
Abstract
The repair of abdominal wall defects following surgery remains a difficult challenge. Although multiple methods have been described to restore the integrity of the abdominal wall, there is no clear consensus on the ideal material for reconstruction. This study explored the feasibility of in vivo reconstruction of a rat model of an abdominal wall defect with a composite scaffold of tenocytes and porcine small intestinal submucosa (SIS). In the current study, we created a 2×1.5 cm abdominal wall defect in the anterolateral abdominal wall of Sprague-Dawley rats, which were assigned into three groups: the cell-SIS construct group, the cell-free SIS scaffold group, and the abdominal wall defect group. Tenocytes were obtained from the tendons of rat limbs. After isolation and expansion, cells (2×107/mL) were seeded onto the three-layer SIS scaffolds and cultured in vitro for 5 days. Cell-SIS constructs or cell-free constructs were implanted to repair the abdominal wall defects. The results showed that the tenocytes could grow on the SIS scaffold and secreted corresponding matrices. In addition, both scaffolds could repair the abdominal wall defects with no hernia recurrence. In comparison to the cell-free SIS scaffold, the composite scaffold exhibited increased vascular regeneration and mechanical strength. Furthermore, following increased time in vivo, the mechanical strength of the composite scaffold became stronger. The results indicate that the composite scaffold can provide increased mechanical strength that may be suitable for repairing abdominal wall defects.
Introduction
In the United States, biological materials, such as the pig small intestinal submucosa (PSIS), pig skin acellular dermal matrix (PADM), human skin acellular dermal matrix, and cow pericardium, have been available commercially for abdominal wall reconstruction for more than 10 years and shown promise in the management of these defects. 11 Two of the most commonly used biological materials are PSIS and PADM. Although both materials exhibit better degradation and less or no immunological response, the ability to promote the regeneration of blood vessels is different, which is believed important to improve the reconstruction and enhance resistance to infection and contamination. 12 Our previous studies have shown that SIS is better in regeneration of blood vessels than ADM. 13 There are few published data addressing whether ADM can secrete cytokines to accelerate early revascularization. 11 How to make biological materials used in abdominal wall defects better revascularization is still an important area that needs to be further studied.
Biomechanical properties are very important for biological materials applied in abdominal wall defects, which should not only incorporate into the tissue adjacent to the scaffold over time, but should also be strong enough to withstand the pressure of the abdominal contents. Several investigators have demonstrated that multilaminate SIS provides the initial mechanical strength appropriate for repairing abdominal wall defects.14,15 A review of biological meshes used in abdominal wall hernia repairs reported that ADM has a 0%–100% recurrence rate and the SIS exhibits low recurrence rates in clean fields, but in infected fields, the recurrence rate could be up to 39%. 16 Therefore, to maintain or increase the mechanical strength of biological materials in reconstruction of abdominal wall defects is another very important issue that needs further research, which may allow an effective solution for the repair of abdominal wall defects.17,18
Tissue engineering offers a promising approach for the reconstruction of abdominal wall defects with the correct mechanical properties, biocompatibility, and biodegradability. Collagen-based matrices have been broadly used for tissue engineering scaffolds, such as blood vessels, 19 ADMs, 20 and SIS.21,22 SIS is widely applied as a biodegradable scaffold in tissue engineering of various tissues of the urogenital, vascular, and musculoskeletal systems.22–25 Various studies have been performed to prove the feasibility of SIS as a tissue engineering scaffold in animal models of rats, dogs, and pigs, and even human patients.25–28 Different types of seed cells have been used for repairing abdominal wall defects, including skeletal muscle, skin fibroblasts, and bone marrow stem cells.21,25,29 However, there have been no published reports on the use of tenocytes to engineer aponeurosis for potential applications in abdominal wall reconstruction. Recent studies have revealed that the tendon and tendon sheath defects can be successfully repaired with a tissue-engineered tendon and tendon sheath using polyglycolic acid fibers and the corresponding cells in a hen model, with good biocompatibility and mechanical properties.30,31 The most important cause of abdominal wall defects, especially in hernias, is a loss of tissue of the aponeurosis of obliquus externus abdominis and/or transverse fascia. Considering that both of these tissues are similar to tendons, and exhibit stronger mechanical properties, increasing the strength of the abdominal wall by implanting a composite scaffold was explored in this study. We applied tissue engineering methods to repair abdominal wall defects in a rat model of an abdominal wall defect. We hypothesized that a cell-SIS construct could be used successfully in repairing abdominal wall defects with lower complications (recurrence, adhesion, and infection) than cell-free SIS constructs.
Materials and Methods
Animals and experimental design
All experiments on Sprague-Dawley rats (150–200 g) were approved by the institutional review committee of Shanghai Jiao Tong University School of Medicine. A self-controlled study was conducted. We created a 2×1.5 cm abdominal wall defect in each side of the anterolateral abdominal wall of the rats, a cell-SIS construct or a cell-free SIS scaffold was applied to the two abdominal wall defects in the experimental rats. Three groups were included in this study: (1) the experimental group (n=14) that received a cell-SIS construct; (2) the scaffold control group (n=14) that received a cell-free SIS scaffold; and (3) the blank control group (n=6) where the abdominal wall defect was left unrepaired. All test animals were sacrificed, respectively, at 5 and 9 weeks postsurgery (seven from the experimental and scaffold control group for gross view, a histological examination, a biomechanical test, and a scanning electron microscopy [SEM] observation). In addition, the blank control group (n=6) was sacrificed at 9 weeks for gross observation of herniation.
Preparation of SIS
SIS was prepared from fresh porcine jejunum as previously described. 32 In brief, a segment of fresh porcine jejunum was obtained from a local slaughterhouse. After removing the intestinal contents, the small intestine was cut into lengths of ∼10 cm each. First, the SIS scaffold was obtained by mechanical removal of the mucosa, muscularis externa, and serosa. Second, the SIS scaffold was incubated in 0.05% trypsin for 12 h and continuously rinsed with distilled water to remove the trypsin. Third, the SIS sheet was further treated with 0.5% sodium dodecyl sulfate for 4 h and rinsed with distilled water three times each. All samples were vacuum-sealed in hermetic packaging, sterilized by gamma irradiation (25KGY), and stored at 4°C until needed. Hematoxylin and eosin staining (H&E) was performed to examine whether host cells were present on the SIS (Fig. 1B). SEM was used to examine the surface morphology of SIS (Fig. 1C, D).
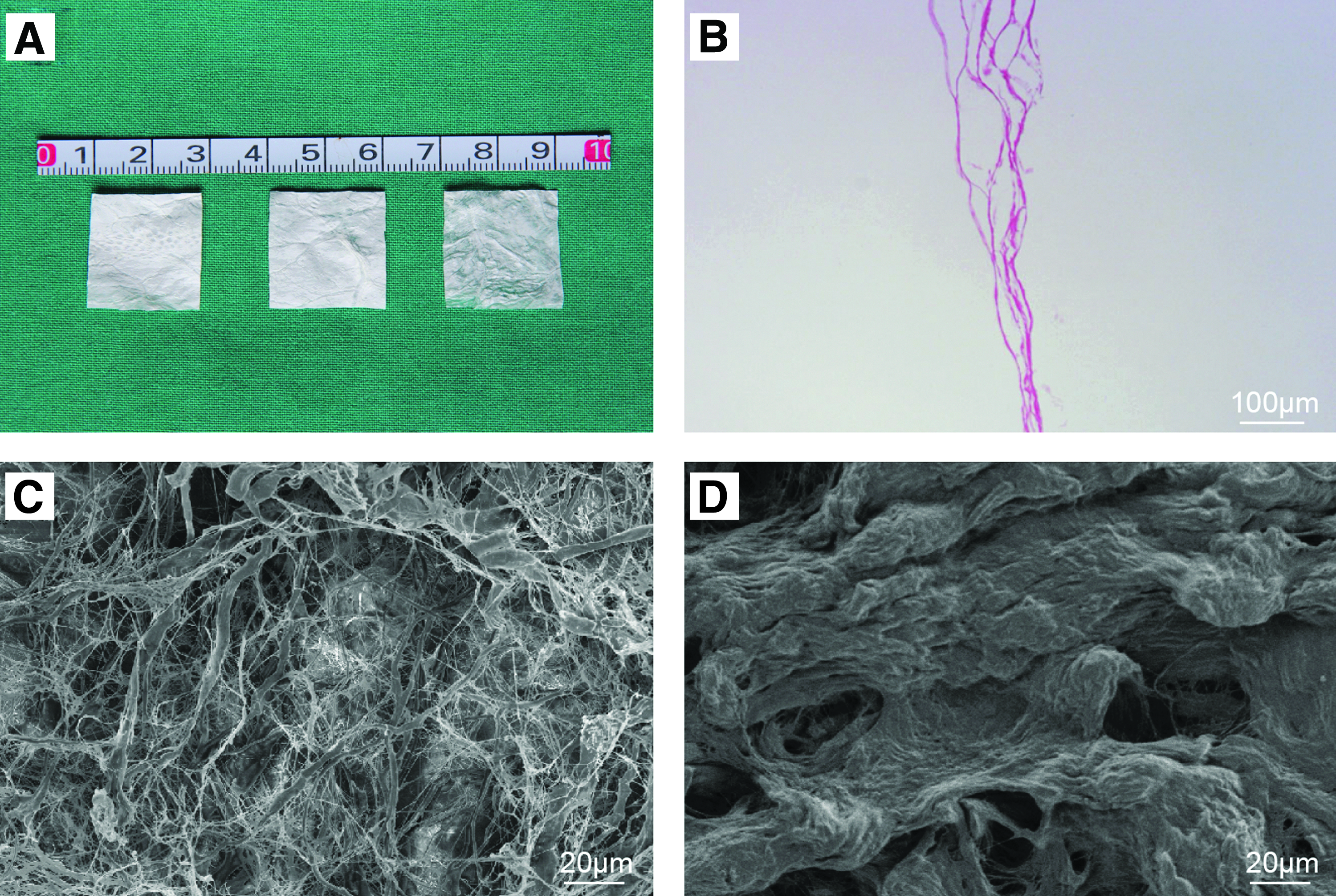
Characteristics of small intestinal submucosa (SIS).
Cell isolation and culture
Tendon tissues were isolated under sterile conditions from the flexor digitorum profundus tendons of the rat limbs. The harvested tissues were immediately placed in 10-cm culture dishes, washed with phosphate-buffered saline three times, and soaked in chloramphenicol for 10 min. The tendon tissues were cut into 1×1×1 mm pieces and the resulting fragments were digested in 0.2% type-I collagenase for 3 h. The mixture was centrifuged at 1500 rpm for 5 min. The supernatant was discarded and the cell pellet was resuspended in the Dulbecco's modified Eagle's medium (DMEM) containing 10% fetal bovine serum (FBS, Gibco),
Immunofluorescent staining
To examine proliferation and collagen secretion from tenocytes, the third passage tenocytes were fixed with 4% paraformaldehyde for 30 min, washed with phosphate-buffered saline (PBS) three times, and then preincubated with PBS containing 10% normal goat serum for 60 min to minimize nonspecific signals. They were then incubated overnight at 4°C with the following primary antibodies in their respective dilutions: anti-Ki67 (1:100, ab66155; Abcam), pro-collagen (1:100, sc8787; Santa Cruz Biotechnology). After the cells were washed with PBS, they were incubated for 1 h at 37°C with secondary antibodies: Alexa Fluor 555-conjugated goat anti-rabbit IgG (1:1000) for Ki67 and Alexa Fluor 488-conjugated goat anti-rat IgG (1:1000) for pro-collagen. All specimens were examined with a confocal laser scanning microscope. Ki67-positive cells or pro-collagen-positive and 4,6-diamino-2-phenyl indole-stained cells were counted by Image-Pro Plus 6.0 and analyzed with three high-power fields (×100).
SIS scaffold preparation and cell seeding
The sterilized SIS was cut into scaffolds of ∼2×2 cm under sterile conditions (Fig. 1A), and immersed into DMEM containing 10% FBS in 10-cm culture dishes in a 5% CO2 incubator at 37°C for 12 h. Before cell seeding, the medium was removed and the scaffolds were dried using sterile filter paper. Third passage tendon cells (2×107/mL) were digested with 0.25% trypsin and seeded into three layers of the SIS sheet. The cell–scaffold constructs were immersed in DMEM containing 50% FBS for 4 h, following which DMEM containing 10% FBS was added and replaced every 24 h. The cell–scaffold constructs were cultured for 5 days in vitro to allow the cells to adhere and proliferate in SIS before implantation. For nonseeded scaffolds, the samples were immersed in the same culture medium during the rehydration and seeding periods (Fig. 2A).
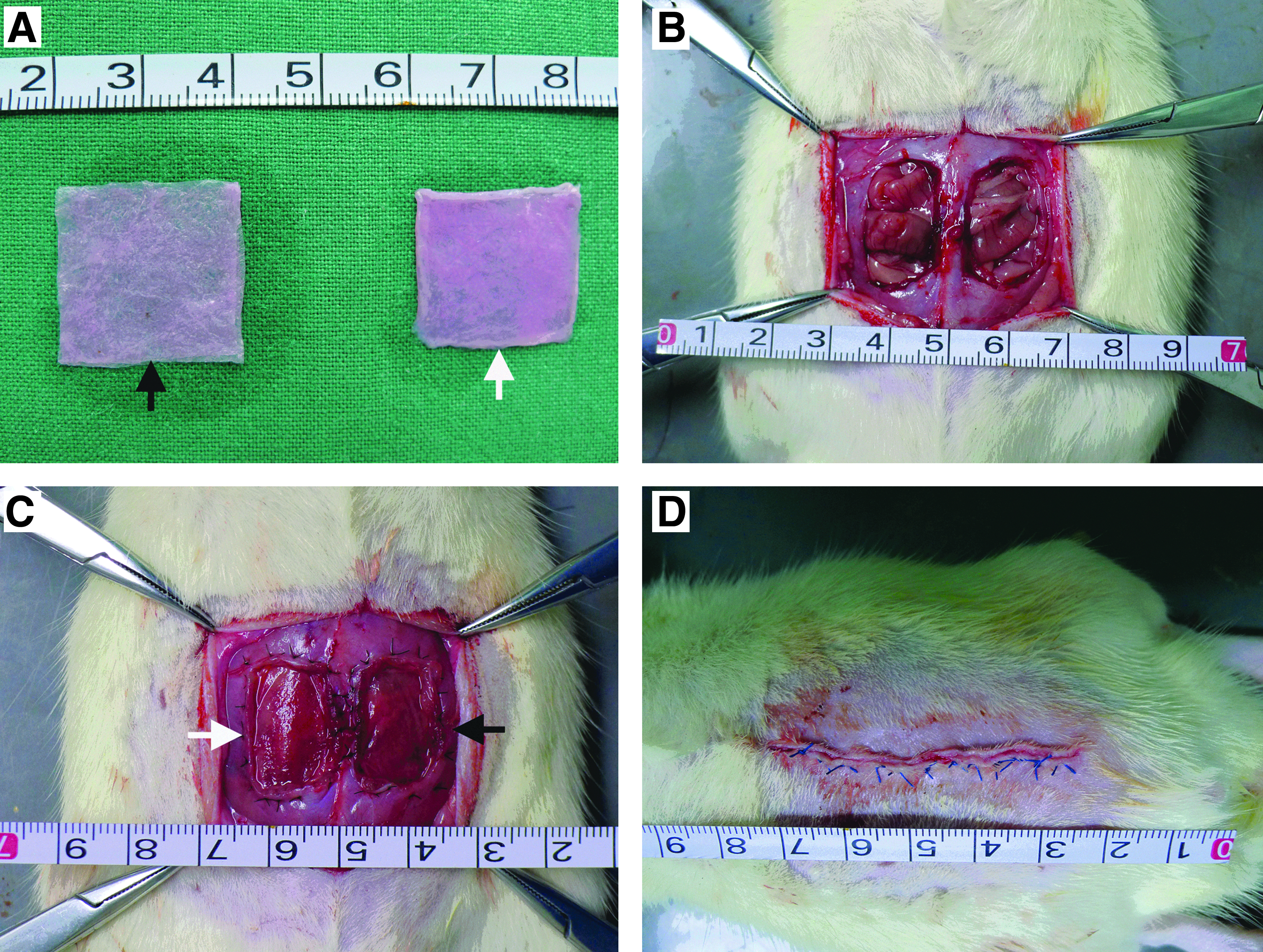
The process of repairment of abdominal wall musculofascial defect with two scaffolds.
SEM examination
After 5 days of culture in vitro, part of the cell–scaffold constructs were prepared for SEM examination as previously reported. 31 Briefly, samples were prefixed with 2% glutaraldehyde for 2 h at 4°C, washed twice with PBS, and postfixed in 1% osmicacid for 2 h at 4°C. After two washes with PBS, the samples were dehydrated with gradient ethanol and dried to a critical point. The samples were then mounted, sputter-coated with gold, and examined under a SEM (Philips-XL-30).
Surgical procedure and evaluation
For the creation of the abdominal wall musculofascial defects, rats were anesthetized by intraperitoneal injections of 10% chloral hydrate (4 mL/kg). The abdominal wall was shaved, disinfected, and covered with sterile draping. A longitudinal skin incision (4–5 cm) was made to expose the surgical area (Fig. 2D). An abdominal wall musculofascial defect (2×1.5 cm) involving the fascia, obliquus externus abdominis, and the peritoneum was then created (Fig. 2B), following which the cell-SIS scaffold was used to the right ventral lateral abdominal wall and the cell-free scaffold was applied to the left side (Fig. 2C). The scaffolds were sutured directly to the edge of the musculofascial defect using simple interrupted silk sutures (Fig. 2C). About 6-0 silk sutures were used to suture the edge of the defect to the implanted scaffold and 3-0 absorbable sutures were applied to close the skin (Fig. 2C, D).
Every week, animals were checked for local or systemic complications, including seroma, hernia, and death. The dehiscence was observed at 5 and 9 weeks after implantation. We graded the adhesions on a numerical score from 0 to 4 according to the following criteria: 0, no adhesions; 1, thin and filmy adhesions easily separable by blunt dissection; 2, definite localized adhesions; 3, definite multiple visceral adhesions; and 4, dense adhesions extending to the abdominal wall. 33
Histological and immunohistochemical examination
Rats were sacrificed by high-dose chloral hydrate followed by cervical dislocation at 5 and 9 weeks postsurgery to harvest the scaffold and surrounding tissue. The tissues were fixed overnight in 4% paraformaldehyde, dehydrated with 95% alcohol for 12 h, and paraffin-embedded and cut into 6–8-mm thickness sections for H&E staining and Masson trichrome staining to examine the tissue structure, particularly for cell density and neo-blood vessels. To assess the neovascularity and immunologic reaction of the repaired site, the samples were analyzed using immunohistochemistry for the Von Willebrand Factor antibody (VWF) and CD45 in both groups. The slides were treated with 0.3% hydrogen peroxide for 10 min to block endogenous peroxidase, blocked with 2% bovine serum albumin, and then incubated with the rabbit anti-rat monoclonal antibody VWF (1: 3000 dilution, ab6994, Abcam) and the rabbit anti-rat monoclonal antibody fo CD45 (1: 500 dilution, ab10558, Abcam) for 2 h at 37°C. After three washes with PBS, the slides were incubated with goat-rabbit IgG conjugated with horseradish peroxidase for 1 h, and finally color developed with Liquid DAB Substrate Chromogen System.
Transmission electron microscopic examination
The rats were randomly sacrificed at 5 and 9 weeks. The harvest tissues were prepared for examination under a transmission electron microscope (TEM) (Philips-CM-120) to examine the distribution of collagen fibrils.
Biomechanical testing
The tissue samples (1×3 cm) obtained from the rats (5 and 9 weeks) were submitted to mechanical testing using a biomechanical analyzer (Instron) to measure the mechanical properties. The length of the tested scaffold was set at 1 cm between two grippers, which were gradually moved at a speed of 25 mm/min until complete rupture of the scaffold to obtain the maximal loading data.
Statistics
All results are presented as mean±standard deviation. Comparisons between groups were performed by the paired student's t-test, and the difference in the collagen fibril diameter and maximal loading were analyzed using the one-way ANOVA test. A p value<0.05 was considered statistically significant. SPSS 16.0 software was applied in statistical analysis.
Results
Cell culture and immunofluorescent staining
Primary tenocytes were successfully isolated from rat tendon tissues by enzymatic digestion, which exhibited similar fibroblast-like morphology and good proliferative ability (Fig. 3A). After subculture, the passaged cells proliferated rapidly and were able to secrete the extracellular matrix, especially for pro-collagen fibrils (Fig. 3B, C).
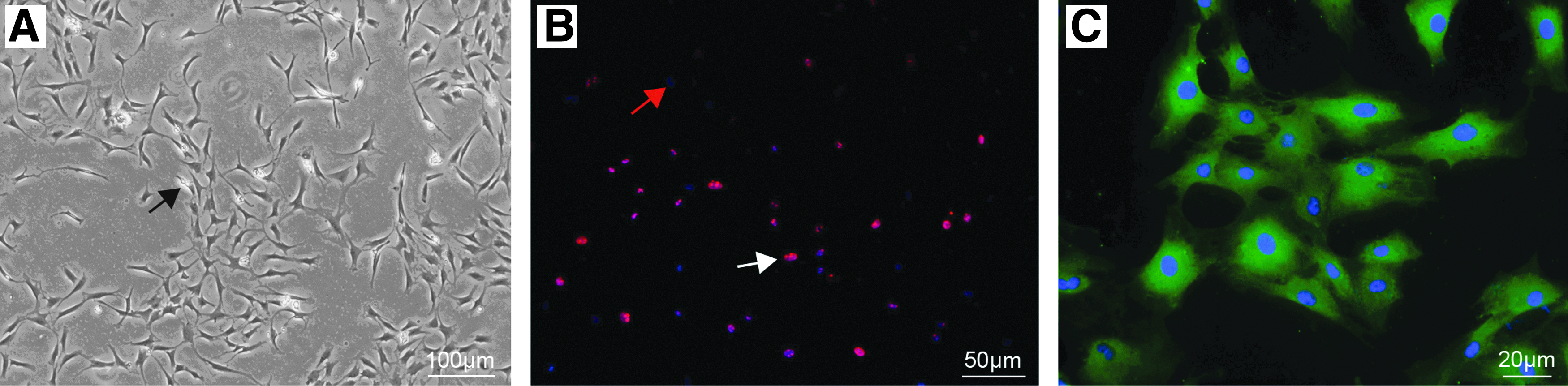
Primary tenocytes and related measurement.
Since a considerable lot of tenocytes should be prepared before the construction of tissue-engineered scaffolds, the proliferative ability is critical for obtaining a sufficient number of tenocytes. Therefore, tenocytes were stained for the proliferating cell marker, Ki67, to detect the proliferated capacity. As shown in Figure 2B, Ki67-positive cells (0.55±0.02) have good proliferative capacity.
Tenocytes are able to synthesize collagen types (I, III, V, and VI), and collagen Type I is the most abundant form of collagen. 33 Pro-collagen type I considered as the precursor protein is the main existence form in early time. Immunofluorescence labeling with the anti-procollagen type I antibody revealed that the presence of pro-collagen type I was mostly around the nucleus and exhibited a strong light reflection with a green color.
SEM of cell-SIS constructs
When the cells reached the required number, the tenocytes were seeded on SIS scaffolds. After culturing in vitro for 5 days, a membrane-like scaffold was obtained (Fig. 2A). The SEM results showed that the tenocytes could adhere to the SIS scaffolds (Fig. 4). In addition, we observed that the surface morphology of SIS was different between the two sides. Close to the serosa layer, pores were much more abundant and bigger in size than the corresponding opposite side (Fig. 4).

SEM images of the surface morphology of the tenocyte-SIS scaffold 2 days after seeding.
Gross observation
In this study, all rats survived the surgery without signs of herniation and dehiscence in both the experimental and scaffold control groups (Fig. 5A). The rats in the blank control group, without the implantation of the scaffold, developed herniation. The scaffolds were integrated in the host tissues and showed different degrees of degradation at 5 and 9 weeks. Adhesion was observed in the repaired sites at each time point (Fig. 5B). Compared with the cell-SIS scaffold, the tenocyte-SIS scaffold either had no adhesion or slight and thin adhesion that was easily separable at the repaired sites (p<0.05) (Fig. 4C).
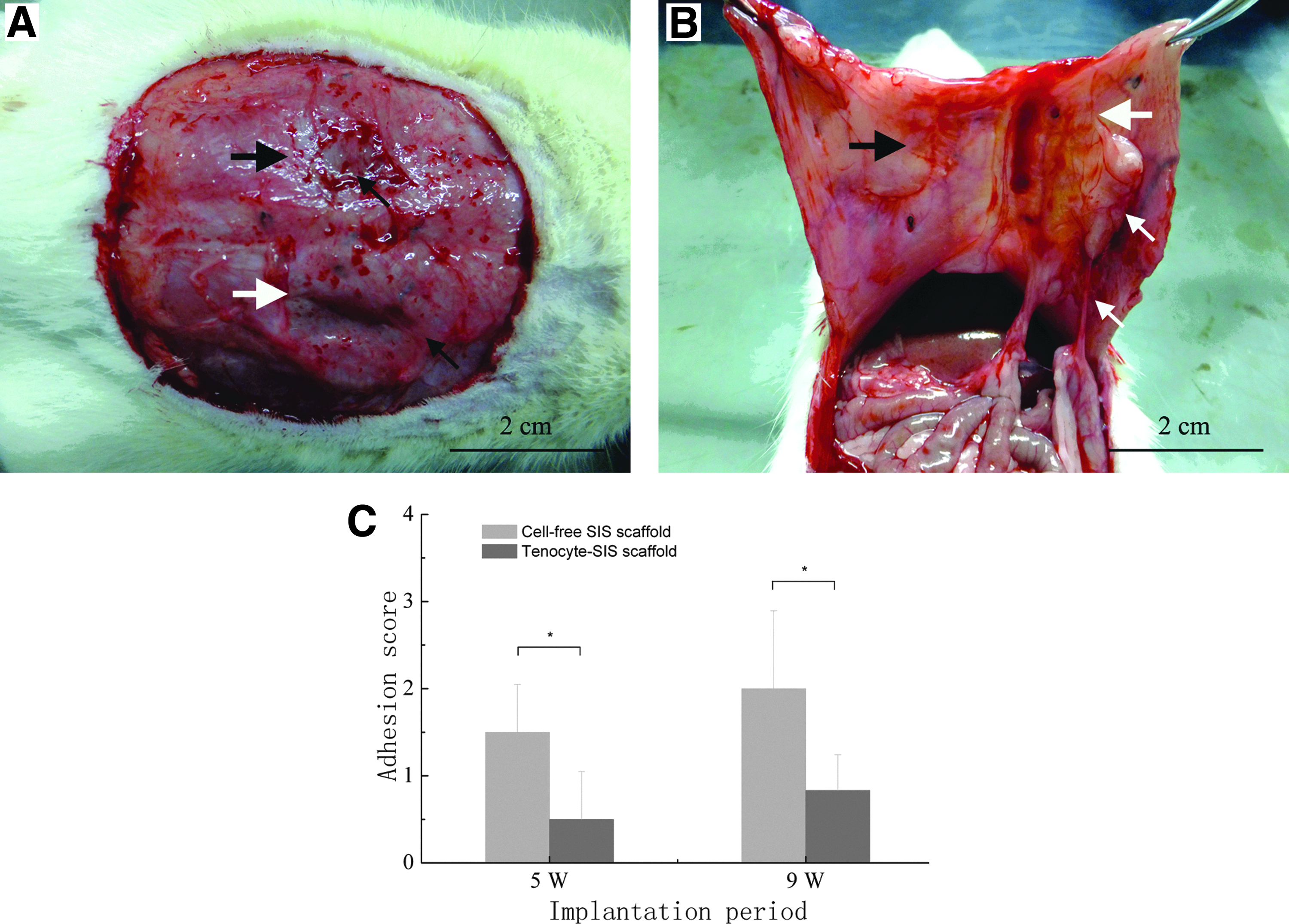
Intra-abdominal adhesion formation after abdominal wall defect repair at 5 and 9 weeks postsurgery.
Biomechanical property
To analyze the mechanical properties of the implanted scaffolds, fresh specimens, including the implanted scaffold and the 0.5 cm peripheral musculofascial tissues, were harvested at 5 and 9 weeks postsurgery and submitted to breaking-strength testing using a biomechanical analyzing instrument. The maximal loading showed no significant difference at the different time points (p>0.05). The elastic modulus of the experimental group showed 2.27±0.34 at 5 weeks and 2.96±0.25 at 9 weeks. In contrast, the scaffold control group showed 1.56±0.25 and 2.03±0.23 at 5 and 9 weeks (p<0.05) (Fig. 6).
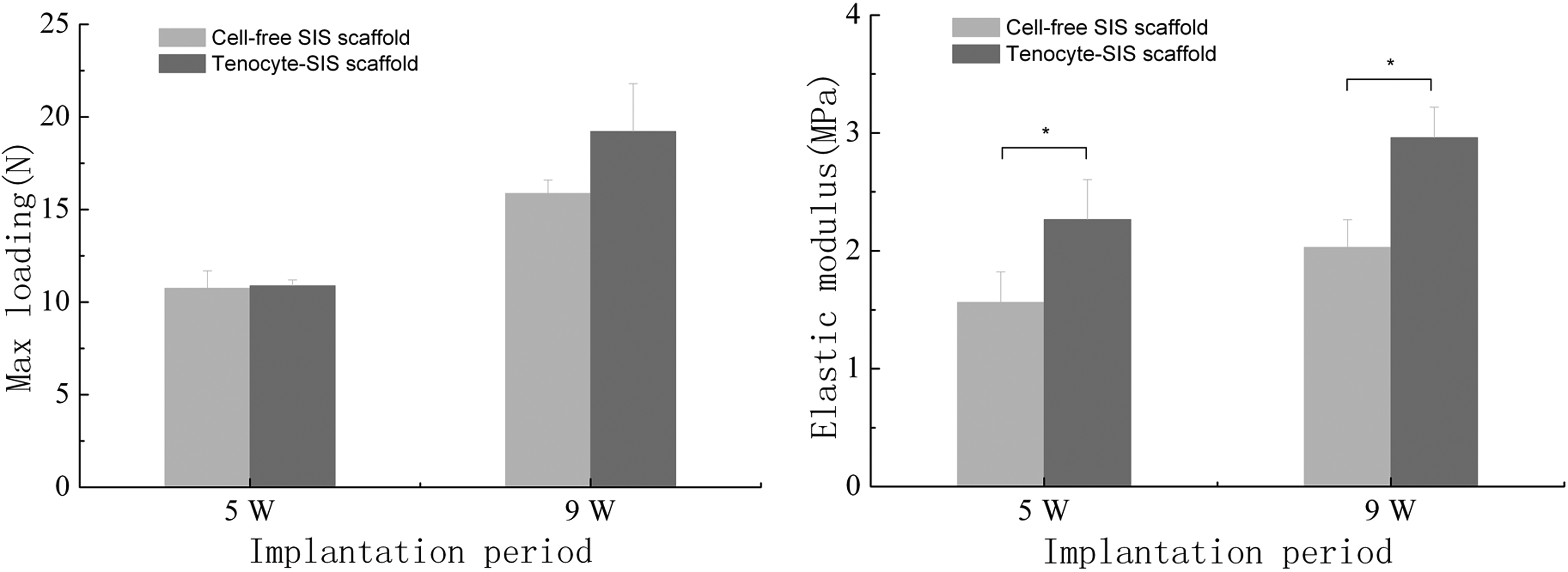
Maximum loading and the elastic modulus were used to evaluate the mechanical properties at 5 weeks and 9 weeks postsurgery. A significant difference was seen in the elastic modulus (p<0.05) and no significant difference was seen in maximum loading (p>0.05). *p<0.05.
Distribution of collagen fibrils
One specimen was randomly chosen for TEM examination at each time point. Irregular collagen fibrils were observed around the tendon cells at 5 weeks (Fig. 7A, B). The fibrils became thickened and regular at 9 weeks (Fig. 7C).

Transmission electron microscope images of the distribution of the collagen fiber in the tenocyte-SIS scaffold, 5
Histological and immunohistochemical analyses
To determine cell infiltration, SIS degradation, and vessel formation, the rats were sacrificed at 5 and 9 weeks for H&E and Masson trichrome staining to observe the structure of the implanted scaffold and the newly formed tissue. Cell infiltration was seen in both junctional and central regions 5 weeks after implantation. However, the black arrow indicates that cell infiltration of the middle layer of a cell-free construct was not sufficient (Fig. 8D, H). No significant difference was observed in cell infiltration in the junctional region at 5 weeks and any region at 9 weeks. Masson trichrome staining could obviously reveal the distribution and degradation of collagen fibers of SIS. Most of the collagen fibers were still present 9 weeks after implantation (Fig. 8M, N, O, P). In addition, the quantification of vascular results showed that high-density angiogenesis was observed in the tenocyte-SIS scaffold compared with the cell-free SIS scaffold at 9 weeks after implantation, especially in the central region of the tenocyte-SIS scaffold (Fig. 8J, N) (Fig. 9). However, a similar degree of neovascularization was found in two scaffolds at 5 weeks after implantation (Fig. 9). The above findings were further confirmed by the results of immunohistochemical staining for VWF, as shown in Figure 10. The tenocyte-SIS scaffold showed a significantly greater degree of vascularization than the cell-free SIS scaffold at each time point. Immunohistochemical staining results for CD45 showed that a slight or less inflammatory response was found at two time points, especially at 9 weeks after implantation (Fig. 11).
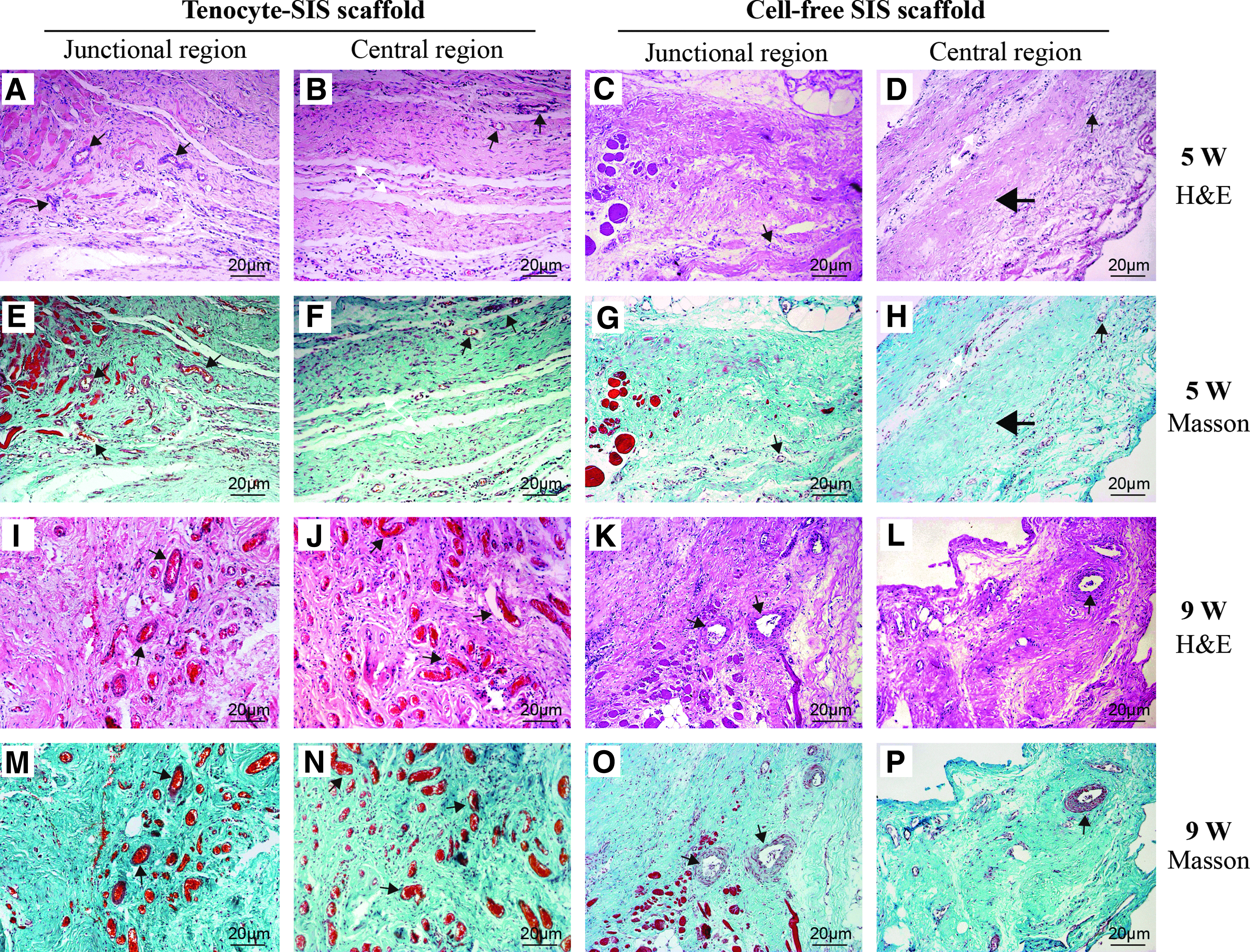
Histological images of the tenocyte-SIS scaffold and cell-free SIS scaffold after 5 and 9 weeks implantation. H&E staining
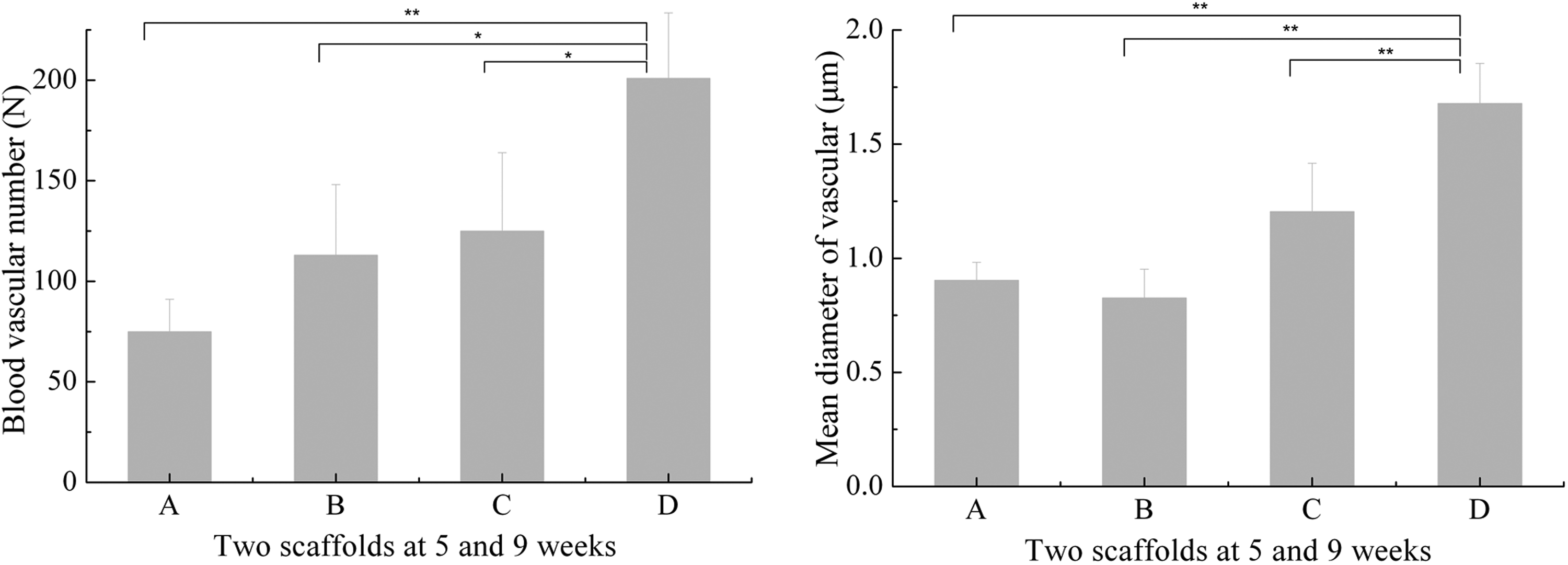
The blood vascular number and mean diameter vascular of two scaffolds at 5 and 9 weeks after implantation.
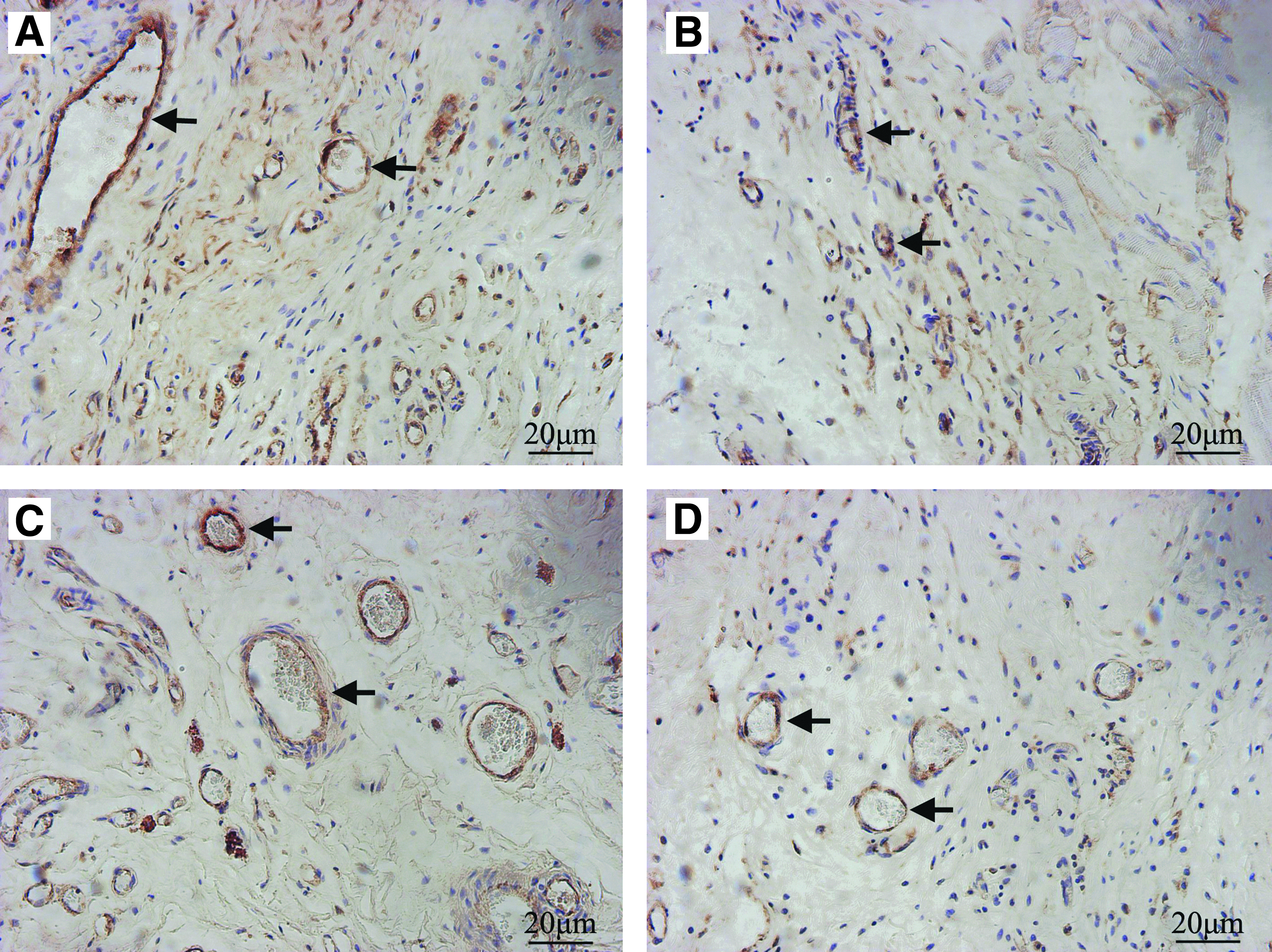
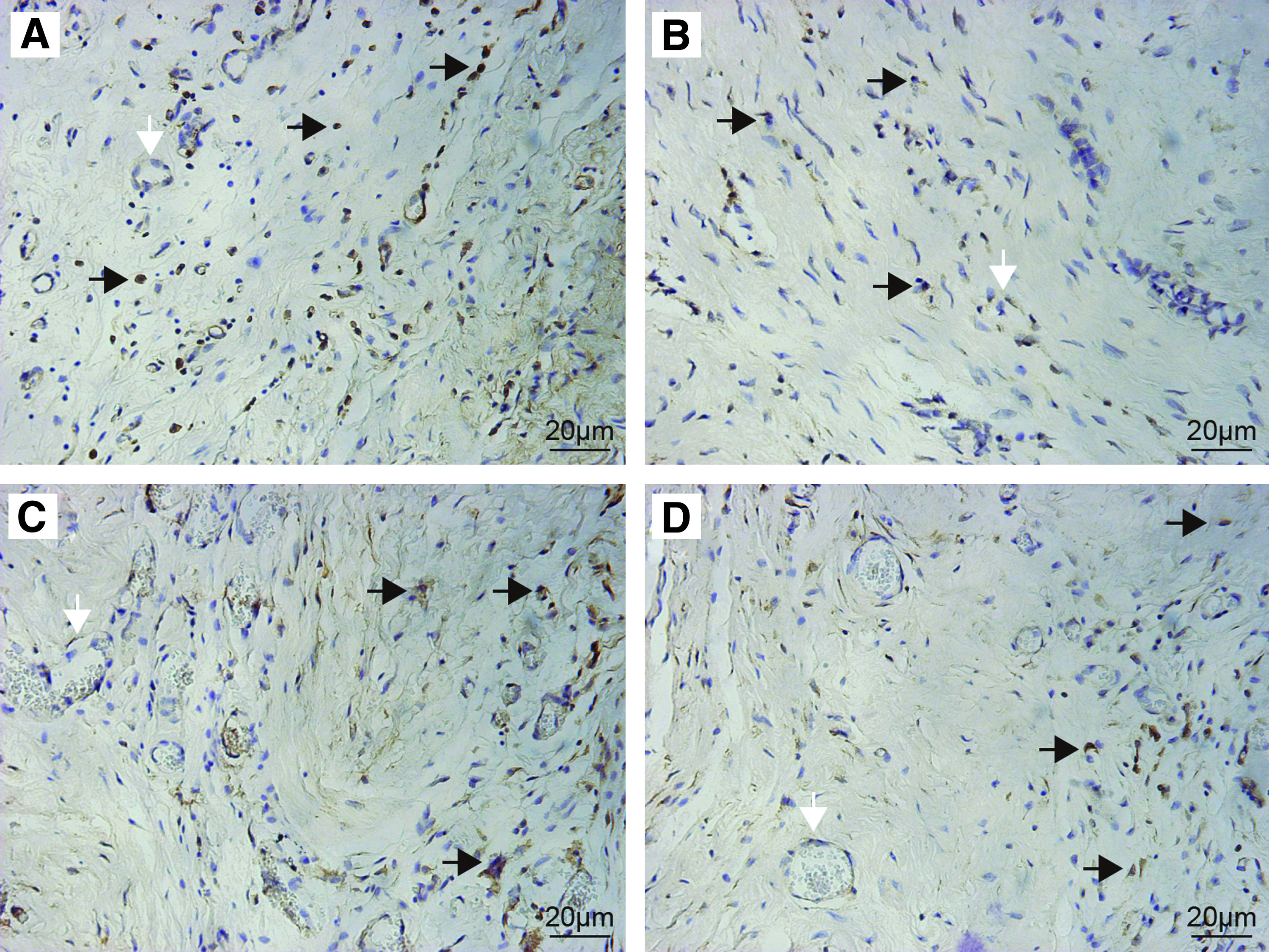
Immunohistochemical (Von Willebrand Factor antibody [VWF]) staining for the tenocyte-SIS scaffold
Immunohistochemical (CD45) staining for the tenocyte-SIS scaffold
Discussion
Reconstruction of abdominal wall defects remains a problem in surgery, especially in cases having insufficient fascia musculares or excessive tension of the defects. Besides surgery, implant materials play an important role in repairing abdominal defects. A variety of materials exist, each with their own advantages and corresponding complications.26,34,35 In tissue engineering applications, some investigators have reported the successful use of various cells and SIS to restore defects.36,37 In the present study, we explored the feasibility of seeding tenocytes onto SIS to reconstruct abdominal wall defects in a rat model.
Choosing a suitable scaffold in the design of tissue engineering products is critical for promoting optimal regeneration of damaged tissues. Among various materials, SIS was chosen as the scaffold in this study. Since it was approved by the US Food and Drug Administration for soft tissue repair in 1999, SIS has been widely used in a variety of tissues and organs, with successful results in tissue regeneration and functional recovery.23,25,38 As an acellular extracellular matrix, the SIS can not only provide a three-dimensional structure for cell adhesion, growth, and migration, but it also secretes growth factors, such as the vascular endothelial growth factor (VEGF), basic fibroblast growth factor, transforming growth factor-β, and tumor necrosis factor-α. 32 These may signal to the host tissue to promote angiogenesis, cell migration, and differentiation. In this study, the results demonstrated the formation of neo-tissue at the junctions between muscle tissue and the scaffold. The SIS was integrated in the host tissues and showed different degrees of degradation at 5 and 9 weeks. Compared with the cell-SIS scaffold, the tenocyte-SIS scaffold either had no adhesion or slight and thin adhesion that was easily separable at the repaired sites (p<0.05) (Fig. 4C). Meanwhile, the scaffold becomes shinner at the central region of the scaffold. The phenomenon suggests that host cells migrated from the surrounding tissue into the scaffold. As shown in Figure 8, the scaffold integrated with the surrounding tissue and a large number of host cells had migrated into the scaffold after 5 weeks implantation, which showed good biocompatibility. In addition, the scaffolds were gradually remodeled by the host tissue. The inflammatory response was observed at 5 weeks and a slight or less inflammatory response was found at 9 weeks probably because the SIS scaffold induced a dynamic immune and cellular response after implantation. 11
The other important issue that needs to be explored for tissue engineering is an appropriate cell source for repairing the defects. Abdominal wall defects have been previously repaired using tissue engineering with a variety of different cell types, but not with tenocytes. In this study, tenocytes were used as the cell source, where they could secrete corresponding matrices, especially collagen fibrils, which might be the reason for increased mechanical strength. Previous studies have described that the maturation of college fibrils is closely related with culture time and mechanical properties.39,40 As shown in Figure 6, TEM examination revealed that the collagen fibrils remained immature (the diameter was small and the arrangement was random), mostly because the scaffold needs a longer culture time in vivo and more cyclic mechanical training.40,41
The mechanical strength of the scaffold plays an important role in reconstructing abdominal wall defects, which can be used to predict the success or failure of the surgery. The mechanical strength provided by the scaffold, can be divided into two parts: the collagen fibrils of the SIS before degradation and the neo-tissue after implantation. The success of the implantation depends on a balance between the rate of degradation and the rate of tissue remodeling. Previous investigators have demonstrated that in a dog model of abdominal wall defect repair, ∼25% of SIS scaffolds were absorbed at 1 month, 75% at 2 months, and were completely replaced by the host tissue at 4 months. 26 If the scaffold has enough mechanical strength to prevent the occurrence of hernia before complete degradation, the recurrence rate of hernia would be significantly reduced. In our study, no significant difference was observed for measuring the maximum loading in both test groups (p>0.05). However, compared to the scaffold control group, the experimental group showed a higher elastic modulus, which is the most important mechanical property for repair (Fig. 5). The higher elastic modulus reveals that the experimental group has a better ability to resist the same pressure than the scaffold control group. Therefore, the cell-SIS scaffold could better reduce the incidence of hernia than the SIS scaffold.
Effective repair of abdominal wall defects depends on early re-establishment of angiogenesis and cellular infiltration. 11 The growth factor contained in the SIS, especially VEGF, can help stimulate angiogenesis. Neo-vascularization has the ability to promote further cell infiltration, which have synergistic effects with each other. In our study, histological analyses revealed that moderate blood vessels were observed after 5 weeks implantation (Fig. 8A, E), most of which were observed in the junction between the scaffold and the autologous tissues. A higher density of blood vessels was found in the junctional and central regions at 9 weeks (Fig. 8I, J, M, N). We speculate that angiogenesis began first in the surrounding tissues of the scaffold (Fig. 7). In addition, some blood vessels with complete vascular walls could be found in the junctional and central regions of the scaffold at 9 weeks. We also observed that with more blood vessels being formed, there was a corresponding increase in host cell infiltration of the scaffold (Fig. 8J, N).
Some limitations of the present study should be mentioned. Although constructing composite scaffolds to repair the abdominal wall defects was the purpose of our experiments, Sprague-Dawley rats, unlike humans, have no apparent aponeurosis-like tissue in the abdomen. Therefore, we cannot mimic the process of repairing normal musculofascial tissue defects in this model. Most importantly, long-term and quantitative studies should be measured for the production of a fully functional scaffold.
Conclusion
This study demonstrates for the first time that engineered aponeurosis can be generated with tenocytes and SIS in vivo. These scaffolds were shown to possess better mechanical loading, biocompatibility, and vascularization. The current findings may provide an alternative, more effective therapy for the repair of abdominal wall defects.
Footnotes
Acknowledgments
This work was supported by a grant from the Medicine-Engineering project, the Shanghai Jiao Tong University (Grant No: YG2009MS36) and Shanghai Hospital Development Center (Grant No: SHDC12010204). We thank Ming Zhang for assistance of surgical procedure and Ke Liu for assistance of picture preparation.
Disclosure Statement
No competing financial interests exist.