
Abstract
The main aim of this study was the comparative evaluation of fibroin scaffolds combined with human stem cells, such as dental pulp stem cells (hDPSCs) and amniotic fluid stem cells (hAFSCs), used to repair critical-size cranial bone defects in immunocompromised rats. Two symmetric full-thickness cranial defects on each parietal region of rats have been replenished with silk fibroin scaffolds with or without preseeded stem cells addressed toward osteogenic lineage in vitro. Animals were euthanized after 4 weeks postoperatively and cranial tissue samples were taken for histological analysis. The presence of human cells in the new-formed bone was confirmed by confocal analysis with an antibody directed to a human mitochondrial protein. Fibroin scaffolds induced mature bone formation and defect correction, with higher bone amount produced by hAFSC-seeded scaffolds. Our findings demonstrated the strong potential of stem cells/fibroin bioengineered constructs for correcting large cranial defects in animal model and is likely a promising approach for the reconstruction of human large skeletal defects in craniofacial surgery.
Introduction
Cranial defects are a relatively common complication that can arise secondary to trauma, surgery, infection, neoplastic, or congenital malformation such as aplasia cutis (AC), and their reconstruction is a challenge in craniofacial surgery. 2 Large cranial defects, which are not rarely observed in AC,3–5 are associated with high morbidity and mortality in the neonatal period and therefore, their treatment is important not only to improve the aesthetic appearance, but mostly important for the reestablishment of the rigid protection of the underlying brain.6,7 Cranial bone losses are today reconstructed by using autologous bone transplants; however, this technique is inadequate for large defects and implicates several risks, including donor site morbidity, graft or flap failure, rejection, or infection.8,9
A critical-size bone defect will not heal spontaneously and this fact makes it suitable for exploring new biomaterials and cell culture–based technologies. 1
It is well understood that ideal bone implants involve cells/scaffold constructs in which target cells are able to expand and develop according to their lineage. The scaffold should provide an optimal three-dimensional (3D) environment and mimic the original extracellular matrix of bone.10–12
Scaffolds have been developed from various classes of materials including synthetic polymers, ceramics, native polymers (hydrogels), and their composites.12–16
According to Meinel et al. 17 the two key requirements in bone tissue engineering are optimal conditions for in vitro expansion of stem cells and suitable scaffolds that provide cell support in such a manner as to enhance osteogenic differentiation followed by functional assembly into bone. Scaffold requirements include biocompatibility, 3D structure, and adequate porosity.18–20
Many researchers have shown the validity of critical-size cranial defect model while employing materials such as poly lactic-co-glycolic acid, 21 octacalcium phosphate precipitated alginate, 22 demineralized bone matrix, 23 composite chitosan/nano-hydroxyapatite, 24 hyaluronic acid–based hydrogel, 25 collagen 2 alone, or in conjunction with mesenchymal stem cells.
The objective of this study was to test the ability of fibroin scaffolds to support the expansion of osteogenic-committed human stem cells transplanted in large cranial defect in parietal region for bone regeneration in vivo.
In fact, our previous study has demonstrated that fibroin scaffold, more than other scaffolds already used in clinical practice, enhanced osteogenic differentiation of dental pulp stem cells (DPSCs) and amniotic fluid stem cells (AFSCs). 26 Fibroin is one of the two proteins composing the silkworm filament. The peculiar aspect of silk fibroin molecule is the presence of two different active sequences, VITTDSDGNE and NINDFDED, recognized by integrin promoting fibroblast growth, that were identified in the N-terminal region of the heavy chain. 27 With different procedures, fibroin can be processed to fabricate films, sponges, nonwoven micro- and nanonets, and solid or injectable gels.28–30
Various potential applications of fibroin for tissue engineering scaffolds have been proposed, due to unique properties that fibroin possesses in terms of biocompatibility and bioactivity.31–34 Kim et al. reported that water-based silk scaffold supports BMSC osteogenic differentiation more efficiently than HFIP-derived silk constructs. 35
Here we compared the osteogenic capability of two sources of stem and progenitor cells obtained from alternative sources, such as dental pulp and amniotic fluid, when seeded in water-based fibroin scaffold. The use of human DPSCs (hDPSCs) or AFSCs is of great interest in bone reconstruction because they can be easily isolated and expanded in culture; moreover, they have shown in vitro and in vivo multipotential plasticity.26,36–40
Materials and Methods
Preparation of fibroin scaffolds
Sponges with randomly distributed pores have been produced by solvent casting particulate leaching starting from fibroin water solution, as follows.
Bombyx mori cocoons purchased from Cooperativa Sociolario were degummed by treating twice with 1.1 g/L Na2CO3 water solution at 98°C for 1 h, washing in deionized water, and air-drying. After degumming, silk was dissolved in 9.3 M (20% w/v) LiBr (Sigma-Aldrich) at 65°C for 2 h. To eliminate LiBr, the solution was then dialyzed in a Slide-A-Lyzer Cassette (Pierce; MWCO3500 Da) against distilled water for 3 days; the fibroin concentration was afterward adjusted to 8% w/v.
Silk fibroin scaffolds were prepared by adding 8 g of granular NaCl (particle size ≈315–425 μm) into 4 mL fibroin solution, and then poured in cylindrical polystyrene plates (3.5 cm in diameter and 1.5 mm in height). The containers were covered, left at room temperature (RT) for 24 h in order to induce gelation, and then immersed in deionized water for 3 days with water change every 6 h in order to remove the salt. 32
All samples were sterilized by Cobalt-60 gamma rays using facilities and control procedures validated in conformity with UNI EN ISO 9001, UNI EN ISO 13485, UNI EN ISO 11137, and GMP by Gammarad Italia S.p.A. with a standard cycle of 25.00 kGy and a dosimeter batch Red Perspex 4034.
Scaffolds' physical characterization
Environmental scanning electron microscopy
The morphology of the silk fibroin scaffolds was evaluated using the Field Emission-Scanning Electron Microscope (FE-SEM) SUPRA 40 (Zeiss Company). Samples were completely dried at RT and gold sputtered before analysis. Images were acquired at 2 kV.
Water content and open porosity
For water absorption evaluation, three specimens of each material were cut in disks (1 cm in diameter), weighed in dry state (Mdry), and then immersed in distilled water for 2 days at RT.
Samples were then blotted dry on filter paper to remove excess water and weighed (Mwet). The percent water content, Wwater referred to the weight of the wet sample, was calculated as:
The open porosity of the SF sponges was quantitatively evaluated on three samples using the principle of liquid displacement. Hexane (n-Hexane; Sigma-Aldrich) was used because it is able to permeate the completely submerged fibroin scaffold without swelling. The scaffold was immersed in a known volume of hexane V1 in a graduate cylinder for 10 min. The volume V2 of the hexane and the sponge was measured. Finally, the sponge was removed and the residual volume of hexane V3 was registered. The total volume of the scaffold can be obtained as follows: V=(V2−V1)+(V1−V3)=V2−V3, where V2−V1 is the volume of the bulk structure of the sponge and V1−V3 is the volume of the hexane retained in the open porosity of the scaffold. The porosity can be calculated from the following equation:
This ratio measures the percentage of the free volume of the scaffold with respect to the total volume of the scaffold.
Mechanical properties
The compressive mechanical properties of silk fibroin sponges were measured using an Instron universal testing machine model 4502, equipped with a 2.5 N load cell. Tests were performed on three disc samples of wet material with a diameter of 12 mm and a height of about 2 mm for fibroin. Elastic moduli were calculated following the ASTM D 1621-04a test method, under displacement control in uniaxial ramp condition at a strain rate of 0.5 mm/min and at RT.
Cell culture and seeding
Supernumerary amniocentesis samples were provided by the Laboratorio di Genetica, Ospedale Santa Maria Nuova. All samples were collected with informed consent of the patients according to Italian law and ethical committee guideline.
AFSCs were isolated as previously described by De Coppi et al. 40 Back-up human amniocentesis cultures were harvested by trypsinization, and subjected to c-Kit immunoselection by MACS technology (Miltenyi Biotec). Human AFSCs (hAFSCs) were subcultured routinely at 1:6 dilution and not allowed to expand beyond the 70% of confluence.
hDPSCs were isolated as previously described by Riccio et al. 41 hAFSCs and hDPSCs were grown in culture medium (α-minimum essential medium supplemented with 10% fetal bovine serum, 2 mM L-glutamine, 100 U/mL penicillin, and 100 μg/mL streptomycin; all from Invitrogen).
Discs with a height of 1.5 mm and diameter of 13 mm were cut from fibroin scaffolds and placed in 24-well tissue culture plates. All the scaffolds were then washed twice with culture medium (1 h for each rinse). Cells were seeded on each scaffold at density of 1500 cell/mm3 and cultured for 24 h with 2 mL of culture medium. After 24 h culture medium was changed with osteogenic medium (culture medium supplemented with 100 nM dexamethasone, 10 mM b-glycerophosphate, and 50 μg/mL ascorbic acid-2-phosphate; all from Sigma-Aldrich). Cells/scaffolds cultures were then maintained in osteogenic medium for 10 days in an incubator at 37°C with 5% CO2, in order to have a cell population committed to osteogenic differentiation but able to proliferate yet. 41 Some samples were stained with 6-CFDA (Sigma-Aldrich) to test the viability of seeded cells.
Surgery and transplantation procedure
To study the bone-forming ability of hAFSCs and hDPSCs on fibroin scaffolds, a critical-size bone defect was obtained by a full-thickness dissection of both the internal and external tables of compact bone and the trabecular diploe constituting the parietal skeletal segment, according to previous studies.2,25 Constructs were then implanted into a critical-size parietal defect up to 4 weeks (Fig. 1 and Table 1). None of the animals died of infection or any other complication.

Cranial defects (5×8 mm) induced in the parietal cranial bones in the rat with
AFSC, amniotic fluid stem cell; DPSC, dental pulp stem cell.
In this study outbred male Sprague-Dawley rats with age ranging between 12 and 14 weeks (Charles River Laboratories) were used. The animals were anesthetized with an intraperitoneal injection (0.2 mL/100 g of body weight) of ketamine hydrochloride (5%). A midline skin incision was performed from the nose-frontal area to the external occipital protuberance.
The skin and underlying tissues, including the periosteum, were reflected laterally to expose the full extent of the calvaria. Two symmetric full-thickness cranial defects of 5×8 mm size were done on each parietal region of 15 animals by a micromotor drill under constant irrigation with sterile physiological solution to prevent overheating of the bone. The underlying dura mater was undisturbed (Fig. 1A).
One scaffold of 5×8×1.5 mm size was implanted into each cranial defect and adapted to fill the entire defect area (Fig. 1B). Each animal received two constructs except the animals of the III group. After the scaffold implantation, the incisions were sutured with prolene 4-0 sutures (Ethicon). Animals were immunocompromised using Cyclosporine A at a dosage of 15 mg/kg body weight (b.w.), administered 4 h before transplantation and then daily for 2 weeks. During the last 2 weeks the daily dosage was reduced gradually up to 6 mg/kg b.w. Four weeks later the rats were sacrificed and the calvarias were rapidly explanted and fixed in 4% paraformaldehyde in phosphate-buffered saline (PBS) for 3 h.
All animal procedures were performed according to the guidelines approved by the Committee of Use and Care of Laboratory Animals of the University of Modena e Reggio Emilia.
Radiography
Explanted calvaria samples were radiographed by a Kodak RVG Digital Radiography Systems.
Histology
Fixed samples were decalcified in 0.5 M EDTA (pH 8.3) and then rinsed in PBS, dehydrated with graded ethanol, diaphanized, and embedded in paraffin. Transversal serial sections (10-μm thick) were cut through the parietal bones containing the implants. Routine hematoxylin/eosin (H&E) staining was performed in order to analyze morphological details. Images of histological samples were obtained by a Zeiss Axiophot microscope equipped with polarizer filters and with a Nikon DS-5Mc CCD color camera.
Confocal microscopy
Histological sections were processed as previously described by Riccio et al. 41 Mouse anti-human mitochondrial protein (Millipore) diluted 1:100 in PBS containing 3% bovine serum albumin (BSA) for 1 h at RT was used as primary antibody (Ab). Secondary Ab was diluted 1:200 in PBS containing 3% BSA (sheep anti-mouse-FITC; Jackson ImmunoResearch). After washing in PBS samples were stained with 1 μg/mL DAPI in H2O for 1 min and then mounted with anti-fading medium (0.21 M DABCO and 90% glycerol in 0.02 M Tris, pH 8.0). Negative controls consisted of samples not incubated with the primary Ab.
Confocal imaging was performed on a Leica TCS SP2 AOBS confocal laser scanning microscope as previously described. 42 The confocal serial sections were processed with ImageJ software to obtain 3D projections. 41 The image rendering was performed by Adobe Photoshop software.
Results
Scaffold characterization: morphology, water content, porosity, and mechanical properties
Scaffold morphology was evaluated by FE-SEM on dry samples. The micrographs of fibroin sponges are shown in Figure 2. Their morphologies are characterized by a high and interconnected porosity but with a different pore diameter range, from 10 to 250 μm; moreover, pores are randomly distributed.
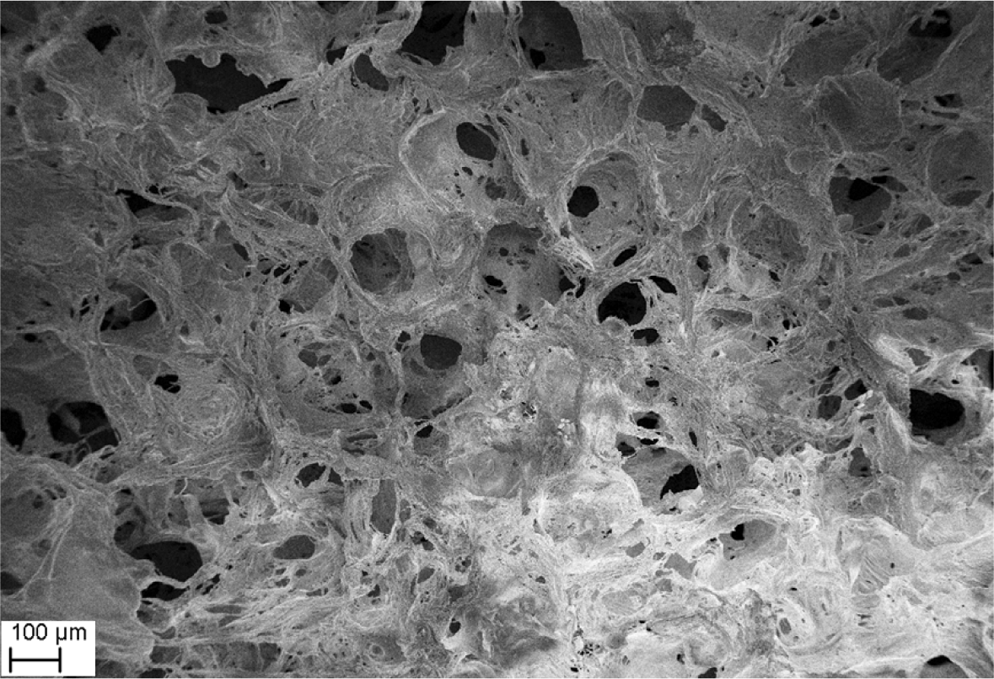
Scanning electron microscopy images of salt-leached silk fibroin scaffolds.
The open porosity as measured by the hexane displacement test was evaluated around 85%±5%, while a water content equal 89% by wt. was measured for fibroin sponges. The data are very close so indicating that most of the water filled the pores and only a negligible amount swelled the solid polymer. Compressive elastic properties of the sponges reflected the effect of material porosity, the absorbed water within the pores, but also the plasticization of the polymer. In the wet state, however, fibroin sponges retained their mechanical consistence, with a measured compressive modulus of 25.69±1.61 kPa.
Radiological analysis
At first we have evaluated the bone healing process at the cranial defects by radiograph 30 days after surgery. Figure 3 shows that the presence of the scaffold alone is able to slightly repair the area removed by the drill. In particular fibroin scaffold restores the bone defect mainly in lateral areas, while no bone repair was observed in the central area of the implant. Overall, the presence of stem cells into collagen and fibroin scaffolds increases radiopacity of the bone defect area that appears similar to the intact bone.
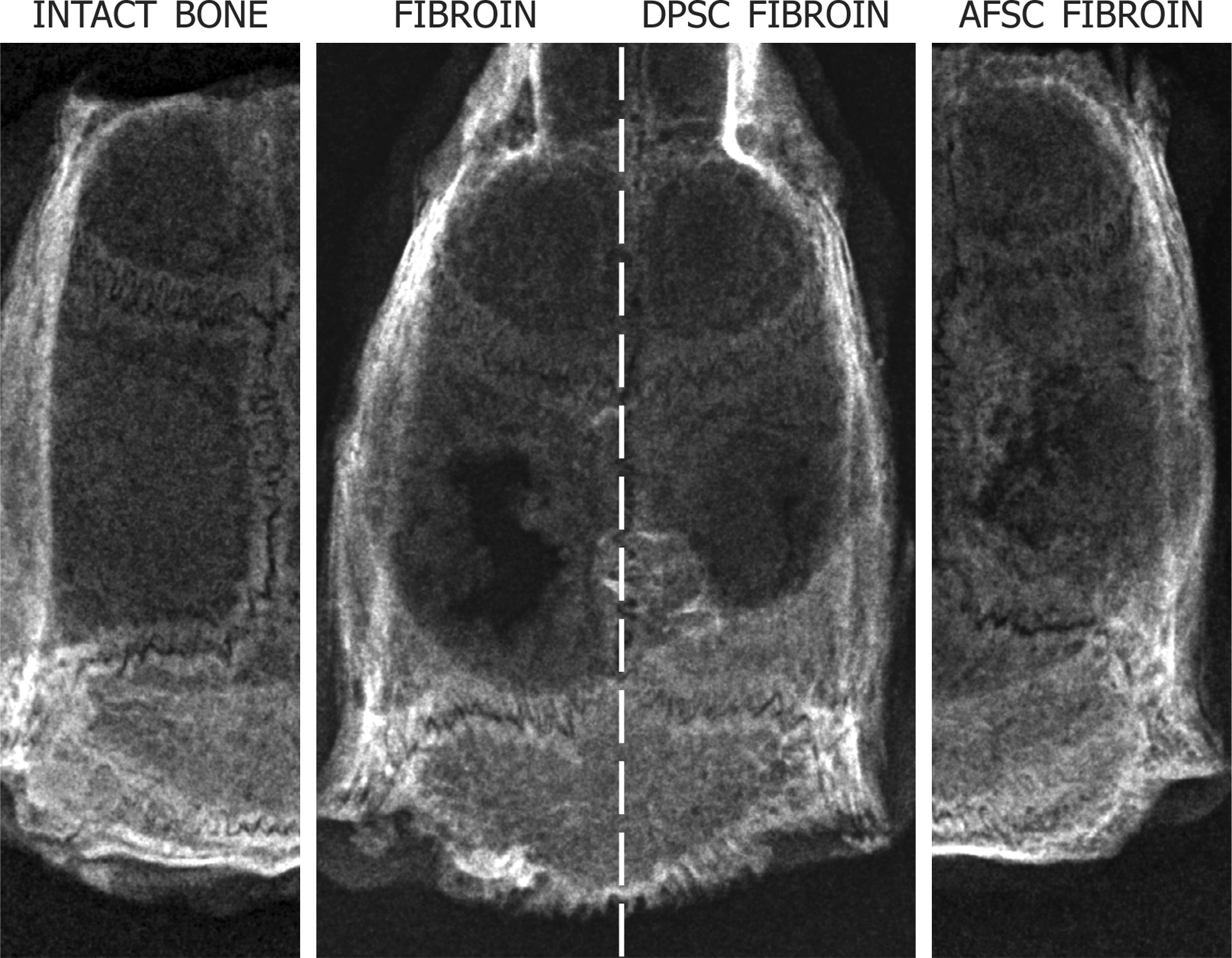
Radiological analysis of rat calvaria dissected 30 days after surgery. Images are representative of the bone healing in the cranial defects of fibroin scaffolds alone and fibroin scaffold seeded with human dental pulp stem cells (hDPSCs) or human amniotic fluid stem cells (hAFSCs).
Histological analysis
To evaluate the parietal bone reconstructing process by histological analysis, serial sections of the parietal bones containing the implants were stained with H&E. Samples were then observed by white field and polarized light microscopy.
Figure 4 shows representative photomicrographs of engineered osseous grafts in vivo. The presence of vessels in the scaffold area indicates that all implanted constructs have been successfully vascularized (Fig. 4D, F, G, K, L).

Comparative histologic analysis of the cranial defect reconstruction by fibroin constructs at 30 days postsurgery. Images show transversal sections carried out through the central area of the implants. Hematoxylin/eosin staining of parietal bone
The untreated critical-size bone defects after 30 days appear filled only by connective tissue and deficient of a significant amount of bone tissue with respect to intact parietal bone (Fig. 4A, B).
Radiograph data for fibroin are confirmed by histological analysis (Fig. 4), since the presence of the scaffold alone causes the formation of small mineralized spots distributed in all the defect area (Fig. 4C–E). This can be an adequate starting step for bone regeneration by stem cells. In fact, the samples containing hDPSCs and hAFSCs even more (Fig. 4F, K) show a complete reconstruction of the internal table of parietal bone and an extensive but incomplete regeneration of the external one. Moreover areas of spongy bone were present between the two tables of compact bone (Fig. 4 F, G, K, L). Polarized light microscopy analysis indicates that new-formed bone presents some areas with lamellar organization compared with preexisting bone characterized by a clear lamellar structure (Fig. 4H, M).
Magnification images highlight area of active bone deposition, as evidenced by the presence of preosteocyte cells partially included in forming lacunae (Fig. 4J) and fibroin remnant islands wrapped by the new mineralized tissue (Fig. 4G, N, O). This indicates a progressive reabsorption of fibroin leaded to ossification process. Fibroin colonized with hAFSCs seems to have a greater regenerative potential with respect to hDPSC/fibroin complex because it forms bone also in scaffold areas distant from dura mater (Fig. 4F, K).
The in vivo data showed that fibroin scaffolds provided hAFSCs and hDPSCs with an optimal microenvironment for their osteogenic differentiation and bone formation.
Confocal analysis
To check whether cells inside the new bone were still from human origin and not from the host, immunofluorescence experiments with anti-human mitochondria Ab were carried out. This Ab recognizes only mitochondrial protein from human origin. In control samples (fibroin alone, Fig. 5A, B) only DAPI staining (red signal) occurs, while human mitochondria (green signal) are not detectable. The autofluorescence phenomenon of fibroin is also evident. Images of stem cell/scaffold implants demonstrate that most of the cells are clearly labeled by anti-human mitochondria Ab (Fig. 5C–G), indicating survival of the donor cells in vivo. In particular, Figure 5C, D, F, and G shows that human cells surround the bone tissue in growth. Furthermore, in Figure 5F it is evident that the new-formed bone tissue wraps modified fibroin islands. Moreover, Figure 5D, E, and G highlights that human cells are included within bone lacunae. These data confirm the central role of human stem cells in bone regeneration after cell/scaffold implant in rat model of large cranial defects.
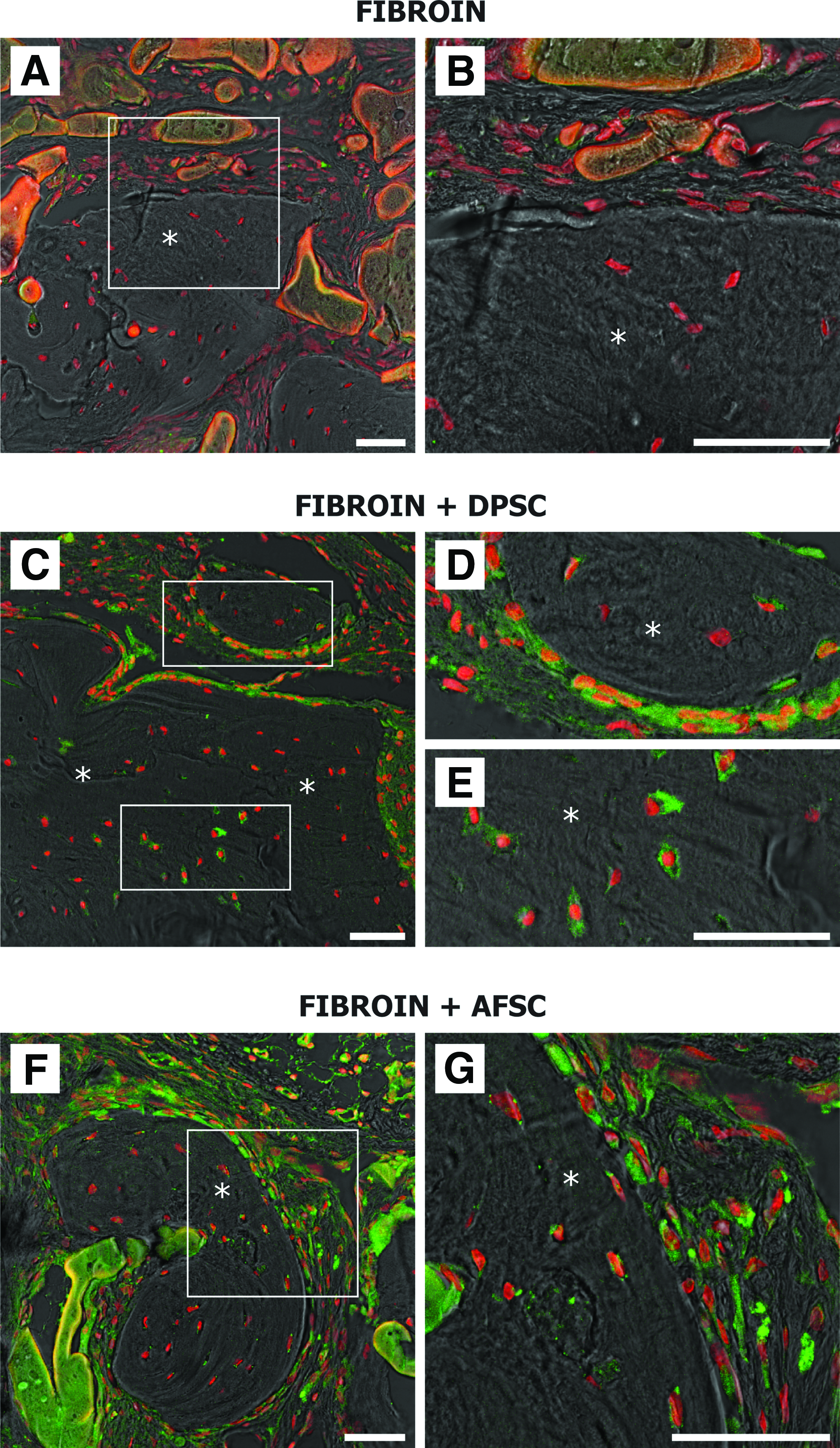
Confocal images of implants obtained 4 weeks after surgery. Double fluorescence signals from DAPI and anti-human mitochondria protein antibody were superimposed to pseudo-phase contrast images.
Discussion
The current study further broadens the future applications of human alternative stem cells in tissue engineering, by including hAFSC or hDPSC/fibroin constructs in repair of bone defects. An engineered osseous graft derived from such an easily accessible cell source, as the amniotic fluid and the dental pulp, would offer several advantages over techniques currently available for the repair of severe bone damages. The engineered approach affords much versatility, as stem cell/scaffold implant can be created into any shape and size, following the anatomical details of the defect.
Our results evaluated fibroin scaffold, seeded with human stem cells (hAFSCs and hDPSCs), in inducing new bone formation in the calvaria critically sized defects.
Radiograph and histological analysis revealed that the highest bone formation occurred in fibroin, seeded with stem cells osteogenically committed, whereas scaffold alone resulted in much lower bone repair. Formation of bone with a very efficient union of the new bone with the margin of the defect area occurred by the use of hDPSC or hAFSC/fibroin constructs. In fact this implant leads to a very homogenous bone formation process, as both parietal tables are in reconstruction, indicating this as a promising approach. The defect was also healed with the use of fibroin only, but the ossification process was evidently incomplete when compared with the use of fibroin plus stem cells. This represents a further evidence of the osteoinductive properties of fibroin.43–45 Results obtained in our recent study on ectopic implants 26 enabled us to identify fibroin scaffold as a promising tool for osteogenic differentiation of human stem cells. The present findings demonstrate that fibroin scaffold promotes human stem cell proliferation and differentiation in parietal bone graft in a rat experimental model.
Fibroin scaffold shows a higher biointegration with rat tissues, since there is a great vascularization and homing of host cells inside the scaffold microenvironment occurs.
Moreover, transplantation of human stem cells in cranial defect model leads to substantial increase in bone formation, and the presence of human cells at 30 days after implantation demonstrates that stem cells, already committed in vitro to osteogenic differentiation, definitively pilot the bone repair in vivo. Confocal analysis shows ossification areas reflecting physiological osteogenesis since a layer of human cells is distributed on the new bone margin, suggesting a bone deposition by osteoblast apposition. At the same time, inside the bone synthesis area, human cells are progressively entrapped in lacunae showing a less intense staining for H-mitochondria protein Ab, indicating a lower metabolic activity, as in osteocytes occurs.
Moreover this study provides additional insight into the potential use of fibroin scaffolds as cell carriers for implantation into skeletal connective tissue defects. Mechanical strength is often a prerequisite for scaffolds destined to bone tissue engineering; however, most of the materials, possessing the needed mechanical forces, are not optimal for cell growth and differentiation. 1 A major advantage of a mechanically stable scaffold is that it contrasts deformation caused by adjacent tissues at the implant site. This deformation can lead to an implant compression within the defect or even displaced beyond the borders of the defect site. 43 Our data indicate that fibroin scaffolds retain high percentage of water maintaining their mechanical properties. Moreover histological analysis demonstrates that fibroin maintains its shape after implant and has been progressively reabsorbed during bone neosynthesis, while remains longer in areas where bone deposition may yet occur, according to data previously reported. 43
Taking together these considerations, fibroin scaffold seems to be an appropriate solution for bone tissue engineering.
Our findings show that an optimal bone defect repair can be obtained colonizing fibroin scaffold with hDPSCs and hAFSCs, both presenting the advantage of easy recruitment without ethical problems.
Autologous transplantation can be performed with both cell types. hAFSCs can be used in neonatal surgery to treat congenital malformation such as the large cranial defects occurring in AC. hDPSCs, available mainly from the puberty onward, can be used to heal pathologies occurring in the adult life.
In respect to other adult stem cell sources, such as adipose-derived stem cells, amniotic fluid and dental pulp are tissues largely available from routine medical practice and therefore useful to be collected in stem cell banks in order to be employed in both autologous and allogenic transplantations. In fact, both the cell types present major histocompatibility complex (MHC) class I but lack MHC II class molecules and seem to have immunosuppressive activity.40,46–48 This aspect could have potential clinical applications in allogenic stem cell transplantation, particularly for calcified tissue reconstruction. 48
All these data indicate that the progenitor cell association with an appropriate scaffold represents an optimal tool in many aspects of bone regeneration and tissue engineering applications.
Footnotes
Acknowledgments
The authors thank Dr. Gianfranco Croci (Laboratorio di Genetica, Ospedale Santa Maria Nuova, Viale Risorgimento, 80-42100 Reggio Emilia, Italy) for providing sample of amniotic fluid cells. This work was supported by grants from “Progetto Strategico per lo sviluppo nella sede di Reggio Emilia della Facoltà di Medicina e Chirurgia” Prot: 2010 0007725, Arcispedale S. Maria Nuova di Reggio Emilia and MIUR FIRB Accordi di Programma 2010 Prot: RBAP10Z7FS. In this study, the confocal microscope Leica TCS SP2 of the C.I.G.S. (Centro Interdipartimentale Grandi Strumenti) of University of Modena and Reggio Emilia was utilized.
Disclosure Statement
No competing financial interests exist.