocardiography data showed no difference among the three groups. At 12 weeks, the LVFS and LV ejection fraction (LVEF) in the CBD-VEGF/collagen group (LVFS: 37.23±4.09, LVEF: 71.43±4.85) were both significantly higher than the control PBS/collagen group (LVFS: 28.62±8.23, LVEF: 58.44±12.46; p<0.05). No significant difference was found between the VEGF/collagen group and the control PBS/collagen group in FS or EF. Hemodynamic examination results at 4 weeks after the operation in Table 2 show that the contractility of the CBD-VEGF/collagen group left ventricle (3127.33±274.26) increased compared with the control PBS/collagen group (1826.46±590.89) as indicated by the higher maximum dp/dt (p<0.05). The results at 12 weeks after the operation in Table 2 show a significant improvement in both maximum and minimum dp/dt in the CBD-VEGF/collagen group (maximum dp/dt: 3399.37±653.65, minimum dp/dt: −2833.19±543.48) and the VEGF/collagen group (maximum dp/dt: 3236.79±314.56, minimum dp/dt: −2642.92±239.43) compared with the control PBS/collagen group (maximum dp/dt: 2351.31±594.84, minimum dp/dt: −2016.48±479.03; p<0.05), which indicated that both systolic and diastolic functions were improved in the CBD-VEGF/collagen and VEGF/collagen groups after 12 weeks.
Data are mean±SEM. At 4 weeks, PBS/collagen, n=4; VEGF/collagen, n=3; and CBD-VEGF/collagen, n=4. At 12 weeks, PBS/collagen, n=5; VEGF/collagen, n=6; and CBD-VEGF/collagen, n=5.
p<0.05 versus control.
LVDs, left ventricular end-systolic dimension; LVDd, left ventricular end-diastolic dimension; FS, fractional shortening; EF, ejection fraction; IVSDT, interventricular septal diastolic thickness; LVPWT, left ventricular posterior wall thickness; LVAWT, left ventricular anterior wall thickness; PBS, phosphate-buffered saline; VEGF, vascular endothelial growth factor; CBD, collagen-binding domain; SEM, standard error of the mean.
Data are mean±SEM. At 4 weeks, PBS/collagen, n=4; VEGF/collagen, n=3; and CBD-VEGF/collagen, n=4. At 12 weeks, PBS/collagen, n=5; VEGF/collagen, n=6; and CBD-VEGF/collagen, n=5.
p<0.05 versus control.
LVSP, left ventricular systolic pressure; LVEDP, left ventricular end-diastolic pressure.
CBD-VEGF/collagen induced more cellularization after 4 weeks
Many cells infiltrated in the remaining collagen membrane. We analyzed the collagen membrane cellularization by counting the cells infiltrated in the remaining collagen membrane under H&E staining (Fig. 3). One-way analysis of variance (ANOVA) resulted in F=47.07 and p<0.05. Further analysis with least significant difference (LSD)-t test revealed that the cell numbers infiltrated in CBD-VEGF collagen (287.04±18.05) and VEGF collagen (174.17±19.91) were both higher than the cell numbers in PBS collagen (100.62±23.03). All the comparisons have significant differences (p<0.05). We have stained the slices using anti-von Willebrand factor antibody and anti-smooth muscle actin antibody. According to these two immunohistochemical analyses and H&E staining, ECs and myocardium cells were observed in the collagen membrane area. Among these cells, the myocardium cells were predominant. We did not find obvious inflammation in the collagen membrane area.
CBD-VEGF collagen increased angiogenesis in the infarcted myocardium
We examined the angiogenesis effect by measuring capillary density in the infarcted myocardium under the collagen membrane by immunohistochemical staining for smooth muscle actin (Fig. 5). One-way ANOVA resulted in F=29.03 and p<0.05. Further analysis with LSD-t test revealed that the capillary density of CBD-VEGF/collagen (290.18±43.19) was significantly higher than both the VEGF/collagen (134.54±30.68) and PBS/collagen groups (119.64±71.64). No significant difference was found between the VEGF/collagen group and the PBS/collagen group.
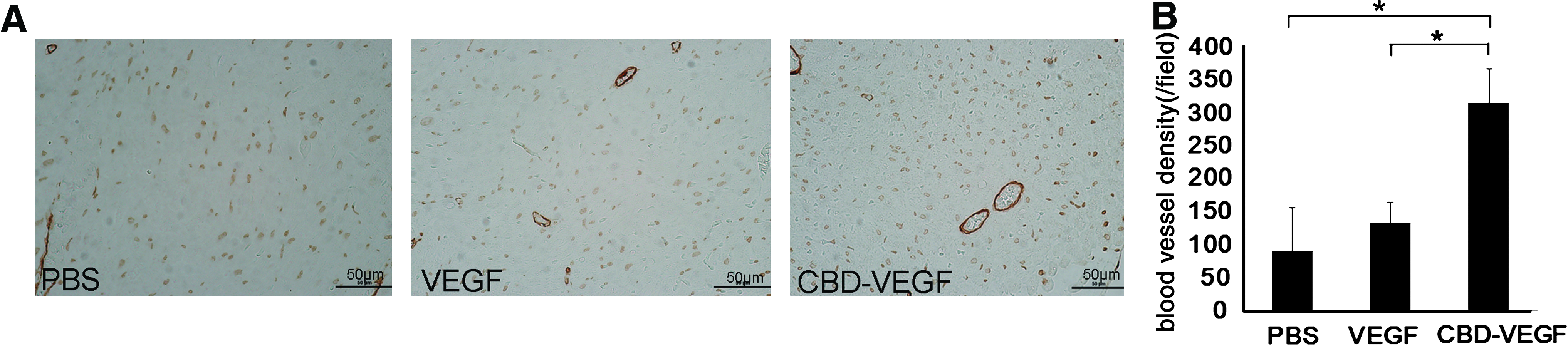
Immunohistochemical staining in infarcted region under collagen membrane at 12 weeks.
Discussion
Tissue-engineered cardiac patch could be able to replace the myocardial defects and effective to improve cardiac function. Traditional biomaterials are usually used as scaffold, which can provide adhesion sites and mechanical support. The modification of the scaffold is needed to increase the repair effect. Modification of the scaffold property to improve the local microenvironment and the addition of active factors such as stem cells or growth factors to the scaffold are mainly involved in current research.19–25 In 2005, Kochupura et al. used porcine urinary bladder ECM as a myocardial patch to repair a full-thickness defect in the right ventricle, and after 8 weeks, the ECM-derived myocardial patch provided better regional mechanical function compared with Dacron patch. 24 In 2005, Robinson et al. used ECM derived from porcine small intestinal submucosa and urinary bladder matrix to replace the infarcted myocardium. The ECM scaffolds retained matrix bound growth factors such as VEGF, which are considered to support cell growth and differentiation. 25 In 2008, Wei et al. used cardiac patch constructed from multilayered mesenchymal stem cells (MSCs). The MSC patches could restore the dilated LV and preserve cardiac functions after infarction. 23
Angiogenesis involves the formation of new capillary blood vessels from the existent microvessels. 26 Angiogenesis is the most important factor for cardiac repair. Proper special structure is beneficial to the diffusion of oxygen and nutrition, which is essential to the successful regeneration of myocardium.27,28 Metabolic waste in the recovery procedure could be removed in time, which is eventually beneficial to the formation, survival, regeneration, and differentiation of tissue cells.29,30 Impaired angiogenesis may influence the myocardial repair and lead to cardiac rupture or immature scar tissue formation. 31 The opinion that stimulating angiogenesis is beneficial to ischemic and infarcted heart has been demonstrated in numerous studies.32–34
Angiogenesis can be stimulated by multiple factors, including growth factors, cells, and mechanical stimulating.35–37 Among the various angiogenic growth factors, VEGF has been the most extensively studied. VEGF is a key mediator in the process of angiogenesis; it can induce the proliferation, migration, and tube formation of ECs.38–40 When VEGF is simply loaded to the collagen membrane, only a small quantity of VEGF will be retained after transplantation because of its rapid diffusion by blood flow and body fluid (Fig. 1A). Biomaterial-based angiogenic protein delivery offers promise for better control of local therapeutic angiogenesis. 8 Our previous results showed that CBD-VEGF could specially bind to the type I collagen.13,17,41–43 In this work, CBD-VEGF was added to the collagen membrane to form a cardiac patch. CBD acted as a substantial binding link between VEGF and the collagen protein on collagen membrane. Our previous work had proved that CBD could help the sustained release of the CBD fusion protein from collagen membrane in vitro effectively.42,44 This would indicate that CBD-VEGF would also be sustainedly released from the collagen membrane. Thus, CBD-VEGF could specially combine to the collagen membrane and prevent it from diffusion and also act as the angiogenesis factor and make the collagen membrane a functional biomaterial (Fig. 1B).
Our work showed that the collagen membrane was generally integrated with the myocardium after transplantation and was degraded over time. The cardiac function examinations including echocardiography and hemodynamics revealed that cardiac function of CBD-VEGF/collagen group increased compared with the PBS/collagen group. This indicated that CBD-VEGF on the collagen membrane helped to improve the cardiac function. According to the normal rabbit echocardiography reference, the EF and FS of normal rabbit would be 69.58±5.33 and 36.01±4.31, respectively. 45 We found that the myocardial function data of the experimental animal would be lower than the healthy animal even in the CBD-VEGF/collagen group. CBD-VEGF improved the cardiac blood flow at 4 and 12 weeks according to the hemodynamic results. This might be because CBD-VEGF slowly spread from collagen membrane; it could maintain a high local CBD-VEGF concentration. VEGF diffused fast from the collagen membrane and it did not cause an increase in cardiac blood flow at 4 weeks. But the administration of VEGF helped the cellularization of collagen membrane. The proliferation and migration of cells, especially the ECs, are important for angiogenesis. These migrated cells were beneficial for vascularization and cardiac function recovery. As a result, the hemodynamic studies showed that the blood flow increased in the VEGF/collagen group compared with the control.
At 4 weeks after implantation, the H&E staining of the cells within the transplanted collagen membrane showed the collagen membrane in CBD-VEGF/collagen with more cells compared with the VEGF/collagen and PBS/collagen. The results indicated that more CBD-VEGF could be retained on the collagen membrane. CBD-VEGF/collagen showed better attraction for the migration and proliferation of cells on collagen membranes.
The migration and proliferation of ECs are important to angiogenesis, and angiogenesis is important to supply nutrients for myocardial regeneration. 46 Neovascularization was observed in the infarcted myocardium. According to the smooth muscle actin staining, the vascular density in the infarcted myocardium of the CBD-VEGF/collagen was more than that of VEGF/collagen and PBS/collagen. VEGF concentration was reported to play a critical role during vasculature formation. 47 These results implied that VEGF concentration in the CBD-VEGF/collagen group was higher than in the VEGF/collagen group. This was because physical absorption of VEGF by the collagen membrane was rapidly diffused by blood flow and body fluid in vivo, and thus, the vascular density in VEGF/collagen showed no significant difference from PBS/collagen.
Conclusion
A cardiac patch was developed by combining collagen membranes with collagen-binding CBD-VEGF for myocardial injury repair. Implantation of CBD-VEGF collagen membrane into the infarcted myocardium could effectively improve left ventricle cardiac function and increase vascular density in a rabbit myocardial infarction model.
Footnotes
Acknowledgments
This work was supported by grants from National Natural Science Foundation of China (81061120528) and the “Strategic Priority Research Program” of the Chinese Academy of Sciences (Grant No. XDA01030401).
Disclosure Statement
No competing financial interests exist.