
Abstract
Objectives:
Percutaneous stenting of occluded peripheral vessels is a well-established technique in clinical practice. Unfortunately, the patency rates of small-caliber vessels after stenting remain unsatisfactory. The aim of the BioStent concept is to overcome in-stent restenosis by excluding the diseased vessel segment entirely from the blood stream, in addition to providing an intact endothelial cell layer.
Design:
The concept combines the principles of vascular tissue engineering with a self-expanding stent: casting of the stent within a cellularized fibrin gel structure, followed by bioreactor conditioning, allows complete integration of the stent within engineered tissue.
Materials and Methods:
Small-caliber BioStents (Ø=6 mm; n=4) were produced by casting a nitinol stent within a thin fibrin/vascular smooth muscle cell (vSMC) mixture, followed by luminal endothelial cell seeding, and conditioning of the BioStent within a bioreactor system. The potential remodeling of the fibrin component into tissue was analyzed using routine histological methods. Scanning electron microscopy was used to assess the luminal endothelial cell coverage following the conditioning phase and crimping of the stent.
Results:
The BioStent was shown to be noncytotoxic, with no significant effect on cell proliferation. Gross and microscopic analysis revealed complete integration of the nitinol component within a viable tissue structure. Hematoxylin and eosin staining revealed a homogenous distribution of vSMCs throughout the thickness of the BioStent, while a smooth, confluent luminal endothelial cell lining was evident and not significantly affected by the crimping/release process.
Conclusions:
The BioStent concept is a platform technology offering a novel opportunity to generate a viable, self-expanding stent structure with a functional endothelial cell lining. This platform technology can be transferred to different applications depending on the luminal cell lining required.
Introduction
In the cases of both coronary artery and peripheral vessel occlusion, normal blood flow can be restored to the tissue using balloon angioplasty, in which a catheter is advanced to the site of obstruction using a minimally invasive, endovascular technique (i.e., percutaneous transluminal angioplasty [PTA]). Once advanced to the site of the lesion, the balloon is inflated to compress the atherosclerotic plaque against the arterial wall. In these cases, however, the arteries frequently undergo restenosis (re-narrowing)—a reparative process that occurs after endothelial injury. The incidence of restenosis can be significantly reduced by implanting an expandable stent at the occlusion site during the angioplasty procedure. Stainless steel stents were initially used in femoropopliteal stenting, but the patency rates compared with PTA alone were not significantly improved. The employment of nitinol as a stent material has led to better patency rates compared with both standard balloon angioplasty (Vienna study) 1 and stainless steel stent deployment in femoropopliteal arteries.2,3 Despite these advances, however, angioplasty and stenting techniques are still hindered by late thrombosis events and in-stent restenosis, which ultimately require repeated interventions, and intense research is ongoing in an effort to develop more biocompatible materials.
In the present study, we propose a novel approach to address this biocompatibility issue by ensheathing a warp-knitted, self-expanding nitinol stent within a cell-seeded fibrin matrix (termed BioStent) (Fig. 1). It is hypothesized that the cell-seeded fibrin matrix of the BioStent can be conditioned to form autologous tissue using a customized bioreactor system, which will ultimately prevent direct contact of the integrated nitinol stent material with either the blood face or the surrounding vascular tissue and atherosclerotic plaques. The newly developed tissue should also prevent vascular cell ingrowth from the surrounding vessel and subsequent restenosis. In addition, a viable, luminal endothelial cell coating of the BioStent should reduce any risk of thrombosis and neointimal formation following stent deployment. The purpose of the present study is threefold: (1) to determine the cytocompatibility of the nitinol stent material with seeded vascular smooth muscle cells (vSMCs), (2) to determine the effect of the BioStent material on vSMC proliferation, and (3) to determine the feasibility of coating the BioStent with an endothelial cell lining to minimize thrombus formation.
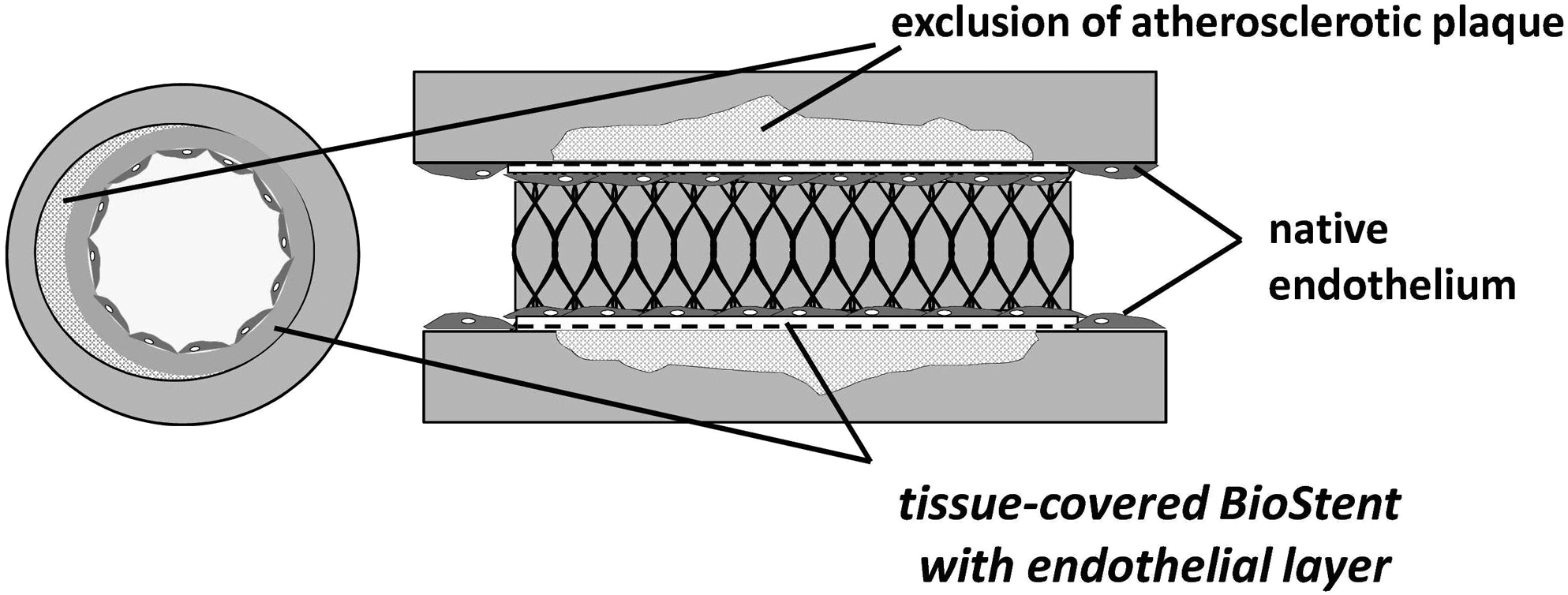
Illustration of the BioStent concept. (1) The foreign body reaction, (2) the cell proliferation with ingrowth into the lumen, and (3) acute thrombosis by hemo-incompatibility need to be avoided in stent angioplasty.
Materials and Methods
Cell culture
The sheep cadavers used to isolate the cells for these experiments were kindly provided by the Institute for Laboratory Animal Science and Experimental Surgery, RWTH Aachen University. All animals were treated in compliance with the European Convention on Animal Care.
For isolation of endothelial cells and vSMCs, carotid arteries from juvenile sheep cadaver were harvested under sterile conditions. After washing the carotid arteries with phosphate-buffered saline (PBS; PAA Laboratories GmbH), endothelial cells were removed using 1 mg/mL collagenase (Type II; Gibco). The isolated endothelial cells were re-seeded on 2% gelatin-precoated tissue culture flasks (T75; Greiner) in endothelial basal medium (PAA Laboratories GmbH) supplemented with endothelial medium supplement (PAA Laboratories GmbH) and 1% antibiotic–antimycotic solution (PAA Laboratories GmbH).
The remaining arterial tissue was minced into 1-mm rings for primary explant culture of vSMCs in Dulbecco's modified Eagle's medium (DMEM; Gibco) supplemented with 10% fetal bovine serum (FBS; PAA Laboratories GmbH) and 1% antibiotic/antimycotic solution. To obtain sufficient cell numbers, each cell population was serially passaged up to four times using 0.25% trypsin/0.02% ethylenediaminetetraacetic acid (EDTA) solution (Gibco) and cultured in 5% CO2 and 95% humidity at 37°C.
Cytotoxicity assays
Lactate dehydrogenase release (necrosis assay)
The indirect cytotoxic effect of the stent material nitinol on the vSMCs was evaluated using a commercial assay kit based on the release of lactate dehydrogenase (LDH) from lysed cells (CytoTox® 96 Non-Radioactive Cytotoxicity assay; Promega GmbH). The test was performed according to a standard protocol described elsewhere. 4 Briefly, vSMCs were cultured in a 24-well plate at a density of 8.0×104 cells/well in medium (DMEM and 5% FBS; Gibco). After 48 h of preculturing, the medium was replaced with test medium (DMEM without FBS, preincubated with the stent material for 72 h at 37°C). The amount of LDH released into the test medium after 4 and 24 h of incubation was determined by measuring the absorbance of test samples with a multiwell spectrophotometer (Tecan Infinity M200; Tecan Deutschland GmbH). The LDH-positive control solution (bovine heart LDH) included in the commercial kit was used as a positive control, while standard cell culture medium, which was not in contact with the material, served as a negative control. Each assay was performed in triplicate.
MTT assay (proliferation assay)
The indirect effect of the stent material nitinol on cell proliferation was determined using the 3-[4,5-dimethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide (MTT) assay. 5 Briefly, vSMCs were seeded in a 24-well plate (3×104 cells/well) in DMEM culture medium and incubated under standard conditions. After 48 h of preculturing, the medium was replaced with test medium (DMEM+10% FBS, preincubated with the stent material for 72 h at 37°C). Standard cell culture medium (DMEM+10% FBS), which was not in contact with the material served as a negative control. DMEM with a reduced supplement of FBS (5%) was used as positive control. Proliferation of cells was determined after 3 and 6 days using the MTT assay: after adding 40 μL of MTT solution (5 mg/mL in Ca2+- and Mg2+-free PBS; Sigma) to each test well, cells were incubated for 1 h at 37°C. The resulting colored formazan crystals were dissolved by adding a 9:1 isopropanol solution/formic acid solution and the optical density was measured at 550 nm using a spectrophotometer (Tecan Infinity M200). Each assay was performed in triplicate.
Fibrin gel fabrication
Fibrinogen (Sigma-Aldrich) was dissolved for 1.5 h in purified water and dialyzed against 4 L of Tris-buffered saline (TBS) in 6000–8000 MW dialysis tubing (Novodirect) overnight. After sterile filtration, the fibrinogen concentration was estimated by measuring the absorbance at 280 nm using a spectrophotometer (Spectronic Genesys TM6; ThermoFisher). The final concentration of fibrinogen solution was adjusted to 10 mg/mL with TBS. The fibrin gel component of the BioStent (2.5 mL total) consisted of 1.25 mL of fibrinogen solution (10 mg/mL), 0.875 mL TBS containing 5×107 vSMCs (2×107 cells/mL), and 188 μL of 50 mM CaCl2 (Sigma) in TBS. Gel polymerization was initialized by adding 188 μL of thrombin solution (40 U/mL; Sigma).
Warp-knitted nitinol stent
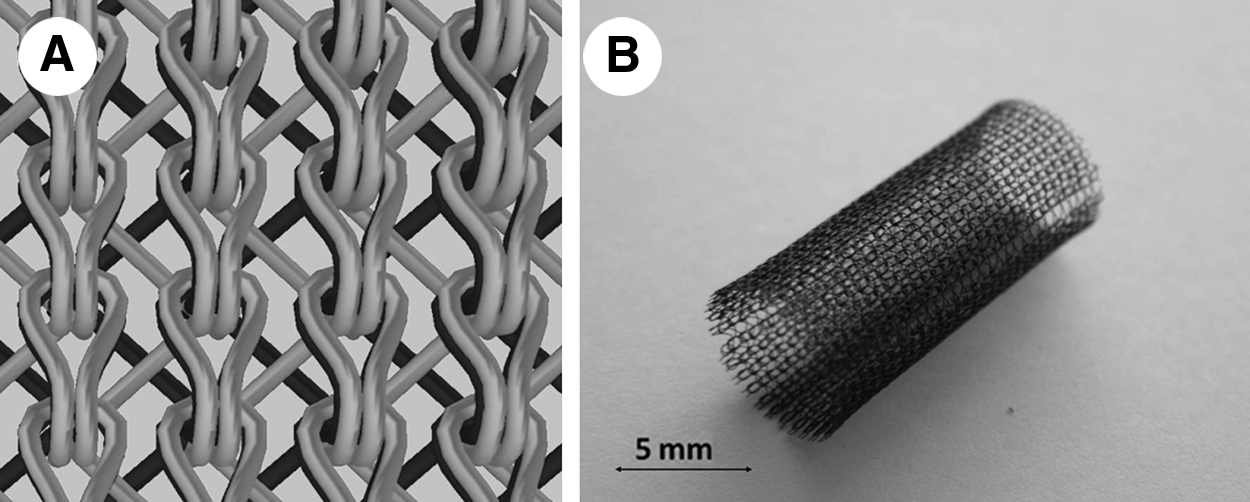
To obtain stent structures with sufficient radial stability, superelastic nitinol wire (NiTi Nr.1SE; Fort Wayne Metals) was employed (76-μm thickness). To achieve adequate surface area coverage, warp-knitted stents with a two-bar tricot interloop were produced on a double-raschel warp-knitting machine (Karl Mayer). With regard to loop density, 12 loops/cm were produced with a needle gauge of 30 needles/inch (E30) (Fig. 2). The fabricated tubular nitinol structures were fixed on a metal core and tempered at 500°C for 15 min in a high-temperature kiln (Heraeus) to achieve the superelastic phase.
This stent design was chosen due to a reduced stent foreshortening compared with other tested stent designs (Fig. 3). Further, the stent strut density of the warp-knitted stent allowed the best complete fibrin gel coverage, compared with other designs (data not shown).

Different stent designs tested regarding tissue coverage of the BioStent.
BioStent moulding/cell seeding
The moulding technique described previously for the fabrication of vascular composite grafts 6 was adapted for ensheathing a warp-knitted, self-expanding nitinol stent within a cell-seeded fibrin matrix (n=4). The mould used to fabricate the BioStent could be directly integrated in a bioreactor system for subsequent conditioning. The mould consisted of a gas-permeable outer silicone cylinder (inner Ø=8 mm; Ismatec), and an inner casting cylinder (Ø=5.5 mm), machined from polytetrafluorethylene (PTFE; Kümpel-Kunststoff-Verarbeitungswerk).
For the moulding process, the stent was pulled over the inner casting cylinder and positioned coaxial to the outer cylinder. The space between the inner and outer cylinders was filled with vSMCs in a fibrinogen suspension (2.1×107 cells/mL) and subsequently combined with thrombin/CaCl2 solution to initiate polymerization using a double-syringe mixer (Medmix Systems AG). After a 45 min of polymerization phase, the inner casting cylinder was removed, with the fibrin/cell-embedded BioStent remaining in the outer cylinder. The outer cylinder was then connected to the main flow circuit in the bioreactor system (Fig. 4).

Bioreactor setup: a peristaltic pump drives a medium flow through the coated stent, thereby conditioning the cells. Pressure is monitored online.
Bioreactor conditioning
Bioreactor conditioning was performed for 21 days according to a protocol described previously. 7 The flow through the BioStent lumen was generated by a peristaltic pump (MCP-Process; Ismatec), and was gradually increased to 200 mL/min (required 60–240 pulses/min) over the conditioning period. A clamp on the tubing circuit distal to the stent enabled the regulation of pressure to physiological levels (∼80/120 mmHg). The pressure was monitored by an online pressure sensor (Codan Medical GmbH), and controlled by a computer via an analog/digital converter (USB6009; National Instruments Germany GmbH). The main flow loop tubing was composed of platinum-cured silicone peroxide (Ismatec), with high gas transfer coefficients for both oxygen and carbon dioxide to provide stable culture conditions. The complete bioreactor system was maintained in a standard incubator at 37°C and 5% CO2. The culture medium used in the bioreactor system consisted of DMEM with 10% FBS, 1% antibiotic-antimycotic solution, and L-ascorbic acid-2-phosphate (1.0 mM; Sigma), and was changed weekly under sterile conditions. Fibrin degradation was controlled by supplementation of the medium with 20 mg/mL aprotinin (Bayer). 8 The culture medium's pH, pO2, pCO2, glucose, and lactate levels were regularly monitored using a blood-gas analyzer (Radiometer EML100; Radiometer).
Endothelialization
To seed a monolayer of endothelial cells on the luminal surface, the conditioned BioStent (plus outer mould cylinder) was disconnected from the bioreactor system and filled with endothelial medium containing 4×106 ovine carotid artery–derived endothelial cells. The cylinder was then sealed at both ends and mounted on a programmable roller pump, which was used to rotate the BioStent about a horizontal axis. The BioStents were rotated for 20 s, followed by a 20-min stationary phase to allow endothelial cell attachment. The cycle was repeated three times before the direction of rotation was changed. In total, endothelial cell seeding was performed for 6 h. After cell seeding, the BioStent (plus outer cylinder) was reconnected to the bioreactor system under sterile conditions, allowing a further 7 days of conditioning under reduced flow conditions (50 mL/min).
Crimping test
To test the feasible application of the BioStent in peripheral vessels (Ø=6 mm) using a PTA technique, the BioStent was initially crimped to 12FR by using silicone fiber to withdraw the stent into a custom-made PTFE catheter. The BioStent was subsequently released into a glass cylinder (Ø=6 mm). Analysis of the endothelial cell layer before crimping and after the release process was performed by scanning electron microscopy (SEM).
BioStent tissue analysis
Light microscopy
Carnoy's-fixed, polymethylmethacrylate (PMMA; Heraeus-Kulzer)-embedded BioStents were sectioned transversely at 10–30-μm thickness via a sawing-and-grinding technique, deplasticized, and analyzed using routine histochemical and immunohistochemical staining. Tissue morphology of the BioStent was evaluated by hematoxylin and eosin (H&E) staining. Polished sections were viewed using routine bright field light microscopy (AxioImager; Carl Zeiss GmbH). Images were obtained using a digital camera (MRc3; Carl Zeiss).
Immunohistochemistry
Nonspecific sites on Carnoy's-fixed, deplasticized sections were blocked and the cells were permeabilized with 5% normal goat serum (Sigma) in 0.1% Triton-PBS for 1 h. Sections were incubated for 1 h at 37°C with the following primary antibodies: rabbit anti-type III collagen (1:100; Acris Antibodies) and mouse anti-alpha-smooth muscle actin (alpha-SMA, 1:400; Sigma). Sections were then incubated for 1 h at 37°C with either AlexaFluor488- or AlexaFluor594-conjugated goat-anti-mouse or goat-anti-rabbit secondary antibody (1:400; Molecular Probes). Cell nuclei were counterstained using DAPI nucleic acid stain (Molecular Probes). As negative controls, samples were incubated only in diluent and secondary antibody. Ovine carotid artery served as a positive control.
Sections were viewed using an epifluorescence microscope (AxioObserver; Carl Zeiss). Images were acquired using a monochromatic digital camera (MRm; Carl Zeiss) and processed using digital software (AxioVision 4.8; Carl Zeiss).
Statistical analysis
Values are expressed as the mean±standard error of the mean. The statistical significance was determined using the Student's t-test. Differences were considered to be statistically significant at p<0.05.
Results
Fabrication of a warp-knitted nitinol stent
The nitinol stent was fabricated successfully on a double-raschel warp-knitting machine using a nitinol wire of 76 μm in diameter. The superelastic phase of nitinol was achieved by heating the stent to 500°C for 15 min. After crimping (without tissue), the stent returned to its original diameter of 6 mm (data not shown).
Cytotoxicity and proliferation assay
The cytotoxicity of the warp-knitted nitinol stent was evaluated with regard to LDH release as illustrated in Figure 5A. The exposure of cells to the stent contact medium for 4 or 24 h showed no significant difference in LDH release compared with the untreated control cells (negative control).
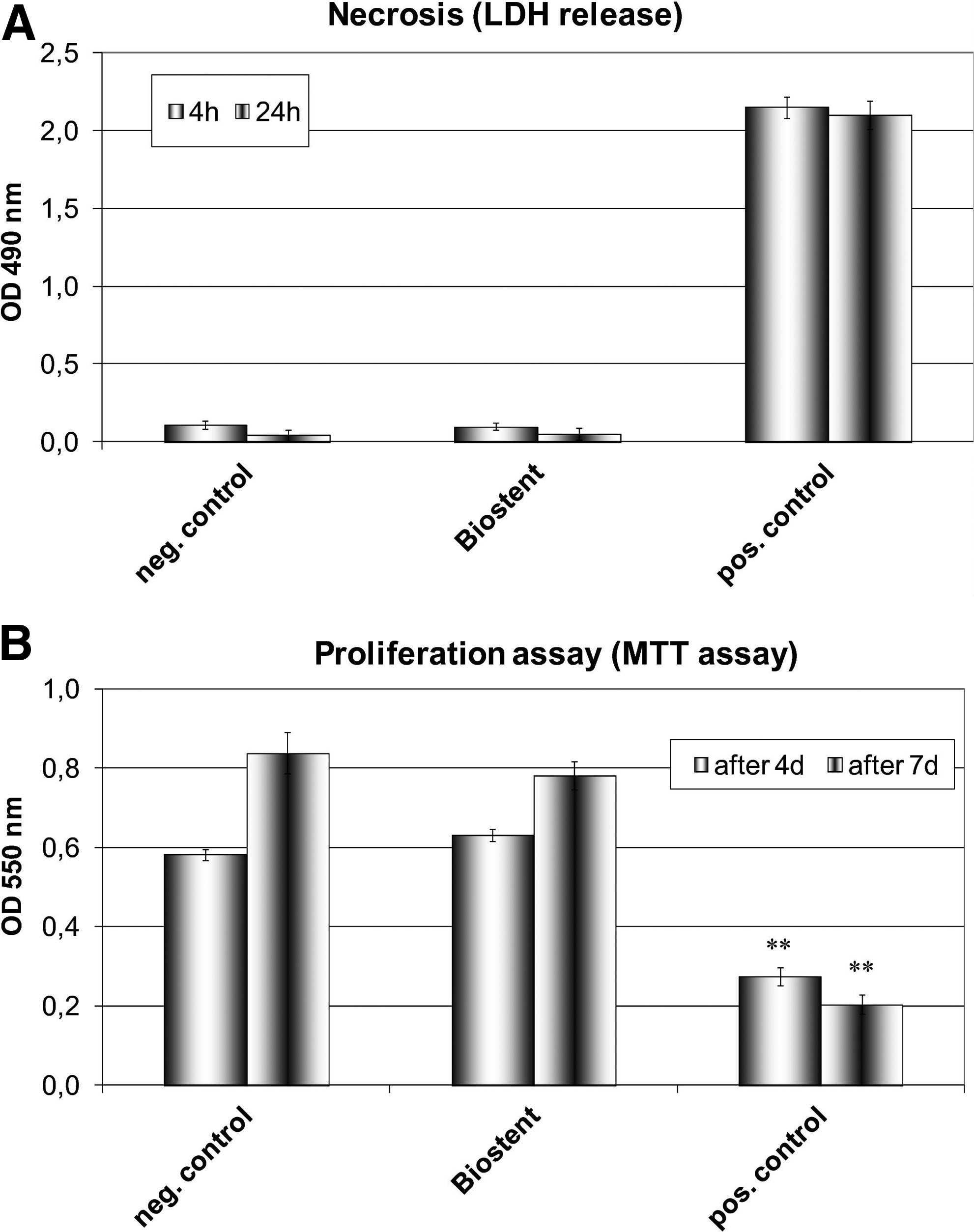
Cytotoxicity assays.
The effect of the nitinol stent on the proliferation of vSMCs was assessed using the MTT assay after 3 and 6 days. The stent contact medium did not cause any significant change in the proliferation of the cells compared with the untreated control (Fig. 5B).
BioStent moulding and tissue analysis
Gross and microscopic analysis demonstrated complete integration of the nitinol stent within cell-seeded fibrin as shown in Figure 6, with stent struts isolated from both the luminal and abluminal surfaces. The stent remained isolated from these surfaces following bioreactor conditioning, as the cell-seeded fibrin was replaced by newly synthesized tissue. The wall thickness of the BioStent before conditioning was 1.25 mm, whereas after bioreactor conditioning, the average wall thickness amounts to 348±18 μm.
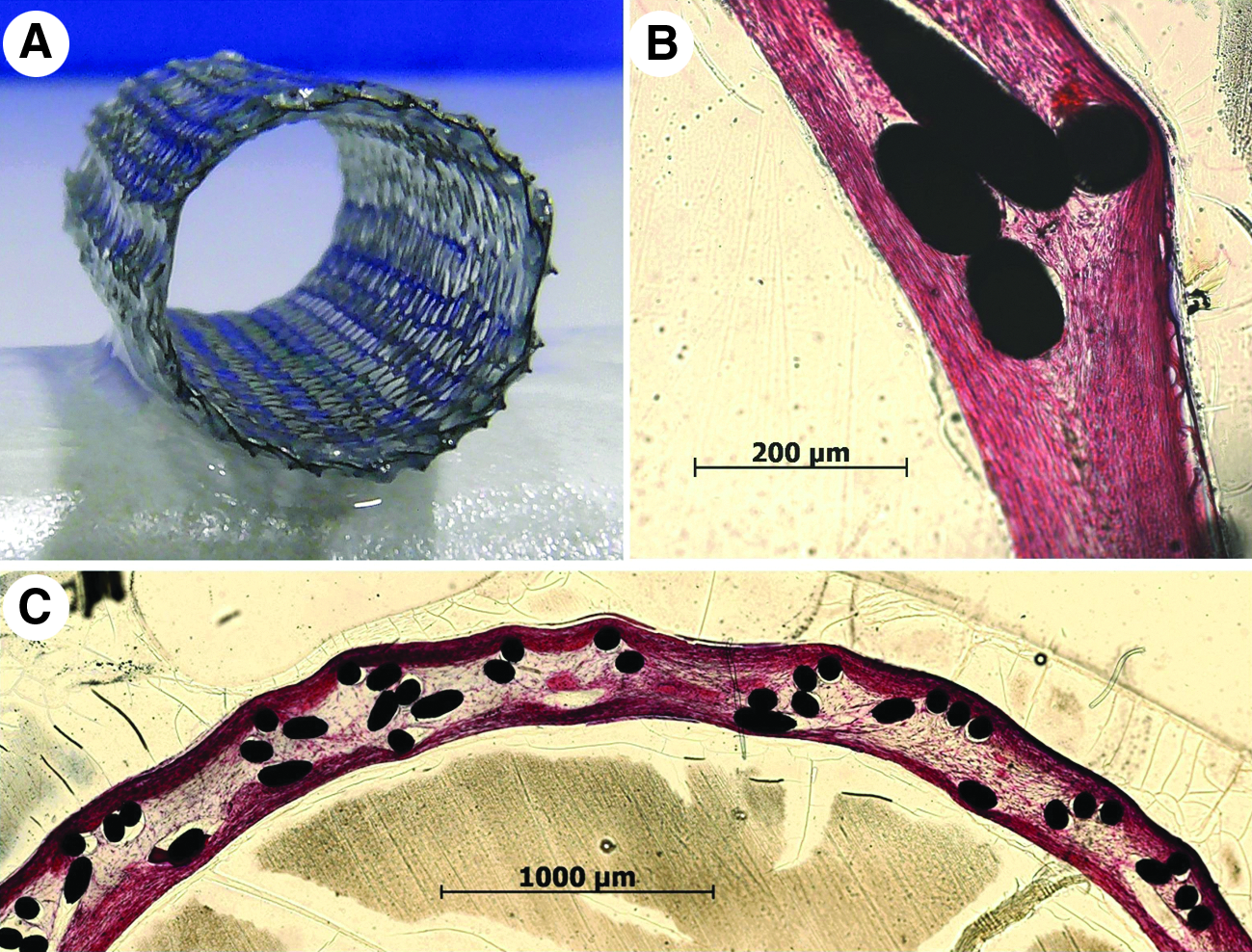
Complete coverage of the nitinol stent with fibrin gel and cells
Conventional histology
Tissue sections of 21-day-cultured BioStents were stained with H&E to demonstrate the tissue morphology (Fig. 6B, C). H&E staining revealed a dense, multilayered homogenous distribution of cells surrounded by connective tissue within the wall of the BioStents, with two collagen-rich tissue layers formed adjacent to the stent structure. All of the BioStents demonstrated a smooth luminal surface. Tissue developed to a lesser extent between the stent struts, but in general, the struts were embedded entirely in neotissue. The tissue thickness of the BioStent coating on either side of the stent material after conditioning was ∼10–60 μm. The total wall thickness of the BioStent was measured as 348±18 μm. No statistical relevant difference could be obtained.
Immunohistochemical staining
Alpha-SMA-positive staining in the walls of the BioStents revealed a rich, uniform distribution of vSMCs similar to native artery (Fig. 7A, B). There was also positive immunostaining for type III collagen (Fig. 7C, D), which was distributed primarily in the two layers adjacent to the stent structure.
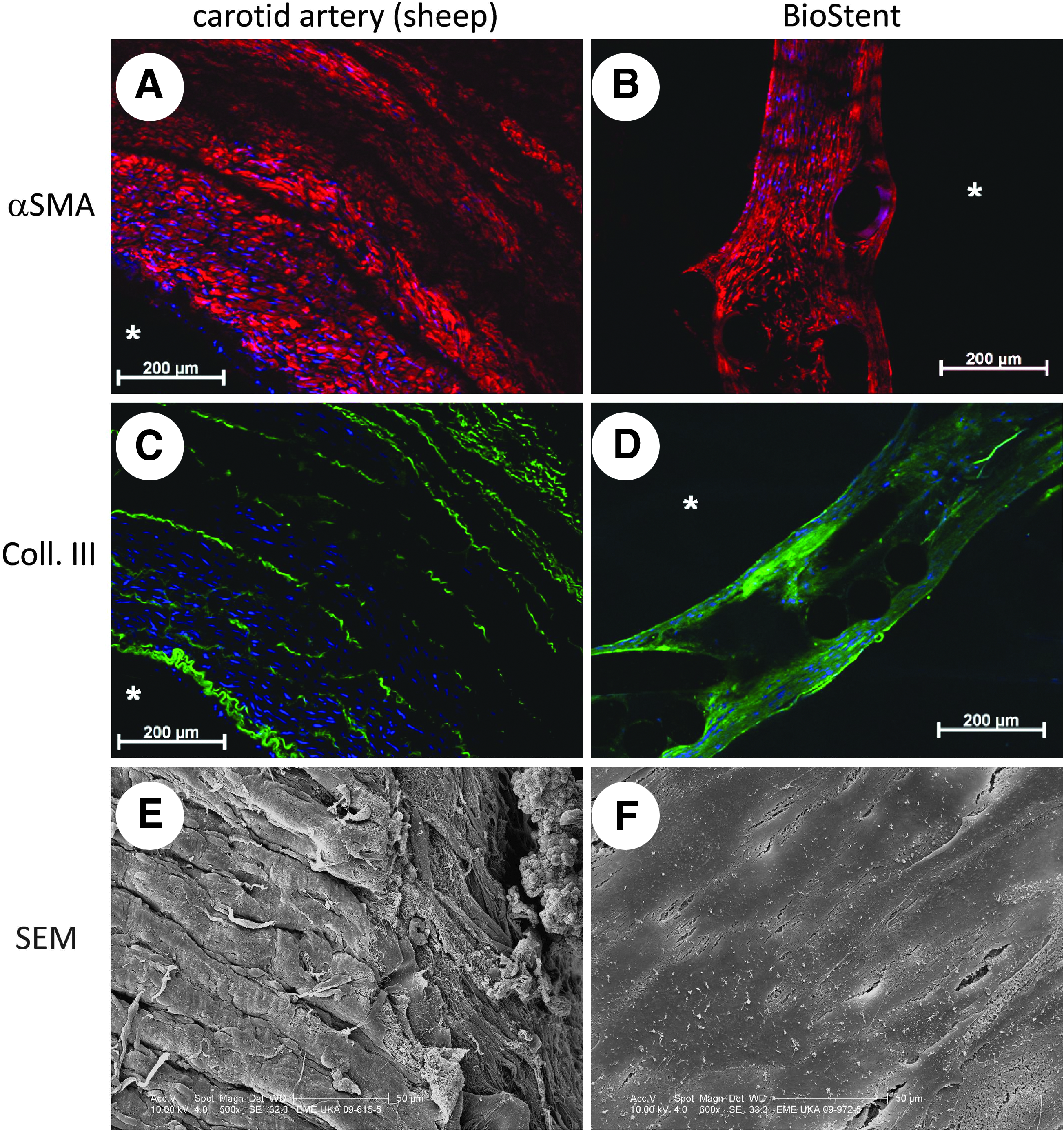
Immunohistochemical staining of PMMA-embedded sections of an ovine carotid artery and the BioStent.
Endothelialization
The development of an endothelial cell layer was observed after 4 days of conditioning in the bioreactor system (Fig. 7F). Compared with native carotid artery (Fig. 7E), the flattened endothelial cell layer was smoother and more regular. A number of minor tears were visible in the tissue-engineered endothelial cell layer.
Stent crimping
The crimping process was realized using a PTFE tubing inside a glass cylinder (Fig. 8). The BioStent was crimped to 12FR in diameter. After crimping, the endothelial cell layer exhibited slightly larger tears than those previously observed, although the surface maintained almost complete endothelial cell coverage.
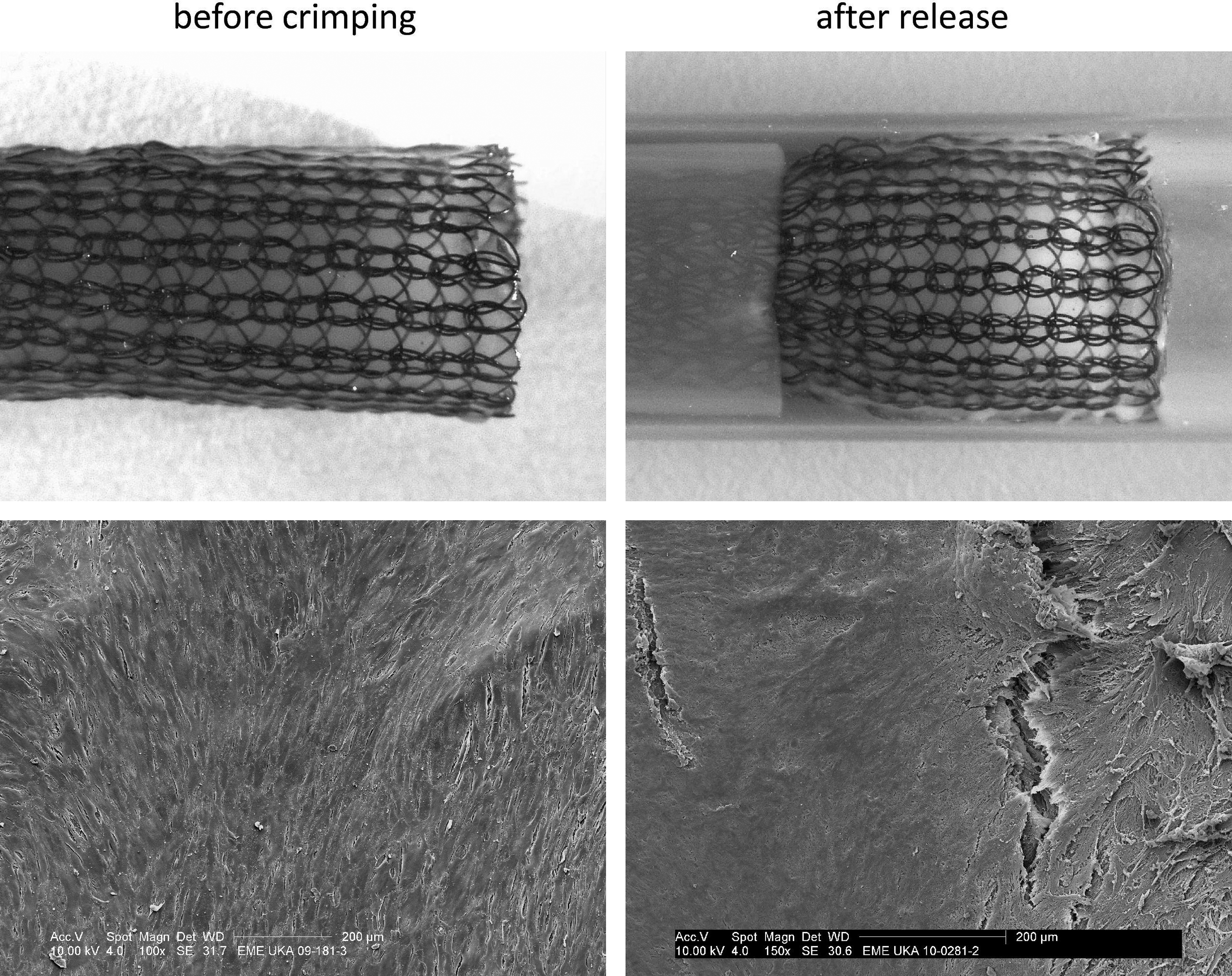
Precrimping and release of the BioStent with the corresponding SEM images of the endothelial cell layer.
Discussion
Almost 20 years ago, stainless steel stents were first used in stenting as an alternative to PTA for the treatment of atherosclerotic lesions in femoral arteries. However, the patency rate in stented arteries compared with those treated using PTA could not be improved.9,10 Steel stents were soon followed by self-expandable alloy stents, such as Elgiloy (Co-Cr-Ni) stents (Wallstent), which also failed to have an ameliorating effect on the patency rate. 2 To overcome the problem of material fatigue, self-expandable nitinol stents have been employed, leading to better patency rates compared with PTA in several clinical trials.1,3
However, a major limitation of stenting in the femoropopliteal region and lower leg arteries is in-stent restenosis. To solve this problem, a number of different approaches have been evaluated to improve the patency rates of current PTA, including drug-eluting balloons, drug-eluting stents, 11 bioabsorbable stents, 12 and covered stent grafts.13–15 Polyester-covered stent grafts were the first covered stents and demonstrated a low patency, significant thrombosis rates, and an inflammatory response in the femoropopliteal artery.16,17 The change of the coating material to expanded PTTE gave rise to the development of the FDA-approved Viabahn endoprosthesis. The Viabahn stent graft showed varying patency rates in femoropopliteal segments, ranging from low (49% after 6 months) 18 to high (93% after 1 year). 19 These studies involved low patient numbers (18 and 15, respectively), whereas larger patient studies (102, 87, and 80 stent graft-treated limbs) showed primary patency rates of 74%, 20 76%, 13 and 78.7% 21 after 1 year, respectively. Additionally, the primary patency rate of a Viabahn graft was similar to that of a PTFE bypass graft. 22 All of the aforementioned techniques to treat atherosclerotic peripheral arteries share a common complication, in that in-stent restenosis is still prevalent with regard to long-term outcome. As a result, intense research is ongoing in an effort to develop more biocompatible materials that could ultimately lead to improved patency rates.
Our current approach, BioStent, is based on the principles of tissue engineering and the premise that complete integration of a self-expandable nitinol stent within engineered tissue will prevent the inflammation and restenosis that is normally caused by deployment injury to the vessel wall. The engineered tissue of the BioStent surrounds the stent structure completely and prevents direct contact of the stent material with either the blood face or the surrounding vascular tissue and atherosclerotic plaques. The newly developed tissue should also prevent vascular cell ingrowth from the surrounding vessel and subsequent restenosis. In addition, a viable, luminal endothelial cell coating of the BioStent should reduce any risk of thrombosis and neointimal formation following stent deployment. These characteristic advantages may lead to improved patency rates following percutaneous transluminal stent angioplasty.
The stent material chosen as a backbone for the BioStent is nitinol. Nitinol has proven an excellent material in femoropopliteal stenting, leading to good patency rates in previous studies. Nitinol displays a number of excellent stent material properties, such as shape memory effect, enhanced radial strength, crush recoverability, and reduced foreshortening. These properties enable smooth release of the currently employed self-expandable stent, minimizing tear formation in the newly formed luminal endothelial cell layer. Considering the form of the warp-knitted nitinol stent, both side branches and stent length can be adapted to the required vessel anatomy during the knitting process. Further, fibrin gel can be easily polymerized in different geometries, so complete infiltration and coverage of the stent struts is possible. The tubing system of the bioreactor system can also be changed to accommodate differently sized BioStent structures.
The stent design was chosen due to both best fibrin gel coverage and a reduced stent foreshortening compared with other tested stent designs, resulting in less stretch and strain forces on the engineered tissue (Fig. 3). Further, the stent strut density of the warp-knitted stent is higher than that of other tested or commercially available stents (e.g., the WallStent). This stent strut density represents a better support for the engineered tissue around the stent struts, and is the major reason for selection of this design. Additionally, the BioStent structure has a larger contact area with the engineered tissue compared with laser-cutted (e.g., Absolute stent) or braided stents (e.g., WallStent) due to the knitting process. This procedure superimposes the used nitinol wire of 76 μm upon itself at least two times, leading to a larger tissue contact area. This stabilizes the tissue for the crimping process.
In addition to accommodating an integrated fibrin component, the Nitinol stent material performed well with regard to cytotoxicity and cell proliferation. The biocompatibility of nitinol as a material has previously been demonstrated using fibroblasts. 23 In the present study, carotid-artery-derived vSMCs were not significantly affected by the stent contact test medium. The assays employed in this study are normally used to detect chemical-induced cytotoxicity and proliferative effects, which do not illuminate the effect of direct stent contact. However, cytotoxic effects from direct stent contact can be disregarded as the vSMCs remained viable and proliferated in the direct vicinity of the stent struts, illustrating the biocompatibility of the nitinol stent.
After moulding and cultivation for 2 weeks, the BioStent is completely surrounded by newly developed tissue with an aligned cell population at the luminal and abluminal surfaces. The complete integration of the stent struts should prohibit the immunological response that is elicited by current state-of-art stents. Mimicking the natural environment with bioreactors affects the tissue development by increasing the transport of nutrients and waste products, improving cell attachment, altering cell orientation, and enhancing the production of extracellular matrix (ECM) proteins. 24 Histology and immunohistochemistry revealed favorable tissue development within the BioStents, including the production of type III collagen. Collagen is considered as an important load-bearing structure in vascular tissues. The mechanical loading applied by the bioreactor seems to result in a more active cell phenotype and a consequent remodeling of connective tissue. 25 This activation was demonstrated by induction of alpha-SMA, a known indicator for ECM remodeling, with a dense population of alpha-SMA-positive cells distributed uniformly throughout the stent section. Minimal alpha-SMA and type III collagen was expressed between the stent struts in the center of the BioStent tissue component, possibly due to inadequate mechanical stimulation or nutritional supply to these areas. However, the tissue on the outer (abluminal) side of the BioStent appears to be well developed. In the course of stent deployment, this outer tissue layer may result in reduced stent strut pressure against the vessel wall, thereby minimizing the injury at the diseased vessel section, and consequently reducing the potential for neointimal hyperplasia. However, the ends of such a stent graft would require some form of anchorage in the diseased vessel, which may cause injury at these points.
A further important consideration with the BioStent was that stent coverage thickness is minimized to reduce the potential luminal step in the vessel after stent implantation, which would result in different fluid dynamics at the stent ends. The thickness of a coated stent should be low enough to display equal-to-lower blood flow turbulences compared with those caused by uncoated stents. Further, the coated stent thickness should still be sufficient to allow a gentle implantation of the stent into the vessel and avoid subsequent intimal hyperplasia. Nakayama reported the first in vivo tissue-engineered biocovered stent with a coverage thickness of ∼1 mm 26 compared with ∼0.5 mm of the autologous vein-covered stent described by Stefanadis. 27 The tissue thickness of the BioStent coating on either side of the stent material after conditioning was ∼10–60 μm. With the strut thickness and the warp-knitting form taken into consideration, the total thickness of the BioStent was measured as 348±18 μm. Before conditioning, the wall thickness has been larger (1.25 mm), since the evoked cells start remodeling of the tissue during conditioning. This leads to an enlargement of the BioStent lumen. Optimization of the knitting technique needs to be addressed in the future to realize a further reduction of the wall thickness.
Regarding the luminal coverage of the BioStent, a smooth, confluent endothelial cell layer was evidenced by SEM. To evaluate any changes due to stent crimping, the BioStents were crimped using a standard application procedure by withdrawing the stent into a catheter (12FR) and subsequently deploying it into a glass cylinder (Ø=6 mm). A number of small tears in the endothelial layer were visible after crimping, which would be expected to heal readily in vivo.
The current feasibility study demonstrates that the BioStent concept can be employed to integrate stent materials within a protective engineered tissue structure. Bioreactor conditioning was used successfully to replace the cell-seeded fibrin component of the BioStent with viable vascular tissue. The complete integration of the stent material will ultimately prevent direct stent contact with either the blood face or the surrounding vascular tissue and atherosclerotic plaques. The newly developed tissue should also prevent vascular cell ingrowth from the surrounding vessel and subsequent restenosis, while a viable, luminal endothelial cell coating should reduce any risk of thrombosis and neointimal formation following stent deployment.
To exclude problems of hemocompatibility, animal studies are going to be performed, since the autologous tissue coverage will prevent the nitinol wire from being exposed to the blood flow. Since fabrication techniques are similar, the BioStent study is comparable to a vascular graft study already published in Biomaterials. 28 In this study we could show that n=6 explanted grafts were patent in each of the investigated groups after 1, 3, and 6 months, with one significant stenosis in 1 explant (3 months). This indicates that the autologous tissue in most of the cases prevents hemocompatibility problems.
In addition to applications in the vascular system, the BioStent concept is a platform technology, which can be transferred to other clinical stent applications depending on the cell type required on the luminal surface (e.g., ureter/urethra, esophagus, endobronchial applications, and bile duct).
In conclusion, the BioStent concept offers a novel opportunity to generate a viable, self-expanding stent structure with a functional endothelial cell lining. Further investigation will evaluate the performance of the novel stent design in vivo, with autologous cells employed to generate patient-specific neotissue.
Footnotes
Acknowledgments
Funding was provided by IZKF Aachen (Interdisziplinary Centre for Clinical Research) of the Medical Faculty of the RWTH Aachen University and by the German Research Foundation (DFG) within the excellence initiative. The authors wish to thank Angela Freund and PD Dr. Ralf Smeets from the Department of Oral and Maxillofacial Surgery, University Hospital Aachen, for their help in sawing and grinding histology techniques. Additionally, we are grateful to the Department of Pathology, University Hospital Aachen, especially Peter Verken, for supporting us with equipment and technical expertise.
Disclosure Statement
No competing financial interests exist.