
Abstract
Residual periodontal ligament (PDL) cells in the damaged tissue are considered a prerequisite for a successful regeneration of the periodontal architecture with all its components, including gingiva, PDL, cementum, and bone. Among other approaches, current concepts in tissue engineering aim at a hormonal support of the regenerative capacity of PDL cells as well as at a supplementation of lost cells for regeneration. Here, we investigated how far an anabolic, intermittent parathyroid hormone (iPTH) administration would enhance the osteoblastic differentiation of PDL cells and the cellular ability to mineralize the extracellular matrix in an in vivo transplantation model. PDL cells were predifferentiated in a standard osteogenic medium for 3 weeks before subcutaneous transplantation into CD-1 nude mice using gelatin sponges as carrier. Daily injections of 40 μg/kg body weight PTH(1–34) or an equivalent dose of vehicle for 4 weeks were followed by explantation of the specimens and an immunohistochemical analysis of the osteoblastic marker proteins alkaline phosphatase (ALP), osteopontin, and osteocalcin. Signs of biomineralization were visualized by means of alizarin red staining. For verification of the systemic effect of iPTH application, blood serum levels of osteocalcin were determined. The osteogenic medium stimulated the expression of ALP and PTH1-receptor mRNA in the cultures. After transplantation, iPTH resulted in an increased cytoplasmic and extracellular immunoreactivity for all markers investigated. In contrast to only sporadic areas of mineralization under control conditions, several foci of mineralization were observed in the iPTH group. Blood serum levels of osteocalcin were elevated significantly with iPTH. These data indicate that the osteoblastic differentiation of human PDL cells and their ability for biomineralization can be positively influenced by iPTH in vivo. These findings hold out a promising prospect for the support of periodontal regeneration.
Introduction
There is considerable agreement that for a complete regeneration of the PDL to occur, including the cell and fiber apparatus, cementum, and bone, residual PDL cells at the injured site are mandatory. This prerequisite originates from the specific characteristics of PDL cells that represent a heterogeneous population that hosts several progenitor cell types that can be further induced to differentiate into cementoblasts, osteoblasts, and fibroblasts. A certain percentage of the PDL cells have been attributed stem cell-like properties such as self-renewal and multilineage differentiation potential, suggesting an important role of those cells in the regeneration of periodontal tissues.5–10 Furthermore, recent experiments have demonstrated an osteoblast-like phenotype of a certain proportion of PDL cells, as evidenced by the expression of bone-associated marker proteins such as alkaline phosphatase (ALP), osteopontin, and osteocalcin, collagen synthesis, response to bone-inductive factors, and by the ability to mineralize their extracellular matrix in the presence of dexamethasone, ascorbic acid, and β-glycerophosphate.5,11–15 These characteristics make PDL cells a promising source to promote periodontal regeneration. Since the number of residual PDL cells in an injured site is limited and endangered to be further pushed back by the downgrowth of epithelial cells that proliferate at a much higher rate, contemporary regenerative approaches in periodontology include the use of growth factors and hormones to promote the proliferation and differentiation of residual cells.16,17 Recent developments in tissue engineering provide new insights into how to support periodontal regeneration. Cultured PDL cells applied in various scaffolds or in suspension were shown to be able to induce a new periodontal tissue apparatus on root dentin surfaces and on dental implants.11,18–20 Several studies point to the potential benefit of transplanting PDL cell sheets into periodontal defects to support the formation of bone and cementum as well as the insertion of collagen fibers into this newly formed hard tissue.13,21,22
Among the proregenerative hormones, parathyroid hormone (PTH) is currently well recognized as an anabolic treatment option in the healing process of bony defects.23,24 Data obtained in healthy and estrogen-deficient rats prove its capacity to protect against periodontitis-associated bone loss.25,26 Previously, we demonstrated that PDL cells express the PTH1 receptor and respond to an intermittent PTH(1–34) administration in an osteoblast-like manner with changes in proliferation, apoptosis, differentiation, and the production of osteoprotegerin, which then, in turn, modified the differentiation and resorptive activity of osteoclasts.27–29 In a recent seminal work, Bashutski et al. demonstrated clinically the benefit of intermittent PTH in the attempt to improve the outcome of periodontal surgery in 40 patients suffering from severe, chronic periodontitis. 30 The authors followed a clinically established protocol for the systemic administration of PTH with an approved dosing regimen. This policy does not disregard the need for a future translation of the findings into a local delivery protocol to minimize side effects before PTH becoming a routine procedure in periodontal regeneration. However, the cited study could not answer the questions whether osteoblasts and/or PDL cells were targeted by PTH and which cells were responsible for the mediation of the proregenerative effect on periodontal structures observed clinically.
In the present investigation, we analyzed for the first time the effect of an intermittent PTH administration on transplanted human PDL in vivo. Gelatin sponges containing explanted and predifferentiated human PDL cells were transplanted into immunocompromised mice for 4 weeks with daily injections of PTH(1–34). Markers of osteoblastic differentiation, including ALP, osteopontin, and osteocalcin, as well as well as signs of starting mineralization were determined.
Materials and Methods
All experimental protocols were reviewed and approved by the ethics committee and the local committee for animal care of the University of Bonn.
PDL cell explantation
Human PDL cells were scraped from the middle third of the roots of premolars of two different human donors, aged between 12 and 14 years, showing no clinical signs of periodontitis. The teeth had been extracted for orthodontic reasons and with informed parental consent. Cells were cultured in the Dulbecco's Modified Eagle's Medium containing 10% fetal bovine serum and 0.5% antibiotics (diluted from a stock solution containing 5000 U/mL penicillin and 5000 U/mL streptomycin; Biochrom AG, Berlin, Germany) and cultured at 37°C in an atmosphere of 100% humidity, 5% CO2, and 95% air.
Induction of osteoblastic predifferentiation
Fifth-passage PDL cells were cultured in 24-well plates at a seeding density of 10,000 cells/well and exposed to a standard osteogenic medium containing 10 nM dexamethasone, 50 μg/mL ascorbic acid, and 10 nM β-glycerophosphate (Sigma Aldrich, Hamburg, Germany) for 3 weeks to induce a more differentiated osteoblastic phenotype as described previously. 4 At harvest, the success of this measure was demonstrated by cell characterization with respect to the gene expression of markers of osteoblastic differentiation ALP-specific activity and PTH1-receptor (PTH1-R) production by real-time PCR as described previously. 31 The primer sequences used were as follows: PTHR1 sense 5′ CTC-CCT-CTC-GAT-CCT-ACA-GTA-ATG-A 3′, antisense 5′ TCA-GAG-TCA-ATG-CCT-CCG-TTC 3′; ALP sense 5′ AGA-GAA-AGC-GAT-GGT-GGA-TG 3′, antisense 5′ CGG-TGG-CAT-TAA-TAG-TGA-GAT-G 3′.
CD-1® nude mice
Twelve 4–6-week-old male CD-1® nude mice with an average body weight of 20 g (Charles River Laboratories, Sulzfeld, Germany) were stabilized at the animal research facility of the University of Bonn of Medicine. Mice were housed one per cage under specific pathogen-free conditions in a room with continuously filtered air, maintained between 21°C and 22°C, with 40%–60% humidity on 12-h light-and-dark cycles and given free access to food and water. Animal body weights were recorded before the onset and at the end of the experiment.
Surgical implantation of PDL cells
Pretreated PDL cells from the two donors were resuspended each in fresh growth media, and 3×106 cells were incorporated into gelatin sponges 3–5 mm in diameter (Gelfoam®; Sullivan-Schein, Melville, NY) by capillary action. The implantation procedure was adopted from Pettway et al. 32 According to this protocol, animals were anaesthetized with 2vol% isoflurane (Forene®; Abbott GmbH, Wiesbaden, Germany), and two mid-longitudinal skin incisions ∼1 cm in length were made on the dorsal surface of each mouse. Blunt dissection was used to form subcutaneous pouches. Two implants per animal were inserted. Postsurgically, mice were monitored daily for any signs of infection like shivering, lethargy, and diarrhea. Neither were signs of impaired healing nor adverse side effects of the procedures or drug dosage observed.
Intermittent PTH(1–34) administration
To examine the mineralization capacity of PDL cells and the anabolic potential of intermittent PTH(1–34) regarding the support of this capacity, mice were randomly assigned to one of two experimental groups, with one group receiving daily subcutaneous injections of 40μg/kg body weight recombinant human PTH(1–34) (Sigma Aldrich) for 4 weeks, starting at day 1 after PDL cell implantation, whereas the other group received sham injections of an equivalent dose of sterile water. The dose of PTH(1–34) used in these studies proved effective in previous experiments. 33 On day 28, the animals were anesthetized with isoflurane, and blood (by means of cardiac puncture) and the implants were collected before euthanasia via cervical dislocation.
Serum analysis of osteocalcin
To demonstrate a systemic effect of the iPTH administration on bone turnover on day 28, serum was separated from blood via centrifugation at 1500 rpm for 30 min at 4°C and stored in single-use aliquots at −80°C for future analysis. Serum levels of mouse-specific osteocalcin were quantified by the use of a commercially available ELISA assay (DRG Instruments, Marburg, Germany) according to the manufacturer's instructions.
Histology
The explants were fixed in 4% phosphate-buffered (according to Sörensen) formaldehyde for 24 h at room temperature. Thereafter, they were first hydrated, then dehydrated in an ascending ethanol series, and finally embedded in paraffin. As a next step, tissue sections of 5-μm thickness were cut in the sagittal plane, mounted on glass slides, and dried at 37°C overnight before further processing. Tissue sections were deparaffinized by passing them through a descending series of ethanol ending with distilled water. Selected sections were stained with hematoxylin and eosin (H&E).
Documentation of the presence of human PDL cells after implantation in immune-compromised mice
To ensure that the investigated cells were the transplanted cells of human origin, the cell nuclei of those cells were detected immunohistochemically using an antibody specific to human, but not mouse cells (MAB1281; Millipore, Schwalbach, Germany). To this end, the immunohistochemical protocol described below was amended by a preincubation step with an unconjucated Fab fragment anti-mouse IgG (IgG-Fc, ab97005; Abcam, Cambridge, United Kingdom) for 1 h at room temperature before the incubation with the primary antibody.
Immunohistochemistry
Tissue sections were placed in a Tris–hydroxy methyl aminomethane-buffered saline (TBS) at pH 7.4 for 10 min. Thereafter, the endogenous peroxidase activity was blocked in 70 mL methanol containing 700 μL of 30% H2O2 for 45 min in the dark. Subsequently, sections were rinsed again and then preincubated with TBS containing 4% bovine serum albumin (TBS/BSA) for 20 min to avoid unspecific background staining. Thereafter, sections were incubated with a polyclonal primary antibody of rabbit origin (ALP: ab011200130; Quartett, Berlin, Germany; osteopontin: ab18625; IBL, Hamburg, Germany; osteocalcin: ab76688; Abcam) in a 1:50 (osteocalcin) or 1:100 (osteopontin) working solution of TBS/BSA either for 1 h at room temperature (osteocalcin) or at 4°C overnight in a humidified chamber (ALP, osteopontin). The anti-ALP antibody was supplied in a ready-to-use working solution by the manufacturer. The slides were rinsed again and incubated for 30 min with a peroxidase-labeled polymer conjugated to a goat anti-rabbit immunoglobulin provided as a ready-to-use solution (Envision; Dako A/S, Glostrup, Denmark) as a secondary antibody. Incubation was stopped in TBS before the substrate–chromogen solution was applied for 10 min. Afterward, the specimens were rinsed and then counterstained with Mayer's hematoxylin, dehydrated, and cover slipped for the light microscopical analysis.
To prove the specificity of the immunoreactions, negative controls were carried out by (1) omitting the primary antibody, (2) omitting both the primary and secondary antibody and using TBS/BSA instead, and (3) substitution of the antibodies with nonimmune species-specific immunoglobulin G in a 1:10 dilution.
Sections of bony tissues carrying significant amounts of the antigens of interest were treated in the same way as the experimental sections and served as positive controls.
Biomineralization
The mineralization capacity of PDL cells was monitored by alizarin red staining as described previously. 34
Semiquantitative assessment of the immunoreactivity
Three representative sections per specimen were randomly selected for the assessment of the staining intensity for a particular antigen resulting in a total of 36 specimens per experimental group. Immunoreactivity was determined semiquantitatively by assigning one of the following grades to the specimen: 0, no immunoreactivity; 1, weak immunoreactivity with only single cells presenting faint immunoreactions; 2, moderate immunoreactivity with about 50% of cells showing a visible immunoreaction; 3, strong immunoreactivity in most of the cells. Reproducibility of the readouts was ensured by analyzing 36 selected specimens in duplicate. An intraobserver error was demonstrated to happen in<4% of the cases, and the deviation did not exceed one grade.
Statistical analysis
For any given experiment, each data point represents the mean±SEM of 36 independent specimens. Statistical significance of the data was analyzed using the Mann–Whitney-U test. p-Values<0.05 were considered to be significant.
Results
Effects of dexamethasone stimulation
The cellular characterization after dexamethasone stimulation of the PDL cell cultures for 3 weeks revealed a significant increase of ALP (3.90±1.74) and PTH1-R (3.37±1.26) mRNA expression as compared to the vehicle-treated controls (1.16±0.73 and 1.07±0.43, respectively) (Fig. 1).

Induction of enhanced osteoblastic differentiation of periodontal ligament (PDL) cells by dexamethasone. After 3 weeks of culture, the alkaline phosphatase (ALP) activity and parathyroid hormone 1-receptor (PTH1-R) transcript expression increased significantly compared to the vehicle-treated controls. The bar graph shows the mean±SEM of six independent cultures that were assayed in duplicate. **p<0.01, dexamethasone-treated group versus vehicle control; ***p<0.001, dexamethasone-treated group versus. vehicle control.
Effect of intermittent PTH(1–34) on osteocalcin blood serum level
Daily subcutaneous injections of 40 μg/kg PTH(1–34) for 28 days raised the blood serum level of osteocalcin approximately threefold (41.61±13.02 ng/mL) compared to the control animals, which only received sham injections (13.90±2.81 ng/mL). These differences proved statistically significant (Fig. 2).
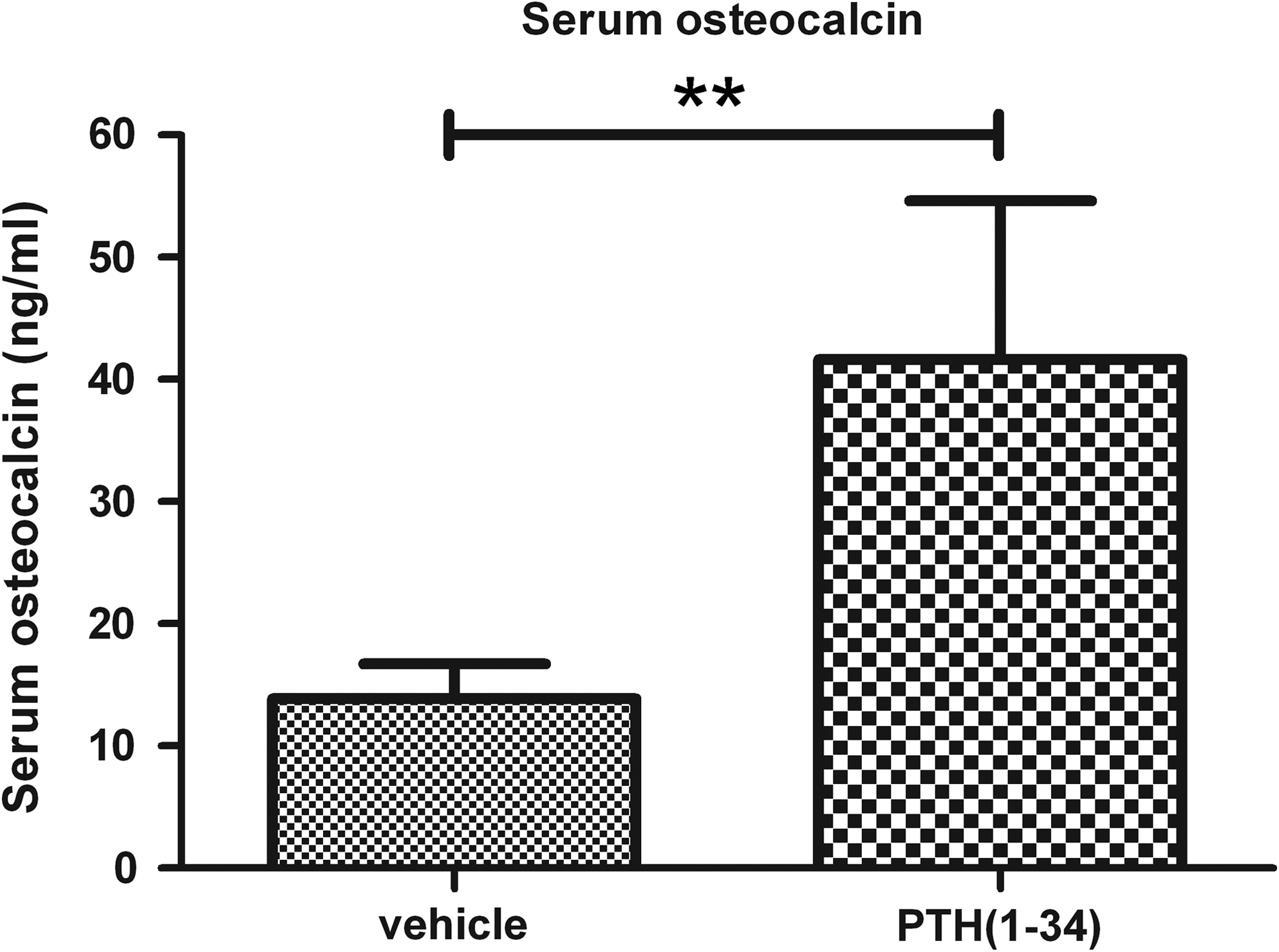
PTH(1–34)-induced increase of osteocalcin serum levels in vivo as determined by ELISA after 4 weeks. The bar graph shows the mean±SEM of six mice per group. **p<0.05, PTH(1–34) versus vehicle control.
Identification of human PDL cells in mouse tissue
Proof of the human origin of the cells under investigation was provided by an immunohistochemical staining specific to human, but not mouse cell nuclei. In all specimens, a positive immunoreaction demonstrated the presence of human-transplanted PDL cells in the gelatin sponges. Mouse parotid gland tissue, which served as a negative control, remained unstained (Fig. 3).

Proof of human cells in the specimens explanted from six CD-1® nude mice. Specimens were processed for immunohistochemical detection of human cell nuclei to identify human PDL cells (left panel; open arrows); C, collagen. The right panel depicts a negative control experiment with mouse parotid gland tissue. Color images available online at www.liebertonline.com/tea
Histology
Histology of the recovered specimens revealed the collagenous structure of the scaffolds, which mostly appeared as a fibrous network containing porous spaces ranging from 50 to 100 μm. In those spaces, a gradual distribution of the PDL cells, including extracellular matrix throughout the gelatin sponges with the outer areas being more populated by PDL cells than the inner regions, became evident. The H&E stainings of the sham-injected animals were characterized by loose connective tissue with only few mineralizing PDL cells lining the scaffold. Signs of osteoid deposition could hardly be observed (Fig. 4A). In the PTH(1–34)-treated groups, the connective tissue in between the pores appeared more condensed; there were several cells in close contact to the gelatin surfaces, and early signs of osteogenesis became apparent as evidenced by thin seams of comparatively immature osteoid deposition (Fig. 4B). Blood vessels were not visible.
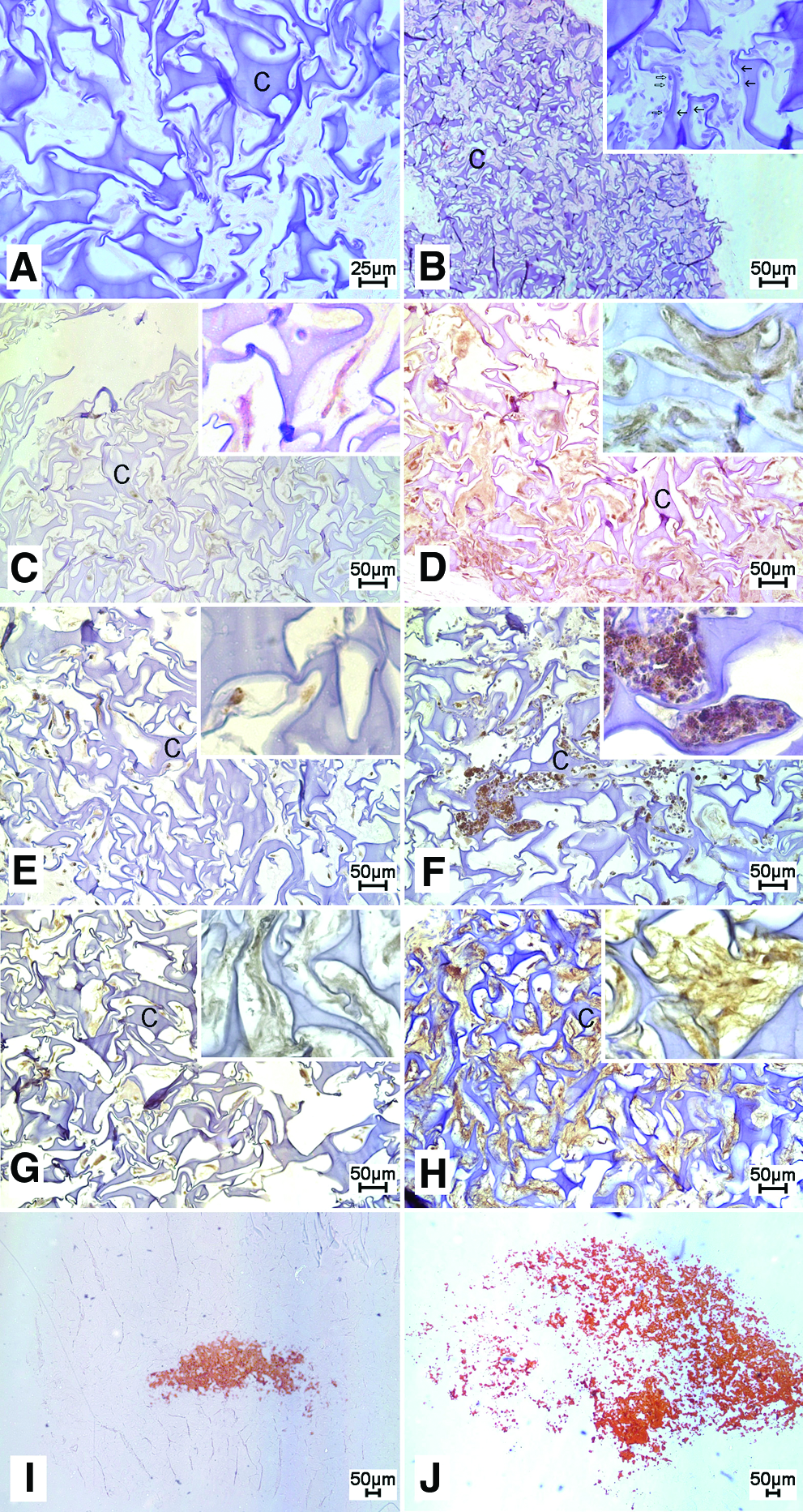
Light microscopic views of scaffolds with human PDL cells of sham-injected mice (left panels) and those treated with PTH(1–34) for 28 days (right panels). The insets demonstrate a detail at a higher magnification. In panels
ALP, osteopontin, and osteocalcin immunohistochemistry
In the control specimens, ALP, osteopontin, and osteocalcin immunoreactivity was detected in the cytoplasm of the PDL cells and in the extracellular matrix, respectively, with the intracellular staining being stronger than the extracellular. Correlating with the cell distribution pattern, it was found to be more intense in the outer areas as compared to the inner zones of the specimens. Intermittent PTH(1–34) administration in the postsurgical period of 28 days resulted in a visible increase of both the number of immunoreactive cells and the staining intensity for all three antigens under investigation as compared to the sham-injected controls (Fig. 4C–H). This visual impression was further substantiated by semiquantitative assessment using a rating system ranging from 0 to 3 and proved statistically significant for all parameters tested (ALP: 2.64±0.09 vs. 1.58±0.09; osteopontin: 2.36±0.11 vs. 1.91±0.14; and osteocalcin: 2.09±0.16 vs. 1.55±0.14) (Fig. 5A–C).

The effect of intermittent PTH(1–34) administration on protein expression of ALP
No immunoreactions were detected in any of the negative control specimens.
Biomineralization
Alizarin red staining as a marker of biomineralization followed a similar staining pattern as described for the osteoblastic marker proteins with ossicles from PTH(1–34)-treated animals exhibiting a significantly higher degree of mineralization (1.50±0.13) than ossicles from vehicle-treated animals (0.81±0.10) (Figs. 4I, J, and 5D).
Discussion
In the present study, a cell-based tissue-engineering model was used to gain further insight into the regenerative capacity of transplanted human PDL cells and the supportive potential of intermittent PTH(1–34) in this respect. The results obtained present the first in vivo evidence for an anabolic effect of intermittent PTH(1–34) on human PDL cells in terms of osteoblastic differentiation and biomineralization. The experimental setup refers to one of the contemporary approaches in tissue engineering, which is to enhance the regenerative activity of cells by hormonal stimulation. The principled suitability of PDL cells for the regeneration of PDL tissue was demonstrated repeatedly, for example, by Akizuki et al., 22 who reported on the successful regeneration of periodontal tissue utilizing a PDL cell sheet in a dehiscence model in vivo in beagle dogs. The use of PDL cells from periodontically healthy donors is appropriate in this setting, although one might argue that PDL cells might change their phenotypic expression under inflammatory conditions such as periodontitis. These phenotypic alterations have indeed been demonstrated in vitro, but they were concomitantly shown to be transient and reversible once a physiological environment was re-established. 35 This consideration is well reflected in current clinical procedures in periodontology, where regenerative treatment protocols are not applied until a successful anti-inflammatory therapy has been carried out.
In our study, the heterogeneous population of PDL cells as a whole was employed that was demonstrated to exhibit osteoblastic traits and an osteoblast-like response to PTH challenge, implicating a potential benefit from using these cells in the attempt to support periodontal regenerative processes. In contrast, Seo et al. presorted PDL cells for the proportion with a putative stem cell character (PDLSC) as evidenced by being STRO-1 and CD-146 positive. 7 This subpopulation was demonstrated to comprise about 10%–15% of the cells, and their proportion decreased with increasing the cell culture passage. 6 The preselected PDLSCs were then transplanted into immunodeficient mice and shown to generate a cementum/PDL-like structure in vivo. 7 Similar to our findings regarding the expression of key proteins of osteoblastic differentiation, including ALP, osteopontin, and osteocalcin, by the transplanted PDL cells, these data demonstrated that the generated tissues closely resembled natural bone or cementum.
The standard osteogenic stimulation protocol applied in our experiments was adopted from reports in the literature, indicating that this supplement is mandatory for PDL cells to facilitate mineralization of their extracellular matrix. 36 Flores et al. reported that, in the absence of the osteodifferentiation medium, PDL cells were unable to produce mineral-like nodules after transplantation in vivo. On the other hand, the addition of dexamethasone, ascorbic acid, and β-glycerophosphate to the cultures for 3 weeks resulted in positive von Kossa staining. 4 These findings confirm our own unpublished observation that PDL cells start to mineralize their extracellular matrix after 15 days in culture with an osteogenic medium only. However, the effect of dexamethasone was shown to be multifaceted, since a cell density-dependent impact of this synthetic glucocorticoid on the proliferation and differentiation of osteoprogenitor subpopulations in adherent cell cultures was demonstrated. The authors concluded on a role for cell–cell interactions in the control of progenitor cells during in vitro culture.37,38 Nevertheless, in the present investigation, a dexamethasone, ascorbic acid, and β-glycerophosphate challenge of the PDL cell cultures led to an increased expression of ALP and PTH1-R mRNA expression, indicating the successful establishment of the intended enhanced osteoblastic differentiation stage of the cells. When discussing the potential adverse effects of dexamethasone, it should not be disregarded that despite of their osteoblastic traits, PDL must not be equated with osteoblasts, and therefore findings obtained in studies on osteoblasts cannot be assumed to be equally valid for PDL cells.
The idea behind using a gelatin sponge as a scaffold for the transplanted PDL cells was to provide a temporary, artificial extracellular matrix to allow for cell attachment and guide three-dimensional tissue formation.39,40 The advantage of gelatin as a denatured biopolymer derived from collagen was the search for a scaffolding material that would not exert an effect itself and, thereby, distract from the parameters of interest, namely, PDL cells and PTH. Furthermore, gelatin sponges were used in several recent reports on cell transplantation models 32 ; therefore, we wanted our experimental setup to allow for a better comparability to previously published results. Future studies will help to throw light on whether scaffolds other than gelatin, for example, hydroxyapatite or tricalciumphosphate, with osteoinductive properties will offer further advantages in the attempt to support the regenerative capacity of PDL cells.
The availability of a sufficient concentration of active PTH in the local microenvironment to exert an effect on the transplanted PDL cells was another major concern in the present study, since this could only be realized by blood diffusion. Diffusion is also needed to provide nutrients for the transplanted cells. It was unlikely that blood vessel growth into the gelatin sponge would occur shortly after sponge transplantation. This consideration is supported by the lack of blood vessels in the histological specimens. However, our results indicate that cells not only survived, but also were able to develop a bone-like tissue, and this capacity was significantly enhanced in the PTH-treated animals by diffusion.
According to Sheehan et al., 41 the anabolic effect of intermittent PTH on bone varies with the species studied as well as with the duration and mode of its administration. One measure to verify a systemic response to subcutaneously injected PTH is the quantification of serum markers of bone turnover. Among others, osteocalcin was demonstrated to be influenced by PTH treatment under different conditions and in different mouse gene types. 41 The mentioned study demonstrated that serum osteocalcin levels were significantly increased after PTH exposure. The authors concluded from their work that intermittent PTH(1–34) for 3 weeks is sufficient to enhance bone formation without enhancing resorption. 41 In accordance with these considerations, our results indicate a significant anabolic effect of PTH(1–34), as evidenced by the enhanced expression of markers of osteoblastic differentiation and biomineralization and also by serum osteocalcin levels in the PTH(1–34)-treated mice.
Using an osteoblast transplantation model similar to ours with PDL cells, Pettway et al. previously indicated the beneficial effect of intermittent PTH in tissue-engineering applications. According to their study, the bone volume and bone content of implanted collagen sponges containing osteoblasts were significantly increased after 4 weeks of PTH administration.32,44
The present data transfer our recently obtained in vitro findings, which demonstrated a maturation state-dependent effect of intermittent PTH on nearly all major PDL cell functions,29,42,43 to an in vivo microenvironment, and provide proof of their physiological relevance. Further support that warrants further research on the anabolic potential of PTH in dentofacial applications was recently provided by the already mentioned work of Bashutski et al. who demonstrated the benefit of intermittent PTH in the attempt to improve the clinical outcome in patients suffering from periodontitis. 30
In summary, our findings show that periodontal regeneration can be supported by a PTH and PDL cell-mediated tissue-engineering approach. This study is a further step toward reaching the goal of regenerating a functional PDL and alveolar bone by using transplantation of PDL cells in combination with the anabolic effect of intermittent PTH. The already-practiced approach of cryopreserving extracted wisdom teeth for later retransplantation in extraction sites also holds out the prospect of using the attached PDL as a source of PDL cells to be transplanted into cell-deficient postinflammatory sites followed by PTH stimulation of their regenerative capacity. However, before clinical application, important safety aspects regarding potential adverse side effects of PTH, the durability of the PTH effect, and the optimal dosing regimen for a local administration have to be addressed.
Footnotes
Acknowledgments
The authors thank T. Schaffrath for expert technical assistance. This research was supported by a research grant from the Deutsche Forschungsgemeinschaft (DFG, KFO 208; LO-1181/2-2) and by the Medical Faculty of the University of Bonn. The authors do not have any conflict of interest.
Disclosure Statement
No competing financial interests exist.