
Abstract
Porous polyethylene (Medpor®) is frequently used in craniofacial reconstructive surgery. The successful incorporation of this alloplastic biomaterial depends on adequate vascularization. Here, we analyzed whether the early vascularization of porous polyethylene can be accelerated by vitalization with human chondrocytes. For this purpose, small polyethylene samples were coated with platelet-rich plasma (PRP) or a suspension of PRP and human chondrocytes. Uncoated polyethylene samples served as controls. Subsequently, the samples were implanted into the dorsal skinfold chamber of CD-1 nude mice to repetitively analyze their vascularization and biocompatibility by means of intravital fluorescence microscopy. PRP-chondrocyte-coated polyethylene exhibited an accelerated and improved vascularization when compared with the other two groups. This was indicated by a significantly higher functional capillary density of the microvascular network developing around the implants. Moreover, a leukocyte-endothelial cell interaction was found in a physiological range at the implantation site of all three groups, demonstrating that the vitalization with PRP and chondrocytes did not affect the good biocompatibility of the alloplastic material. Additional histological, immunohistochemical, and in situ hybridization analyses revealed that the chondrocytes formed a bioprotective tissue layer, which prevented the accumulation of macrophages and foreign body giant cells on the polyethylene surface. These findings clearly indicate that vitalization of polyethylene with chondrocytes promotes early implant vascularization and incorporation into the host tissue and, thus, may be a promising approach that prevents postoperative complications such as implant extrusion, migration, and infection.
Introduction
To overcome this problem, porous polyethylene implants may be vitalized with an autologous layer of chondrocytes. For this purpose, chondrocytes could be harvested from a patient by biopsy, expanded in vitro, and subsequently seeded on the alloplastic material. In this case, the polyethylene provides a three-dimensional shape and a stable backbone to the implants, whereas the chondrocytes may act as a bioprotective layer, which improves the incorporation of the implants into the surrounding host tissue. 6 In line with this view, Monroy et al. recently demonstrated in a pig model that chondrocyte-coated polyethylene implants healed 30% faster than nonseeded controls when subjected to experimental exposure after a chronic implantation period of 10 weeks. 7
Therefore, the aim of the present study was to analyze whether vitalization with human chondrocytes improves the vascularization of porous polyethylene during the first 14 days after implantation. This early observation period may be of major importance for the successful incorporation of the implants without the development of infections at the implantation site. In fact, Sclafani et al. reported that polyethylene implants are, in particular, susceptible to infection when exposed to bacteria before the ingrowth of newly formed blood vessels from the surrounding host tissue. 8
For our analyses, we coated porous polyethylene with human chondrocytes, which were suspended in platelet-rich plasma (PRP). PRP is a portion of the blood plasma fraction having a platelet concentration above baseline 9 that forms a solid gel after activation and, thus, can easily be used for coating of alloplastic materials. PRP-chondrocyte-coated as well as PRP-coated and uncoated control polyethylene samples were implanted into the dorsal skinfold chamber of CD-1 nude mice. In previous studies, we and others could demonstrate that this model is an excellent tool that repetitively studies in vivo the vascularization and biocompatibility of implants by means of intravital fluorescence microscopy.10–12 In addition, PRP-chondrocyte-coated polyethylene samples were subcutaneously implanted into the flank of CD-1 nude mice to study chondrocyte maturation over a longer observation period of 6 weeks.
Materials and Methods
Isolation of human chondrocytes
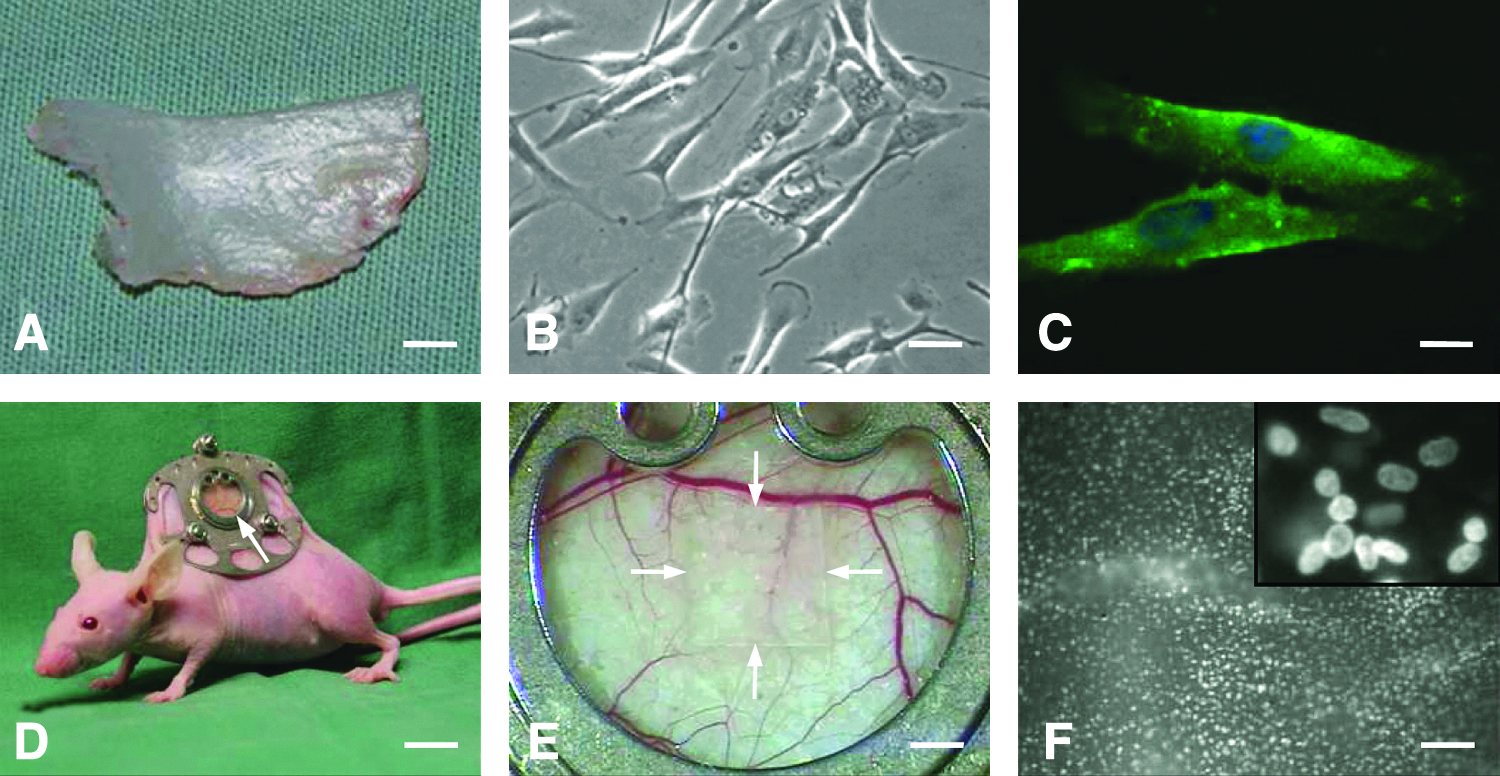
Human chondrocytes were isolated from nasal septal cartilage collected at the Department of Otorhinolaryngology, Head and Neck Surgery of the University of Saarland, Germany, with approval of the local ethics committee (Fig. 1A). All patients were informed and gave their written consent.
Fresh cartilage tissue from two female and five male patients at the age of 21 to 48 years was minced and digested with a three-step digestion protocol: 30 min at 37°C with 0.125% trypsin in Dulbecco's phosphate-buffered saline (PBS; PAA, Pasching, Austria); 1 h at 37°C with 1 mg/mL hyaluronidase (Type I-S, 440 U/mg; Sigma, St. Louis, MO) in Dulbecco's PBS; and overnight at 37°C with 1000 U Worthington collagenase II (Cellsystems, Troisdorf, Germany) in Dulbecco's modified Eagle's medium (DMEM)-Low Glucose plus 2.5 μg/mL amphotericin B and 1% penicillin/streptomycin (PAA). Between the digestion steps, two washings with Dulbecco's PBS were performed. Digested cells were separated with a 100 μm cell strainer and subsequently cultivated and expanded in DMEM-Low Glucose plus 10% fetal calf serum, 1% penicillin/streptomycin, 2.5 μg/mL amphotericin B, 1 mM sodiumpyruvate, and 80 μg/mL
Implant preparation
Four weeks after isolation and cultivation of human chondrocytes, micro-thin sheets of porous polyethylene (Medpor; DIM 38×50×0.25 mm; Porex Surgical Inc., Newnan, GA), which were carefully cut with a scalpel into small samples of 3×3×0.25 mm under a stereomicroscope, were coated with PRP or a suspension of PRP and chondrocytes. To guarantee a comparable content of growth factors in each PRP-coated implant, the entire PRP used in the present study was extracted from a single blood sample of a human donor. The PRP was collected in an S-citrat monovette 9NC (Sarstedt, Nümbrecht, Germany) by centrifugation of the monovette for 15 min at 110 g. For implant coating, 5 μL PRP alone or enriched with 5×105 chondrocytes was activated with 0.5 μL thrombin (Sigma Aldrich) to form a gel and was placed immediately on the upper side of the scaffold. Subsequently, the lower side of the polyethylene implant was coated in the same way. Uncoated polyethylene implants served as controls.
To analyze the distribution and viability of the chondrocytes directly after the coating procedure, the cells were stained with the fluorescent dye bisbenzimide (H33342; Sigma Aldrich). For this purpose, the PRP-chondrocyte-coated implants were placed for 1 min in a 30-mm-diameter Falcon plastic Petri dish filled with 37°C warm PBS and 200 μg/mL bisbenzimide. Then, the implants were carefully washed in 37°C warm bisbenzimide-free PBS for 2 min before implantation into the dorsal skinfold chamber.
Dorsal skinfold chamber model
Vascularization and biocompatibility of PRP-coated, PRP-chondrocyte-coated, and uncoated polyethylene implants were analyzed in the dorsal skinfold chamber model, as described in earlier biomaterial studies.10,13,14 To avoid rejection of the cell-coated implants, the dorsal skinfold chamber was prepared in immunoincompetent CD-1 nude mice (body weight: 22–25 g) lacking a T cell-mediated adaptive immune response (Fig. 1D). The animals were housed one per cage and received tap water and standard pellet food (Altromin, Lage, Germany) ad libitum. All experiments were approved by the local governmental animal care committee and were conducted in accordance with the German legislation on protection of animals and the NIH Guidelines for the Care and Use of Laboratory Animals (NIH Publication #85-23 Rev. 1985).
For the preparation of the chamber, the mice were anesthetized by an intra peritoneal (i.p.) injection of ketamine (75 mg/kg body weight; Pharmacia GmbH, Erlangen, Germany) and xylazine 2% (15 mg/kg body weight; Rompun, Bayer, Leverkusen, Germany). Two symmetrical titanium frames were implanted on the extended dorsal skinfold of the animals, so that they sandwiched the double layer of skin. One layer of skin was then completely removed in a circular area of ∼15 mm in diameter, and the remaining layers, consisting of striated skin muscle, subcutaneous tissue, and skin, were covered with a removable coverslip within the observation window of one of the titanium frames. 15 To exclude alterations of the microcirculation due to anesthesia and surgical trauma, the mice were allowed to recover for 72 h before implantation of the polyethylene samples.
For the implantation of the polyethylene samples, the cover glass of the chamber was removed, and one sample was carefully placed onto the striated muscle tissue within the center of each chamber, taking care to avoid contamination, mechanical irritation, or damage of the host tissue (Fig. 1E). Subsequently, the chamber was closed again with a novel cover glass.
Intravital fluorescence microscopy
For in vivo microscopic observation, the mice were fixed on a Plexiglas stage, which allowed for horizontal positioning of the dorsal skinfold chamber under the microscope. Subsequently, 0.1 mL 5% fluorescein isothiocyanate (FITC)-labeled dextran 150,000 for contrast enhancement by staining of blood plasma and 0.1 mL 0.1% rhodamine 6G (Sigma Aldrich) for direct in vivo staining of leukocytes were intravenously injected via the retrobulbary space. 16 Intravital fluorescence microscopy was performed by means of a Zeiss Axiotech microscope (Zeiss, Oberkochen, Germany) with a 100 W mercury lamp attached to an epi-illumination filter block for blue, green, and near-ultraviolet light. The microscopic images were recorded by a charge-coupled device video camera (FK6990; Pieper, Schwerte, Germany) and transferred to a DVD system for off-line evaluation. By means of 5×, 10×, and 20× long-distance objectives (Zeiss) magnifications of ×115, ×230, and ×460 were achieved on a 14 inch video screen (KV-14CT1E; Sony, Tokyo, Japan). 16
Microcirculatory analysis
The microscopic images were quantitatively analyzed by means of the computer-assisted image analysis system CapImage (Zeintl, Heidelberg, Germany). Leukocyte-endothelial cell interactions and microhemodynamics were assessed at a magnification of ×460 in four different microvascular regions of interest (ROIs) in the border zones of the polyethylene implants. In each ROI, one to three postcapillary or collecting venules were selected for analysis. To guarantee that identical standard locations for ROIs were visualized at each observation time point, images of ROIs were printed out with a video printer (UP-895CE; Sony) during the first microscopy, that is, directly after implantation of the polyethylene samples into the dorsal skinfold chamber. These ROIs were then repetitively analyzed throughout the entire in vivo experiment.
Leukocytes were classified according to their interaction with the vascular endothelium as rolling or adherent cells. 17 Rolling leukocytes were defined as cells moving with a velocity less than two-fifths of the centerline velocity, and are expressed as the number of cells per minute, passing a reference point within the microvessel. Adherent leukocytes were defined as cells that did not move or detach from the endothelial lining of postcapillary venules within a 20 s observation period, and are expressed as the number of cells per square millimeter of the venular endothelial surface. Endothelial surface was calculated from the diameter and length of the vessel segment studied, assuming cylindrical vessel geometry.
Diameters, centerline velocity, volumetric blood flow, and wall shear rate were determined in those venules in which leukocyte-endothelial cell interaction was analyzed. Diameters (d) were measured in μm perpendicularly to the vessel path. Centerline red blood cell velocity (v) was analyzed by the computer-assisted image analysis system using the line shift method. Volumetric blood flow was calculated by Q=π * (d/2) 2 * v/1.6 (pL/s), where 1.6 represents the Baker–Wayland factor that corrects for the parabolic velocity profile in microvessels with diameters >20 μm. 18 Moreover, wall shear rate (y) was calculated based on the Newtonian definition: y=8 * v/d.
Angiogenesis was analyzed at a magnification of ×460 in eight different microvascular ROIs in the border zone and eight different microvascular ROIs in the center of the polyethylene implants. As already described, identical ROIs were repetitively analyzed throughout the entire in vivo experiment. ROIs were defined as being positive for angiogenesis when signs of blood vessel development, that is, capillary sprouts or newly formed microvessels ingrowing into the implants, could be identified. In addition, functional capillary density, that is, the length of newly formed red blood cell-perfused capillaries per observation area, was measured by CapImage and is given in cm/cm2.
Experimental protocol
A total of 22 CD-1 nude mice was equipped with dorsal skinfold chambers. After 72 h, PRP-chondrocyte-coated (n=8; six samples: chondrocytes from separate patients, two samples: chondrocytes from one patient), PRP-coated (n=8), or uncoated polyethylene samples (control; n=6) were implanted into the chambers. Intravital fluorescent microscopic analyses were performed directly after implantation as well as at days 3, 6, 10, and 14. At the end of the in vivo experiments, the animals were sacrificed with an overdose of the anesthetics, and the dorsal skinfold preparations were excised for further histological, immunohistochemical and in situ hybridization (ISH) analyses.
In a subset of experiments, we studied the in vivo maturation of human chondrocytes by means of a subcutaneous implantation model. For this purpose, four CD-1 nude mice were anesthetized by i.p. injection of ketamine (75 mg/kg body weight; Pharmacia GmbH) and xylazine 2% (25 mg/kg body weight; Rompun, Bayer), and two PRP-chondrocyte-coated polyethylene samples per animal (from separate patients) were implanted into subcutaneous pockets of the right and left flank. After 6 weeks, the samples were excised for histological analyses.
Histology and immunohistochemistry
For light microscopy, formalin-fixed specimens were embedded in paraffin. Four-micrometer-thick sections were cut and stained with hematoxylin and eosin according to standard procedures. In the group of PRP-chondrocyte-coated polyethylene implants, the sections were additionally stained with toluidine blue to study the formation of extracellular cartilage matrix.
Immunohistochemical staining of macrophages and foreign body giant cells in the newly formed granulation tissue around the implants was performed by a rat polyclonal anti-F4/80 antibody as a primary antibody (1:50; Abcam, Cambridge, United Kingdom). This was followed by a peroxidase-conjugated goat anti-rat IgG antibody (1:200; Dianova GmbH, Hamburg, Germany). For the detection of different macrophage phenotypes, M1 polarized macrophages were stained with a rabbit polyclonal anti-CCR7 antibody 19 (1:1200; Abcam), and M2 polarized macrophages were stained with a rabbit polyclonal anti-arginase (anti-Arg)-1 antibody 20 (1:1000; Sigma Aldrich) as a primary antibody. This was followed by a peroxidase-conjugated goat anti-rabbit IgG antibody (1:200; Dianova GmbH). 3,3′ diaminobenzidine was used as chromogen. The sections were counterstained with Mayer's hemalaun (Merck, Darmstadt, Germany) and examined by light microscopy (BX60; Olympus, Hamburg, Germany).
For immunofluorescence staining of collagen II in cultivated human chondrocytes, cells were grown on glass cover slips and fixed in paraformaldehyde (4% in PBS). Subsequently, the cells were permeabilized, blocked with 0.3% NP40/PBS and 5% bovine serum albumin/PBS (Merck, Darmstadt, Germany) for 30 min at 37°C, and then incubated with the primary α-collagen II antibody (AB761; Millipore, Danvers, MA) 1:10 overnight at 4°C. After several washings with PBS and 0.3% NP40/PBS, the cells were incubated with the secondary FITC-conjugated goat anti-rabbit IgG antibody (Sigma Aldrich) 1:1000 for 60 min at 37°C. DNA was stained with 0.2 μg/mL 4′,6-diamidin-2′-phenylindoldihydrochlorid (Sigma Aldrich) in methanol to visualize individual nuclei. Collagen II expression was studied with a BX61 fluorescence microscope (Olympus) with a cooled charged-coupled device camera.
Cot—in situ hybridization
For the identification of human chondrocytes surrounding the implants at day 14 after implantation into the dorsal skinfold chamber, 4 μm-thick paraffin-embedded sections were deparaffinized in xylene followed by postfixation in paraformaldehyde (4% in PBS) and digested for 3 min with an in situ hybridization kit (Qbiogene, Heidelberg, Germany) according to the manufacturer's protocol. The sections were rinsed twice for 5 min in 2× saline-sodium citrate buffer (SSC) at room temperature and incubated in 2× SSC for 30 min at 70°C. Endogenous peroxidase was blocked for 10 min in 1.5% H2O2. After rinsing in aqua dest, the slides were dehydrated and air dried.
Human Cot DNA (Roche Diagnostics, Mannheim, Germany) was labeled with biotin by standard nick translation (Roche Diagnostics) according to the manufacturer's protocol. The hybridization mixture containing 50% formamide in 2× SCC and 50 ng biotin-labeled Cot DNA was denatured for 5 min at 80°C. Target DNA was denatured in 70% formamide/2× SSC at 80°C for 20 min. After applying the hybridization mixture, simultaneous denaturation was performed for 90 min at 80°C, followed by incubation overnight at 37°C. Stringency washing was done twice in 2× SSC and thrice in 57% formamide/2× SSC at 42°C for 10 min each. Detection of the biotin signals was carried out using StrepABComplex/horseradish peroxidase (Dako, Glostrup, Denmark), followed by diamino benzidine (DAB) staining for 5–10 min with 1 mg/mL DAB (Sigma Aldrich), 0.02% H2O2, and 25 μg/mL nickel chloride (Merck) in aqua dest. The nuclei were counterstained with Mayer's hemalaun (Merck).
Statistics
After testing the data for normal distribution and equal variance, differences between the three study groups were analyzed by analysis of variance (ANOVA) followed by the appropriate post hoc comparison. To test for time effects in the individual groups, ANOVA for repeated measures was applied. This was followed by the paired Student's t-test, including correction of the α-error according to Bonferroni probabilities for repeated measurements (SigmaStat; Jandel Corporation, San Rafael, CA). All values are expressed as means±standard error of the mean. Statistical significance was accepted for a value of p<0.05.
Results
Cell distribution and viability of PRP-chondrocyte-coated polyethylene implants
Directly after implantation into the dorsal skinfold chamber, fluorescence microscopy of bisbenzimide-stained PRP-chondrocyte-coated polyethylene implants showed a homogeneous distribution of chondrocyte nuclei on the implant surface (Fig. 1F). Moreover, individual cell nuclei lacked chromatin condensation and fragmentation, indicating the absence of apoptotic cell death in the course of the coating procedure (Fig. 1F, inset).
Vascularization of polyethylene implants
In all three groups, the polyethylene implants induced angiogenesis in the dorsal skinfold chamber. At day 3 after implantation, first capillary buds and sprouts, which originated from capillaries and postcapillary venules of the host tissue, could be detected in the border zones of the implants. During the further time course of the experiment, these sprouts grew continuously inside the pores of the biomaterial and finally interconnected with each other to form new blood-perfused microvascular networks at the implantation site (Figs. 2 and 3). In the groups of PRP-coated and uncoated porous polyethylene, these networks exhibited a comparable functional capillary density of ∼40 cm/cm2 in the border zones and ∼20–35 cm/cm2 in the center zones of the implants at day 14 (Fig. 2C, D).

Analysis of angiogenesis-positive regions of interest (ROIs) (%)
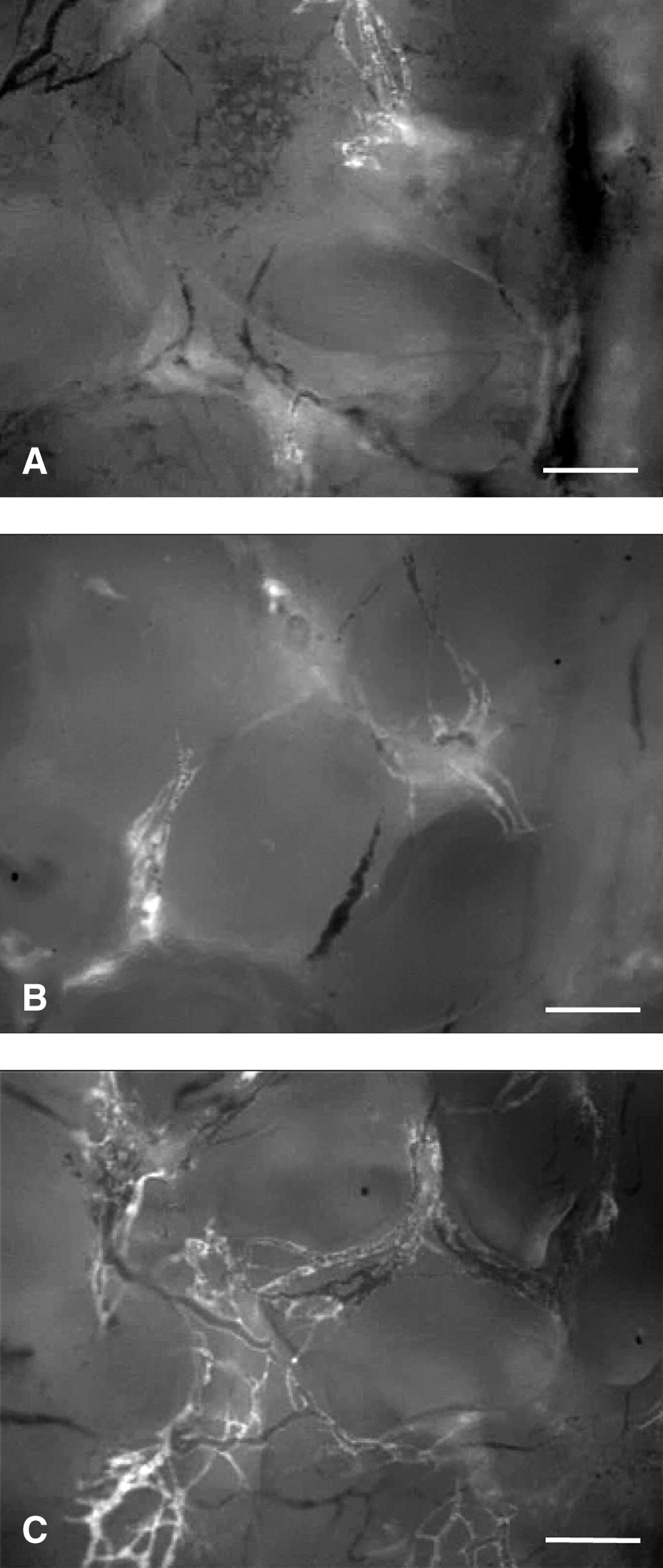
Intravital fluorescence microscopy of ROIs within the center of an uncoated
Of interest, the vascularization of PRP-chondrocyte-coated polyethylene implants was markedly accelerated and improved when compared with the other two groups. This was indicated by an increased number of angiogenesis-positive ROIs in the border and center zones of the implants from day 6 until the end of the observation period (Fig. 2A, B). Accordingly, the PRP-chondrocyte-coated polyethylene was finally surrounded by new microvascular networks, which exhibited a functional capillary density of ∼130 and 90 cm/cm2 in the border and center zones at day 14 (Fig. 2C, D).
Microhemodynamics and inflammatory response to polyethylene implants
To study in vivo the early leukocytic inflammatory response of the host tissue to uncoated, PRP-coated and PRP-chondrocyte-coated porous polyethylene, leukocyte-endothelial cell interaction was analyzed in postcapillary and collecting venules at the implantation site. For this purpose, microhemodynamic parameters of these vessels were assessed in a first step, because the interaction of leukocytes with the microvascular endothelium may be affected by changes in wall shear rates over time independently from inflammatory stimuli induced by the implantation of the biomaterial. 21 The diameter and centerline velocity of the analyzed microvessels ranged between 31–37 μm and 215–411 μm/s throughout the observation period of 14 days without marked differences between the three implant groups (Table 1). Accordingly, calculated values of volumetric blood flow and wall shear rate of all three groups were comparable (Table 1), indicating standardized microcirculatory conditions for the analysis of leukocyte-endothelial cell interaction.
Means±SEM.
p<0.05 versus d0 and d6 within each individual group.
p<0.05 versus control at corresponding time points.
p<0.05 versus d0 within each individual group.
p<0.05 versus d10 within each individual group.
PRP, platelet-rich plasma; SEM, standard error of the mean.
Importantly, postcapillary and collecting venules in direct vicinity to uncoated, PRP-coated, and PRP-chondrocyte-coated polyethylene implants presented with comparable numbers of rolling and adherent leukocytes ranging between 18–31 min−1 and 117–223 mm2 throughout the observation period (Table 2). This finding indicates that the coating of the biomaterial with PRP or a combination of PRP and chondrocytes does not promote an increased leukocyte-endothelial cell interaction at the implantation site.
Means±SEM.
Incorporation of polyethylene implants
Histological examinations of the polyethylene samples at day 14 after implantation into the dorsal skinfold chamber revealed that the implants of all three groups were surrounded by a vascularized granulation tissue (Fig. 4A–C). However, in the group of PRP-chondrocyte-coated polyethylene implants, this granulation tissue was thicker and characterized by an increased cell density when compared with the other two groups (Fig. 4A–C), indicating an improved biomaterial incorporation into the surrounding host tissue.
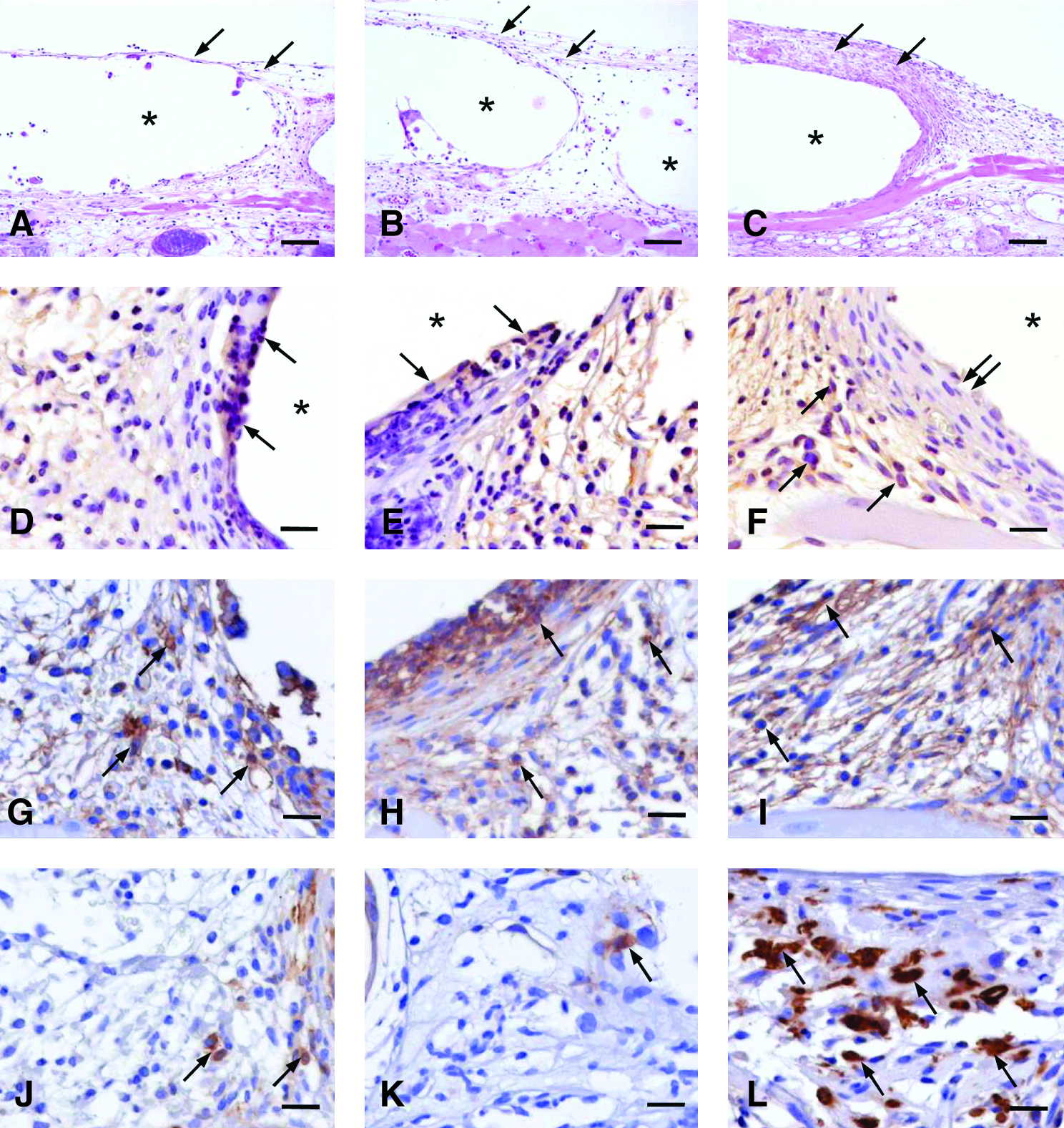
The additional immunohistochemical detection of F4/80 showed that PRP-chondrocyte-coated polyethylene implants were covered with a tissue layer, which was completely free of F4/80-positive macrophages and multinucleated foreign body giant cells, whereas these cell types could be detected directly adjacent to the surface of PRP-coated and uncoated control implants (Fig. 4D–F). More detailed analyses of the polarization of macrophages revealed that the newly formed granulation tissue surrounding the implants contained CCR7-positive M1 polarized macrophages in all three groups (Fig. 4G–I). In contrast, high numbers of Arg-1-positive M2 polarized macrophages could only be detected in the granulation tissue of PRP-chondrocyte-coated polyethylene implants (Fig. 4J–L).
By means of Cot-ISH, it could be shown that the tissue layer covering the PRP-chondrocyte-coated polyethylene implants consisted of human chondrocytes, which had survived and had formed a bioprotective layer on the surface of the implanted polyethylene throughout the observation period of 14 days (Fig. 5A, B). In contrast to macrophages, newly formed microvessels of mouse origin were able to grow inside this layer (Fig. 5B). Toluidin blue staining demonstrated the lack of extracellular cartilage matrix formation around the implants at this early time point (Fig. 5C). However, PRP-chondrocyte-coated polyethylene samples, which had been subcutaneously implanted for 6 weeks into the flank of additional CD-1 nude mice, were surrounded by a toluidine blue-positive cartilage tissue (Fig. 5D).

Discussion
In the present study, we analyzed in dorsal skinfold chambers of CD-1 nude mice the vascularization of porous polyethylene implants, which were vitalized with human chondrocytes. Former studies could already demonstrate that it is possible to reliably produce such bioimplants and that they maintain their shape over long-term observation periods of up to 20 weeks.6,7 Herein, we now add the important finding that PRP-chondrocyte-coated polyethylene implants exhibit a markedly accelerated and improved vascularization within the initial 14 days after implantation when compared with uncoated control implants. This rapid vascularization is of major importance for the successful incorporation of the implants, because it may reduce the overall time window during which the implants are susceptible for extrusion, migration, and infection.5,8
For our in vivo analyses, we used small porous polyethylene samples with a size of 3×3×0.25 mm. This was necessary, because the implantation into the dorsal skinfold chamber implants should not be thicker than 1 mm to guarantee the closure of the chamber free from air. 22 Moreover, the implants should not substantially exceed a size of ∼3×3 mm to enable analyses of the host tissue surrounding the implants. Thus, the porous polyethylene could not be tested in a size, which may be more relevant under clinical conditions. This, however, does not necessarily represent a disadvantage for the analysis of the angiogenic and inflammatory host tissue response to the implants. In fact, since all studies in the dorsal skinfold chamber are performed using such small sample sizes, this allows for the comparison of the polyethylene samples with other biomaterial implants analyzed under the identical experimental settings.
The use of chondrocytes for the generation of an autologous protective tissue layer on porous polyethylene may have several advantages when compared with other cell types. Cartilage grafts have been routinely used for a long time in plastic surgery for auricular reconstruction or rhinoplasty, because they offer excellent elastic properties and are well incorporated into craniofacial defects. Therefore, there exists already a large experience in tissue engineering of cartilage, including the isolation, in vitro expansion, and seeding of chondrocytes onto various biomaterials.23,24 Moreover, cartilage is a relatively simple tissue that has a low metabolic demand and can survive by diffusion alone to a certain extent without the need for its own vascular supply. Accordingly, chondrocytes seeded on alloplastic materials may be able to survive during the early implantation phase, when the implants are not yet fully surrounded by a vascularized granulation tissue. In line with this view, we could demonstrate by means of Cot-ISH that even 14 days after implantation into the dorsal skinfold chambers of mice, the vitalized polyethylene implants were still covered with an intact cell layer of human origin. However, at this time point, the cell layer did not yet secrete any extracellular cartilage matrix. In contrast, PRP-chondrocyte-coated polyethylene samples, which had been subcutaneously implanted for 6 weeks into the flank of additional animals, were surrounded by a toluidine blue-positive cartilage tissue, indicating that the chondrocytes were able to maturate during this longer observation period of several weeks.
The seeding of chondrocytes on polyethylene implants bears some challenging difficulties, because the nonbiological material is hydrophobic and, therefore, provides suboptimal adhesion properties for the cells. In former studies, this problem was overcome by suspending isolated chondrocytes in hydrogel 7 or alginate, 6 which were then applied as solid gels around the surfaces of the implants. In the present study, we suspended the cells in PRP for several reasons. PRP is defined as a portion of the blood plasma fraction having a platelet concentration above baseline. 9 Accordingly, PRP is an autologous product that can be easily produced under clinical conditions from a blood sample of the patient, and, thus, offers an optimal biocompatibility. Moreover, the highly viscous mixture of PRP and chondrocytes easily penetrates into the pores of the polyethylene and, on activation with thrombin, forms a solid gel that attaches well to the surface of the alloplastic material. Finally, PRP contains a mixture of different pro-angiogenic growth factors that are released from the activated platelets, such as vascular endothelial growth factor (VEGF) and platelet-derived growth factor.25–27 The combination of these factors may be much more effective to stimulate blood vessel development than a single growth factor alone. Unexpectedly, however, we found that the PRP-coated polyethylene implants only induced an angiogenic host tissue response, which was comparable to that of uncoated control implants. These results are in line with the findings of previous studies, reporting that the incorporation of even high amounts of VEGF or basic fibroblast growth factor into porous polyethylene does not result in an improved vascularization when compared with growth factor-free control implants.11,28 Thus, we conclude that the vitalization of polyethylene with cells is a much more effective strategy that promotes the ingrowth of new blood vessels into the implanted biomaterial than the bioactivation with pro-angiogenic growth factors contained in PRP.
Since platelets have been shown to act as pro-inflammatory cells,29,30 we additionally analyzed, in the present study, whether the coating with PRP- or PRP in combination with chondrocytes might affect the biocompatibility of polyethylene implants. For this purpose, we studied the leukocyte-endothelial cell interaction in postcapillary and collecting venules of the host tissue, which were located in direct vicinity to the implants and exhibited comparable microhemodynamic conditions. By this, we found that in all three experimental groups, the number of rolling and adherent leukocytes ranged between 18–31 min−1 and 117–223 mm2 throughout the observation period of 14 days. These results confirm the data of a previous study (rolling leukocytes: 21–31 min−1; adherent leukocytes: 144–245 mm2), which was performed under identical experimental conditions, but in balb/c mice. 10 This indicates that the response of the innate immune system to the polyethylene implants in nude mice is similar to that in immunocompetent animals. Furthermore, incompatible biomaterials usually promote a much stronger leukocytic activation. For instance, in the work of Rücker et al., 31 the implantation of hydrogel scaffolds into dorsal skinfold chambers of balb/c mice induced severe inflammation with massively increased numbers of rolling (∼40 min−1) and adherent leukocytes (∼700 mm2). Thus, our data demonstrate that polyethylene implants exhibit an excellent in vivo biocompatibility without inducing a strong leukocytic inflammatory host tissue response during the initial phase after implantation. Moreover, the biocompatibility of the implants is not affected by PRP- or PRP-chondrocyte coating. In fact, vitalization with human chondrocytes results in the formation of a bioprotective tissue layer on the polyethylene surface, which prevents the accumulation of macrophages and foreign body giant cells on the implants' surface. In addition, this implant modification promotes the recruitment of M2 polarized macrophages, which may contribute to the improved incorporation of PRP-chondrocyte-coated polyethylene implants into the surrounding granulation tissue, because this macrophage phenotype has been shown to scavenge debris and to promote tissue repair.19,32 Thus, the coating with PRP and chondrocytes may even have a positive effect on the chronic foreign body reaction to the implanted polyethylene.
Taken together, the present in vivo study demonstrates that vitalization of porous polyethylene with chondrocytes promotes early implant vascularization and incorporation into the host tissue without affecting the good biocompatibility of the alloplastic material. Accordingly, this promising approach may help during future reconstructive interventions that prevent postoperative complications such as implant extrusion, migration, and infection.
Footnotes
Acknowledgments
The authors are grateful for the excellent technical assistance rendered by Janine Becker (Institute for Clinical and Experimental Surgery, University of Saarland), Monika Hoffmann, and Ulrike Bechtel (Department of Otolaryngology, Head and Neck Surgery, University of Saarland).
This work was supported by the research program of the Medical Faculty of the University of Saarland (HOMFOR 2008).
Disclosure Statement
No competing financial interests exist.