
Abstract
Porous three-dimensional tyrosine-derived polycarbonate (TyrPC) scaffolds with a bimodal pore distribution were fabricated to mimic bone architecture using a combination of salt-leaching and phase separation techniques. TyrPC scaffolds degraded in register with bone regeneration during the 6-week study period and compressive moduli of the scaffolds were maintained >0.5 MPa at 6 weeks of incubation in PBS at 37°C. The TyrPC scaffolds either unsupplemented or supplemented with recombinant human bone morphogenetic protein-2 (rhBMP-2) were implanted in a rabbit calvarial critical-sized defect (CSD) model and the TyrPC scaffolds treated with rhBMP-2 or TyrPC coated with calcium phosphate scaffold alone promoted bone regeneration in a rabbit calvarial CSD at 6 weeks postimplantation. A synthetic TyrPC polymeric scaffold either without a biological supplement or with a minimal dose of rhBMP-2 induced bone regeneration comparable to a commercially available bone graft substitute in a nonrodent CSD animal model.
Introduction
BGS must fulfill specific biological and biomechanical criteria that include functioning as a template for cell attachment, amplification, and differentiation with subsequent expression of extracellular matrix proteins that will mineralize. 3 Moreover, the bone substitute must include performance properties of biocompatibility, biodegradability, osteoconductivity, osteoinductivity, as well as biomechanical functionality. 4 A porous micro- and macroarchitecture must be exploited to enable angiogenesis, cell migration and viability, and osteoconduction.3,5 In addition, the bone substitute must have adequate mechanical strength during bone healing, including nonload-bearing zones of the cranium where cyclic stresses occur due to dural pulsation. 6
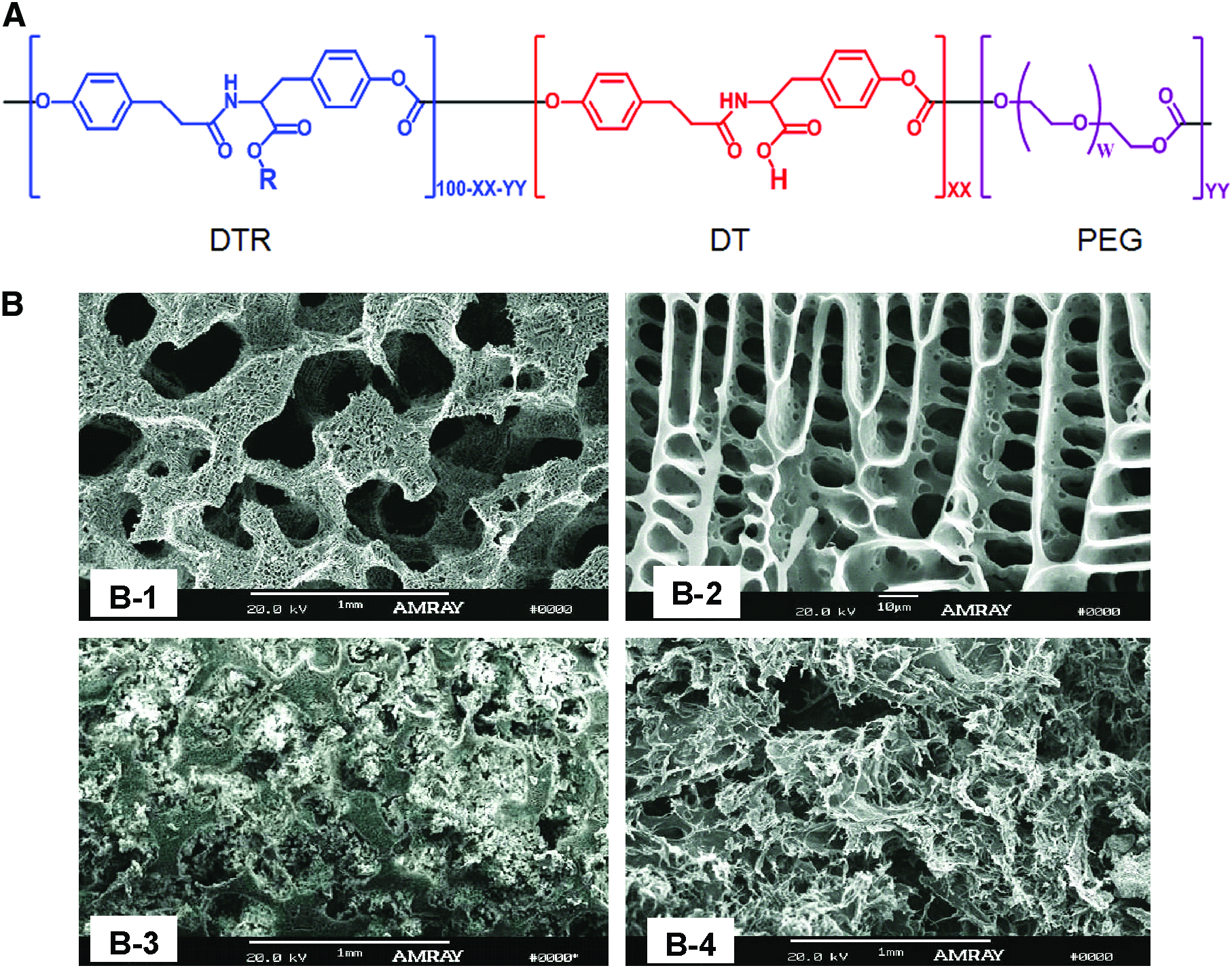
A new class of tyrosine-derived polycarbonates (TyrPCs) has been developed that is composed of desaminotyrosyl-tyrosine alkyl ester (DTR), desaminotyrosyl-tyrosine (DT), and poly(ethylene glycol) (PEG). By combining these three monomers, the resulting terpolymers can provide precise control of physical, chemical, biomechanical, and biological properties requisite for bone regeneration.7,8
Polymers in combination with calcium phosphates (CPs) have been used as grafts for bone repair to improve bone–scaffold integration, to enhance bone regeneration by promoting the deposition of hydroxyapatite in vivo, and to enhance adhesion and differentiation of osteoprogenitor cells.9–12 CPs have been coated on the polymer surface or have been prepared as polymer-CP composites. Polymer surfaces can be coated by immersion in solutions resembling body fluids, such as simulated body fluid,13,14 or solutions of calcium and phosphate. 15
In this study, we report in vivo assays to verify that TyrPC properties can be engineered to match the bone regeneration cascade using a rabbit calvarial critical-sized defect (CSD) model. The objective of the rabbit calvarial CSD model studies was to determine the biocompatibility and bone regeneration potential of TyrPC-based scaffolds either unsupplemented or supplemented with recombinant human bone morphogenetic protein-2 (rhBMP-2). The hypothesis for the study was that the TyrPC-based scaffolds will be biocompatible, biodegrade after 6 weeks, and regenerate bone in the rabbit calvarial CSD. To test the hypothesis, in vivo tissue responses to the three-dimensional (3D) TyrPC-based scaffolds were assessed and bone regeneration was determined in a standardized CSD rabbit calvarial model.
Materials and Methods
Scaffold preparation
TyrPCs were fabricated into 3D porous scaffolds as described previously. 7 Pore architecture of sputter coated scaffolds was determined using a scanning electron microscope (Amray 1830I, 20 kV). TyrPC coated with CP (TyrPC+CP) scaffolds were prepared by immersing the TyrPC scaffolds in 1 M CaCl2 solution followed by addition of 0.96 M K2HPO4 solution. The% Ca (by weight) that was incorporated was determined by elemental analysis using inductively coupled plasma optical emission spectrometry (Intertek). Scaffolds were sterilized using ethylene oxide (AN74i; Andersen Products) and sterility was verified using a Steritest® (AN-80; Andersen Products).
In vitro physical properties
The degradation of TyrPC scaffolds was evaluated by incubating TyrPC scaffolds in PBS at 37°C. 7 Scaffolds and aliquots of the buffer (n=3) were collected at predetermined intervals up to 8 weeks. The scaffolds were characterized by GPC for molecular weight loss relative to polystyrene standards and the aliquots by high-performance liquid chromatography for mass loss relative to monomer calibration curve. 7 Molecular weights and weights were normalized with respect to zero-time measurements. Mechanical properties of PBS-incubated scaffolds (n=3), with thickness of around 2.5 mm and diameter of around 15 mm, were evaluated at predetermined time points and were measured in wet state in PBS at 37°C using ReNew MTS Systems. The tests were run at 0.5 mm/min and the data were collected and analyzed using TestWorks 4 (Ver. 4.11 C; MTS Systems).
Prior to incorporation of rhBMP-2 solution, the scaffolds were conditioned for 1 h with PBS to reduce hydrophobicity. rhBMP-2 (Wyeth) was dissolved in deionized water (1 mg/mL) and added to each scaffold dropwise. The scaffolds were air-dried overnight. The samples were placed into the tissue culture media supplemented with 100 U/mL penicillin, 100 μg/mL streptomycin, and 1% bovine serum albumin and incubated at 37°C and 5% CO2. The releasate was collected each day, stored at −80°C, and replaced with fresh media. The rhBMP-2 released from the scaffolds was measured using an ELISA kit (R&D Systems).
Rabbit calvarial surgery
A BGS (20% bovine type-I collagen and 80% tricalcium phosphate)—which is a Food and Drug Agency (FDA)–approved, commercially available bone void filler—was used as a control for in vivo studies. Six types of scaffolds were used: a BGS without rhBMP-2 (group 1, n=4), TyrPC without rhBMP-2 (group 2, n=4), TyrPC+CP without rhBMP-2 (group 3, n=5), BGS with rhBMP-2 (50 μg) (group 4, n=6), TyrPC with rhBMP-2 (group 5, n=4), and TyrPC+CP with rhBMP-2 (group 6, n=5).
Skeletally mature New Zealand White male rabbits weighing 3.5–4.5 kg were used for the study. A CSD (15-mm diameter) in the calvaria was carefully prepared to avoid dural tear and was located between the supraorbital ridge and across the midsagittal suture in the parietal bones using a 15-mm-diameter surgical trephine with copious physiological saline for irrigation. 7 Each scaffold was gently inserted into the single 15-mm-diameter craniotomy and soft tissues were closed in layers with resorbable 4-0 Dexon sutures. Skin was closed with surgical staples. At 6 weeks postimplantation, rabbits were euthanized humanely according to the National Institutes of Health (NIH) and University guidelines with an intravenous overdose of barbiturate (200 mg/kg body weight). Harvested tissues were placed immediately into individual labeled vials of formalin at a 1:10× volume (tissue:fixative) and prepared for microcomputed tomography (μCT) and histological analysis.
Microcomputed tomography
Each specimen was placed on the scanning platform of a GE eXplore Locus μCT (GE Healthcare) and 360 X-ray projections were collected (80 kVp; 500 mA; 26 min total scan time). Projection images were preprocessed and reconstructed into 3D volumes (20 μm resolution) on a 4PC reconstruction cluster using a modified tent-FDK cone beam algorithm (GE reconstruction software). The 3D data were processed and rendered (isosurface/maximum intensity projections) using MicroView (GE Healthcare).
Histology
The recipient bone and implants (referred to collectively as specimens) were dehydrated in ascending grades of ethanol, cleared in xylene at 4°C to minimize implant solvation during the processing, and embedded in poly(methyl methacrylate). The specimens were cut and ground to 30-μm-thick sections with an Exakt diamond band saw and MicroGrinder (Exakt Technologies). The slides were prepared and stained with Sanderson's Rapid Bone Stain and counterstained with van Gieson's picrofuchsin, which resulted in soft tissue staining blue and bone staining pink/red.
Quantification of new bone formation
Trabecular bone volume in a defect site was calculated using the image analysis (MicroView; GE Healthcare) of μCT data. Briefly, after 3D reconstruction, each volume was scaled to Hounsfield Units (HU) using a calibration phantom containing air and water (phantom plastic); a plug within the phantom containing hydroxyapatite was used as a bone mimic for bone mineral/density calculations. Volumes were imported into Matlab (R2009b; Mathworks) for automated batch analysis. Briefly, a fixed cylindrical volume of interest (14-mm diameter, 5-mm height) was applied to each volume. Since each volume was calibrated using a fixed standard, CP, cortical bone, trabecular/woven bone, and scaffold content were determined using predefined Hounsfield Unit thresholds (>3000, 2000–3000, 750–2000, and 300–750, respectively). To account for partial volume and beam hardening artifacts around CP granules, CP regions were morphologically “dilated” by five voxels and subtracted from the trabecular/woven bone mask.
New bone formation within the defect was also measured histomorphometrically using an image analysis program (Optimas version 6.5; Media Cybernetics). Briefly, the defect area (region of interest) including new bone area on each histology section was determined on each histology section at 1.5×. The areas of new bone were determined by capturing each region based on predetermined color thresholds. The percentage of new bone area was obtained by dividing the bone area by whole defect area.
Statistics
All data were reported as a mean±standard deviation and tested for significance (p<0.05) using single-factor analysis of variance. Individual differences among the groups were determined using a post hoc multiple comparison test (p≤0.05).
Results
3D scaffold preparation
Scaffolds were prepared using TyrPC terpolymers containing DTR, DT, and PEG building blocks (Fig. 1A). The 3D porous (porosity: 85%) scaffolds were produced using a combination of solvent casting, porogen leaching, and phase separation techniques that produced bone tissue–like pore structures. 7 A bimodal pore distribution with interconnected macropores (>200 μm) and oriented micropores (<20 μm) surrounding the macropores was observed for TyrPC (Fig. 1B-1, B-2) and TyrPC+CP (Fig. 1B-3) scaffolds. The pore architecture of TyrPC-based materials was compared with the FDA-cleared bone void filler (i.e., BGS) (Fig. 1B-4), which revealed random, nonoriented pores.
In vitro characterization
After 8 weeks of incubation in PBS at 37°C, molecular weight retention of TyrPC and TyrPC+CP was less than 40%, with TyrPC degrading faster than TyrPC+CP (Fig. 2A). Consequently, compressive moduli and yield strength of TyrPC+CP were greater than those of TyrPC throughout the test period up to 8 weeks (Fig. 2B, C). It is noteworthy that while the molecular weight of TyrPC decreased to 20% of its original value, the compressive modulus at 6 weeks was greater than 0.5 MPa.
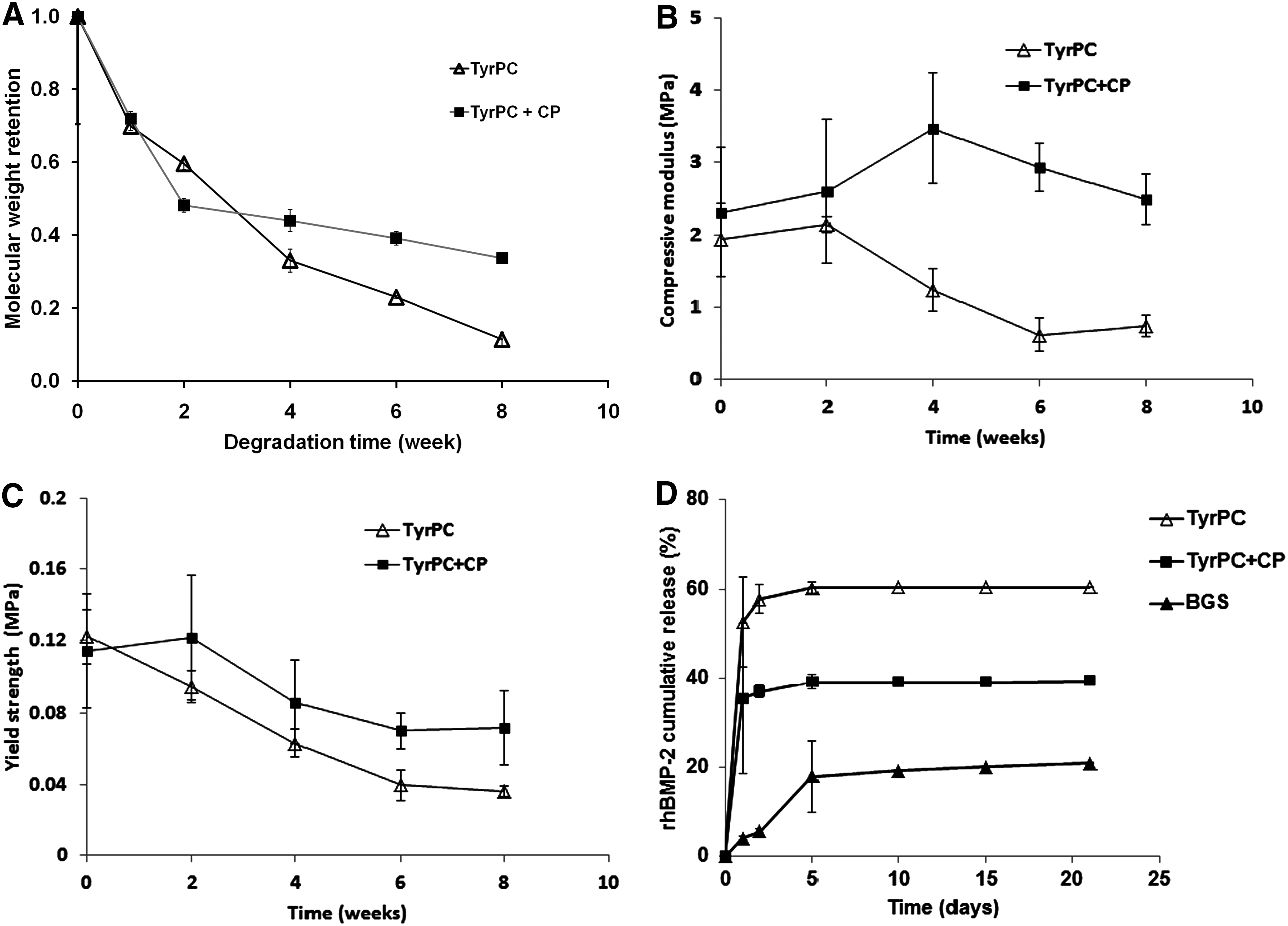
All scaffolds demonstrated a typical biphasic rhBMP-2 release profiles, an initial burst release up to 5 days (∼90% total release) followed by slow release up to 21 days (Fig. 2D). The initial cumulative release of rhBMP-2 from the TyrPC scaffold was greatest among the tested scaffolds, followed by TyrPC+CP, and the predicate device scaffold had the least amount of cumulative rhBMP-2 release.
Bone regeneration in CSD rabbit calvaria
The surgical properties of TyrPC and TyrPC+CP scaffolds were better than the clinical BGSs. The BGS scaffold was friable and difficult to handle during insertion into the defects. In contrast, TyrPC and TyrPC+CP materials were sturdy; if deformed, they “rebounded” and upon surgical implantation, they imbibed blood. This property is significant in that the clotted blood contains stimulatory, influential osteogenic and angiogenic cues. Moreover, at necropsy (6 weeks postimplantation), all the recipient sites implanted with tested materials displayed normal-appearing tissues with neither swelling nor tissue necrosis (Fig. 3). In addition, there were no clinical complications (e.g., infection, wound breakdown, or exudate) detected at the implant sites.

Implant images before and after surgery using the critical-sized defect (CSD) (15-mm diameter) rabbit calvarial model. All test implants fit snugly into the craniotomy sites. There were no adverse tissue observations at necropsy (yellow dotted circle showed the implant site). Color images available online at www.liebertonline.com/tea
Two-dimensional sections (coronal and transverse planes) of μCT images of the calvarial specimens revealed that without rhBMP-2, the BGS-treated and TyrPC-treated CSDs had marginal new bone formation. In distinction, rhBMP-2–supplemented scaffolds (50 μg rhBMP-2/scaffold) had significant bone regeneration at 6 weeks (Fig. 4A). μCT images of the BGS without rhBMP-2 suggested bone regeneration in isolated zones at the periphery of the scaffolds. In addition, μCT revealed that BGS fragments were still present in the recipient CSD.
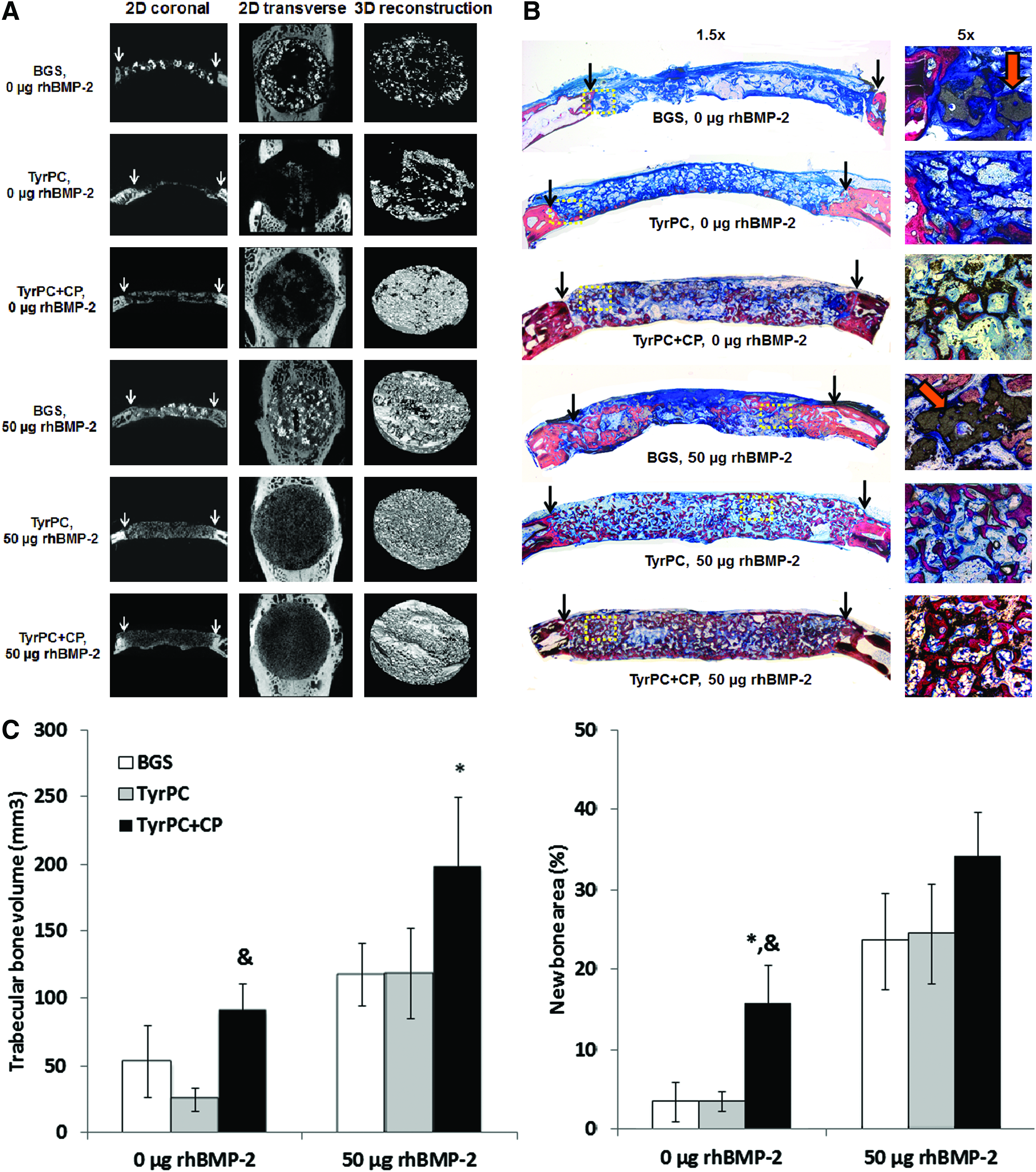
The coronal plane of the histological sections was stained with Sanderson's Rapid Bone Stain and counterstained with van Gieson's picrofuchsin (panels on the left at 1.5× magnification; inset: yellow dotted lines at 5× magnification on the right) (Fig. 4B). There appeared to be no adverse tissue responses such as inflammatory reactions (e.g., macrophages or foreign body giant cells) or osteolysis in the defect area. The histology images suggested bone formation along the dural surface and modest osteoconduction in the TyrPC scaffolds. In contrast to TyrPC, there was substantial bone formation throughout TyrPC+CP scaffolds. There was sparse bone formation in the BGS scaffolds without rhBMP-2. Further histological examination suggested that the rhBMP-2–treated scaffolds had robust trabecular bone formation. It is noteworthy that BGS (orange arrows) scaffold fragments were still present after 6 weeks, regardless of rhBMP-2 supplementation. In distinction, TyrPC-based scaffolds were almost completely degraded by 6 weeks.
The μCT data suggested that in general, rhBMP-2–treated scaffolds had significantly greater trabecular bone volume than their counterpart scaffolds without rhBMP-2 (Fig. 4C). There were no significant differences in trabecular bone volume between BGS and TyrPC scaffolds without rhBMP-2. TyrPC+CP scaffolds without rhBMP-2 had more trabecular bone volume than TyrPC. Among the rhBMP-2–treated scaffolds, there was a significant difference in trabecular bone volume between TyrPC+CP and BGS treatment groups. Histomorphometric data (new bone area) mirrored μCT data. The results suggested that without rhBMP-2 treatment, TyrPC+CP had more bone area compared with TyrPC and BGS. The data also validated μCT analysis in that TyrPC and TyrPC+CP containing 50 μg rhBMP-2 had significantly greater bone area than the scaffolds without rhBMP-2.
Overall, the TyrPC implants were biocompatible and histology and histomorphometry data supported μCT data for new bone formation at 6 weeks postimplantation. Furthermore, there were no significant differences in quantitative analysis data (such as trabecular bone volume and bone area) between TyrPC+CP alone (90.8±19.8 mm3 and 15.8%±4.7% for trabecular bone volume and new bone area, respectively) and BGS with rhBMP-2 (117.4±23.4 mm3 and 23.6%±6.0% for trabecular bone volume and new bone area, respectively). Although further investigation maybe needed to validate these in vivo data, this striking outcome underscores that TyrPC+CP without rhBMP-2 promoted similar new bone formation compared with BGS supplemented with rhBMP-2.
Discussion
Despite vigorous efforts to mimic physical and biological properties of bone in the design of novel biomaterials for bone tissue engineering, contemporary biomimetic scaffolds have failed to match stringent clinical performance criteria for bone regeneration.16,17 Some materials have produced compelling bone regeneration outcome in rodent models; however, there is little fidelity between rodent and human bone physiology. 18 To improve suboptimal properties of contemporary synthetic bone substitute scaffolds, a family of TyrPC scaffolds has been developed. It is noteworthy that in contrast to poly(α-esters), the TyrPCs have consistently produced superior biocompatibility.19,20
Previous data have reported that poly(DTE carbonate) was biocompatible and osteoconductive in the distal femur and proximal tibia of rabbits,21,22 a canine bone chamber model, 19 the calvaria of a rabbit non-CSD, 23 and rabbit mandibular defects.24,25 However, despite the reported osteoconductive outcomes from those studies, bone regeneration was limited. These observations may have been caused by a mismatch between the poly(DTE carbonate) degradation to new bone formation. To mitigate against this mismatch, modification of the polymer backbone was achieved by incorporating DT and PEG. By varying the composition of TyrPC terpolymers, polymer properties such as polymer degradation can be tailored. 7 Furthermore, the presence of free carboxylic acid groups enables chelation of calcium ions, which in turn may act as nucleation sites for the formation of a hydroxyapatite layer, thus promoting new bone formation.22,26 Adding CP throughout the TyrPC scaffolds, the treatment group TyrPC+CP may improve host–scaffold integration, enhance the rate and quality of bone formed during regeneration, and may accelerate bone regeneration.9,10,27
In this study, we report a newly designed TyrPC platform. The terpolymer-designed TyrPC bone substitute promoted impressive new bone formation in a challenging rabbit CSD calvarial model at 6 weeks. Chemically, TyrPC terpolymers are composed of DTR, DT, and PEG. The DTR and DT provide mechanical strength and PEG enhances physical and biological properties (Fig. 1A). The presence of DT and PEG in the polymer backbone accelerates degradation rate. 7 Furthermore, the pore size range (>200 μm) and architecture of the TyrPC scaffolds resembles trabecular bone and supports osteoconduction (Fig. 1B). In addition, micropores (<20 μm) aligned around the macropores may benefit angiogenesis and osteoconduction by increasing surface area, thus enhancing endogenous protein adsorption, exogenous protein retention, as well as ion exchange for apatitic formation. 3
The in vitro characterization assays of the physical properties of TyrPC scaffolds revealed that polymer degradation was >70% at 6 weeks in PBS at 37°C (Fig. 2A). Moreover, the compressive modulus of the porous TyrPC scaffolds was >0.5 MPa after 8 weeks of degradation at 37°C (Fig. 2B), which is a target performance value for the BGS.6,28
In vivo resorption appeared to be almost complete by 6 weeks and likely was a consequence of enzymatic and/or cellular interactions. 29 Furthermore, biodegradability of TyrPC-based scaffolds appeared to match the bone formation rate (∼2 μm/day). 30 In distinction, the clinical predicate (i.e., BGS) had significant bulk remaining after 6 weeks (Fig. 4B). We posit that this observation may be due to a slower resorption rate of the tricalcium phosphate of the BGS in contrast to the TyrPC-based implants.
Although bone healing speed between rabbit and human is quite different, rabbit sigma correlates with the temporal groups we selected. In addition, a rabbit model provides a sequential, systematic approach to assess the biomaterial in a clinically relevant preclinical model. 18 A precise match between the biodegradation of the biomaterial eventually will have to be made in the appropriately designed clinical study. Nevertheless, the literature teaches and biology underscores the fact that biodegradation in the rabbit preclinical model is a compelling antecedent to the clinical model and, further, can be exploited to predict accurately the likely outcome in the clinical condition.
The in vivo outcome data revealed that TyrPC alone had marginal bone formation and may lack innate osteogenic capacity to regenerate bone in a rabbit calvarial CSD model. However, when TyrPC was supplemented with either rhBMP-2 or CP, new bone formation in the defects significantly increased (Fig. 4C). Studies using the rabbit CSD calvarial model have reported rhBMP-2 dosing up to 290 μg/defect site delivered with a collagen sponge 31 and coral. 32 In this study, at 6 weeks we achieved remarkable bone regeneration in a stringent rabbit CSD model with either TyrPC+CP unsupplemented with rhBMP-2 or in conjunction with 50 μg rhBMP-2/defect site. This is a greater than 20% decrease of the reported doses and could have compelling clinical implications for rhBMP-2 devices. A possible explanation for the performance superiority of TyrPC-based scaffolds may be attributable to chemical and physical properties that promoted cell attachment, amplification and differentiation to an osteogenic phenotype, and degradation in register with bone regeneration, thus improving regenerative outcome with a 50 μg dose versus traditional rhBMP-2 dosing that are five times greater. 8
The minimal dose of rhBMP-2 supplementation of TyrPC scaffolds significantly enhanced bone formation. There is a profound patient benefit when a delivery system (i.e., bone biomimetic substitute) provides a physiological, calibrated dose of rhBMP-2. A localized and physiological dose for therapeutic effect is safer and more economical than a supraphysiological dose of rhBMP-2. In addition, a localized effective dose of rhBMP-2 may mitigate against ectopic bone formation. 33 More importantly, we demonstrated that TyrPC+CP without rhBMP-2 may stimulate as much bone formation as a commercially available BGS supplemented with rhBMP-2. This compelling result is one of the most attractive features of the TyrPC family as BGS. Moreover, in contrast to potential immunogens used to deliver rhBMP-2, such as type I bovine collagen, 34 we do not anticipate immunological sequelae from TyrPCs.
Conclusions
The results revealed that porous 3D TyrPC scaffolds were biocompatible, and maintained biomechanical properties upon degradation. Furthermore, at 6 weeks, in the rabbit CSD model, the following observations were noted:
(1) The TyrPC scaffolds did not promote adverse systemic or localized tissue responses, had minimal new bone formation, and significantly increased trabecular bone volume when supplemented with rhBMP-2. (2) TyrPC treated with rhBMP-2 produced a similar quantity of woven bone volume to an FDA-approved, commercially available BGS with rhBMP-2. (3) TyrPC+CP alone had more trabecular bone formation than TyrPC and promoted similar new bone formation to BGS supplemented with rhBMP-2.
Footnotes
Acknowledgments
This research was sponsored by the Armed Forces Institute of Regenerative Medicine (AFIRM) award number W81XWH-08-2-0034. The U.S. Army Medical Research Acquisition Activity is the awarding and administering acquisition office. The content of the manuscript does not necessarily reflect the position or the policy of the Government, and no official endorsement should be inferred. This work was also funded by the Bone Tissue Engineering Center (BTEC) at the Carnegie Mellon University and New Jersey Center for Biomaterials (NJCBM) at Rutgers, The State University of New Jersey. The authors sincerely thank Dr. Durgadas Bolikal and Matthew Laughland for synthesizing the TyrPC, and BTEC members for their technical assistance and helpful discussion. The authors also acknowledge the staff at Allegheny General Hospital for their excellent care of the rabbits for animal studies.
Disclosure Statement
No competing financial interests exist.