
Abstract
The aim of this study was to explore the effects of maxillary sinus floor elevation and simultaneous dental implantation with a tissue-engineered bone complex of calcium phosphate cement (CPC) scaffolds combined with bone marrow stromal cells (BMSCs). A large animal goat model is used with the tissue engineering method. Eighteen bilateral maxillary sinus of nine goats were randomly allocated into three groups; the CPC/BMSC complex (n=6) was used to elevate maxillary sinus floor with a simultaneous implant placement; the effects were compared with those treated with CPC alone (n=6) or autogenous bone (n=6). After a healing period of 3 months, sequential triad-color fluorescence labeling, micro-CT, as well as histological and histomorphometric analyses indicated that the tissue-engineered BMSC/CPC complex could promote earlier bone formation and mineralization, and maximally maintain the volume and height of the augmented maxillary sinus. By comparison, CPC-alone or autogenous bone achieved less bone formation and later mineralization. Besides, the average bone-implant contact value reflecting the osseointegration was 35.63%±9.42% in the BMSCs/CPC group, significantly higher than 22.47%±4.28% in the CPC-alone group or 28.26%±8.03% in the autogenous bone group. In conclusion, CPC serves as a potential substrate for BMSCs for the maxillary sinus floor augmentation and simultaneous implantation. The tissue-engineered bone might enhance the stability of implants and thus be of great significance to achieve improved quality to restore the oral function in clinic.
Introduction
Ideal grafting materials should meet a number of requirements; for example, they should be biocompatible and should contain osteogenic, osteoconductive, and osteoinductive properties.3,5–7 Autogenous bone maximally matches the above requirements and has therefore been defined as the gold standard among the grafting materials. It could be harvested from the parts of the human body such as oral cavity and iliac crest, but the patients would suffer from donor-site morbidities as well as the additional surgical procedures.3,4,8 On the other hand, the use of allograft and xenograft is limited by the risks of eliciting an immune response and by the potential induction of transmissible diseases. Therefore, synthetic materials are introduced in the field as part of the medical practice. 1
Among the synthetic materials, hydroxyapatite (HA), tricalcium phosphate (TCP), and a calcium phosphate compound such as calcium phosphate cement (CPC) have excellent biocompatibility and osteoconductivity.9–12 HA is biocompatible and does not induce a sustained foreign body response or a toxic reaction. However, under physiological pH, it is least soluble among the naturally occurring calcium phosphates.13,14 β-TCP belongs to another biocompatible and osteoconductive calcium phosphate biomaterials. It provides a scaffold with potential bony in-growth. 15 However, β-TCP degraded too fast, and often less bone was formed as compared with the rate of scaffold degradation.16,17 As an alternative to those calcium phosphate scaffolds, CPC grafting material includes advantages such as biocompatibility, the ability to be fabricated into functional shapes, controlling biological absorption ability, and easy process. 18 Porous CPC alone as a grafting material has been widely used, including an alveolar ridge augmentation, maxillofacial reconstruction, and cranial defect reparation.7,19,20
Nevertheless, those above-mentioned materials still lack an osteogenic ability. Fortunately, the tissue engineering technique was introduced into the field by combining bioactive cells into the three-dimensional (3D) porous scaffolds. 21 Bone marrow stromal cells (BMSCs) can be harvested from bone marrow. They allow a large-scale production, but require only a limited tissue source, and what is more important is that they have definite osteogenic potency. As a result, the combination of BMSCs and bioengineered scaffolds, including CPCs, for bone regeneration has been investigated by many research groups.1,22–28 Based on these findings, we hypothesize that the CPC/BMSC complex might be an ideal alternative in lifting maxillary sinus to overcome the limitations by using the autograft, allograft, or artificial bone materials alone. 28
In this study, we explored the effects of maxillary sinus floor elevation with the CPC/BMSC complex in a goat model with simultaneous dental implantation. Importantly, simultaneous implantation could avoid multiple surgeries and reduce the duration of treatment compared with the delayed dental implantation. However, this more challenging surgical procedure for oral function restoration required enhanced osteogenesis and osseointegration. Thus, we are trying to find out whether a tissue engineering method by combining BMSCs with CPC scaffolds will be more beneficial in terms of enhanced new bone formation and implant-bone contact rate after simultaneous dental implantation in this preclinical large animal model.
Materials and Methods
Animals
Nine healthy female goats, 12 months old and about 18–22 kg in weight, were used in the study with the experimental protocol formally approved by the Animal Care and Experiment Committee of Ninth Peoples Hospital affiliated to Shanghai Jiao Tong University, School of Medicine.
CPC scaffold
CPC was fabricated based on equimolar amounts of tetracalcium phosphate (TTCP) and dicalcium phosphate anhydrous (DCPA). 29 TTCP was synthesized by a solid-state reaction between calcium phosphate and calcium carbonate at 1500°C for 10 h, and DCPA was obtained at 120°C by removing the crystallization water in dicalcium phosphate dihydrate, which was prepared from (NH4)2HPO4 and Ca(NO3)2 in an acidic environment. The CPC powders were fabricated by mixing TTCP and DCPA in a molar ratio of 1:1. Finally, porous CPC scaffolds were prepared by a particulate-leaching method. In short, the CPC powder was mixed with water using a spatula at a powder/liquid ratio of 3:1 (g/mL) to form a cement paste. Sodium chloride (NaCl) particles sieved with the sizes of 300–500 mm were added as a porogen into the CPC paste. The mixture of CPC paste/NaCl was placed into stainless steel molds with the size of 3-mm diameter×3 mm, and the mixture was molded under a pressure of 2 MPa. After storage in beakers in a constant temperature oven at 37°C and 100% relative humidity for 2 days, the samples were then immersed in deionized water to leach out the porogen. Finally, these samples were dried at 50°C in an oven to obtain sponge-like porous scaffolds. The morphology and the pore size of the CPC scaffolds were characterized by a scanning electron microscope (SEM; Philips SEM XL-30), and the porosity of the scaffolds was measured by the Archimedes method in distilled water. Three samples were tested to calculate the average porosity. 30
Cell isolation, culture, and tests of osteoblastic characteristic tests
Autologous BMSCs were obtained from the bone marrow of goats about 3 weeks before the surgical time. Under general anesthesia, 5 mL of bone marrow was aspirated from the iliac bone using an 11-gauge bone aspiration needle moistened with heparin (1000 U/mL). After being washed and centrifuged in phosphate-buffered saline (PBS), the obtained cell suspension was cultured in a sterile 100-mm dish (Falcon) with the Dulbecco's modified Eagle's medium (Gibco) containing 10% (v/v) fetal bovine serum (FBS) (Hyclone, Perbio) and incubated under standard cell culture conditions of 37°C, 5% CO2, 95% O2, and 100% saturated humidity. The medium was changed after 5 days, and the change of it was done every 3 days thereafter. When the cells became 70%–80% of confluence, they were detached with 0.25% trypsin and 0.01% EDTA, and subcultured at a density of 1×105 cells/mL in an osteogenic induction medium (a primary medium containing 10−8 M dexamethasone, 10 mM β-glycerophosphate, and 50 μg/mL ascorbic acid) (Sigma Chemical Co.). After two passages, the sufficient amount of BMSCs would be obtained for the following studies.
After being cultured in an osteogenic induction medium for another 14 days, BMSCs were detected for their differentiation by alkaline phosphatase (ALP) activity using p-nitrophenylphosphatase as a substrate, and the level of mineralization was determined by Von Kossa staining for nodules containing calcium mineral as was described by Bonewald et al. 31
Osteocalcin immunohistochemistry staining
BMSCs were cultured for immunohistochemistry staining to investigate the expression of osteocalcin (OCN). In so doing, the cells were seeded on the slides for 2 days and fixed with 4% paraformaldehyde for 20 min. They were treated with 0.25% Triton-X for 10 min at room temperature and washed with PBS. Nonspecific binding was blocked with normal goat serum for 30 min at room temperature. The slides were incubated with mouse monoclonal antibodies against OCN (Abcam) overnight at 4°C. The goat anti-mouse secondary antibody (Boster) was incubated for 2 h and then washed with PBS. Diaminobenzidine (DAB) staining (Boster) was made by DAB substrate. The slides were counterstained with hematoxylin, dehydrated through a series of alcohols and cleared through xylene, and then mounted with resin. The positive cells stained brown and the negative cells showed only blue/green nuclei, but no brown cytoplasm. The controls consisted of incubation with PBS instead of a primary antibody.
Transcription analysis of osteoblastic genes
The transcription of collagen I (Col I), ALP, and OCN was detected by the reverse transcription–polymerase chain reaction (RT-PCR). Briefly, total RNA was prepared from the BMSCs by using Trizol reagent according to the manufacturer's protocol (Invitrogen). cDNA was generated by using Oligo(dT) and AMV reverse transcriptase (TaKaRa). The following PCR amplification reaction utilized the Taq polymerase (TaKaRa) and gene-specific primers (Shenggong) as was specified in Table 1. All the primer sequences were designed with Primer Premier 5.0 Software, and synthesized commercially.
Col I, collagen I; OCN, osteocalcin; ALP, alkaline phosphatase; PCR, polymerase chain reaction.
Preparation of BMSC/CPC constructs
CPC scaffolds (3-mm diameter×3 mm), with a volume porosity of ∼70% and a mean pore size of 300–500 μm, were sterilized by 60 Co irradiation before being used. For the cell seeding, BMSCs were collected and then resuspended in the osteogenic induction medium without FBS at a density of 2×107 cells/mL. The cell suspension was pipetted tardily onto the scaffold, and BMSCs were seeded into the scaffolds up to a final saturation. After the scaffolds were returned to the incubator for 4 h to allow a cell's initial attachment, implantation surgeries were performed in vivo. The additional cell-seeded CPCs were prepared for the in vitro analysis of cell attachment on the construct by SEM.
Surgical procedure
The second and third maxillary premolars of each goat were extracted bilaterally 3 months before the operation. The maxillary alveolar height was reduced to 5 mm to simulate the clinical situation, and the extraction sites were allowed to be healed as was previously described by the current group. 32
Preoperatively, the animals were starved fasted for 48 h, but were allowed water ad libitum. All surgical procedures were performed under general anesthesia by intravenous administration of pentobarbital sodium (30 mg/kg). After orotracheal intubation and ventilation, the goats were connected to a heart monitor, and the general anesthesia was monitored during the entire course of surgery.
The procedure of maxillary sinus floor augmentation with simultaneous implant placement was performed identically on both sides of each goat (Fig. 1). In brief, the bony facial wall was exposed through a paramedian oblique sagittal skin incision about 6 cm in length. After one third of the masseter muscle was released at its origin, a bone window of 1.5×1.5 cm2 was created with a bur, and the sinus membrane was gently lifted from the maxillary sinus floor with bent dissectors (Frios® sinus Set; Friatec), and care was taken to avoid perforation of the antral membrane. Then, the maxillary edentulous region was slit by a supracrestal incision, extended from the first maxillary premolar to the first molar. The mucoperiosteal flap was raised to gain access to the underlying alveolar bone. One cylinder-screwed implant of pure titanium with a sandblasted and acid-etched surface (ITI®-SLA; Strauman AG) and a mold of 3.3 mm in diameter and 12 mm in length was placed on the position of the third maxillary premolar. The elevation spaces between the antral membrane and the sinus floor were then randomly filled with the following three groups of granular grafts around the implant with 1.5 cm3 in volume: Group A, the tissue-engineered BMSC/CPC complex (n=6); Group B, CPC alone (n=6); Group C, autogenous bone obtained from an iliac crest (n=6) as a positive control. For the autogenous bone grafts, cancellous bone was harvested through a fenestration in the ipsilateral iliac crest and kept in physiological saline before use. Finally, the mucoperiosteal flap was repositioned and sutured. To prevent postoperative infections, the animals received penicillin for 3 days. They were kept on a soft diet during the first week after surgical procedures.
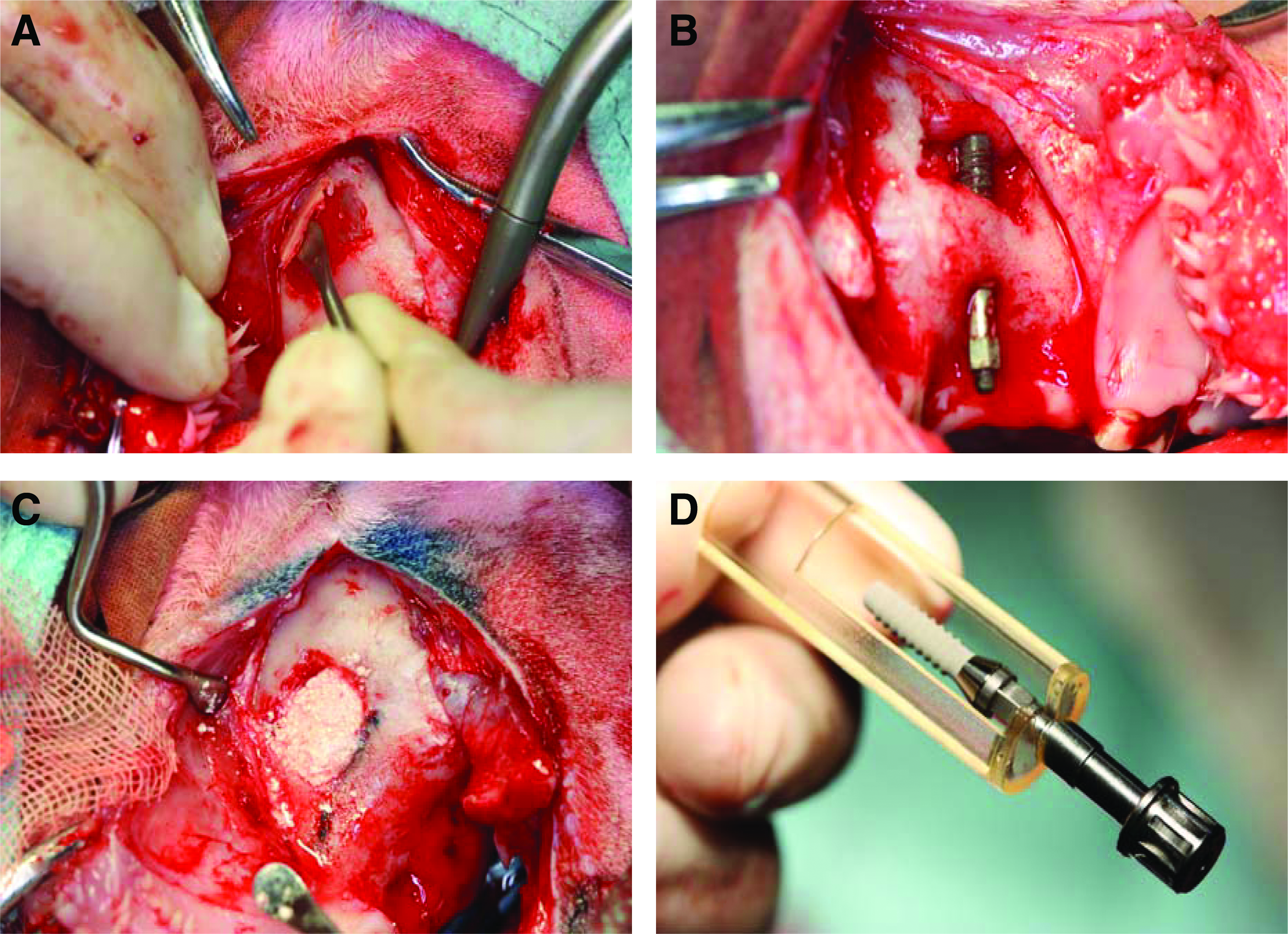
Operation procedure of goat maxillary sinus floor augmentation with simultaneous implant placement.
Polyfluorochrome sequential labeling
Polyfluorochrome sequential labeling was carried out to assess the time course of new bone formation and mineralization. The goats received tetracycline hydrochloride (Sigma Chemical Co.) of 25 mg/kg subcutaneously 4 weeks postoperatively, and 30 mg/kg of alizarin red S (Sigma Chemical Co.) 8 weeks postoperatively, respectively. Two weeks before sacrifice, 20 mg/kg of calcein green (Sigma Chemical Co.) was administrated subcutaneously. 33
Sample preparation
Three months after the operation, the goats were sacrificed by intravital intracarotid perfusion under general anesthesia. Ten liters of physiological NaCl solution was applied to the carotid artery under 120 mm/Hg pressure to wash out the blood from the vessels. Subsequently, the goats were perfused with 10% neutral-buffered formalin (full formalin 100 mL, distilled water 900 mL, sodium dihydrogen phosphate 4.0 g, and disodium hydrogen phosphate 6.5 g) (Sigma Chemical Co.) for the internal fixation of the tissues.34,35 Then, the maxillas were immediately dissected and the overlying soft tissues scraped away, with the segments of maxillary sinus containing the implant block-resected and fixed in 10% neutral-buffered formalin for 4 days.
Micro-CT scanning
Each specimen was subjected to microcomputed tomography scanning using a desktop micro-CT device (μCT-80; SCANCO Medical AG). The microfocus of the X-ray source of the μCT system had a spot size 7 μm and maximum voltage 36 kV. A high-resolution protocol (pixel matrix, 1024×1024; voxel size, 36 μm; slice thickness, 36 μm) was applied. The specimens were scanned with up to 400 transverse slices. After measuring the ranges and means of the gray levels characteristic of the CPC scaffold and the newly formed bone, the visually determined threshold to separate the CPC scaffold from the newly formed bone was selected, allowing a reliable distinction between the two tissue types. 36 The volume of the regenerated bone within the sinus augmentation region was calculated using μCT-80 auxiliary software (Scanco Medical AG). Micromorphometric bone parameters, including relative bone volume (RBV, newly formed bone voxels per complete tissue voxels of the initially implanted CPC volume: %), trabecular thickness (Tb.Th: mm), and trabecular separation (Tb.Sp: mm) as well as trabecular number (Tb.N: 1/mm) were separately calculated.37–41
Histological and histomorphometric observation
The implant-bearing specimens were dehydrated in ascending grades of ethanol and embedded in polymethylmethacrylate (Sigma Chemical Co.) for 14 days before polymerization. The specimens were cut and ground along the longitudinal axis mesiodistally parallel to each implant with the Exact Cutting and Grinding Equipment (Exact Apparatebau) to a thickness of 180 μm, according to the technique described by Donath and Breuner. 42 Afterward, each section was further ground to a thickness of 40 μm.
Fluorescent labeling was observed with the undecalcified sections under a confocal laser scanning microscope (Leica TCS Sp2 AOBS). Excitation/emission wavelengths for each of the fluorescence were as follows: 405/580 nm (TE, tetracycline, yellow), 543/617 nm (alizarin red S, red), and 488/517 nm (calcein, green), respectively. To explore the bone formation and mineralization in the augmented maxillary sinus around the implants, the fluorochrome staining of the newly formed bone was quantified within a 2-mm-wide zone lateral to the implant surface (interface zone), including the five most apical threads in the augmentation area. 43 Five photographs were taken in the same area for each sample: three using fluorescence microscopy images to analyze the fluorochromes tetracycline, alizarin red S, and calcein green with one merging image of three fluorescent labeling used to reflect the mineralization of elevated sinus floor, and with one regular image under transmission light microscopy without a specific filter combined with the former merged image to show the newly form bone in an overlapping manner. The five images were stored digitally and then evaluated histologically and histomorphometrically with an image analysis system (Image-Pro Plus™ 6.0). The parameters included single-labeled surface (sLS), double-labeled surface, bone surface (BS), mineralizing surface (MS/BS, %), mineral apposition rate (MAR, μm/day), and bone formation rate (BFR/BS, μm3/μm2/day) according to the American Society for Bone and Mineral Research histomorphometry nomenclature committee. 44 Besides, the fluorochrome staining of the newly formed bone was also quantified within the five most-apical implant threads in the augmentation area (Fig. 2) to reflect the peri-implant bone osseointegration and the bone contact to the implant. The single fluorochrome-stained area (%) was calculated and compared as was previously described.43,45–47

The undecalcified sections were further stained with Van Gieson's picric acid-fuchsin. The central sections along the longitudinal axis mesiodistally parallel to each implant were evaluated by using the Olympus light microscope (Olympus BX51) and analyzed histologically and histomorphometrically with an image analysis system (Image-Pro Plus 6.0). The digital photographs of each implant section were recorded to reveal the bone formation surrounding the implant in the augmented sinus, and the measurement consisted of the height of newly formed bone in the augmented area (mm) defined as the distance between the top level of the newly formed bone and the sinus floor48,49 and the percentage of mineralized bone in direct contact to the implant within the five most apical threads in the augmented area (bone-implant contact [BIC], %)50–52 as well as the percentage of material remnant in the whole-sinus augmentation region (material remnant rate [MRR], percentage of original material/percentage of the total surface area, %). 53
Statistical analysis
To check the validity of the parameters distribution, the Kolmogorov–Smirnov method with Lillifors' significance correction was applied, and then all the data were presented with mean±standard deviation. An analysis of the variance test was taken to assess the possible differences in the mineralized surface, MAR, bone formation rate, sLS, BIC, and the height of bone in the augmentation area among the different groups at different time points after the test for homogeneity of variance, while the Kruskal–Wallis nonparametric procedure was adopted to test the RBV and Tb.N, and the Mann–Whitney U test was taken for the MRR. p-Value <0.05 was considered statistically significant. The statistical analysis was performed using SPSS 12.0 statistical analysis software (SPSS, Inc.).
Results
In vitro induction of BMSCs into osteogenic cells
During in vitro culture, the primary-cultured BMSCs reached 70%–80% of confluence around the 14 days postseeding (Fig. 3A). The cells subcultured in the osteogenic induction medium demonstrated osteogenic phenotypes such as positive ALP staining (Fig. 3B) and calcified nodule formation with Von Kossa staining (Fig. 3C). Besides, the OCN expression, a later marker of the osteoblastic marker, was confirmed by immunohistochemistry staining (Fig. 3D, E). Additionally, the RT-PCR analysis demonstrated the transcription of extracellular matrix (ECM) genes Col I, ALP, and OCN (Fig. 3F), indicating that the cultured cells expressed the expected osteoblastic phenotype after amplification in vitro.
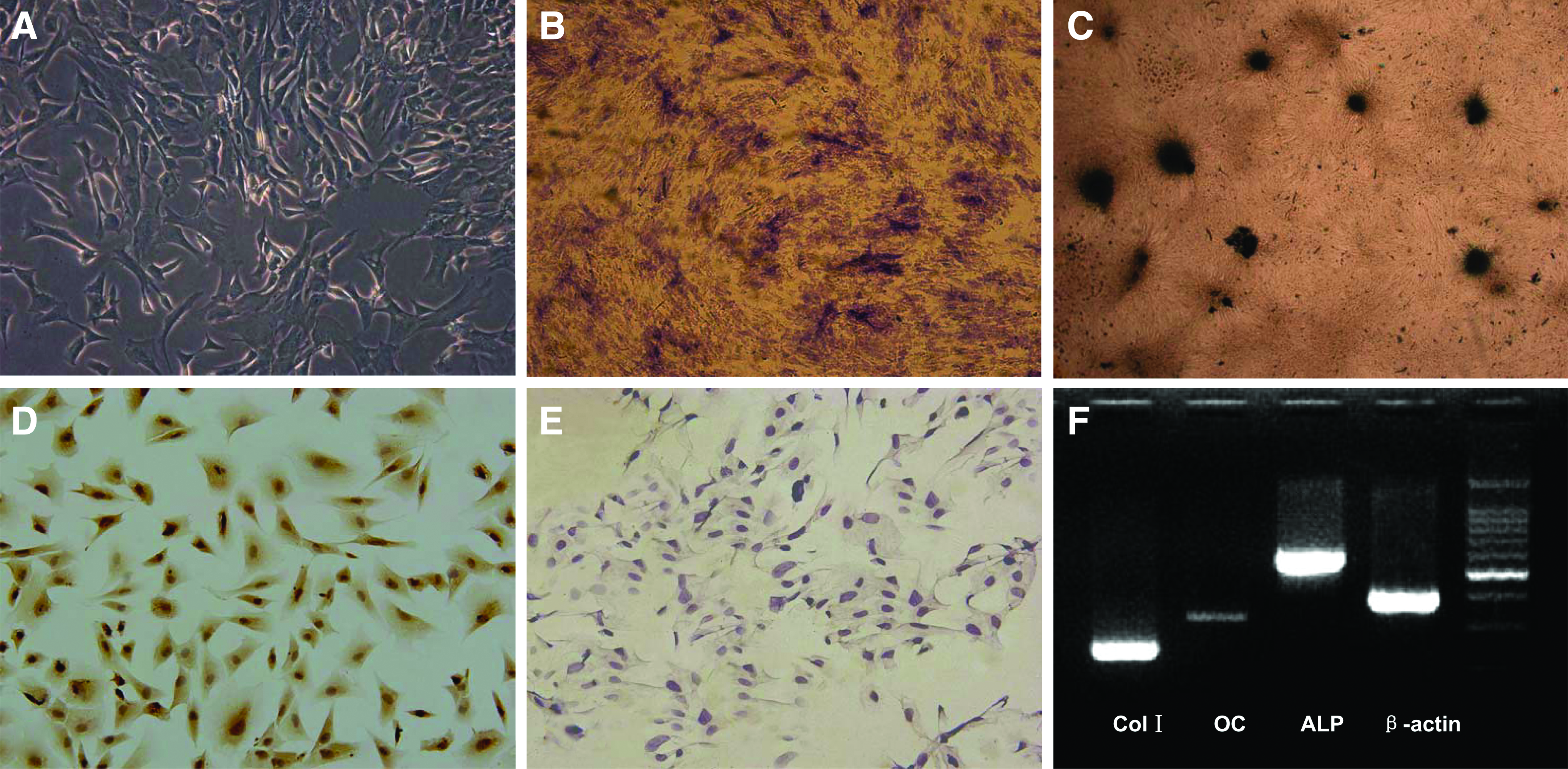
In vitro cultured primary BMSCs
Adhesion and distribution of BMSCs in CPC
CPC scaffolds appeared porous in structure under the SEM, and the average pores were 300–500 μm in size with interconnection pores of 250 μm like the human cancellous bone (Fig. 4A). Four hours after the BMSCs were combined with the material, the cells attached to the surface of the scaffold in vitro. After 24 h, the cells firmly attached and spreaded well on the scaffold surface (Fig. 4B). Four days later, the cells that had spreaded well formed a confluent layer in intimate contact with the material surface (Fig. 4C). These results suggested that the material was of benefit to the initial adhesion and the spreading of BMSCs onto its surface.

Scanning electron microscope photographs of porous CPC.
Clinical observations
All the goats that survived the surgical procedures were healthy during the entire observation period. Eighteen sinus floor elevation procedures were carried out on nine goats. Particularly, no perforation of the sinus membrane occurred, and the wound healing in all cases was uneventful as well.
Micro-CT evaluation
The reconstructed 3D images showed a clear spatial bone formation around the implants in all the groups. The bone that was found grown into the screw-threads filled the augmented sinus space (Fig. 5). The image analysis modules were used to determine the newly formed bone amount around the implants. As shown in Figure 6, the RBV of tissue-engineered bone surrounding the implants remained 54.5%±15.8%, a figure, which was significantly higher than that in either Group B 41.6%±19.7% or Group C 32.1%±5.2% (p<0.05). Tb.N in Group A, Group B, and Group C was 1.08±0.15 1/mm, 0.93±0.20 1/mm, and 0.79±0.17 1/mm, respectively, and there was a significant difference between Group A and Group C (Fig. 6).
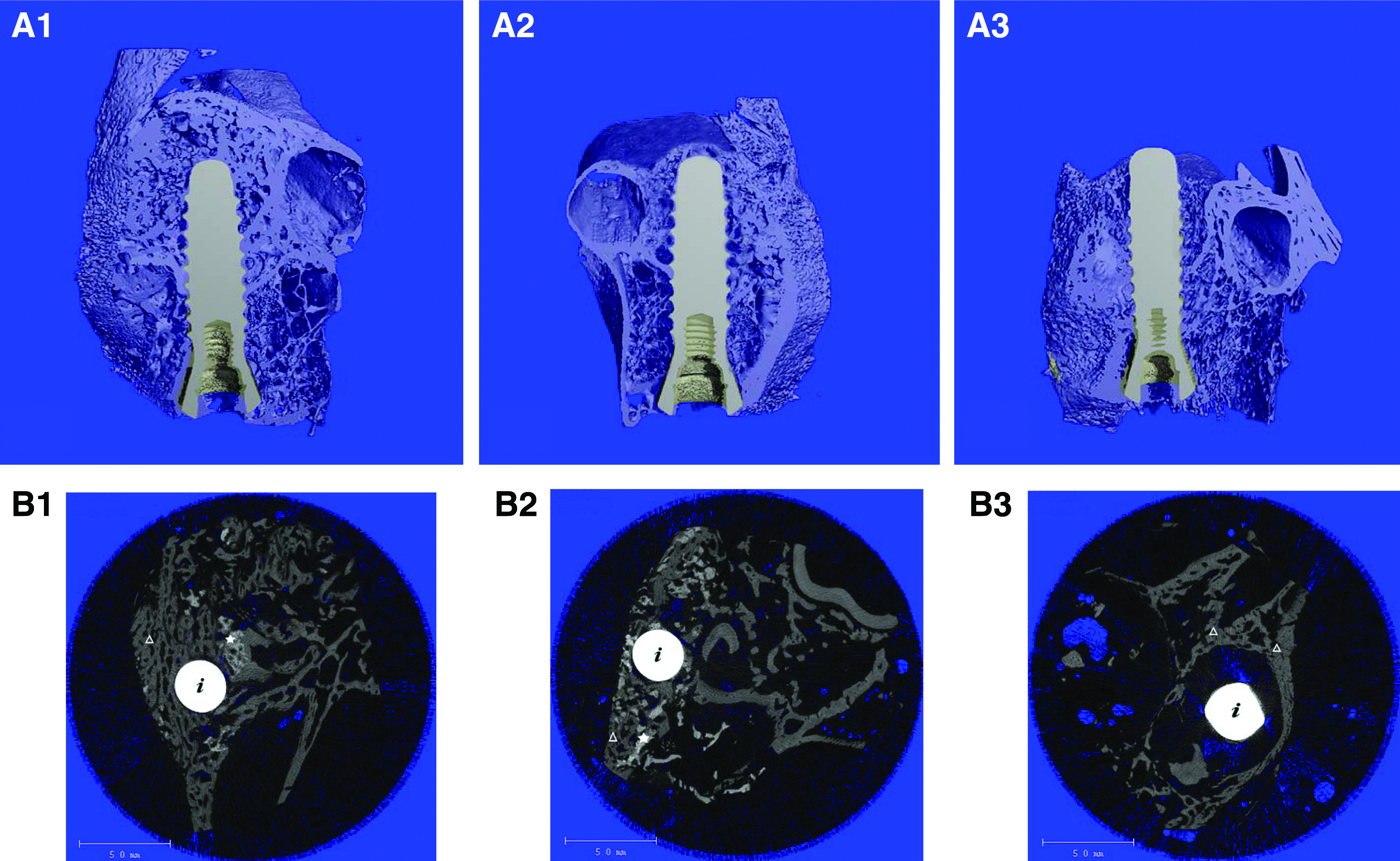
Reconstructed micro-CT three-dimensional images of the surrounding bone tissue with implant
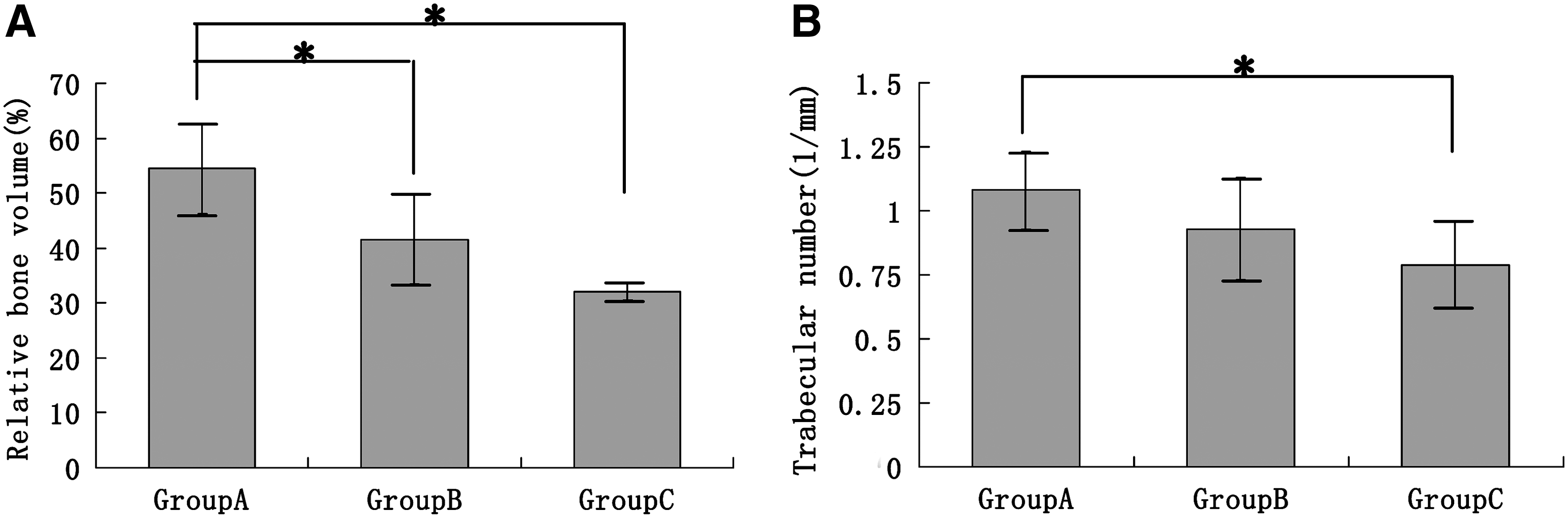
The graph showed the RBV
Fluorochrome-labeling histomorphometric change analyses
Bone histomorphometric indices were evaluated initially by fluorescent labeling measurement and then compared among the different groups (Fig. 7). In Group A (BMSCs/CPC), the values of MS, MAR, and bone formation rate were all higher than their corresponding ones in Group B (CPC) or Group C (autogenous bone) during both 4–8- and 8–12-week postoperation periods (Fig. 8). There were significant statistical differences between Group A and Group B or Group C (p<0.05) with these dynamic parameters.

The images of polychrome sequential fluorescent labeling of undecalcified section under confocal laser scanning microscope. The images represented fluorochromes labeling of tetracycline
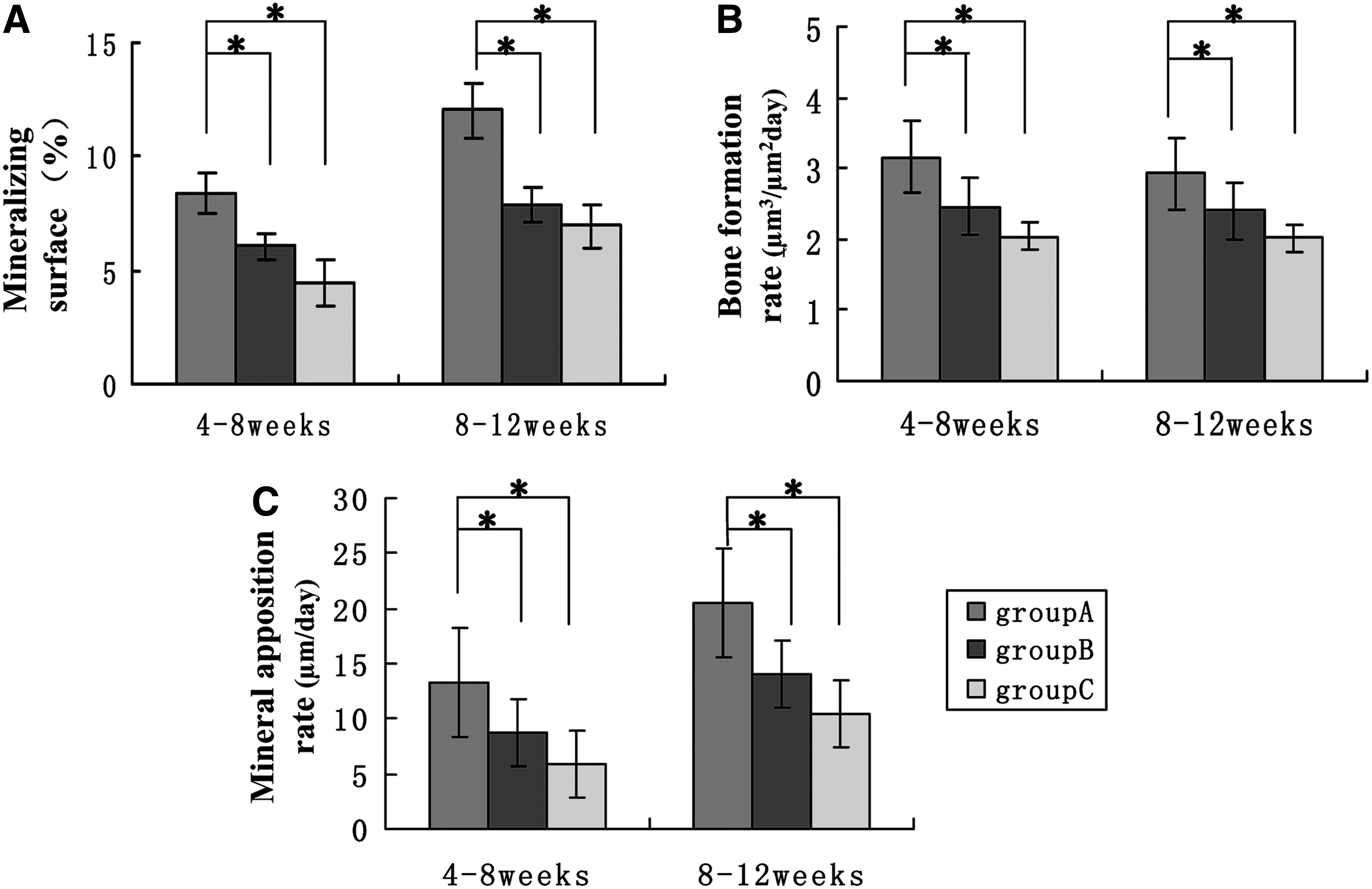
New bone formation and mineralization parameters, including mineralizing surface (%)
What is more, the tetracycline-stained area (%) inside the implant threads in Group A (8.33%±4.53%) was significantly greater than that in Group B (3.23%±1.06%) and Group C (2.41%±2.29%), which was a reflection of the peri-implant osteointegration and the bone contact with the implant 4 weeks after operation. However, the indices were getting closer among three groups 8 and 12 weeks after the operation, which was shown by the red and green fluorescence labeling areas (Table 2). It should be noted that the area occupied by the dental implants showed a red fluorescence under excitation/emission wavelengths of 543/617 nm, but not under other wavelengths. Interestingly, the early tetracycline labeling was found a direct contact with the implant surface directly in Group A, and it was not seen in Group B and Group C.
p<0.05.
TE, tetracycline hydrochloride; AL, alizarin red S; CA, calcein green.
Histological findings
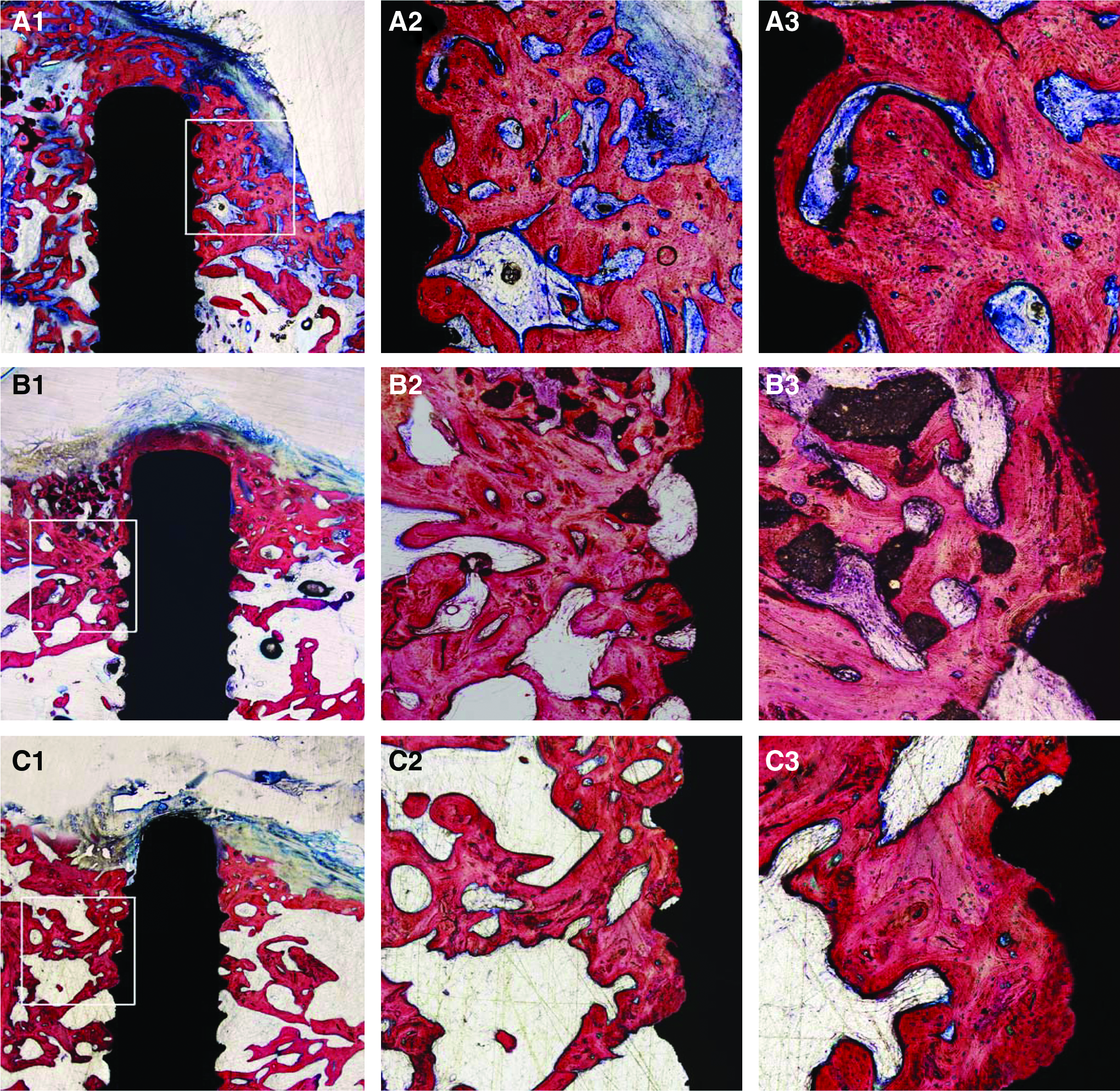
Consistent with micro-CT findings, histological observations showed that 3 months after the surgery, a great amount of new bone with thicker and more trabeculae was found in Group A, with CPC scaffolds almost degraded and absorbed in this group. Inside the implant threads, the new bone contacted well with the implant surface indicated an excellent osseointegration. The implant was also covered apically with the new bone (Fig. 9A). In Group B, new trabecular bone was also seen in the elevated sinus space; however, there were more fibrous tissues inside or between the new bone and the implant (Fig. 9B). The scaffolds were gradually degraded into small granules, and the new bone formation was seen between the remaining degraded material particles or was seen accumulated directly on the surface of these materials. Concerning the autogenous bone group, little slender trabecular bones were found, and the implants were only covered apically with a layer of fibrous connective tissue or sinus membrane (Fig. 9C).
In all these groups, the direct bone deposition occurred on the implant surface. Under the light microscopy, undecalcified sections in Group A demonstrated that the BIC value was higher (35.6%±9.4%) than that in Group B (22.5%±4.3%) and Group C (28.3%±8.0%), and there was a significant difference between Group A and Group B (p<0.05) (Fig. 10A). Similarly, at 3 months postoperation, the maintained elevated height of the sinus floor in Group A, Group B, and Group C was 9.06±2.09 mm, 7.82±1.54 mm, and 6.24±2.41 mm, respectively. Although the elevation height of Group A was more than that in Group B and Group C, there were no statistical significant differences found among the groups (p>0.05) (Fig. 10B). In Group A, the CPC materials were almost resorbed, and the MRR was 6.09%±3.92%, less than that in Group B (15.18%±3.28%), and there was a significant difference between the two groups (p<0.05) (Fig. 10C).
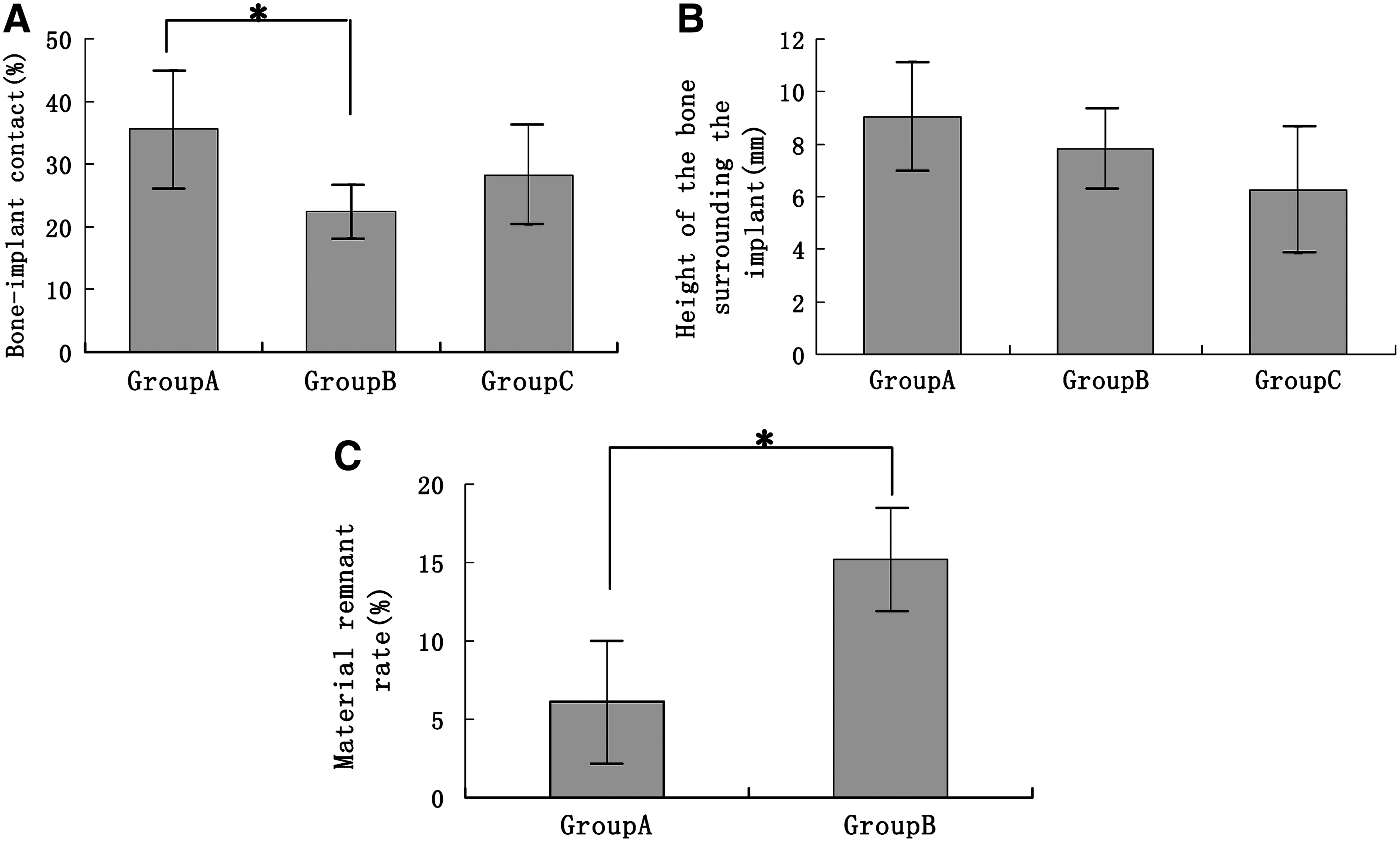
The graphs showed the bone-implant contact values
With a higher magnification, the woven bone was displayed in close vicinity to the implant surface in Group A and Group B. Osteocytes of typical morphology arrayed orderly inside the new bone, while osteoblasts surrounded the newly formed bone (Fig. 11A1). After osteoblasts deposited the matrix, the new bone formation might occur directly on the resorbed surface of CPC (Fig. 11A2). The resorption lacunae with multinucleated cells around the cement surface indicated that CPC degradation could be associated with cell-mediated phagocytosis (Fig. 11B1). Besides, free cement particles were observed in bone marrow cavities, suggesting the existence of passive dissolution (Fig. 11B2).
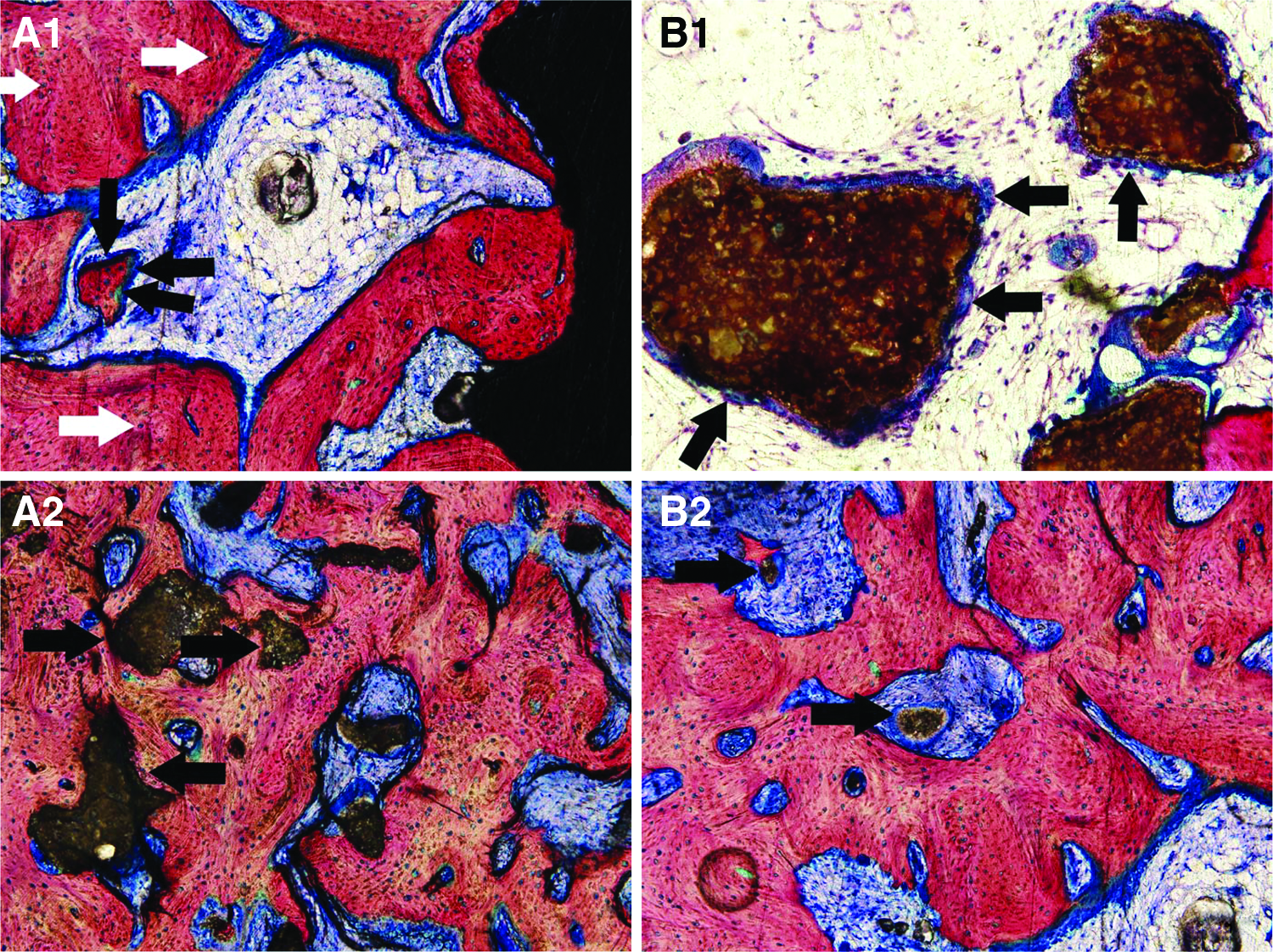
Undecalcified histological sections with Van Gieson's staining: woven bone was close vicinity to the implant surface, with osteoblasts surrounding the bone
Discussion
The inherent advantages of bone tissue engineering have been shown to overcome the shortages of commonly used materials. 50 Among the key elements of tissue engineering, how to prepare the materials with similarity to natural bone in microstructure and composition, and make them possess good osteoconduction properties is of great significance in clinical practice. 54 CPC was developed by Brown and Chow in 1980. Being self-setting and resorbable under physiological conditions, it is involved in tissue metabolism and could promote bone tissue growth after being implanted into a human body. 55 The CPC scaffold in this study was fabricated by a solid-to-solid reaction between calcium phosphate and calcium carbonate at a temperature of 1500°C for several hours.56,57 Unlike CaP cement without sintering, it would not generate obvious pH and ionic changes that may have an adverse effect on BMSCs seeded directly on the surface of CPC. The current study and previous observations have proved that there are no obvious cytotoxity noticed for seeding cells. Besides, the calcium and phosphate ions released from the porous CPC scaffold did not show a negative effect on BMSCs. 58 Also, the augmented sinus and the surrounding area, including sinus membrane, showed no obvious inflammation and necrosis. Thus, CPC scaffolds used in the present study are considered safe for cells and in vivo implantation.
To evaluate the effects of different bone substitutes used in maxillary sinus augmentation, large-animal models were suggested before a clinical application.9,59,60 A goat model was adopted in this study since the maxillary sinus cavity in goat has similar characteristics to that of human beings. They included the size, morphologic anatomy, bone physiology, and structure. Besides, the thickness of goat sinus mucosa has enough consistency to carry out sinus floor elevation surgery. The cortical bone of goat in the lateral wall is as thin as that of edentulous patients, and the antrum is easily reachable by trepanation using a surgical bur. Furthermore, the relationship between the sinus floor and teeth is similar to that in human beings, for the implant placement procedure through the alveolar crest, which maximally represents the clinical situation when maxillary sinus floor elevation with simultaneous dental implantation procedures is requested.32,61 After the maxillary sinus floor elevation surgery, there is continuous air pressure on the scaffold as breathing. Rapid resorption of autologous bone could lead to the reduced elevated height after the surgery. However, many inorganic scaffolds have been suggested to withstand the sinus air pressure and maintain the height of the elevated space.28,62
After the maxillary sinus augmentation surgery, the goats got healed on an even keel. The dynamic morphological observation of confocal laser scanning fluorescence microscopy showed that the percentages of MS/BS (%), MAR (μm/day), and BFR/BS (μm3/μm2/day) measurements in Group A were higher than those of the other two groups (p<0.05) during the whole observation period. Besides, since the status of osteogenesis within threads was the basis of implant-bone osseointegration, 63 the fluorochrome within the threads could well reflect the osteogenesis, suggesting a trend of local implant-bone osseointegration. Consequently, the fluorochrome staining was quantified within the five most apical implant threads in the augmentation area. The tetracycline fluorochrome-stained area (%) between the threads in Group A reflecting the new bone formation and mineralization 4 weeks after surgery was significantly higher than that of Group B and Group C (p<0.05). The increased fluorescence expression detected around the implant surface as well as inside the threads suggested that Group A had a rapid process of mineralization and osteogenesis and an enhanced osseointegration at an early stage.
This can further be confirmed by micro-CT and histomorphometric analysis. For example, it was shown by micro-CT that more new bone was found around the implant in Group A, including the apex of the implant and inside the spaces between the implant threads. Besides, based on the histology findings, CPC scaffolds were almost resorbed, and the MRR was only 6.09%±3.92% in the BMSC/CPC group and 15.18%±3.28% in the CPC group, which really reflected that in the BMSC/CPC group, new bone formation increased as compared with the CPC-alone group; and further, histomorphometric measurements also demonstrated that the percentage of new bone formation around the implant and the BIC rate in Group A were significantly higher than those in others. The maintained average elevated height value of Group A was also higher, even though there were no statistical differences of the elevation height among three groups, which might be due to a higher variation caused by the limited number of goats. All these above-mentioned data showed a better osteogenesis and osseointegration with the BMSC/CPC complex.
Early bone mineralization and a good BIC rate would benefit to the clinical outcome for dental implantation to achieve an early loading and mastication function restoration. This was of great significance particularly to simultaneous implant placement, which could release the patients from a second-stage surgical procedure, and shorten the period of healing. After all, the goal of maxillary sinus augmentation in clinic is to create enough tissues to install and support an implant.
All the above results indicated that the height of the bone surrounding implant and RBVs of autogenous bone were lower than those in Group A or Group B. We believe that free autogenous bone graft could form a new bone by creeping and substitution, but there was a bone reabsorption process. Some clinical information showed 64 that the autogenous bone graft could absorb up to 47% within 6–7 months after maxillary sinus lifting. Watanabe 65 compared the resorption among different sources of autogenous bone. He believed that the iliac bone was more easily absorbed than the chin. Secondly, the bone graft material needed the stimulation of functional load to offset the inherent absorption reaction.1,66 In this study, the submerged implants did not exercise any function load and was thus in lack of physical stimulation. In fact, the absorption of autogenous bone was reported not only in the maxillary sinus lifting but also in the alveolar ridge augmentation and some other parts of bone defect repair.67,68
Bone formation and material degradation occurred at the same time, which was similar to the bone remodeling, as osteoblasts deposited matrix with new bone formation and the resorption lacunae with multinucleated cells occurring directly on the resorbed surface of CPC. 69 Likewise, the histological observations showed that 3 months after the surgery, the CPC scaffolds in Group A were almost degraded, and the MRR of Group A was significantly less than that in Group B. In general, there were two forms of material absorption mechanism: the passive absorption mediated by the dissolution of body fluids and the active absorption by the cell-mediated phagocytosis. In our experiments, both the absorption and degradation mechanisms seemed to be existent. For example, multinucleated giant cell-mediated absorption lacuna could be seen around CPC particles, suggesting the existence of cell-mediated absorption, and the tiny particles could be seen in bone marrow-like cavities, suggesting the existence of passive dissolution. 70 Similarly, Vall also found the existing of passive absorption and active absorption for CPC. In that report, the materials fully contacted with body fluids dissolved and collapsed quickly. Four weeks later, the collapse of the particles could be seen surrounded by multinucleated giant cells. In his view, the presenting of multinucleated giant cells played an important role to balance the bone reconstruction. Our results showed that when CPC scaffolds were seeded with BMSCs, the speed of degradation increased, and that the CPC scaffold remnant rate was less than that in the CPC-alone group. The possible mechanism is that BMSCs play a kick-off role in attracting other cells from the host by releasing biological factors. 71 Alternatively, the creation of a permissive microenvironment such as ECM could be a primary need for migration of multinucleated giant cells. Also, bone-forming cells through the deposition of ECM protein could modify the material surface, thus favoring a multinucleated giant cell adhesion; for example, the osteoblasts might produce and secrete osteopontin to promote adhesion of multinucleated giant cells to the surface of material through their argine–glycine–aspartatic acid (RGD) motif. Furthermore, the stimulated cells such as BMSCs in a bone microenvironment and the factors they produced, such as granulocyte-macrophage colony-stimulating factor, could lead to an enlargement of the multinucleated giant cell pool and of their activity. 72 In the present study, a higher degree of degradation of CPC scaffolds along with an early bone formation and improved BIC is an advantageous characteristic of the CPC/BMSC complex material over the control groups, and such characteristic would be beneficial to the potential dental implant restoration in clinic. Nevertheless, the resorption of CPC and the new bone formation could not be fully completed just within 3 months. It means that a longer observation time is needed.
Conclusion
As was demonstrated by the sequential triad-color fluorescence labeling, micro-CT, and histological and histomorphometric analyses, the tissue-engineered complex of BMSCs and CPC could promote an earlier bone formation and mineralization, and could maximally maintain the height and volume of the augmented maxillary sinus in a large-animal goat model. The average BIC value reflecting the osseointegration was significantly higher in that group. Thus, the tissue-engineered bone of BMSCs/CPC might be an ideal alternative and superior to the autogenous bone or CPC alone for the maxillary sinus floor augmentation and simultaneous implantation. This would be potentially of great significance to achieve an early loading of implant to restore the oral function in clinic.
Footnotes
Acknowledgments
This work was supported by the National Basic Research Program of China (973 Program, 2012CB933600-4); National Natural Science Foundation of China (30400502 and 30772431); Program for New Century Excellent Talents in University (NCET-08-0353); Science and Technology Commission of Shanghai Municipality (08DZ2271100, 0952nm04000, 09JC1411700, and S30206); Shanghai Education Committee (Y0203 and 07SG19); and Shanghai Jiao-Tong University School of Medicine (09XJ21030).
Disclosure Statement
No competing financial interests exist.