
Abstract
Aim:
Fibrin glue has been used for tissue adhesives and wound sealing. This study aimed to establish an approach to treat rabbit urethral injuries using fibrin glue and mesenchymal stem cells (MSCs).
Methods:
Rabbit urethral injury was performed by excising the subcutaneous tissue from the ventral aspect of the penile urethra. Thirty-six New Zealand rabbits were divided into four groups: injured without treatment (control), glue treatment (glue), glue and MSCs treatment (glue + MSCs), and without injury (normal). Animals were sacrificed and the penises were excised for analysis after treatment for 10 days (n=4) and 30 days (n=5).
Results:
The fibrin glue had a porous structure with cellular compatibility to MSCs. Two rabbits developed urethral fistulae in the control group, but none did in either the glue or the glue + MSCs groups at day 10 and 30. Hematoxylin and eosin staining showed that the distance between the skin and the epithelial layer at the ventral aspect of the penis increased in the glue and glue + MSCs groups compared to the control group at day 10 and 30. The density of blood vessels in the injured area increased in the glue and glue + MSCs groups compared to the control at day 10 and 30. The average thickness of the epithelial layer in the glue + MSCs group showed the same increasing trend among the three groups at day 10 and 30. The thickness and the area of the smooth muscle that surrounds the urethral mucosa at the operative region increased compared to the thickness in the control and glue groups at day 10 and 30. Pancytokeratins (AE1/AE3) staining showed weak signals in the urethral fistulae in the control group compared with the glue and glue + MSCs groups. The transplanted MSCs have differentiated into endothelial and smooth muscle cells, contributing to the formation of blood vessels and the recovery of urethral smooth muscle.
Conclusions:
MSCs combined with fibrin glue showed improved neovascularization and smooth muscle formation in repairing urethral injury, resulting in effective prevention of the development of urethral fistulae. Our data indicate that fibrin glue combined with MSCs may be a feasible approach for repairing urethral injury.
Introduction
With improved viral safety and optimized preparation process, fibrin glue has been used as a hemostatic, adhesive, and sealing agent in Europe and the United States. 1 Some reports have shown that application of fibrin glue to the repair of hypospadias can greatly decrease the incidence of fistula formation. 1 In addition, using fibrin glue as a transport and support matrix seeded with urothelial cells (UCs) successfully created an artificial urethra. 2 Fibrin glue was used in cardiovascular surgery as a hemostatic agent against diffuse bleeding from friable tissue and along suture lines. In a sciatic nerve repair model, fibrin glue can circumvent the typical learning curve in microneurosurgical operations. 3
Fibrinogen is a soluble blood component. Concentrated fibrinogen can be obtained by cryoprecipitation or by chemical precipitation of plasma. 4 The fibrinogen molecule contains three pairs of polypeptide chains joined by disulphide bonds to form a symmetric trimeric structure. Thrombin can activate fibrinogen by cleaving fibrinopeptide A and B off its central domain. 5 The resulting fibrin monomers assemble to form two-stranded fibrils by noncovalent interactions. These two-stranded fibrils can form a stable clot by covalent cross-linking in the presence of activated Factor XIII. Optimal cross-linking is achieved at a concentration between 5 and 20 mM CaCl2 with an ionic strength of 0.15 M. 6 Aprotinin, epsilonaminocaproic acid, or trans-4-(aminomethyl) cyclohexanecarboxylic acid is usually added to inhibit degradation of the fibrin clot because they inhibit activation of plasminogen. 6
Recently, more and more attention has been focused on bone marrow-derived mesenchymal stem cells (MSCs) in tissue engineering. MSCs can be obtained by simple bone marrow isolation and easily expanded in cell culture. These cells can elude host immune responses and differentiate into many cell types, including pneumocysts, 7 hepatocytes, 8 neural cells, 9 bone, 10 cartilage, 11 and skin. 12 Another role of MSCs is to stimulate angiogenesis. The rapid and transient growth of new capillaries, a process called angiogenesis, is central to most human life processes, including tissue development, regeneration, and repair. 13 Many factors play a positive role in angiogenesis, such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), transforming growth factor, tumor necrosis factor α, angiopoietins, angiogenin, and interleukin-8.14,15 Among these factors, VEGF is a critical growth factor for revascularization of ischemic tissues and has been proven to promote the growth of vascular endothelial cells derived from arteries, veins, and lymphatics. 16 The potential of human MSCs as a source of VEGF-producing cells in vitro and in vivo has been reported. 17
It has also been shown that a fibrin glue spray system delivering autologous MSCs to cutaneous wounds was safe and could accelerate the healing process. 18 In our previous study, acellular artery matrix seeded with VEGF-modified rabbit bladder UCs was subcutaneously implanted into rabbits. The VEGF-modified UCs enhanced the neovascularization and urethral layer formation compared to the control green fluorescent protein-expressing UCs. 19 At present, clinical urethral injury repair and urethral reconstruction by tissue engineering is generally focused on how to create or retain a complete and functional epithelial layer, while the issue of protection and recovery of the urethral smooth muscle layer has been overlooked.
To address this issue, rabbit urethral injury was performed by excising the subcutaneous tissue without damaging the urothelial layer. The effect of fibrin glue combined with autologous MSCs on regeneration of urethral smooth muscle was investigated.
Materials and Methods
Cell culture, identification, and labeling
Bone marrow cells were flushed out from the tibia of New Zealand white rabbits (male, weight 2–2.5 kg; purchased from the Animal Facility, Tianjin Medical University), which were anesthetized with urethane (1.5 g/kg intravenous). MSCs were then isolated by density-gradient separation using Lymphoprep reagent (Hao Yang Biological Co., Ltd.). The isolated cells were resuspended in Minimum Essential Medium alpha (Invitrogen, Grand Island, NY) containing 20% fetal bovine serum, 100 U/mL penicillin, and 100 μg/mL streptomycin, and cultured in a humidified incubator at 37°C with 5% CO2. MSCs from passage three were collected and labeled with DiI (Molecular Probes) before implantation. For cell characterization, MSCs from the third passage were cultured on cover slips and fixed with −20°C methanol for 10 min. The cells were then blocked with 4% bovine serum albumin in phosphate buffered saline (PBS) for 30 min and incubated with 1:100 dilution of mouse anti-human CD29 (BD Bioscience), 20 mouse anti-rabbit CD44 (BD Bioscience), 21 and CD45 (Santa Cruz) 20 for 2 h at room temperature. The slips were further incubated with 1:400 dilution of biotinylated goat anti-mouse immunoglobulin G (IgG) (BD Bioscience). Signals were visualized with alkaline phosphatase conjugate (Vector Laboratories) and Fast Red (Sigma). The negative control omitted the primary antibody.
Preparation of fibrin glue
Commercially available fibrin glue, Chuangxuefeng® (Song Li Bio-Technology Co., Ltd.), was supplied in 2-mL kits. It was prepared right before the experiment according to the manufacturer's instructions. Briefly, in one vial, the pig fibrinogen concentrate was mixed with the Factor XIII-containing diluent. In another vial, the pig thrombin concentrate was mixed with CaCl2. The fibrinogen/Factor XIII and the thrombin/CaCl2 solutions were drawn up in separate syringes connected by a Y piece, so that they were mixed just before delivery. In the MSCs treatment group, the cells were suspended into the fibrinogen/Factor XIII solution.
Cellular compatibility
MSCs were suspended in the fibrinogen/Factor XIII solution at 2.5×105 cell/mL. For tests using 96-well plates, 20 μL of MSC solution was added to each well and then mixed with an equal volume of the thrombin/CaCl2 solution to form stable fibrin polymers with encapsulated MSCs. For two-dimensional culture, the fibrin glue was first prepared in a cell culture plate and MSCs were seeded on the surface of the glue. A culture of MSCs at the same density in a plate without fibrin glue was used as control.
An MTT [3-(4,5)-dimethylthiahiazo (-z-y1)-3,5-diphenytetrazoliumromide] assay was used to evaluate the influence of fibrin glue on cell viability. Twenty microliters of MTT (5 mg/mL in PBS) was added to each well and incubated for 4 h. The supernatant was then discarded and cells were washed with PBS. One hundred microliters of dimethyl sulfoxide was added and the plate was put on a shaker for 20 min to dissolve the formazan salts. Finally, 50 μL of dissolved solution from each well was transferred to a new 96-well plate. The absorbance at 492 nm was measured with a Bio-Rad Microplate Reader (iMark; Bio-Rad).
For scanning electron microscopy (SEM) analysis, the samples were fixed in 2% (vol/vol) glutaraldehyde for 12 h, dehydrated with liquid nitrogen, and frozen dry. They were then mounted on an aluminum stub, coated with gold, and examined with an X-650 SEM (Hitachi).
Animal experiments
Thirty-six New Zealand white rabbits (male, weight 2–2.5 kg) were included in this study. All animal experiments were approved by the Animal Care and Use Committee of Nankai University.
The animals were anesthetized with urethane (1.5 g/kg) and the lower abdominal skin was shaved and sterilized. A French-6 catheter was inserted into the bladder and fixed to the abdominal wall. A 1-cm longitudinal incision was made on the ventral aspect of the urethra using a No. 10 knife cutting down through the skin. The subcutaneous tissue was excised with the skin keeping the urothelial layer intact. The rabbits were divided into four groups (n=4). In the control group, the wounds were not filled with glue or cells. In the glue treatment group, the wounds were filled with 60 μL of fibrin glue. In the glue + MSCs treatment group, the wounds were filled with 60 μL fibrin glue mixed with autologous MSCs (6×105). The glue was wrapped and closed by suturing the skin with 8-0 nylon sutures. The edges of the surgical area were marked with permanent sutures for future reference. Elizabeth masks were used to prevent the animals from biting the wounds. The animals in the normal group received no injury or treatment.
All of the animals stayed nothing per oral for 6 h postsurgery, and then feeding was resumed. The living environment was adjusted to 60% humidity and 25°C. Daily antibiotic treatment with gentamycin sulfate at 40,000 U/kg was started at the time of surgery and continued for 5 days. The animals were monitored for infection development and fistula formation, and were euthanized after 10 or 30 days.
Histological analysis
The entire penis was excised, fixed with 4% paraformaldehyde, and embedded in paraffin. The tissues from the center of the injured area were cut into 5 μm in thickness and stained with hematoxylin and eosin (H&E). At the ventral aspect of the penis samples, the distance between the skin and the closest epithelial layer was measured with a stereo microscope at five randomly selected sections. Similarly, epithelial thickness and blood vessel density were measured at nine randomly selected fields from three sections of each sample with CD31 staining and the mean values were calculated. The ratio of cells and collagen within wound sites was analyzed with Masson Trichrome staining and stereo microscopy at five randomly selected sites.
For immunofluorescence staining, the paraffin sections underwent an antigen recovery process. Basically, the sections were put into sodium citrate solution and heated in a 600-W microwave for 5 min, and then left to cool to room temperature. In total, four rounds of heating and cooling steps were conducted for optimal antigen retrieval. Monoclonal antibodies to pancytokeratin clone AE1/AE3 (1:100; BD Bioscience) and mouse anti-smooth muscle myosin heavy chain I (MYH, 1:1000; Abcam) and mouse anti-rabbit CD31 (1:100; Abcam) were used as primary antibodies, and fluorescein isothiocynate (FITC)-conjugated anti-mouse IgG was used as the secondary antibody (Molecular Probes). The slides were mounted and viewed with a fluorescence microscope (Eclipse TE2000-U; Nikon).
Cell-tracking analysis
To track the implanted cells, MSCs were labeled with DiI before transplantation. The sections were stained with mouse anti-rabbit CD31 as the primary antibody, and an FITC-conjugated second antibody. The sections were viewed under a fluorescence microscope (IX71; Olympus) and images were recorded on a monitor (Flex Scan L557; Eizo Nanao).
Statistical analysis
All data were compared with one-way analysis of variance tests using SPSS software. A p-value less than 0.05 was considered to be statistically significant.
Results
Cell culture and identification
MSCs can be easily isolated and expanded a quantity sufficient for analysis and treatment. MSCs from the third passage showed typical fusiform shape. These cells were positive for CD29 and CD44 antibodies and negative for CD45 antibodies (Fig. 1A–C). Flow cytometry data showed that the DiI labeling efficiency was 99.67% (Fig. 1D–F).

Cell identification and labeling. Immunochemical characterization of MSCs was performed with antibodies to CD29
Cellular compatibility of the fibrin glue
SEM images showed that the fibrin glue had a porous structure with pores connected to each other (Fig. 2A). This structure was similar to natural extracellular matrix, so it provided a suitable environment for MSCs to grow well on the surface (Fig. 2B) or within the network of the fibrin glue (Fig. 2C). On day 3, the number of cells cultured on the glue surface or within the glue was comparable to that of cell culture plate (Fig. 2D).
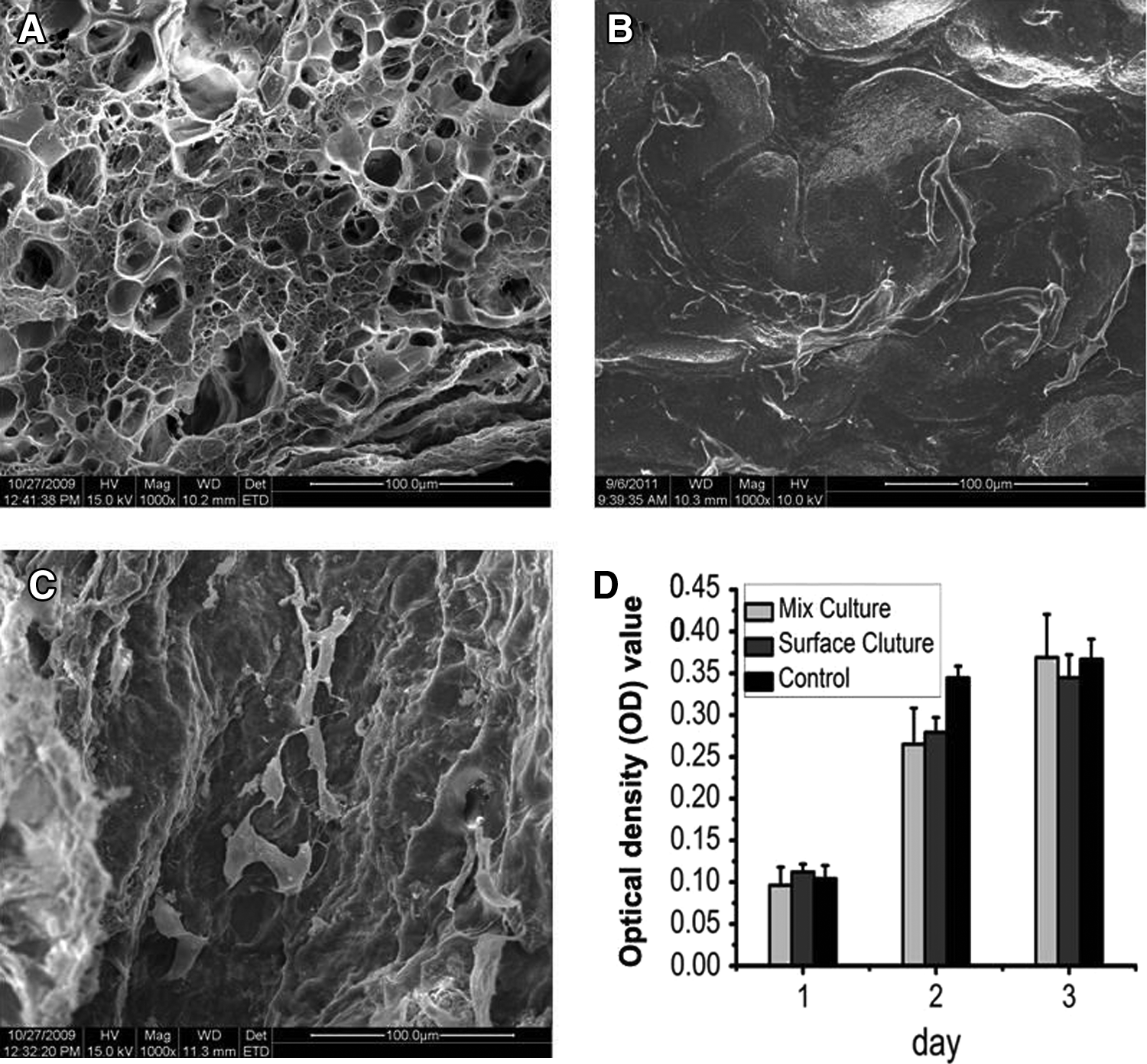
Cellular compatibility of the fibrin glue.
Histological analysis
The results of H&E staining showed that two rabbits in the control group developed urethral fistulae at both 10 and 30 days (Table 1). One and two rabbits developed urethral distortion at 10 and 30 days, respectively. The deformed urethra was in the vertical position under the penile corpus cavernosum in contrast to the normal horizontal position. In the glue group, two rabbits developed urethral distortion at both 10 and 30 days. However, urethral fistulae and distortion were not observed in the glue + MSCs group at 10 and 30 days.
MSCs, mesenchymal stem cells.
To evaluate the urethra deformation, the distance between the ventral skin of the penis and the closest epithelial layer was measured according to the H&E staining images recorded at the same magnification (Fig. 3A–G). The average distances obtained from five randomly selected sections that were cut from the center of injured area were 0.47±0.22 mm at 10 days and 0.52±0.36 mm at 30 days in control group, 1.61±0.32 mm at 10 days and 0.96±0.37 mm at 30 days in the glue group, and 1.99±0.27 mm at 10 days and 1.45±0.39 mm at 30 days in the glue + MSCs group. For the normal rabbit penis, the average distance was 1.30±0.17 mm (Fig. 3H, I). The differences between control and glue (p<0.01), control and glue + MSCs (p<0.001) was significant at 10 and 30 days.
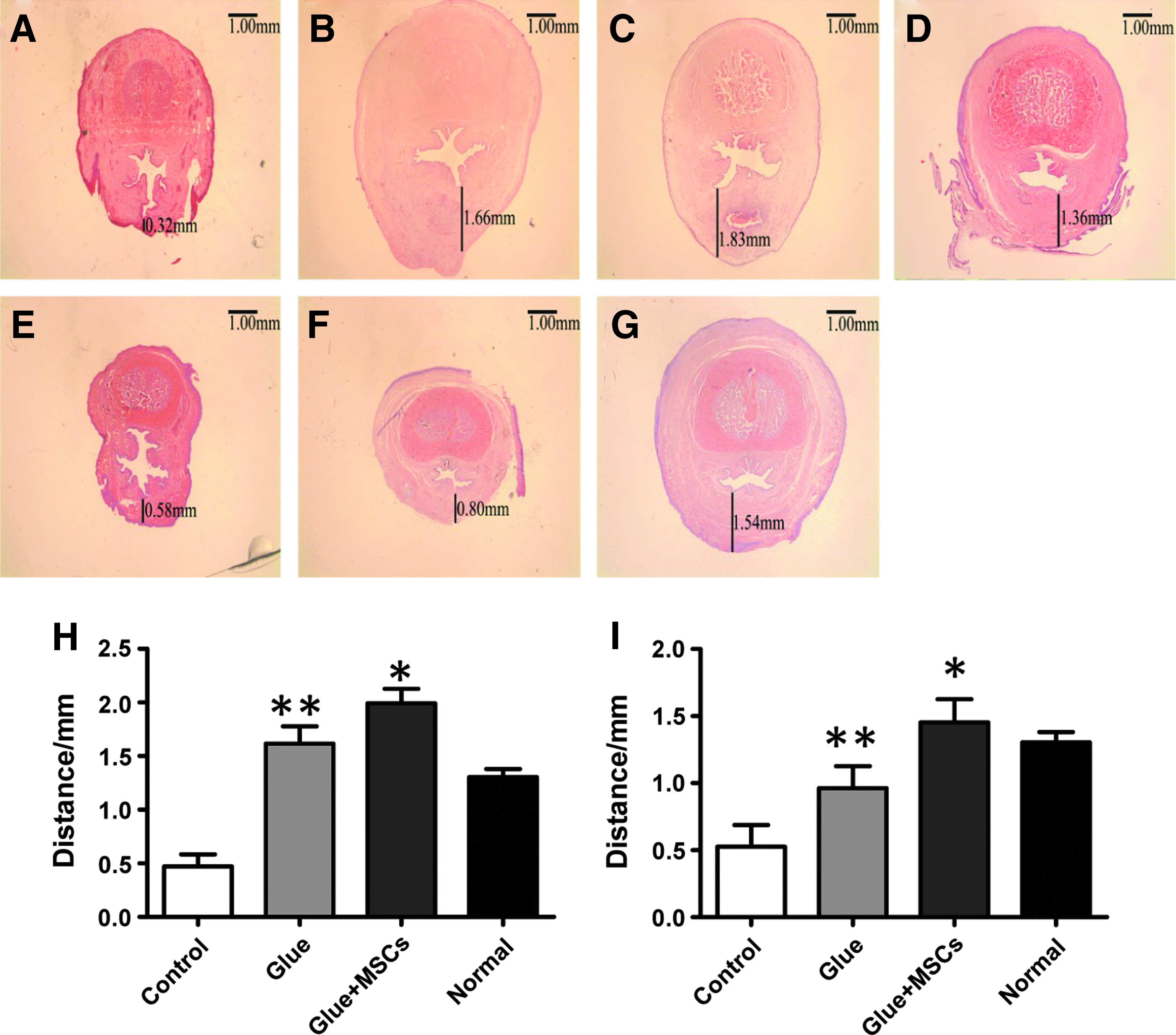
Hematoxylin and eosin staining of urethra at day 10 and 30. The distance between the skin of the ventral aspect of the penis to the closest epithelial layer was measured with a stereo microscope in different groups. All images 1.5×.
Epithelial thickness was measured in the four groups according to the H&E staining images (Fig. 4A–G). The epithelial thickness appeared to be similar among all the four groups, which were 28.34±3.03 μm at 10 days and 28.3±3.34 μm at 30 days in the control group, 29.77±2.33 μm at 10 days and 29.36±6.89 μm at 30 days in the glue group, 28.70±3.86 μm at 10 days and 28.37±6.32 μm at 30 days in the glue + MSCs group, and 28.27±4.46 μm in the normal group, respectively (Fig. 4H, I). The differences were not significant among the four groups (p>0.05).

Thickness of the epithelial layer at day 10 and 30.
Immunofluorescence analysis
The density of the blood vessels in the surgical area was also quantitatively analyzed according to the images stained with mouse anti-rabbit CD31 (Fig. 5A–H). The mean number of vessels per field was 4.14±0.72 at 10 days and 4.07±1.18 at 30 days in control group, 6.80±0.54 at 10 days and 8.13±1.54 at 30 days in glue group, 10.25±0.41 at 10 days and 12.35±1.32 at 30 days in glue + MSCs group, and 7.62±0.87 in normal group, respectively (Fig. 5I, J). Treatment with glue alone or combined with MSCs significantly increased the vessel density compared to the control. The differences between control and glue (p<0.01), control and glue + MSCs (p<0.001), or glue and glue + MSCs (p<0.001) was significant at 10 and 30 days, suggesting the additional benefit of stem cell transplantation.

The density of microvessels in the surgical area at day 10 and 30.
Immunofluorescence analysis using mouse anti-smooth muscle MYH I is shown in Figure 6. In the control group (Fig. 6A, E), a few disorganized smooth muscle cells (SMCs) were observed in the submucosal layer with few blood vessels formed in the graft. In the glue group, more SMCs were observed in the injured area and they were well organized. However, these SMCs were located far from the epithelial layer, leaving an empty area underneath the epithelial layer (Fig. 6B, F). In the glue + MSCs group, the smooth muscle and blood vessels were significantly increased compared with the control and glue groups. More importantly, the SMCs formed directly underneath the epithelial layer and were well organized into the physiological architecture (Fig. 6C, G) similar to normal urethra (Fig. 6D). Accordingly, the average thickness of the muscular layers were 135.63±20.77 μm at 10 days and 148.43±118.62 μm at 30 days in the control group, 186.92±12.90 μm at 10 days and 211.22±26.52 μm at 30 days in the glue group, 223.73±24.83 μm at 10 days and 255.13±21.33 μm at 30 days in the glue + MSCs group, and 272.98±57.79 μm in the normal group, respectively (Fig. 6I, J). The difference between the control and the glue + MSCs groups was significant (p<0.05) at 10 and 30 days.

Characterization of smooth muscle cells at day 10 and 30. The thickness of the muscular layer was measured by immunofluorescence staining with anti-smooth muscle myosin heavy chain I.
Area of smooth muscle bundles
The regeneration of smooth muscle was also quantitatively characterized by area. In the control group, a few smooth muscle bundles sparsely appeared in the injured area (Fig. 7A, E). In the glue group the smooth muscle bundles were more abundant (Fig. 7B, F), but much less than that in the glue + MSCs group (Fig. 7C, G), which was close to the normal urethra (Fig. 7D). The measured SMCs areas were 2.20±0.06×104 μm2 at 10 days and 2.33±1.03×104 μm2 at 30 days in the control group, 2.81±0.28×104 μm2 at 10 days and 3.19±0.82×104 μm2 at 30 days in the glue group, 3.35±0.21×104 μm2 at 10 days and 4.29±0.42×104 μm2 at 30 days in the glue + MSCs group, and 4.77±0.47×104 μm2 in the normal group, respectively (Fig. 7H, I). The difference between control and glue + MSCs (p<0.05), or glue and glue + MSCs (p<0.05) was significant, suggesting the additional benefit of MSCs transplantation.

The area of smooth muscle bundles at day 10 and 30. The area of smooth muscle bundles was measured by immunofluorescence staining with anti-smooth muscle myosin heavy chain I.
Immunofluorescence staining of epithelial cells
Immunofluorescence staining for pancytokeratin (AE1/AE3) showed that the fluorescent density of epithelial cells in the control group was weak, which indicates the unhealthy condition of the epithelium due to lack of protection from the smooth muscle layer (Fig. 8A, E). Increased cytokeratin expression level was observed in the glue group (Fig. 8B, F), but it was still not as high as the glue + MSCs group (Fig. 8C, G), which was almost the same as normal epithelium (Fig. 8D).

Immunofluorescence staining of epithelial cells with pancytokeratin clone AE1/AE3 antibody at day 10 and 30.
Cell-tracking analysis
It is well known that MSCs have high differentiation potential and can secrete a variety of growth factors. To investigate the effect of MSCs, cells were labeled with the fluorescent dye DiI before transplantation. DiI-labeled cells were clearly observed in the surgical region (Fig. 9B) and 30 (Fig. 9E) days after treatment, indicating their survival and engraftment. Immunochemical staining with mouse anti-rabbit CD31 antibody and anti-smooth muscle myosin heavy chain I antibody revealed that some DiI-positive cells differentiated into endothelial cells and SMCs, and surrounded the newly formed microvessels in the glue + MSCs group.

Cell-tracking assay at day 10 and 30. MSCs were labeled with DiI before transplantation.
Discussion
With the rapid advance of surgery and tissue engineering, the materials and methods for injury repair have improved dramatically. Fibrin glue has been used extensively in all kinds of surgery and research, including urethral reconstruction 22 and tissue-engineered urethra. 2 In this study, fibrin glue combined with autologous MSCs was used to repair rabbit urethral injury. Our results show that the fibrin glue was cellular compatible. The fibrin glue had triaxial and porous structure, which was as conducive as the native environment in facilitating cell growth and adhesion. 23 The treatment enhanced angiogenesis (Fig. 5) and smooth muscle regeneration (Figs. 6, 7), which consequently maintained the function of the urethral epithelium (Fig. 8) and prevented the formation of urethral fistulae and urethral distortion (Table 1).
Angiogenesis, defined as the sprouting of new vasculature from a preexisting vascular network, is a process crucial to the growth and maintenance of tissues. 24 Ghajar et al. reported that MSCs stimulated capillary morphogenesis via special proteolytic mechanisms in fibrin matrix. 25 Recent studies have shown that MSCs can release numerous protein mediators, including VEGF, basic FGF, placental growth factor, and monocyte chemoattractant protein-1. 26 MSC-conditioned media enhanced proliferation of endothelial cells and SMCs in a dose-dependent manner. Anti-VEGF and anti-FGF antibodies partly attenuated these effects. 26 In our study, the transplanted MSCs engrafted into the injury site and differentiated into SMCs that contributed to the formation of blood vessels and recovery of urethral muscle. It is possible that the transplanted MSCs involved angiogenesis either by direct differentiation into the vascular endothelial cells 27 or by secretion of cytokines that stimulated angiogenesis.
The transitional uroepithelial cells of the urethra are important for successful ureter tissue engineering. They help to maintain the luminal space and prevent calculus formation.28–31 In this study, the epithelial layer was not removed during the surgery. Although the thickness of the uroepithelial layer was consistent in all the four groups (Fig. 4), the expression of pancytokeratins (AE1/AE3) was much different among the four groups. It was the weakest in the control group, but normalized in the glue + MSCs group. The expression of pancytokeratins (AE1/AE3) was correlated to the density of blood vessels and recovery of smooth muscle underneath the epithelium. One possible explanation was that the transplanted MSCs secreted cytokines that protected the epithelial cells from apoptosis and stimulated angiogenesis. The enhanced formation of new blood vessels provided nutrients and oxygen to the epithelial cells and the newly formed urethral smooth muscle.
The regeneration of urethral smooth muscle is important for prevention of urethral fistulae and distortion. In this study, nontreatment led to severe urethral fistulae and distortion (Fig. 3A), while treatment with fibrin glue combined with autologous MSCs successfully recovered the urethral smooth muscle and prevented remodeling of the urethra. The distance between the skin of the ventral aspect of the penis to the epithelial layer in the glue + MSCs group was greater than the normal animals. Although the overgrowth of urethral smooth muscle caused no urethra stricture up to 30 days, long-term experiments are needed to evaluate the possibility.
In this study, the subcutaneous tissue was excised with the skin and the urothelial layer remained. The subcutaneous tissue mainly included the muscular layer and collagen layer. In the normal group, the SMC area of was less than the area of the collagen; the ratio of cell/collagen was about 34.6% (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/tea). In the control group at 10 days, the collagen layer and SMCs were both less than the normal group; however, SMCs were more seriously reduced, so the ratio of cell/collagen was lower than the normal group. In the glue group at 10 days, the collagen layer was also less than the normal group because the fibrin glue was still not fully degraded, while SMCs increased due to the better compatibility, so the ratio of cell/collagen was higher than the control and normal groups. In the glue + MSCs group at 10 days, the collagen layer was replaced by numerous autologous MSCs and the area of SMCs was more than glue group, so the ratio was highest in this groups. Tissue reconstruction was almost finished at 30 days and there was a trend that the ratio of cell/collagen was returning to normal.
In conclusion, the use of MSCs combined with fibrin glue in the repair of urethral fistulae showed improved neovascularization and smooth muscle formation, which effectively prevented the development of urethral fistulae. Our data indicate that fibrin glue combined with MSCs may be a feasible approach for repairing urethral injury.
Footnotes
Acknowledgments
This work was financially supported by the National Key Project for Basic Research of China (No. 2011CB964903 and 2011CB606202), NSFC (No. 30600136), the National Outstanding Youth Found (No. 30725030), and the Tianjin Research Program of Basic Application and Advanced Technology (11JCYBJC09800). X.-L.Z is the recipient of a Senior Scholar Award of Alberta Innovates—Health Solutions (AIHS).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.