
Abstract
This study analyzed the long-term cartilage and subchondral bone repair of microdrilled defects treated with chitosan glycerol-phosphate/blood implant, using thrombin (Factor IIa) to accelerate in situ solidification. We also evaluated the cartilage repair response to six smaller microdrill holes compared with two larger holes. Bilateral knee trochlear cartilage defects were created in n=8 skeletally mature rabbits, drilled with six proximal 0.5 mm and two distal 0.9 mm holes, then covered with in situ-solidified IIa-implants (treated) or with IIa-alone (control). After 6.5 months of repair, cartilage repair tissues were analyzed by histological scoring and histomorphometry for hyaline matrix characteristics and osseous integration. Subchondral repair bone was analyzed by 3D microcomputed tomography and compared to acute defects (n=6) and intact trochlea (n=8). Implant-treated cartilage repair tissues had higher structural integrity through the entire defect (p=0.02), twofold higher percent staining for glycosaminoglycan (p=0.0004), and ∼24% more collagen type II staining over the smaller drill holes (p=0.008) compared with controls. Otherwise, hole diameter had no specific effect on cartilage repair. The subchondral bone plate was partially restored in treated and control defects but less dense than intact trochlea, with evidence of incomplete regeneration of the calcified cartilage layer. More residual drill holes (p=0.054) were detected in control versus treated defects, and control defects with more than 40% residual holes presented abnormally thicker trabeculae compared with treated defects. Low osteoclast numbers after 6.5 months repair suggested that bone was no longer remodeling. The subchondral bone plate surrounding the defects exhibited a significant thickening compared with age-matched intact trochlea. These data suggest that debridement and drilling can lead to long-term subchondral bone changes outside the cartilage defect. Compared with drilled controls, chitosan implants solidified with thrombin elicited a more hyaline and structurally integrated osteochondral unit, features needed for long-term durability.
Introduction
Current clinical use of chitosan-GP/blood implants involves a mini-arthrotomy approach and a 15 min waiting period for the implant to solidify in the defect. 12 To reduce the time interval for closing the surgical site, we developed a method whereby thrombin is applied to the drilled defect surface to accelerate implant in situ solidification time. 13 In skeletally mature rabbits, thrombin-solidified chitosan-GP/blood implants exhibit therapeutic effects on drilled cartilage repair compared with control defects treated with thrombin alone. Implants stimulated osteoclast formation, subchondral bone remodeling, and angiogenesis during the first 2 weeks postoperative, and promoted a more integrated and hyaline repair cartilage after 8 weeks of repair.14,15 The chitosan implant (with or without thrombin) also promoted a more complete subchondral bone repair at 8 weeks compared with drilled control defects.9,14,15 Drilled rabbit cartilage defects consistently show incomplete drill hole repair at 8–12 weeks postoperative, in several rabbit models, and incompletely repaired drill holes are frequently filled at the top with cartilage that shows signs of hypertrophy and endochondral resorption.9,14–18 The extent and influence of initial surgical bone damage and implant treatment on the long-term quality of cartilage and bone repair remain unclear.
Using microcomputed tomography (micro-CT), we recently showed in a skeletally mature rabbit model that the surgical debridement of the calcified layer followed by microdrilling removed a considerable quantity of subchondral bone plate. 19 Consequently, marrow-stimulation procedures should also be considered as initiating a bone repair response in addition to a cartilage repair response, where the durability of the cartilage repair tissue relies on adequate subchondral bone repair architecture. Incomplete bone repair was previously associated with a more fibrous superficial cartilage repair,9,14 and the presence of an advanced and irregular subchondral bone plate was associated with degradation of the repaired articular cartilage. 20 Thus, the evaluation of bone quality following cartilage repair procedures is becoming increasingly important and is related to bone strength, volume, microarchitecture, degree of mineralization, and bone remodeling. 21
The principle aim of this study was to evaluate the long-term quality and stability of the cartilage repair tissue and regeneration of the underlying bone structure after 6.5 months of repair in microdrilled cartilage defects treated with thrombin (IIa)-solidified chitosan-GP/blood implants. Repair cartilage quality was compared with contralateral defects treated with IIa-alone. Repair bone characteristics were compared with 1-day acute defects and intact knees of age-matched rabbits. The second aim was to determine whether six smaller-diameter versus two larger-diameter holes could improve marrow-derived cartilage repair in treated and control defects after 6.5 months in vivo. Cartilage repair was evaluated through the drill holes and between the drill holes by histology, whereas bone repair quality below the debrided cartilage defect area was evaluated using 3D micro-CT models.
Materials and Methods
In vivo articular cartilage repair using bone marrow stimulation
All animal experimentations were carried out following protocols approved by the University of Montreal Animal Division. Skeletally mature New Zealand White rabbits (n=11) were subjected to sequential small knee arthrotomies to create bilateral 3.5×4.5 mm full-thickness articular cartilage defects debrided into the calcified layer. Defects were then microdrilled with two distal 0.9 mm diameter holes and six proximal 0.5 mm diameter holes (all holes were 3–4 mm deep). 13 Alternating right and left defects were treated with 3 μL purified human thrombin (45 U/mL tissue culture-grade; Sigma-Aldrich) 13 followed by 1 hanging drop (∼25 μL) of sterile chitosan-GP/blood implant, using qualified medical-grade (BST-CarGel®, chitosan lots CG3020607B, CG3020612A, and GP lot CG5790606A; BioSyntech, for 6.5 month repair) or research-grade chitosan-GP containing rhodamine isothiocyanate (RITC)-chitosan fluorescent tracer 14 for 1 day repair (see Table 1). Contralateral control defects were treated with 3 μL thrombin-alone, as previously described.13,14 Trochlear defects were closed in layers using prolene nonresorbable sutures. Animals were allowed immediate, unrestricted, postoperative activity in cages. Femurs ends were collected 10 min after euthanasia by sodium pentobarbital intravenous injection under anesthesia. Intact trochlea from skeletally mature rabbits (9–12 months, n=4) were used to compare the healing state of the 6.5 months repair control and treated defects. Distal femoral ends of rabbit knees were fixed in 4% paraformaldehyde/100 mM cacodylate pH 7.4 or ethanol (intact trochlea), trimmed of the diaphysis and condyles, and scanned by micro-CT before histoprocessing (Table 1).
F, female; M, male; GP, glycerol phosphate; RITC, rhodamine isothiocyanate.
Histoprocessing, staining, immunohistochemistry, tartrate-resistant acid phosphatase staining, and digital slide scanning
At 6.5 months postoperative, many drill holes were completely repaired and no longer macroscopically visible. Therefore, specific criteria were taken to ensure the collection of serial sections in three distinct levels in the defect: through three proximal 0.5 mm diameter drill holes (3H), between the distal and proximal microdrill holes (BH), and through the two distal 0.9 mm diameter drill holes (2H) (Fig. 1A). Defect samples were decalcified in ethylene diamine tetraacetic acid/0.1% paraformaldehyde (up to 4 months, 4°C), transversely cut through the middle of the defect into the proximal and distal halves, then photodocumented with a dissection microscope (1.25×magnification), equilibrated in sucrose, and embedded in OCT. The location of the repaired drill holes in each cryoblock sample was estimated based on (1) digital photos taken of all defects at surgery, (2) calibrated line measurements (from the cut edges in the middle of the defect) of the decalcified defect images using histomorphometric software (Northern Eclipse; Empix), and (3) the use of a cryostat equipped with a digital micrometer to monitor the extent of trimming into each frozen sample edge (Leica Model CM3050S; Leica Microsystems). At each level (3H, BH, 2H) (Fig. 1A), serial cryosections with 10 μm thickness, two sections per slide and 14–30 consecutive slides per level were collected using the CryoJane tape system (Instrumedics). Each slide was assigned to a predetermined staining plan prior to histoprocessing, to ensure an unbiased assessment of overall defect repair. For sections that were unsuitable for analysis (torn, folded, poor staining), the nearest suitable serial section was restained and used for the analyses. All sections analyzed within a given level (3H, BH, 2H) were within 200 μm of each other. Sections were stained with hematoxylin eosin (to assess new tidemark), Safranin-O/Fast Green/Weigert Iron Hematoxylin (SafO), immunostained for collagen type II (col2, anti-collagen type II, clone II-II6B3; DHSB) and collagen type I (col1, anti-collagen type I, clone I-8H5; MP Biomedical), as previously described.14,22 Omission of primary antibody controls showed no staining. Sections through the distal holes were enzymatically stained for tartrate-resistant acid phosphatase (TRAP) to identify osteoclasts. 14 Stained slides were blinded and scanned at 40×magnification using a slide scanner (Hamamatsu Nanozoomer RS; Olympus Canada, Inc.). To allow calibration of the software used for measurements, an ISO-certified pinwheel micrometer slide was scanned along each sample batch and an image of the calibrated pinwheel was saved at the same magnification as the samples to permit appropriate scale bar calibration with the ImageJ (RSB-NIH) and Northern Eclipse software.
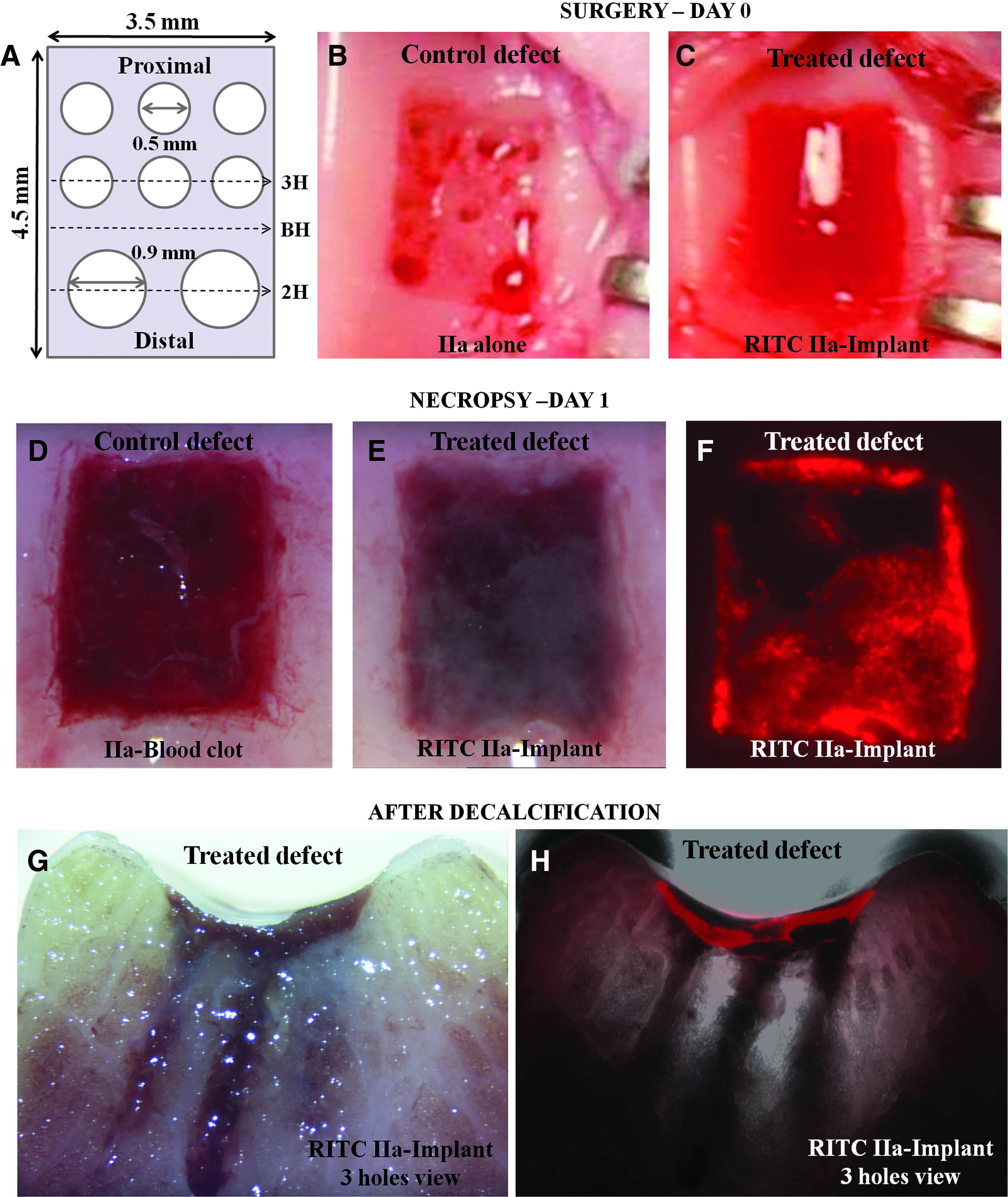
Macroscopic appearance of microdrilled cartilage defects at surgery and implant retention at 1-day postoperative.
Quantitative histomorphometry and histological scoring
Quantitative histomorphometry measurements were performed by one trained and blinded observer (C.M.) at three distinct levels in the cartilage defect area. Bias in the histomorphometric analyses was avoided through the use of blinded sections with an experimental and control group. Since each slide carried two sections, one of the two blinded sections was identified as the most intact or representative before scoring. Standardized methods were used to analyze the same portion of repair cartilage in all defects (i.e., between the two black arrows on Fig. 2, panels “b” and “g”), as previously described.9,14,23 A line or polygon tool was used to draw a line following a slightly curved projected tidemark through the repair cartilage-bone interface. Only soft repair tissue above the projected tidemark was analyzed. Percent detached repair tissue (cartilage repair tissue growing over and not integrated with bone) and percent integrated repair along the base of the defect was determined on SafO-stained sections by line measurements using Northern Eclipse software (Empix), as previously described. 9 Reproducibility of the line measures was verified by a second blinded reader (G.C.). Soft repair tissue above the projected tidemark was cropped and the cross-sectional area and threshold limits for Safranin-O, col1, and col2-stained tissue were obtained with ImageJ (RSB-NIH; Threshold Colour plugin by Gabriel Landini). An in house Matlab (Mathworks) routine was then used to automatically measure the cropped image area (representing the soft repair tissue cross-sectional area above the projected tidemark), and percent SafO, col1, and col2-positive repair tissue. Positively stained pixels for each stain were determined by using a single set of threshold limits in the hue-saturation-value colorspace. O'Driscoll histological scoring 24 with the modification of adding another 3-point value for subchondral bone health (0=cyst or fibrous tissue, 1=callus, 2=remodeling bone, 3=normal subchondral bone) was performed by a blinded observer (G.C.) on SafO-stained sections at the three levels, verified with scores generated by a second blinded observer (C.M.), and the median score (range) reported. For O'Driscoll scores that differed by 2 points or more between readers, a consensus was reached by the two observers while the sections were still blinded. 23
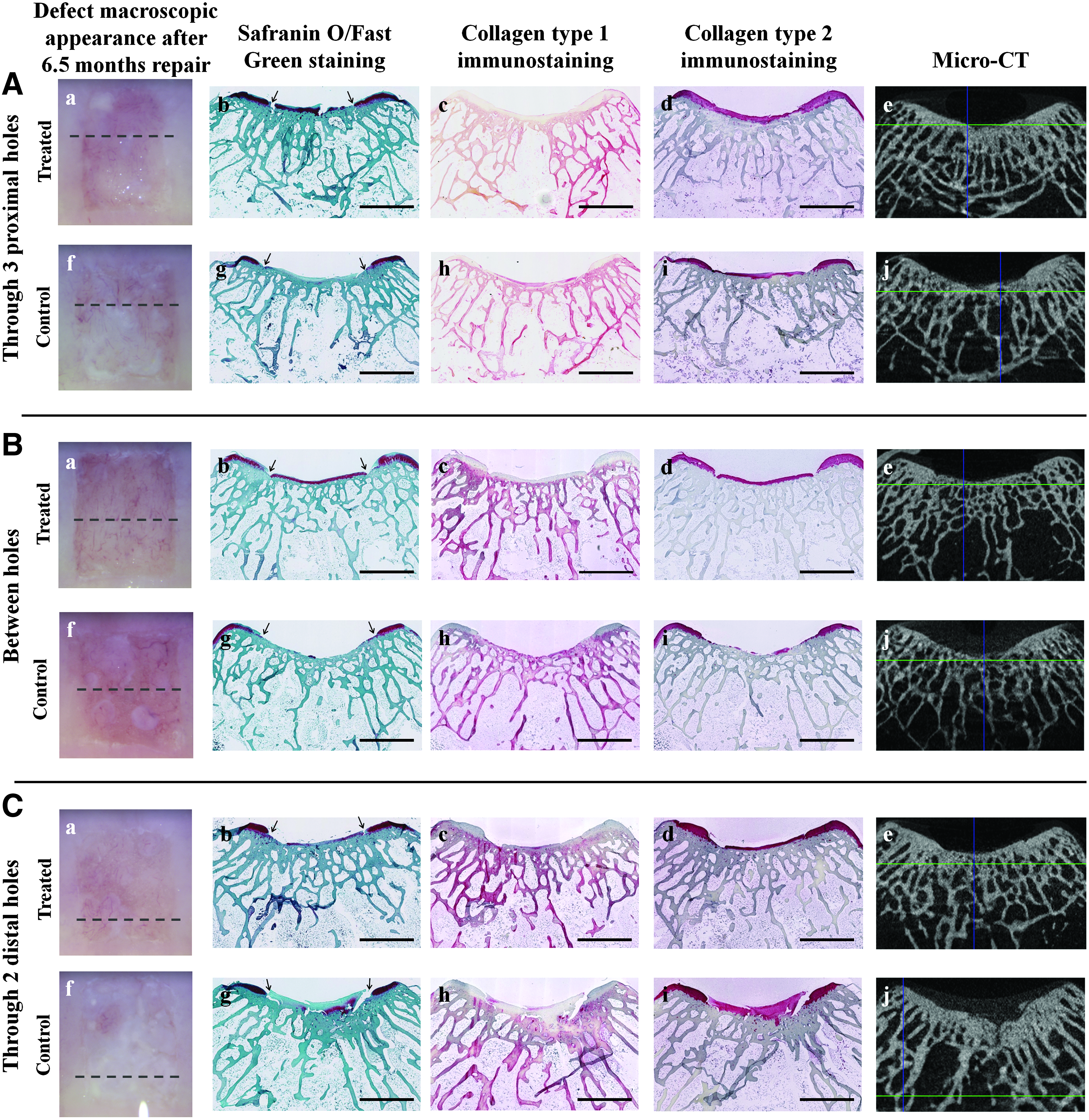
Representative macroscopic, histologic, and corresponding micro computed tomography (micro-CT) images of bilateral control and treated defects after 6.5 months of repair. Histology sections at three different levels in the repaired defect were analyzed for Safranin-O/Fast Green (FG)
Micro-CT evaluation of bone repaired tissue
Femur ends were micro-CT scanned (Skyscan model 1172; Skyscan) and the image stacks reconstructed and repositioned as previously described. 19 Subchondral bone structure in all samples (bone volume/tissue volume [BV/TV%], bone mineral density [BMD, g/cm3], object number, connectivity density [1/mm3], open porosity [%], and trabecular thickness distribution (μm)] was analyzed with CTAn software (Skyscan) using two distinct, standardized 3D volume of interest (VOI) models 19 : the rectangle-adapted surface (RAS) model consisted in a 3.5 mm wide and 1 mm deep transverse rectangle precisely adapted at the top to the slightly irregular defect surface, and interpolated 3.6 mm in length along the proximo-distal axis (see below, Fig. 4A) and the curved rectangle adapted surface (C-RAS) model with the same width and length but only 250 μm deep (see below, Fig. 4B). The C-RAS model was used to analyze bone within a specific anatomical region: the bone plate from 0.0 to 0.25 mm (TOP), the trabecular bone from 0.5 to 0.75 mm (MID), and the deeper trabecular bone from 1.0 to 1.25 mm (DEEP) below the defect surface.
The residual drill holes were identified by visually assessing the three orthogonal planes of the reconstructed and repositioned datasets using DataViewer software (Skyscan). To be qualified as a residual hole, its location should match the surgical photo for the original position of the surgical hole and the spacing from adjacent holes or the edge of defect. The residual holes also need to be seen through a minimal consecutive depth (≥100 μm) and confirmed in three view planes. Each identified residual hole was given a score of 1, with a maximum of eight detected residual holes per defect (eight holes=100%). Data were reported as the mean of percent residual holes±95% confidence intervals.
Statistical methods
The general linear model (GLM, Statistica version 6.1; StatSoft) was used to test the effect of treatment and level in the defect (3H, BH, 2H) on cartilage repair parameters including % SafO, % col1, % col2, tissue integration and detached repair. Treatment-specific differences in cartilage repair at each level were analyzed using the paired Student's t-test. The Mann-Whitney U nonparametric test (Statistica) was used to evaluate the effect of treatment on O'Driscoll histological scores at each of the three different levels in the defect (with exact values p<0.05 considered significant). GLM with repeated measures (TOP, MID, DEEP) was used to analyze the effect of treatment on the presence of residual holes. Analysis of variance of the mean (one-way ANOVA) with Tukey post hoc was used to analyze differences in subchondral BV/TV% and BMD (3D RAS and C-RAS VOI), and bone plate thickness outside the defect area for four groups: intact age-matched trochlea (n=8), acute defects (n=6), 6.5 month repair bone of control (n=8), and treated (n=8) defects. The Student's t-test was used to analyze the differences in bone parameters (object number, connectivity density, open porosity, C-RAS VOI) between intact (n=8) and repair bone (control and treated, n=8 each), and the paired Student's t-test was used to analyze differences in average trabecular bone thickness distribution for control defects with over 40% residual holes and matching contralateral treated defects (n=3). Significance was set at p<0.05.
Results
Macroscopic evaluation at 1 day and 6.5 months postoperative
All defects were debrided into the calcified layer and punctuate bleeding was sometimes observed from the debrided defect base (Fig. 1B). With thrombin (Factor IIa) preapplied to the defect surface, liquid chitosan-GP/blood implants solidified in situ on average within 3 min of application 13 (Fig. 1C). After 1 day of repair and unrestricted cage activity, all defects were homogeneously covered with IIa-blood clot or IIa-chitosan-GP/blood implant over the entire defect area (Fig. 1D–F). IIa-chitosan implants were contiguous with bone marrow-derived clot filling the drill holes (Fig. 1G, H) as revealed by the red fluorescent RITC-chitosan tracer in the day 1 implants (Fig. 1F, H). For the purpose of brevity, drilled defects that received IIa-alone are from here on referred to as “control defect” and IIa-implant-treated defects as “treated defect.”
After 6.5 months of repair, four treated defects, and one control defect, out of n=8 were covered with a homogeneous, glassy repair tissue with visible blood vessels underneath, the best of which corresponded to a thin, hyaline-like repair (Fig. 2 panel B-a). Most control defects were either incompletely resurfaced with white tufts over the drill holes (Fig. 2 panel B-f ), or filled with an inhomogeneous white opaque repair tissue that most frequently corresponded to a fibrous or fibrocartilage tissue (Fig. 2 panel C-f ). Osteophytes not present at surgery were observed with a distinct “ball” shape in some control and treated defects along the trochlear ridges notably where the surgical retractors were systematically laid (data not shown).
Histologic study of cartilage repair
After 6.5 months repair, an irregular tidemark was observed where new cartilage repair tissue (fibrocartilage or hyaline-like) was integrated with the subchondral bone, in control or treated defects. The calcified cartilage layer, when present, was very thin and irregular (∼10–60 μm) compared with the calcified layer of intact trochlea in skeletally mature rabbits, which has been previously evaluated to be ∼70–100 μm thick.9,25
Cartilage repair tissue after 6.5 months of repair was significantly more hyaline in treated versus control defects, throughout the three levels analyzed (3H, BH, 2H) according to an approximately two-fold increase in SafO staining for glycosaminoglycan p=0.00043, Fig. 3A), higher % col2 immunostaining above the proximal smaller drill holes (p=0.0076, 82% vs. 58% black bars, Fig. 3B) and low col1 immunostaining (Fig. 3C). Interestingly, treated repair tissue was ∼15% more integrated at the cartilage-bone interface versus controls throughout the defect (p=0.021, Fig. 3D–F). The average soft repair tissue cross-sectional area in transverse sections above the projected tidemark was slightly lower in treated versus control defects (∼0.36 vs. 0.55 mm2, data not shown). In control defects, the repaired cartilage tissue was often observed “sprouting” from the holes and expanding over adjacent bone without significant adhesion (Fig. 3G–I), an observation also made in other studies, in microdrilled cartilage defects after 2–3 months of repair.9,18,24,25 The same level of ≤20% exposed mineral was seen along the repaired bone base of control and treated defects.

Cartilage repair tissue after 6.5 months of repair was analyzed at three different levels in the defect by quantitative histomorphometry for percent staining for Safranin-O/FG
O'Driscoll histological scoring showed that repair tissue of treated defects had significantly better structural integrity than control tissue through all the levels analyzed (3H, BH, 2H), better surface regularity through the two distal larger holes, and higher overall scores between the holes and through the proximal smaller holes (p<0.05, Table 2). Over the small proximal holes, repair tissue of treated defects had a higher chondrocyte cellular morphology than control repair tissue (p<0.05, Table 2), consistent with the superior SafO and col2 staining observed in this area (Fig. 3A, B). Otherwise, drill hole diameter showed no specific effects on cartilage repair, when treated or control defects were separately analyzed (compare 3H vs. 2H, Table 2, Fig. 3).
p<0.05 compared with control.
p<0.01 compared with control.
p<0.005 compared with control.
Micro-CT subchondral bone analysis
Treatment-related improvements observed in soft tissue cartilage repair integration, percent SafO staining, structural integrity, and chondrocyte cell phenotype were not paralleled by different repair bone 3D features in control and treated defects, using two distinct VOI models. Micro-CT analyses showed that treated and control 3D bone repair tissues were strikingly similar after 6.5 months of repair, but different from intact trochlea. In a curved subchondral bone 3D VOI encompassing the defect area and 1 mm deep (Fig. 4A), intact trochlea had a 71% bone volume fraction (BV/TV%) that was reduced to 22% by debridement and drilling, 19 and increased to ∼54% in treated and control defects after 6.5 months of repair (Fig. 4B). Bone regeneration after 6.5 months was incomplete, attaining ∼63% bone volume fraction (p<0.05) and ∼75% of the native BMD (p<0.01) of intact trochlear bone (Fig. 4B, C). When the TOP, MID, and DEEP trabecular bone regions were separately analyzed using 250-μm-thick 3D VOIs (Fig. 4D), similar BV/TV% and BMD values for each of the three regions were observed between control and treated bone repair tissue, that were only 54%–80% of the matching volume analyzed in intact trochlea (Fig. 4E, F). The TOP zone had the most bone depletion in acute defects, and control and treated defects had the lowest bone regeneration ratio (54% and 64%, respectively) of the three zones analyzed when compared with intact trochlea (p<0.005, Fig. 4E, TOP).

Quantification of 3D subchondral bone repair features of intact trochlea, acute defects, and 6.5 months repaired defects using 3D adapted-surface volume of interest (VOI) models rectangle-adapted surface (RAS)
Subchondral bone mineralization 3D features in the TOP, MID, and DEEP trabecular bone regions also showed evidence of incomplete repair, as reflected by a high number of objects, that were highly connected with a much higher open pore structure, compared with intact trochlea (Fig. 5, panels A1–A4, B1–B4, C1–C4). The bone trabecular architecture of the repaired subchondral bone plate (control and treated defects) showed a broad range of thinner trabecular structures compared with intact trochlea (Fig. 5, panels A5–C5). The most striking differences between repair and intact bone were in the bone plate area (p<0.005, Fig. 5 panels A1–A5). The bone plate features in repaired defects more resembled trabecular bone, versus the typically dense bone plate of intact trochlea. These data were consistent with a much thinner and irregular calcified cartilage layer histologically observed at the repair cartilage-bone interface (see e.g., Fig. 3F).

Three-dimensional bone structural features analyzed using 3D adapted-surface VOI C-RAS model within the TOP
A close assessment of all 3D micro-CT images revealed more residual drill holes (both smaller 0.5 mm and larger 0.9 mm diameter, p=0.054), in subchondral bone of controls compared with treated defects, particularly in bone regions 500 and 1000 μm from the surface (Fig. 6A–C). An abnormal thicker trabecular distribution profile was observed in three control defects with the highest residual hole numbers (≥40%) that was not observed in contralateral treated defects in the same animals (Fig. 7A vs. B). As shown by the trabecular distribution profiles in these defects, trabeculae were significantly thicker in control repair bone compared with treated defects (Fig. 7C, D), especially in the DEEP bone region (*p≤0.0083, Fig. 7D).
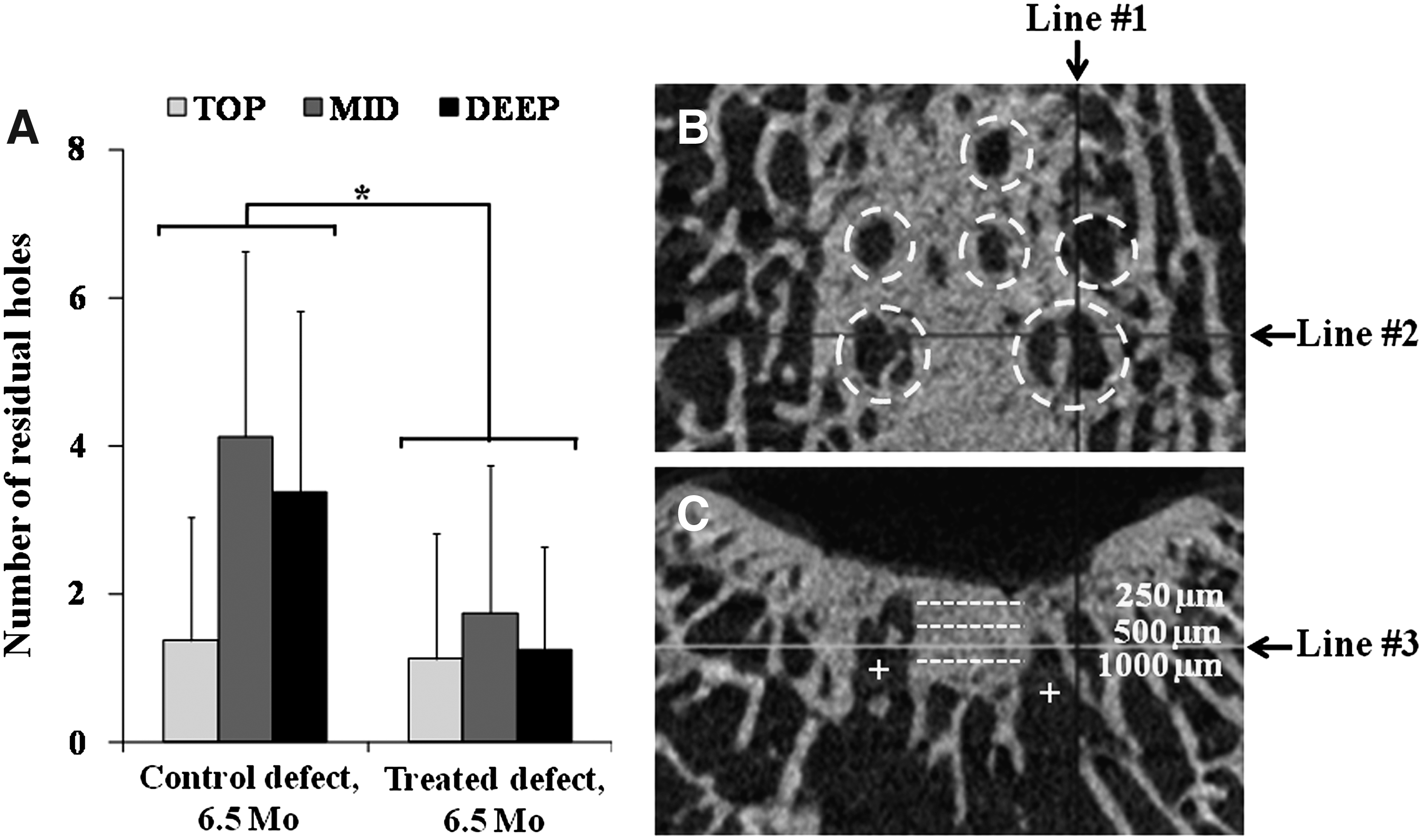
More residual drill holes were detected in control versus treated defects after 6.5 months of repair, especially in the MID and DEEP zones. Residual holes were quantified within three bone regions relative to the surface of the bone plate: TOP (0–250 μm, light gray column), MID (500–750 μm, gray column), and DEEP (1000–1250 μm, black column)

Thicker repairing bone trabeculae were observed in three control defects with the highest residual hole (HRH) numbers (≥40%) [
In bone areas proximal and distal to the trochlear defects, a general subchondral bone plate thickening was detected after 6.5 months of repair in all trochlea carrying marrow stimulation defects, compared with intact trochlea and compared with acute defects, at day 1 postoperative (p<0.0001, Fig. 8). Note that the bone plate thickness measured in surrounding areas included calcified cartilage, which sometimes showed a duplicated tidemark in flanking cartilage adjacent to 6.5 month repaired defects. A similar and low TRAP+osteoclast (OC) density was seen in sections through the larger drill holes in both treated and control defects (∼0.04 TRAP+OC/mm2), reflecting a negligible level of bone remodeling at 6.5 months postoperative (data not shown).
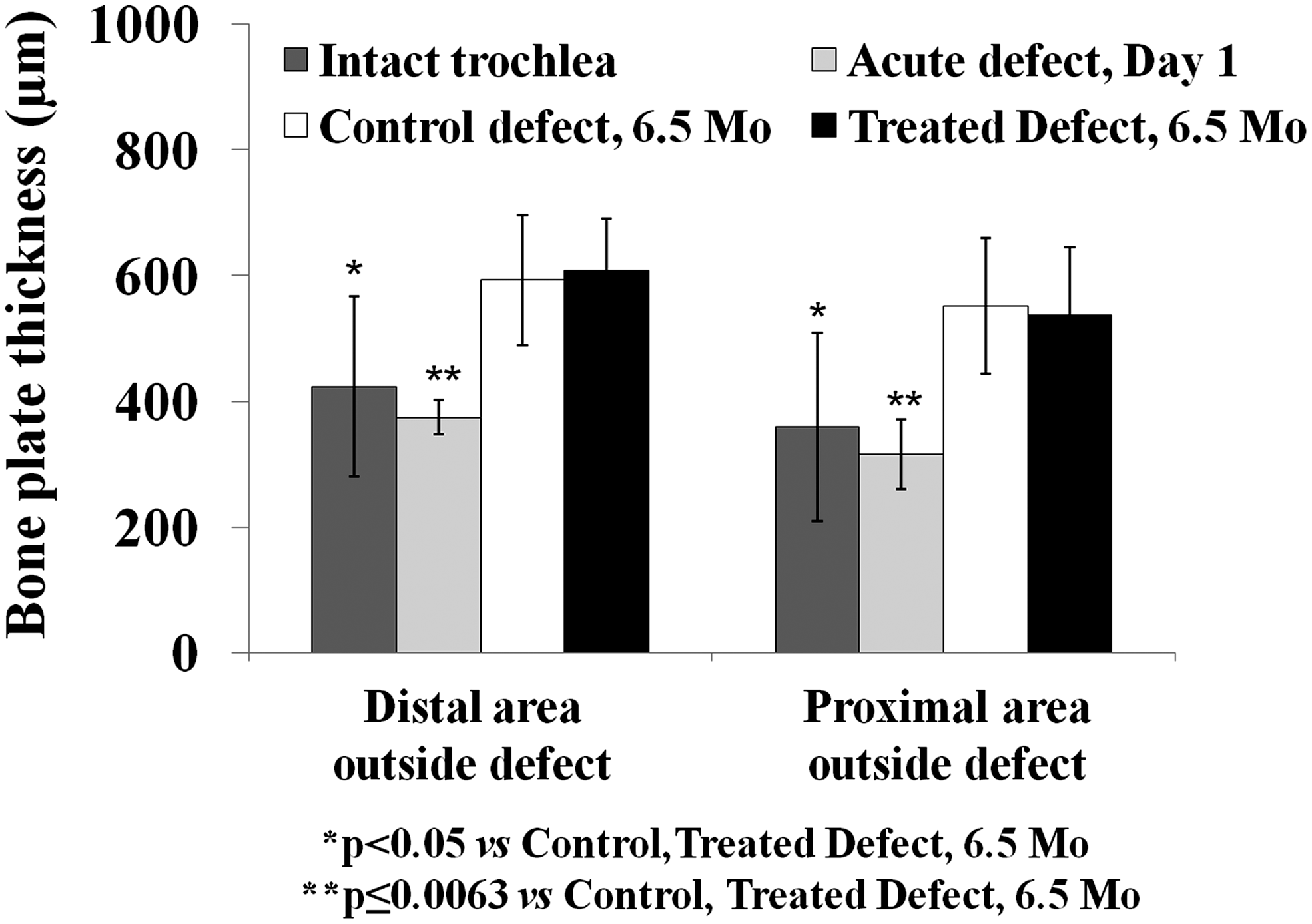
A significant bone plate thickening was detected in the bone surrounding control (n=8) and treated defects (n=8) after 6.5 months of repair, when compared with matching areas of intact trochlea (n=8) and acute defects, day 1 (n=6). Treated versus control data were not statistically different. Data are presented as mean±standard deviation. Symbols: *p<0.05 versus control, treated defect, 6.5 months, **p≤0.0063 versus control, treated defect, 6.5 months.
Discussion
Thrombin-solidified chitosan-GP/blood implants elicited better cartilage-bone integration, structural integrity, and hyaline matrix quality after 6.5 months of repair postdrilling, compared with thrombin-alone. Thrombin accelerates in situ solidification of the implant 13 and reduces the arthrotomy time. Although thrombin is also known to exert many positive effects on different cells types implicated in wound healing,26–29 it is difficult to argue that thrombin alone had any positive effects on cartilage repair, given the similar detached and heterogeneous repair tissue morphology obtained with and without thrombin treatment of drilled control defects at 2 months9,14 and 6.5 months (Fig. 3 in this article). Given the excessive levels of antithrombin in blood, 30 we conclude that thrombin acted quickly, locally, and directly on implant solidification.
Our results extend previous studies using chitosan-GP/blood implants with an earlier 2 month repair endpoint, and show that the therapeutic effects of chitosan-GP/blood implant on cartilage repair at 2 months are maintained after 6.5 months of repair, including better cartilage repair integration and histological scores for hyaline matrix.9,14 It was previously observed at 2 months postoperative that the average percent GAG throughout the cartilage repair tissue was more variable in control defects (15–48% GAG) than chitosan implant-treated defects (40%–48% GAG, n=7) 14 , whereas in this study at 6.5 months postoperative, control tissues showed significant GAG depletion (12%–23% GAG) compared with implant-treated defects (30%–54% GAG treated n=8, p=0.00043, Fig. 3). It is well known that GAGs are crucial for the biomechanical function of the cartilage tissue. In our study, the lower overall GAG composition in repair tissue of control defects was associated with the presence of a more detached and less integrated repair tissue at the cartilage-bone interface of the repaired defect. Altogether, these data are consistent with the notion that tissue durability is critically dependent on cartilage-bone integration that is promoted by chitosan-GP/blood implant treatment.
Repaired bone had a significantly different bone architecture compared with intact femoral trochlea, mainly in the superficial subchondral bone plate area, where endochondral ossification is favored in repairing osteochondral defects.6,10 Superficial repair bone contained an irregular tidemark, a thin calcified cartilage layer, and high open porosity, number of objects and connectivity density. Usually, a higher connectivity density is explained by a higher number of trabeculae. But in the case of repaired bone plate, the high connectivity density along with a high object number may be best explained by many small mineralized structures fully isolated from other ones, such as mineralization foci observed in forming bone31,32 that have multiple projections with many connections. During the human bone repair process, once new bone has formed, its mineralization will quickly reach a level of 65%–70%, but to fully mineralize it will take 6–12 months or even more.33,34 The slow and gradual maturation of the mineral component during the secondary mineralization will lead to an increase in the amount of crystals and/or an augmentation of crystal size toward their maximum dimensions. 35 Our data show that the bone plate mineralization after 6.5 months of repair has not yet formed a dense and uniform mature mineralized network, and has not regenerated a substantial layer of calcified cartilage.
After 2 months of repair in this rabbit model, many untreated drill holes are filled at the top with cartilage instead of bone.9,14 In this study, we showed that this subchondral cartilage will proceed through endochondral ossification to form bone in the bone plate area at 6.5 months (Fig. 5 panels A1–A5). Soft cartilage repair tissue formed at 2 months in drilled control defects 14 did not clearly improve during the subsequent 4.5 month repair period in this study, suggesting that the quality of hyaline cartilage formation is generated during a relatively narrow 2-month time frame in this rabbit repair model; after 2 months the bone is largely reformed, sealing off access of the repairing defect to bone marrow progenitor cells. These data are also consistent with the observation that cartilage foci that form in response to drilling will resorb to bone when they arise too deep in the drilled defect, and can generate articular cartilage repair when situated at the surface of the repair tissue. 17
Our micro-CT quantitative analyses of specific bone regions revealed few differences between control and treated defects at 6.5 months of repair. In other rabbit cartilage repair studies, early differences in bone features between experimental groups were no longer present after 6 months of repair.36,37 We detected a general thickening of the subchondral bone plate in both control and treated defects in the area surrounding the defect (Fig. 8), a phenomenon previously linked to osteoarthritis. 33 Moreover, thicker trabeculae were observed, mainly in control defects that had a score of residual holes over 40% (Fig. 7C, D). The mechanisms driving this bone repair response are unclear, although abnormal mechanical loading, 38 and osteocyte-driven osteoblast activity and bone formation in response to mechanical load38–40 could be involved. The creation of an acute trochlear defect, along with drill holes, will lead to uneven load-sharing in the surrounding cartilage and subchondral compartment that in turn could stimulate trabecular thickening to locally compensate for the failure to repair drill holes. By comparison, chitosan-GP/blood implants were shown to stimulate a “wound bloom” phase, 14 during which remodeling and enlargement of the drill hole edge permits more cell influx to the drill hole and eliminates drilled hole boundaries—a phenomenon not observed in control defects.10,14 Differential stimulation of bone remodeling could explain the lower number of residual holes and higher cartilage repair integration in treated knees, and the persistence of drill holes and incomplete soft tissue integration in most of the control knees.
Conclusions
Marrow stimulation in conjunction with thrombin-solidified chitosan-GP/blood implant elicited a coordinated osteochondral repair response that resurfaced the defect with a more hyaline and integrated tissue that remained stable for 6.5 months repair. By contrast, treatment of drill holes with thrombin-alone resulted in a more detached and structurally inferior cartilage repair, especially over smaller drill holes, and abnormal repair bone trabecular thickening and persistence of residual drill holes in three out of eight control defects. In situ-solidified chitosan implants have the potential to improve the clinical outcome of marrow stimulation, a first-line treatment for focal cartilage defects.
Footnotes
Acknowledgments
The data presented in this article are part of the Ph.D. thesis at the École Polytechnique, Montréal, Quebec, Canada of C.M. Most of the data were presented at the 56th annual meeting of the Orthopaedic Research Society, 2010. We thank Geneviève Picard and Corine Martineau for valuable technical support. This work was supported by the Canadian Institutes of Health Research (CIHR, 185810-BME). Salary support was provided by the Canadian Arthritis Network (C.M.), Fonds de la Recherche en Santé du Quebec (FRSQ; C.M. and C.D.H.), FRSQ Groupe de Recherche en Sciences et Technologies Biomédicales (N.T.K.), and BioSyntech (J.S.).
Disclosure Statement
It is disclosed that CM is a consultant (since April 2011) for Piramal Healthcare Canada. None of the other authors have competing financial interests.