
Abstract
Background:
In mutilating hand injuries, tissue engineered tendon grafts may provide a reconstructive solution. We have previously described a method to decellularize cadaveric human flexor tendons while preserving mechanical properties and biocompatibility. The purpose of this study is to evaluate the immunogenicity and strength of these grafts when implanted into an immunocompetent rat model.
Methods:
Cadaveric human flexor tendons were divided into two groups. Group 1 was untreated, and Group 2 was decellularized by treatment with sodium dodecyl sulfate (SDS), ethylenediaminetetraacetic acid (EDTA), and peracetic acid (PAA). Both groups were then analyzed for the presence of major histocompatibility complexes by immunohistochemistry (IHC). Pair-matched tendons from each group were then placed into the dorsal subcutaneous tissue and anchored to the spinal ligaments of Wistar rats for 2 or 4 weeks, and harvested. The infiltration of B-cells and macrophages was determined using IHC. The explants where then subjected to mechanical testing to determine the ultimate tensile stress (UTS) and elastic modulus (EM). Statistical analysis was performed using a paired Student's t-test.
Results:
The decellularization protocol successfully removed cells and MHC-1 complexes. At 2 weeks after implantation, there was increased infiltration of B-cells in Group 1 (untreated) compared with Group 2 (acellular), both in the capsule and tendon substance. There was improved ultimate tensile stress (UTS, 42.7±8.3 vs. 22.8±7.8 MPa, p<0.05) and EM (830.2±206.7 vs. 421.2±171.3 MPa, p<0.05) in tendons that were decellularized. At 4 weeks, there was continued B-cell infiltration in Group 1 (untreated) compared with Group 2 (acellular). There was no appreciable difference in macrophage infiltration at both time points. At 4 weeks Group 2 (acellular) demonstrated persistently greater UTS (40.5±9.1 vs. 14.6±4.2 MPa, p<0.05) and EM (454.05±101.5 vs. 204.6±91.3 MPa, p<0.05) compared with Group 1 (untreated).
Conclusions:
Human flexor tendons that were decellularized with SDS, EDTA, and PAA resulted in removal of cellular antigens and a decreased immune response when placed into Wistar rats. These grafts showed better mechanical properties at 2 and 4 weeks when compared with control tendons. Decellularization is an important step toward the use of tissue engineered flexor tendons in upper extremity reconstruction.
Introduction
One strategy is to harvest a cadaveric flexor tendon, remove all donor cells and debris, and repopulate this scaffold with the recipient's cells, thereby creating a “pseudo-autograft.” We have previously described a method to treat a cadaveric human flexor tendon with a detergent and chelating agent3,4 to remove any antigenic debris, followed by an oxidation 5 step to increase porosity. We have subjected constructs to mechanical stimulation using a bioreactor6–9 to improve strength and stiffness, and reseeded them with fibroblasts, tenocytes, and adipoderived stem cells.1,10–12 Although we have shown decellularization with hematoxylin and eosin (H&E) staining of treated tendon, we have yet to prove that this process eliminates major histocompatibility complexes and is nonimmunogenic in vivo. The purpose of this study is to verify that these scaffolds are nonimmunogenic and are biocompatible when implanted into an immunocompetent rat model.
One of the best studied tendon allograft models is anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone or semitendinosus allograft. These allografts are commonly used and although they include risks such as transmission of infectious diseases, they provide the benefit of improved surgical healing times without donor site morbidity.13–15 Jackson et al. found that allograft and autograft incorporation progress through similar phases: graft necrosis, cellular repopulation, revascularization, and collagen remodeling. However, they found that autografts progress through this process and arrive at their ultimate strengths sooner than allografts. 13 In a goat model, these same researchers found that allografts had weaker mechanical properties at 6 months, and had a slower rate of biologic incorporation and a persistent inflammatory response. 16 In humans, results have not been conclusive. Some studies show equivalent long-term results among allografts and autografts,17–20 whereas others support the preferential use of autografts.21,22
One hypothesis for the initial mechanical difference between autografts and allografts is the development of an immune response. Pinkowski et al. noted in a prospective human trial that patients with allograft ACL reconstruction had a positive immune reaction via the lymphocyte blast transformation test.14,23 Thorson et al. noted that dogs treated with allografts had increased antibody response in addition to elevated synovial leukocytes. 24 Although the general consensus is that allografts do regain strength over time and are an acceptable means of reconstruction, an option that imparts early strength without significant immune reaction would be ideal for reconstruction and rehabilitation.
Flexor tendon allografts are not as well studied in the literature because they are not used as commonly as ACL allografts. In addition, the hand and forearm is a highly vascular location—unlike the relatively avascular knee joint, which some argue to be an immune privileged space 25 —and will thus develop a stronger immune reaction to any antigenic components. It is believed that insoluble collagen, which is conserved across species, is not immunogenic whereas cellular debris, specifically major histocompatibility complexes, are relatively immunogenic.26,27 It is for this reason that any suitable graft material for the upper extremity must be completely free of donor cellular debris. Although our lab focuses on decellularization using a detergent, other options include deep freezing, freeze drying, irradiation, and chemical denaturing.3,5,28–32 We hypothesize that (1) our decellularization process, involving sodium dodecyl sulfate (SDS) and ethylenediaminetetraacetic acid (EDTA), and our oxidization process utilizing peracetic acid (PAA), successfully removes all cellular debris, and most importantly, all major histocompatibility complexes. The result is an acellular tendon scaffold that is nonimmunogenic. We also hypothesize that (2) inserting these decellularized scaffolds into immunocompetent Wistar rats will lead to less of an inflammatory response than untreated grafts. As a result, decellularized scaffolds may demonstrate greater strength and stiffness compared with the control, untreated group in the early healing period.
Materials and Methods
Harvest of human flexor tendon
Human flexor digitorum profundus tendons were obtained from fresh, frozen cadaver forearms (Science Care). Tendon scaffolds were harvested from the musculotendinous junction proximally to the osseotendinous junction distally. They were then stored in phosphate buffered saline (PBS) at −70°C until use. Tendons from each hand were pair matched to the contralateral side, and one tendon from each pair was randomly selected for decellularization. Untreated tendon scaffolds were designated as Group 1 while decellularized scaffolds were designated as Group 2.
Decellularization of human flexor tendon
Our lab has previously developed an optimal decellularization protocol using SDS and EDTA 3 . In addition, we have also identified an oxidizing process using PAA to increase construct porosity and facilitate cell penetration 5 . Group 2 constructs were treated in a solution of 0.1% EDTA and 0.1% SDS for 24 h at room temperature, followed by 6 h incubation in buffered 5% PAA.3,5 Tendons were then washed with PBS for 24 h to remove and residual chemicals and stored at −70°C until use.
Immunohistochemical staining for major histocompatibility complex-1
Group 1 (untreated) and Group 2 (acellular) tendon scaffolds were fixed in formalin, embedded in paraffin, and sectioned at a thickness of 7 μm. Slides were immersed in 2% blocking serum for 1 h, followed by incubation with rabbit anti-human MHC-1 primary antibody (Santa Cruz Biotechnology) for an additional hour. After washing in PBS, the slides were incubated for 1 h with the appropriate biotinylated secondary antibody followed by an avidin- FITC conjugate (Vector Biotechnology). The slides were then washed and mounted with a fluorescent mounting-media containing propidium iodide to visualize all cells.
Implantation of flexor tendon into Wistar rats
We used a human-to-rat xenograft model as a surrogate for a human-to-human allograft model because of the practical difficulty in performing a preclinical human-to-human allograft experiment in humans. The term “allograft” will be used in the remainder of the paper to describe the transplantation of nonself donor scaffold and cells into an immunocompetent recipient. Male Wistar rats aged 8–10 weeks were purchased from Charles River, and cared for at our institutional veterinary medical unit. All procedures were performed in accordance with our institutional review board and within an approved animal protocol. Matched tendon pairs consisting of scaffolds from both groups were divided into 5 cm segments and incubated overnight in F12 media (Gibco–Invitrogen) containing an antibiotic and antimycotic agent (Anti-Anti, Gibco–Invitrogen). Under general inhalational anesthesia, the Wistar rats were shaved and cleansed with povidone iodine. Each rat received two tendon scaffold segments from the same Group (either two fresh frozen, or two acellular) to avoid cross-reactivity between groups. Cranial and caudal transverse incisions were made over the dorsal surface separated by the approximate length of the tendons to be implanted. Tendons were subcutaneously tunneled, drawn out to length, and secured to the vertebral spinous processes, interspinous and supraspinous ligaments on either side of the midline with 3–0 Prolene (Ethicon–Johnson & Johnson). The overlying skin was closed with a combination of 4–0 Prolene sutures and skin staples (Proximate, Ethicon Endo-Surgery) which were removed after 10 days. Each animal received postoperative antibiotics for 7 days. There were a total of eight rats at each of the two time points (Eight matched tendon pairs per time point). At the appropriate time, rats were euthanized and the tendons were explanted.
Immunohistochemical staining for B-cells and macrophages
Harvested tendon specimens were processed for immunohistochemistry (IHC) in the manner previously described. For B-cell staining, a goat anti-rat CD20 primary antibody was used (Santa Cruz Biotechnology). For macrophage staining, a mouse anti-rat CD68 primary antibody was used (Santa Cruz Biotechnology). Rat spleen was used as a positive control. Sections were also stained with H&E to evaluate tendon microarchitecture and cellular infiltration.
Evaluation of mechanical properties
Immediately after harvest, tendons were kept hydrated in PBS and meticulously dissected free of adherent tissue and capsule. Tendon scaffold ends were then fastened between two layers of fine grade sandpaper using commercially available cyanoacrylate glue and attached to the crossheads of a servo-controlled materials testing system (MTS 858; MTS). Pretest orthogonal images (together with a known scale) were obtained using a digital camera to allow calculation of graft cross-sectional area. A series of 10 preconditioning cycles (0-100N, 10 mm/min) was implemented before distraction to failure. After the tenth cycle, the tendon was pulled to failure, and the system recorded force and displacement over time. This data was used to calculate the ultimate tensile stress (UTS), defined as the ultimate load divided by the cross-sectional area at the failure site, and the elastic modulus (EM), defined as the slope of the stress-strain curve.
Statistical analysis
Analysis of biomechanical properties was performed using a paired-student's t-test. Significance was set at a p-value<0.05.
Results
Immunohistochemical staining for major histocompatibility complex-1
Treatment with EDTA, SDS, and PAA resulted in successful removal of MHC-1 complexes and nucleic acids (Fig. 1) in Group 2 (acellular) scaffolds. There was preservation of normal collagen architecture with increased porosity. In contrast, MHC-1 complexes and nuclei were abundant in the untreated, fresh-frozen control tendons (Group 1).
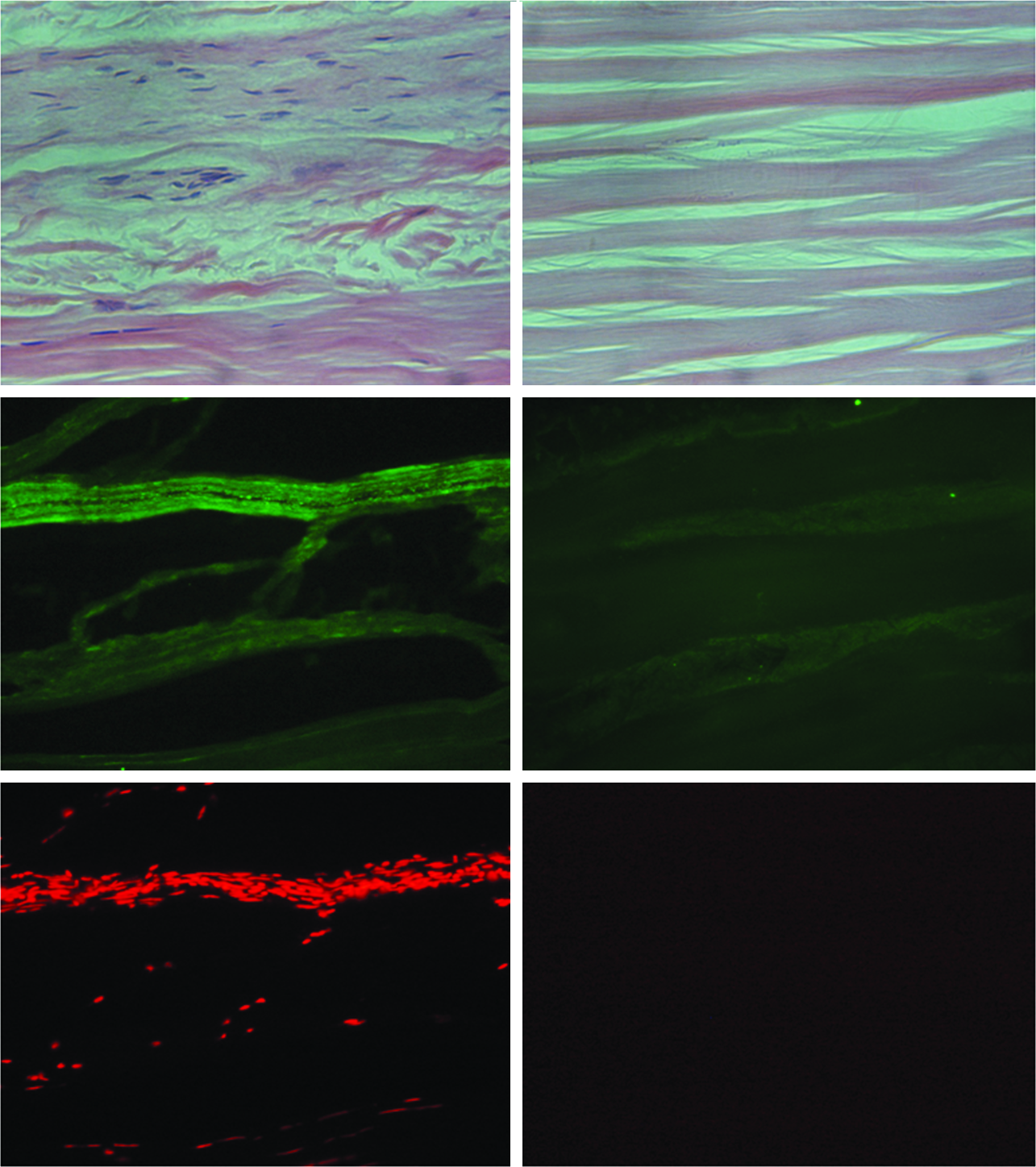
Comparison of Group 1 (untreated, left) human flexor tendon and Group 2 (Acellular, right) human flexor tendon. Top: Hematoxylin and eosin (H&E) sections. Middle: Immunohistochemicial staining for human MHC-1 complexes. Bottom: Propidium Iodide staining. All images at 20× magnification. Color images available online at www.liebertonline.com/tea
Two-week explants
There was noticeable difference in inflammation and cellularity between both groups on H&E stains (Fig. 2). There was a larger capsule in the control group (Group 1) with a greater degree of cellularity within the tendon. This level of inflammation appeared to disrupt the normal collagen architecture.
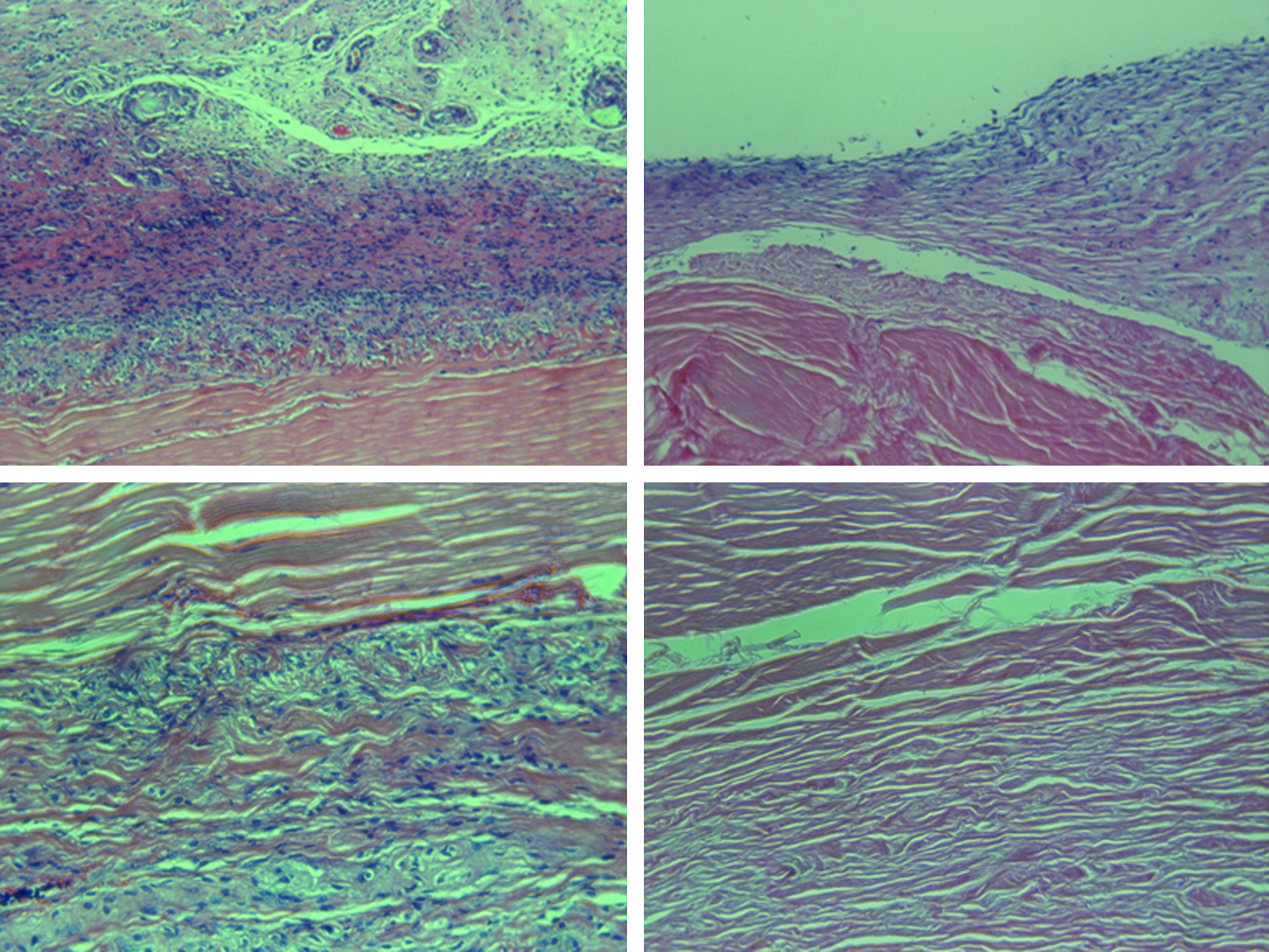
H&E staining of Group 1 (untreated, left) and Group 2 (acellular, right) explants at 2 weeks. Top: Inflammatory capsule (10×). Bottom: Tendon core (20×). Color images available online at www.liebertonline.com/tea
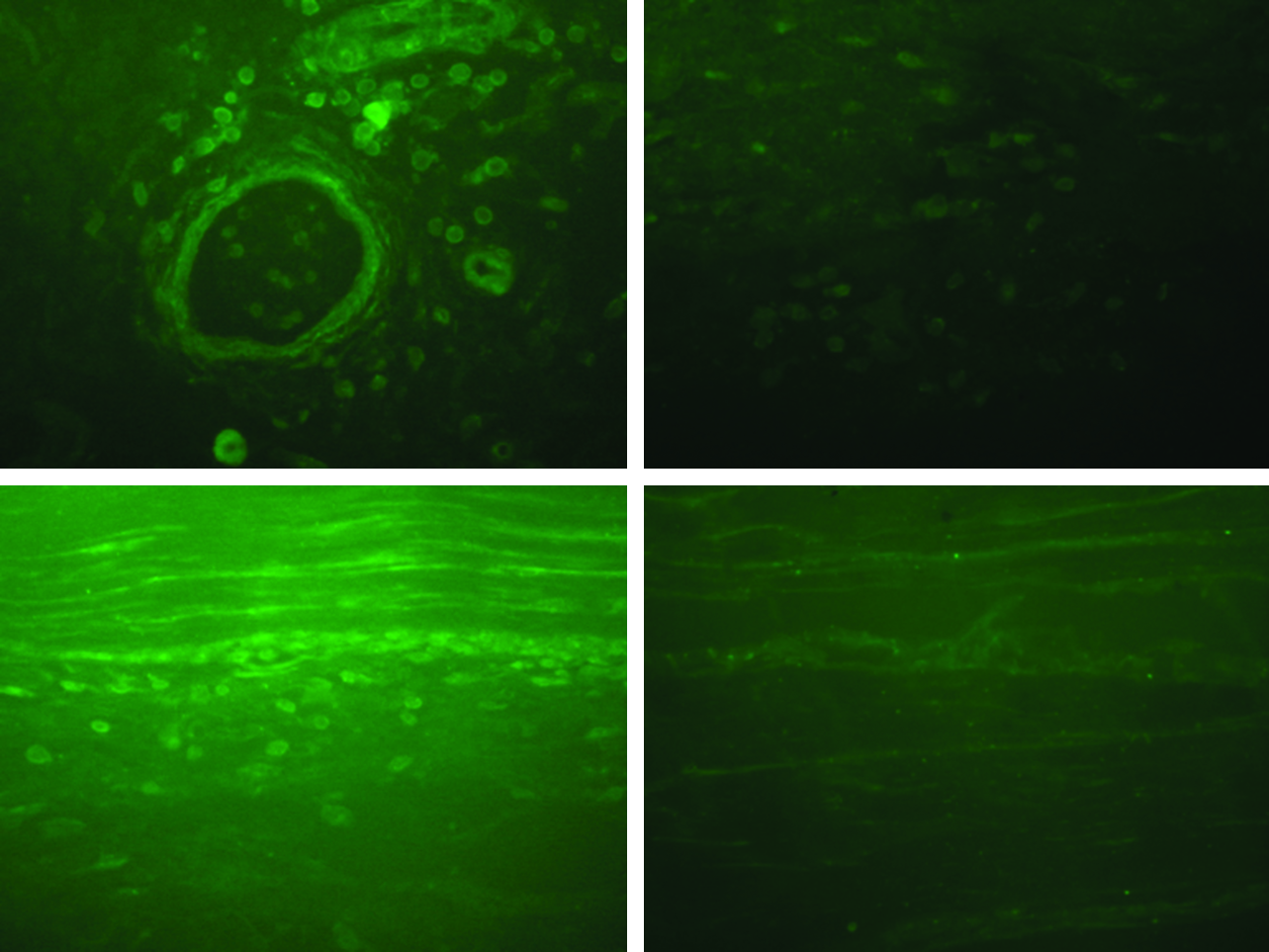
Immunohistochemical staining for CD-20 (B-cells) showed a noticeable difference between the control (Group 1) and decellularized group (Group 2) (Fig. 3). There was greater B-cell infiltration into both capsule and deep tendon substance in the control group (Group 1). There was minimal B-cell infiltration in the decellularized group (Group 2).
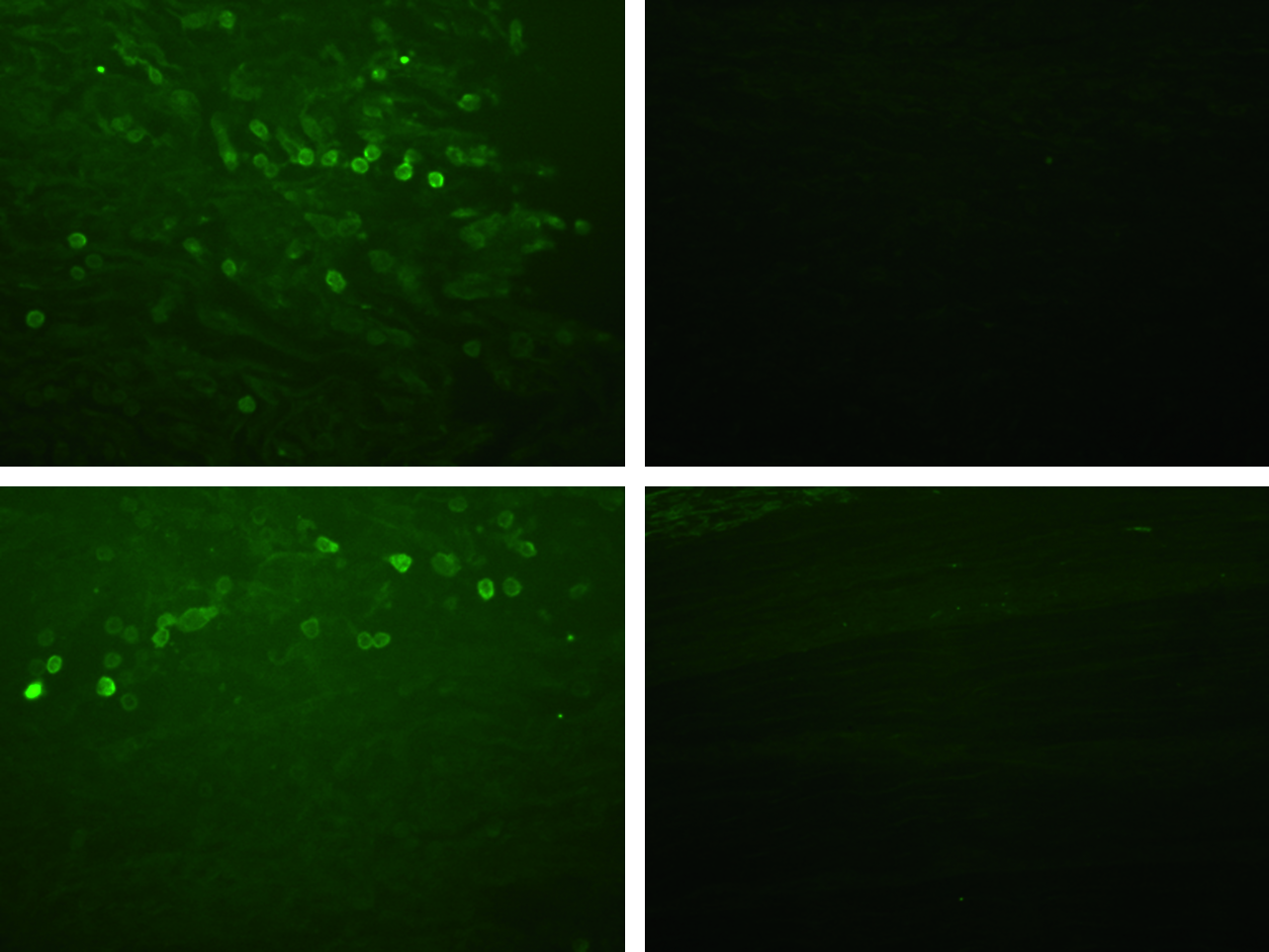
Immunohistochemimcal staining of CD20 (B-cells) of Group 1 (untreated, left) and Group 2 (acellular, right) explants at 2 weeks. Top: Inflammatory capsule. Bottom: Tendon core. All images 40× magnification. Color images available online at www.liebertonline.com/tea
There was no appreciable difference in macrophage (CD-68) infiltration between the two groups, in either the capsule or the deep tendon substance (Fig. 4).

Immunohistochemimcal staining of CD68 (Macrophages) of Group 1 (untreated, left) and Group 2 (acellular, right) explants at 2 weeks. Top: Inflammatory capsule. Bottom: Tendon core. All images 40× magnification. Color images available online at www.liebertonline.com/tea
Four-week explants
H&E stained sections of the 4-week explants showed a significant difference in immune response (Fig. 5). Group 1 (untreated) tendon constructs had capsules with increased cellularity and vascularity, and sheets of inflammatory cells penetrating into the tendon substance, disrupting normal collagen architecture. Group 2 (acellular) tendon constructs had smaller inflammatory capsules and lacked deeply penetrating sheets of inflammatory cells. Group 2 appeared to have physiologic repopulation of the tendons by spindle-shaped fibroblast-like cells.
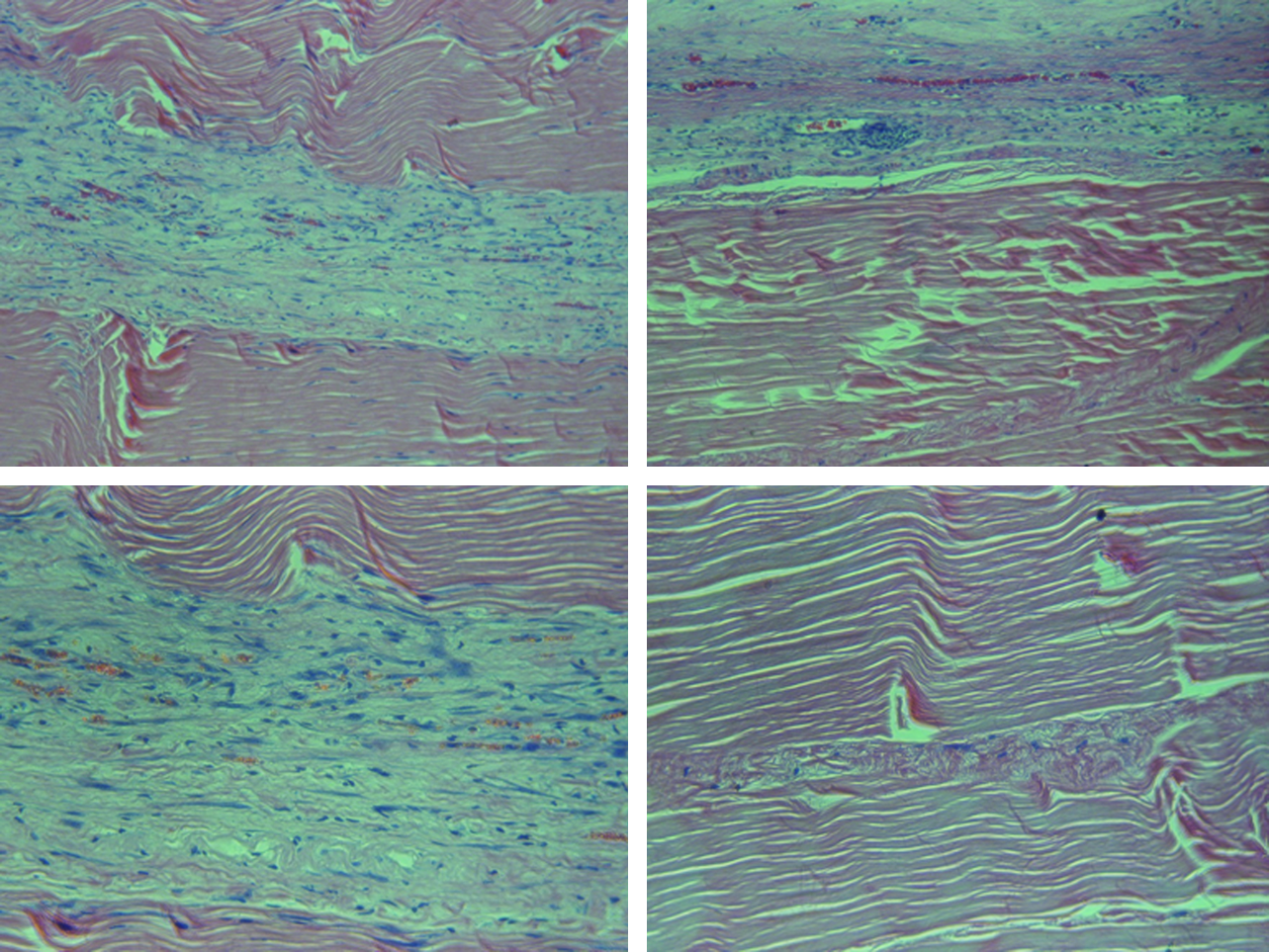
H&E staining of Group 1 (untreated, left) and Group 2 (acellular, right) explants at 4 weeks. Top: Inflammatory capsule (10×). Bottom: Tendon core (20×). Color images available online at www.liebertonline.com/tea
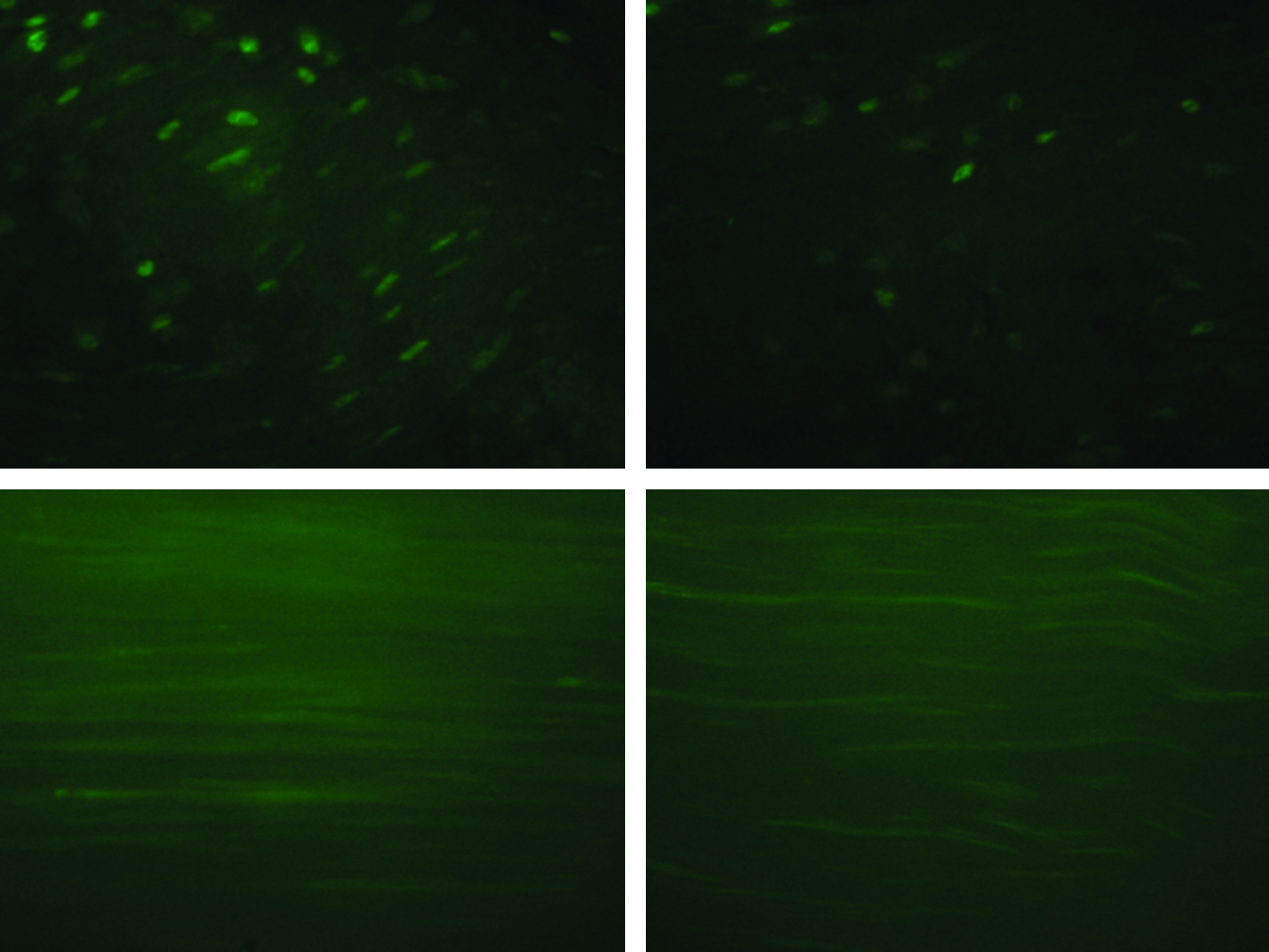
Immunohistochemical staining for CD-20 showed an increased number of B-cells in the capsule of Group 1 explants (Fig. 6). In addition, B-cells were present within Group 1 explants but not in Group 2.
Immunohistochemimcal staining of CD20 (B-cells) of Group 1 (untreated, left) and Group 2 (acellular, right) explants at 4 weeks. Top: Inflammatory capsule. Bottom: Tendon core. All images 40× magnification. Color images available online at www.liebertonline.com/tea
At 4 weeks, there was still no appreciable difference in macrophage infiltration between the two groups (Fig. 7). There were macrophages present in the capsule in both groups, but not within the tendon substance.
Immunohistochemimcal staining of CD68 (Macrophages) of Group 1 (untreated, left) and Group 2 (acellular, right) explants at 4 weeks. Top: Inflammatory capsule. Bottom: Tendon core. All images 40× magnification. Color images available online at www.liebertonline.com/tea
Mechanical testing of explants at 2 and 4 weeks
UTS and EM were calculated at the 2 and 4 week time points. At 2 weeks (n=8 pairs), Group 1 (untreated control) had UTS of 22.8±7.8 MPa and EM of 421.2±171.3 MPa. Group 2 (acellular) had higher UTS of 42.7±8.3 MPa and higher EM of 830.2±206.7 MPa (p<0.05 for both, paired Student's t-test). Overall, strength was 1.87-fold greater and stiffness was 1.97-fold greater in Group 2 (acellular) (Fig. 8).
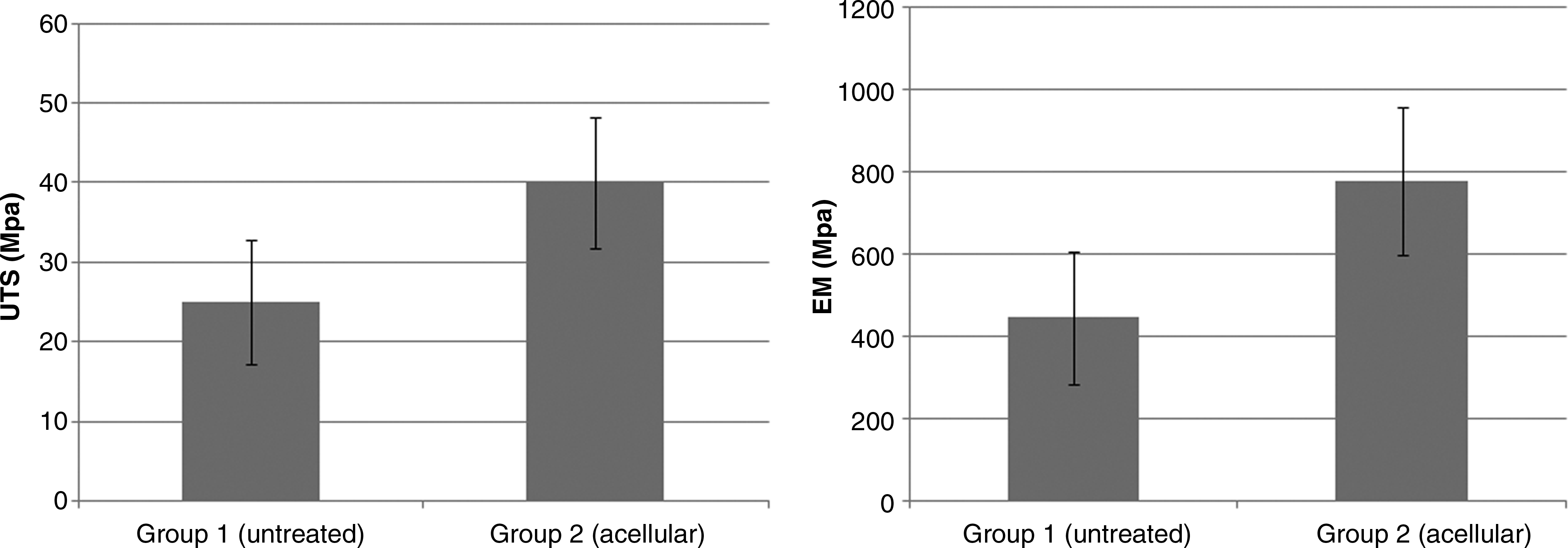
Biomechanical properties of explants at 2 weeks. Ultimate tensile stress (UTS) is displayed in the graph on the left with elastic modulus (EM) on the right. Group 1 (untreated) had a mean UTS of 22.8±7.8 MPa and EM of 421.2±171.3 MPa. Group 2 (acellular) had mean UTS of 42.7±8.3 MPa and EM of 830.2±206.7 MPa (p<0.05, paired Student's t-test).
At 4 weeks (n=8 pairs), Group 1 (control) explants had UTS of 14.6±4.2 MPa and EM of 204.6±91.3 MPa. Group 2 (decellularized) explants continued to have higher UTS of 40.5±9.1 MPa and EM of 454.05±101.5 MPa (p<0.05, paired Student's t-test). Overall, strength was 2.56-fold greater and stiffness was 2.21-fold greater in Group 2 (Fig. 9).
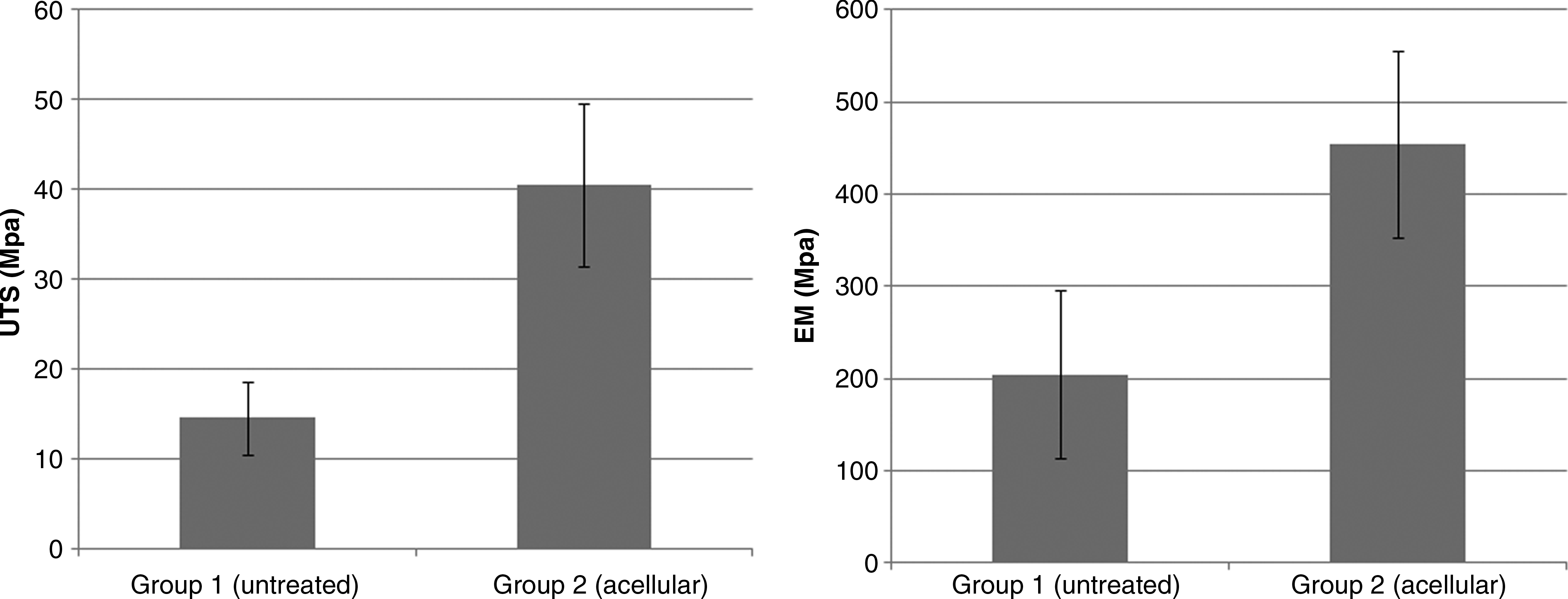
Biomechanical properties of explants at 4 weeks. UTS is displayed in the graph on the left with EM on the right. Group 1 (untreated) had a mean UTS of 14.6±4.2 MPa and EM of 204.6±91.3 MPa. Group 2 (acellular) had mean UTS of 40.5±9.1 MPa and an EM of 454.05±101.5 MPa (p<0.05, paired Student's t-test).
Discussion
The focus of our research is to use tissue engineering principles to create a source of flexor tendon allografts. This is clinically important because when faced with large volume tendon losses, autograft sources are quickly exhausted. Other commercially available allografts such as semitendinosus grafts are anatomically distinct from flexor tendons. In particular, these tendons lack the synovial layer found on flexor tendons and have higher rates of adhesion formation when used for reconstruction.33,34 We have previously described a method to decellularize cadaveric human flexor tendons, increase their porosity, and reseed them with fibroblasts, tenocytes, and adipoderived stem cells.3–5,11,35 In this study, we aimed to evaluate the immunogenicity of these decellularized scaffolds in an animal model. We were able to show that SDS, EDTA, and PAA treatment of human flexor tendon successfully removes potential antigens and that these constructs elicit a diminished immune response and have superior mechanical properties when implanted into an immunocompetent rat model.
Immunohistochemical staining for major histocompatibility-1 complexes showed nearly complete removal of these proteins when compared with Group 1. This is an important finding because MHC-1 complexes interact with immunological cells such as B-cells, T-cells, and macrophages to elicit an immune response. Baseline H&E staining is not sufficient to demonstrate decellularization because only nuclear and cytoplasmic components are stained, and extracellular and membranous proteins such as MHC-1 complexes remain undetected. This complex plays a significant role in humoral immunity, and we would expect that when used in reconstruction, this component of an immune response would be blunted.
We chose an immunocompetent Wistar rat model for our in vivo studies. Although this model is not the ideal human-to-human transplant model, we thought it would be appropriate given that there have been reports in the literature of reactivity of MHC complexes between mouse and human cell lines. 36 In addition, compared with the smaller mouse model, the larger rat model allows implantation of longer (5 cm) flexor tendon segments. This allows for more secure anchoring to fixed structures and facilitates cross-head clamping (1 cm each end) during biomechanical testing. Reliable markers to evaluate the degree of immune response, namely CD20 (B-cells) and CD68 (macrophages), were also available. Further, in our in vivo model these 5 cm tendons were anchored to the vertebral spinous processes and associated ligaments. The anchoring sutures kept the tendon scaffolds at length and allowed delivery of periodic tensile load during flexion and extension of the rat spine during movement. Although this setup was not able to accurately reproduce the physiological flexor tendon environment, it afforded us a way to evaluate both the immune response and mechanical properties of tendons implanted into a richly vascular environment comparable to the hand and upper extremity.
Both IHC for B-cells and macrophages, and H&E staining at 2 and 4 weeks showed a difference between Group 1 (untreated) and Group 2 (decellularized) constructs. In Group 1 at 2 weeks, H&E staining showed a larger capsule and increased cellular infiltration throughout the tendon. There was also a capsule in Group 2. However it was neither as pronounced nor as vascular. We believe that this is attributable to a foreign body reaction rather than gross rejection. IHC for B-cells demonstrated a stark difference. There was prominent B-cell infiltration throughout both capsule and deep tendon substance in Group 1 (untreated control), but not Group 2 (acellular). With regard to macrophages, we found that these innate immune cells localized to the capsule, but were not found in the tendon substance in both groups.
At 4 weeks, H&E staining showed further tendon substance infiltration in the Group 1 (untreated). These inflammatory cells appear to invade the tendon in “sheets,” physically separating the collagen fibers. In Group 2 (decellularized), there were cells in the tendon core which were absent at 2 weeks. These cells displayed spindle shape morphology, appeared in monolayers, and had not disrupted the collagen structure. This appearance suggests normal physiologic repopulation of these tendon grafts that takes place over time. B-cell infiltration is again very prominent in the Group 1, both in the capsule and tendon substance. Interestingly, some B-cells are now apparent in Group 2, but only in the capsule and not in the tendon substance. Similar to the 2 week time point, macrophages are only seen in the capsule.
These findings indicate that the immune response to these grafts is primarily of the humoral pathway of the immune system. B-cells were the dominant cell type and increased in number from the 2- to 4-week time point. They were present throughout the capsule and in the tendon core at sites of collagen degradation and more importantly, compromised tendon structure. Macrophages, on the other hand, were limited to the capsule, which may indicate that they were present as a reaction to a foreign body, rather than to cellular proteins and MHC-1 complexes.
The findings on microscopic examination provide explanation for the results of biomechanical testing. At 2 weeks, the UTS was 1.8-fold greater and EM was 1.9-fold greater in the Group 2 (decellularized) compared with Group 1 (untreated controls). At 4 weeks, UTS was 2.5-fold greater and EM was 2.2-fold greater in Group 2 compared with Group 1. The immune response increased in Group 1 as time progressed, leading to a divergence in strength and stiffness between the two groups. This suggests that the immune response plays a role in the mechanical properties of the tendon. Although fresh-frozen allografts and autografts may ultimately have similar mechanical properties, our data demonstrate that compared with untreated MHC-1 rich allografts, acellular grafts may have greater mechanical properties in the initial healing period that will allow for early rehabilitation and decreased morbidity.
One potential limitation in this study was the use of Wistar rats as our recipient species. The ultimate goal would be to study these scaffolds used for clinical reconstruction in humans—but this undoubtedly has many clinical and regulatory hurdles. However, our aim was to demonstrate that the decellularization process renders these tendon scaffolds nonimmunogenic. In this study, we verified this through transplantation of xenogeneic cellular (Group 1, untreated control) and xenogeneic decellularized (Group 2, treated) grafts, illustrating that there is minimal inflammation and immune response in the latter group.
Another limitation that we observed was implementing a model that delivers physiological axial load to the tendon scaffolds. In pilot studies, grafts were anchored to the underlying fascia. However we found that even at short time points, these grafts tore free of their anchors, curled up, degraded, and had poor biomechanical properties. This suggested that maintaining the tendons in a natural elongated shape, under some tension, is very important. Woon et al. found that tendons treated with cyclic load in a bioreactor significantly weakened when placed in media for 48 h following cycle completion before mechanical testing. 9 In particular, the EM was more significantly affected than the ultimate tensile strength. Interestingly, we saw similar results in the mechanical properties of the tendons at the 2 and 4 week time points. For example, in the fresh frozen group, EM dropped from 421.2 to 204.6 MPa, and in the acellular group, the EM dropped from 830.2 to 454.1 MPa. Although these tendons are not pair-matched temporally and direct pairwise comparison between tendon explants harvested at two disparate time points is not possible, it is interesting to note that EM declined without a corresponding drop in UTS. This could possibly indicate that at longer time points, our model breaks down from a mechanical standpoint, reflecting reduced mechanical stimulation of a tissue that is used to being under constant strain in its native environment. This is consistent with the findings reported by Woon et al.
One avenue for future studies is to study these constructs in a more physiologic animal model. Smaller tendon segments could be implanted in anatomical locations in larger animal models, such as dogs, for flexor tendon repair. This would eliminate the issue described earlier with delivery of physiological stimulation to these constructs. Another option is to consider reseeding these scaffolds with autologous cells such as fibroblasts, tenocytes, or adipoderived stem cells. It is believed that if cells from within the tendon initiate healing, it progresses through an intrinsic healing process that leads to increased strength and less adhesions and inflammation. Woon et al. found that reseeded construct had superior mechanical properties when compared with acellular constructs. 9
Further, the use of growth factors could be explored as ways to augment healing and reconstruction. Thomopoulos et al. showed that exogenous delivery of FGF and PDGF led to improved tendon strength and healing in a canine model.37,38 Using an extended delivery vehicle similar to what Thomopoulos described, we could study the effects of growth factors on the healing and incorporation of these constructs.
In summary, the twofold aim of this study was to (1) evaluate the extent of decellularization of cadaveric flexor tendons in vitro, and (2) determine their immunogenicity when used in vivo. We have shown that following decellularization with EDTA, SDS, and PAA, MHC-1 complexes were removed. In addition, these constructs did not elicit a potent immune response, which was seen in the fresh-frozen control. The constructs also were mechanically superior after explantation at 2 and 4 weeks. Decellularization is an important step in the tissue engineering of human flexor tendons using natural flexor tendon scaffolds.
Footnotes
Acknowledgments
We thank Derek Lindsey, biomechanical engineer at VA Palo Alto Health Care System, for his technical assistance to this project. This work was funded by a VA Medical Merit Review Award and a VA Rehabilitation R&D Merit Review Award.
Disclosure Statement
No competing financial interests exist.