
Abstract
We evaluated the use of an automated, point-of-care instrument to derive canine adipose stromal vascular fraction cells, and the subsequent deposition of these cells onto the luminal surface of an expanded polytetrafluoroethylene (ePTFE) vascular graft for use as a bypass graft. The hypothesis evaluated was that an instrument requiring minimal user interface will provide a therapeutic dose of cells to improve the patency of synthetic vascular grafts in an autologous animal model of graft patency. The stromal vascular fraction (SVF) cells were isolated using an automated adipose tissue processing and cell isolation system and cells sodded onto the surface of an ePTFE vascular graft. Control grafts, used off-the-shelf without cell treatment were used as a control to assess patency effects. Each animal received a control, untreated graft implanted in one carotid artery, and the cell-treated graft implanted in the carotid artery on the contralateral side. The grafts were implanted for 6 months utilizing 12 animals. Results indicate a fully automated adipose tissue processing system will consistently produce functional autologous cells for immediate use in the operating room. Cell-sodded polymeric grafts exhibited improved patency compared to control grafts after 6 month implantation in the canine carotid artery model.
Introduction
The accelerated formation of an endothelial cell lining on synthetic grafts has been associated with improved patency.10–15 Previous studies have established that stromal vascular fraction cell populations isolated from adipose tissue and transplanted onto the blood contacting surface of synthetic vascular grafts accelerates the formation of an antithombogenic endothelial cell lining.2,6,16–28 The formation of this endothelial cell lining on small diameter grafts is associated with improved long term patency. 29 These previous studies have utilized a “laboratory method” where the adipose tissue processing, including enzymatic digestion and cell isolation by centrifugation is performed using standard laboratory equipment. This includes test tubes, pipettes, incubators and table top centrifuges. The current study has focused on the development of a totally integrated, fully automated system for stromal vascular fraction (SVF) cell population isolation. The equipment developed consists of a hardware component and a disposable component. This instrumentation represents a point of care device that internalizes all fluid paths and requires minimal user manipulation.
This fully automated system was evaluated in a canine model of adipose tissue digestion and SVF isolation. The SVF cell population was subsequently used to coat the inner lining of expanded polytetrafluoroethylene (ePTFE) vascular grafts utilizing a pressure driven cell deposition process defined as sodding. 25 The function of the SVF cell population isolated using the automated system was evaluated in a canine carotid interpositional vascular graft model. The animals were used as their own control with the test graft implanted in one carotid artery and the treated graft implanted in the other. The grafts were implanted for 6 months utilizing 12 animals. These studies establish the ability to utilize a fully automated system to isolate adipose SVF cell populations and establish the function of these isolated cells, once transplanted onto grafts, toward improved patency of vascular grafts.
Materials and Methods
Animal selection and welfare
All animal studies were performed following protocols approved by the University of Louisville Institutional Animal Care and Use Committee (IACUC). All procedures were performed and the animals housed in American Association for Accreditation of Laboratory Animal Care (AALAC) approved facilities. The National Research Council “Guide for the Care and Use of Laboratory Animals” was followed.
Twelve canines, weighing 23–33 kg, were selected based on overall health. No analysis was performed to determine interanimal variability with respect to platelet or clotting factor reactivity. After the acclimation phase the animals were medicated with persantine (200 mg BID) 4 days before implant surgery and aspirin (325 mg daily) for 1 day before implant surgery. Both medications were continued for 5 weeks postsurgery. Blood work for basic health was obtained before surgery.
On the day of surgery animals were sedated with Telezol IM, intubated, and maintained on Isoflurane anesthetic for the entire implant surgery. Carprofen and buprenorphine were administered IV before surgery for analgesia and per os for the first 2–4 days postsurgery. Animals received cephalexin at the time of surgery which was continued for the first 10 days postsurgery.
Stromal vascular fraction cell isolation
A small midline laparotomy was performed to retrieve approximately 30 g falciform ligament fat. The abdomen was closed and the animal kept anesthetized, while the SVF cells were isolated from the fat. The fat was placed in media (Media 199E; GIBCO, Invitrogen) and minced into small sections. Using sterile technique, the minced fat was placed in a digestion chamber and an equal volume of purified collagenase (Worthington crude collagenase purified according to the methods of Williams et al. 30 ) was added. The digestion of extracellular matrix and subsequent isolation of the SVF cell population was completed in an automated instrument utilizing the processing conditions previously established for SVF isolation in the laboratory. After 30 min of collagenase digestion, the cell slurry was centrifuged at 900 g to separate the buoyant adipocytes from the dense SVF cell population. The SVF cell pellet was then washed and suspended for transplantation onto the surface of the grafts.
Graft preparation
The grafts utilized in this study were Impra (Bard), 30 μm intermodal distance, ePTFE vascular grafts with an internal diameter of 4 mm. All dogs received one cell treated graft and one without cells. Before cell transplantation the graft that would receive the cells was infused with media containing 0.1% bovine serum albumin (BSA). The media was pushed through the interstices of the graft at 5 psi with the ends of the graft capped. The wetted graft was set aside until the time of cell transplantation. The control, noncell treated graft remained dry.
The automatic cell isolation was completed in approximately 1 h utilizing a fully automated Cell Isolation System abbreviated the CIS. The final product of cells suspended in media was automatically placed in a syringe for delivery to the graft. A small aliquot of the cell suspension was collected and the number of cells and viability of the cells in the suspension was counted utilizing a NucleoCounter (ChemoMetec) automated cell counting and cell viability instrument. Cell number was calculated and the appropriate number of cells to provide 2×105 cells per cm2 graft surface area was drawn up in a syringe for cell transplantation onto the graft. One end of the graft was capped and the cells were pushed through the graft maintaining 5 psi within the graft lumen. This pressure was monitored via a pressure gauge that is placed in line between the graft and the syringe. Once the cell suspensate was pushed into the graft, four graft volumes of media with 0.1% BSA were pushed through the graft wall. The cell treated graft was then ready for implantation. Small sections of the cell treated grafts were removed from the graft before implant, placed in formalin, and subsequently stained with bisbensimide to evaluate cell coverage on the intimal surface postcell transplantation.
Graft implantation
A midline neck incision was performed and both carotid arteries were isolated. Heparin was administered (3000 U) intravenously. Flow for both arteries was measured utilizing a Transonic flow probe. The carotid artery that would receive the noncell treated graft was clamped and the mid section removed between the clamps. The control graft was implanted utilizing an end-to-end anastomosis with 6-0 Prolene. Flow was restored and flow measurements recorded. When the cell treated graft was ready, the graft was implanted in the contralateral carotid artery. Once flow had been observed for at least 30 min the neck was sutured and the animals were recovered with direct observation.
Patency evaluation
Graft patency was evaluated every month utilizing a Sonosite M-Turbo ultrasound system (Sonosite, Inc.). The grafts were visualized by digital two dimensional imaging as well as M Mode to evaluate flow and graft position. Color Doppler analysis was performed on the entire graft to evaluate flow. All evaluations were recorded.
Graft explantation
After 26 weeks the animals were anesthetized and prepared for surgery as above. Ultrasound was performed to evaluate flow for each graft followed by a cut down to the femoral artery for angiogram evaluation. Angiograms of the carotid arteries were performed to evaluate patency. The grafts were exposed through a midline neck incision and flow for each graft was measured with a flow probe. Gross photographs of each graft and surrounding tissue were obtained. In addition, patency was assessed by direct needle puncture into each graft.
The grafts, with at least 2 cm of native artery at both anastomoses, was excised and gently flushed with warm buffer containing 0.1% BSA. The animals were euthanized. Graft samples were sectioned into segments and prepared for light histology and scanning electron microscopy (SEM).
Histology
Representative samples of graft with surrounding tissue were fixed in 4% parformaldehyde. Samples were dehydrated and brought to paraffin, sectioned and stained with hematoxylin/eosin (H&E). The slides were examined and photomicrographs were obtained.
Samples were also obtained for SEM. Samples were fixed in 3% glutaraldehyde in PIPES buffer, dehydrated in a graded series of acetone, and critical point dried. Dry samples were sputter coated using a gold target. The samples were evaluated in a JEOL scanning electron microscope and digital photomicrographs were obtained.
Results
Automated stromal vascular fraction cell isolation
The automated adipose tissue processing and SVF cell isolation system is illustrated in Figure 1a. The instrument consists of a controller box; a temperature controlled upper chamber, a dual syringe compartment, a computer screen, and disposable plastic components. Before processing fat tissue the system was powered and the disposable components loaded as instructed by the instrument's software. The disposables included a digestion chamber, a fluid path regulating insert, syringes (one containing collagenase), and IV bags (one bag containing media for cell processing and washing) all interconnected with medical grade plastic tubing. Once assembled, the instrument alerted the user, through the incorporated computer screen, that the adipose tissue was ready to be injected into the system.
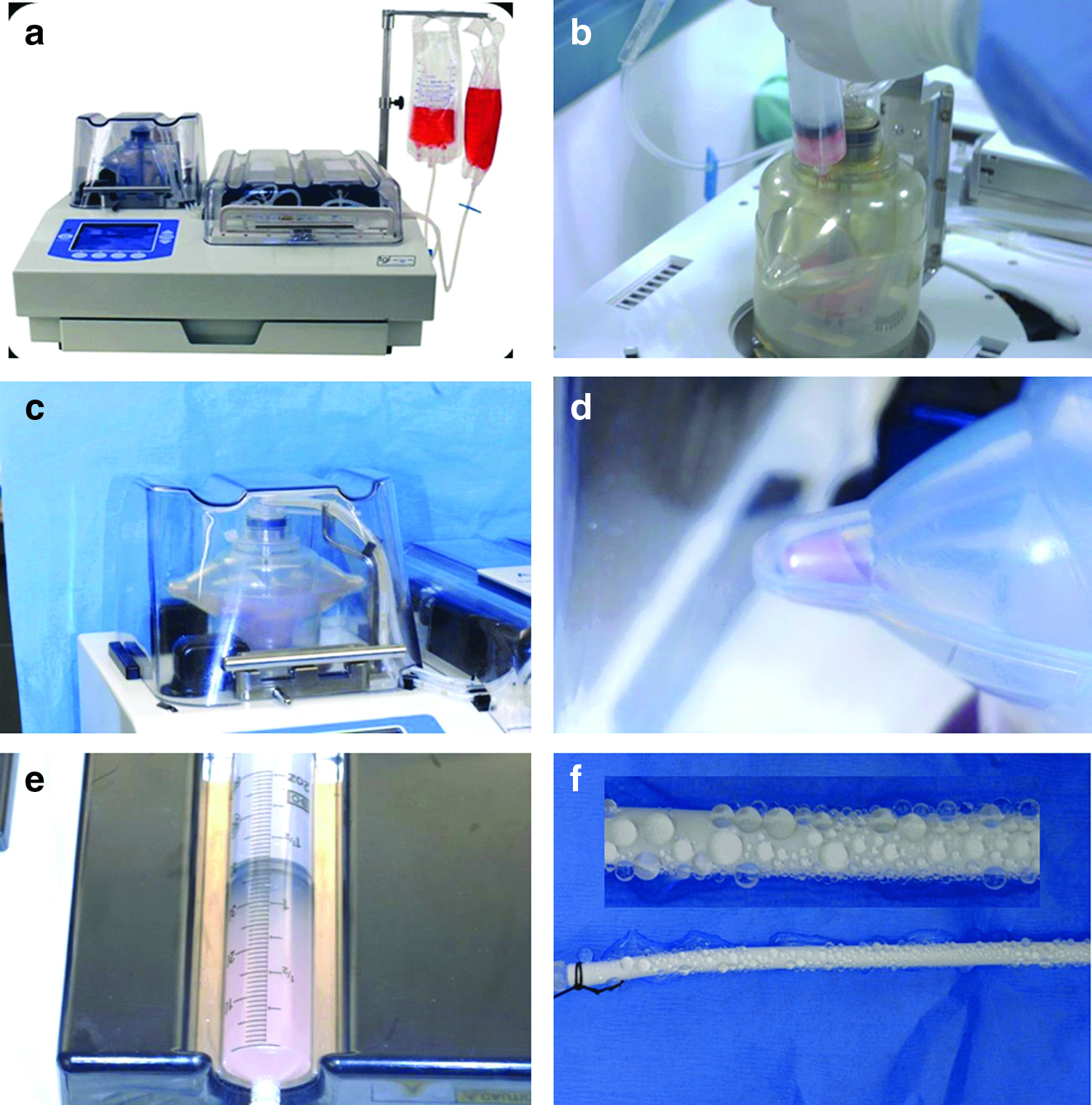
Automated adipose stromal vascular fraction cell isolation system.
All animals exhibited sufficient falciform ligament fat to provide a 30 g sample for processing. Unlike human liposuction fat that is sufficiently minced during the process of lipoaspiration, the canine fat must be hand-minced using scissors before infusion into the instrument. The infusion of the minced canine fat is illustrated in Figure 1b. Once the digestion chamber was filled with fat, the instrument processed the fat tissue using the SVF cell isolation procedure previously reported for canine tissue utilizing the “laboratory method.” The steps in this isolation procedure that are duplicated in the instrument include addition of collagenase, agitation of the tissue-collagenase slurry (Fig. 1c) for 30 min, and centrifugation of the cellular slurry to pellet the SVF cell population and separate the SVF from the buoyant adipocytes. The digestion chamber in the instrument contains two lobes that receive the SVF cells resulting in the formation of a pellet as illustrated in Figure 1d. This cell pellet was subsequently washed from the collection lobe using a spray of media, the cells suspended in 35 mL of media using an inline filter, and the final cell suspension collected in a 60 mL syringe (Fig. 1e). The processing time from fat infusion to the collection of cells in the final product syringe is approximately 1 h.
All canine fat samples were successfully processed and SVF cell suspensions were produced from all animals. The average SVF cell yield for each animal was 7.10×106 SVF cells per ml of fat. The average cell viability was 78%. The instrument and disposables performed as intended for all isolations. Microbiologic cultures were performed on a sample of the SVF cell population, swabs from the fat infusion port, and the fluid from the sodded grafts before implant. These cultures were all negative for growth out to 14 days.
The vascular grafts to receive SVF cells were infused with media before receiving cells to “prewet” the surface of the grafts as well as infuse buffer into the porous interstices of the grafts. This infusion of media utilizing a pressure head of 5 psi results in the weeping of fluid through the graft as illustrated in Figure 1f (higher magnification inset illustrates beading of fluid). Each SVF cell treated graft was sodded using a volume of cells that would provide 2×105 cells/cm2 surface area of ePTFE graft. A sample, obtained from the end of each graft, was processed for observation of cell surface density using the nuclear stain bisbenzimide. Figure 2 illustrates the dispersion of cells into the luminal surface of the porous ePTFE grafts. At the time of graft sodding, the cells were observed to be present in the interstices of the graft with limited cell deposition on the nodes of the ePTFE graft material.

Epifluorescence micrograph illustrating the distribution of sodded SVF cells on the luminal surface of an ePTFE graft. The samples were treated with bisbenzimide to identify cell nuclei.
Implant phase observations
All animal's recovery from surgery was unremarkable. All incisions, for removal of fat and placement of grafts, exhibited normal healing progression. Following protocol, all animals received both aspirin and persantine for 5 weeks after which no anticoagulant medications were administered. All animals remained in the trial to the end of the 26-week implant phase, at which time the grafts were explanted and evaluated.
Explant evaluation
The grafts were exposed through a midline neck incision and photographs of the external surface of the grafts obtained, although not quantified, tissue associated with the exterior surface of the sodded grafts appeared more vascularized by visual appearance as compared to the control grafts. The grafts, with a length of proximal and distal vessel, were explanted, cut into segments and evaluated. Gross visualization of the explanted grafts revealed the luminal surface of all patent sodded grafts exhibited a glistening white luminal surface free of any identifiable thrombus. The luminal lining was homogeneous across the entire surface. The single patent control graft exhibited some areas of red thrombus on the luminal surface and gross evidence of luminal cellularization was limited to the region of proximal and distal anastomoses. Clotted grafts contained a dense thrombus. Figure 3 illustrates a mid graft cross section of a sodded (right) and control (left) graft. The sodded graft exhibits no evidence of luminal restenosis.
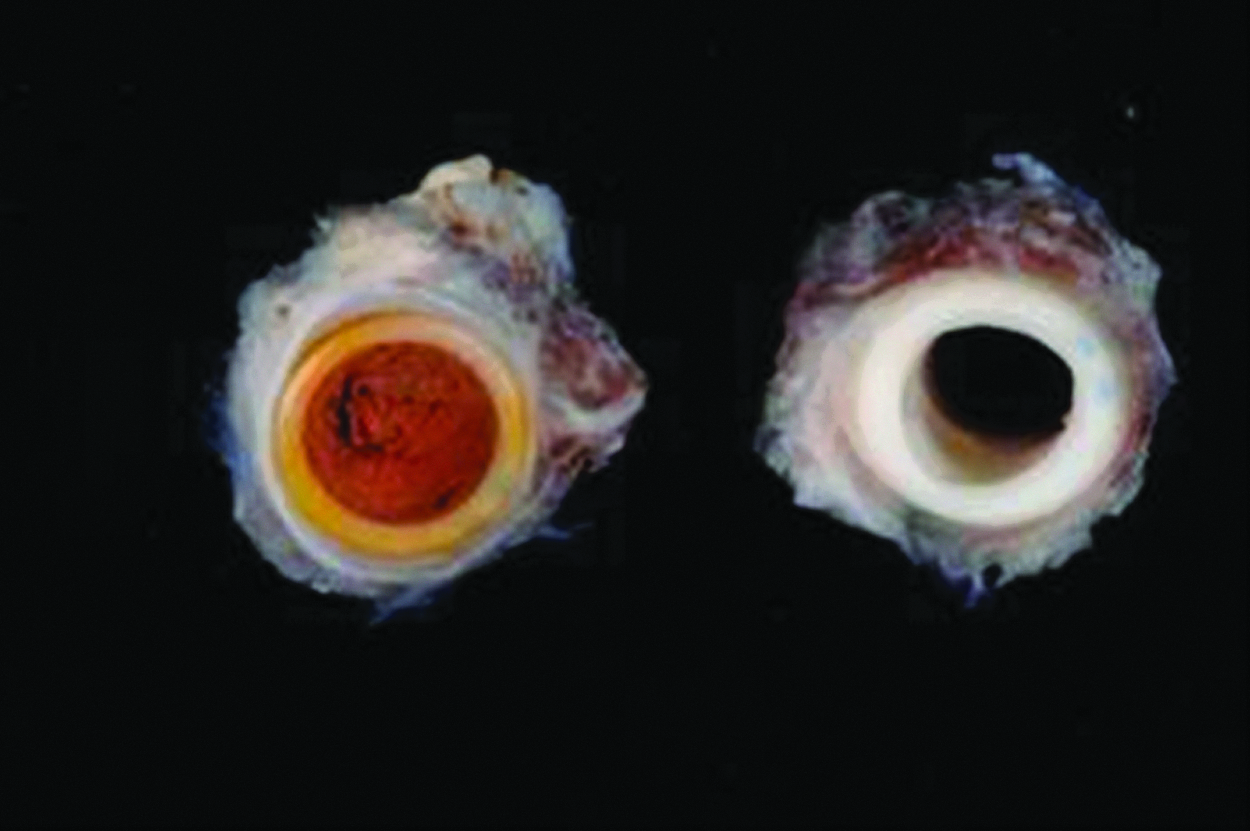
Gross photograph of a mid cross section of a control and sodded ePTFE graft.
Histology
Patent SVF cell treated grafts all exhibited, after sectioning and hemotoxylin/eosin staining, both a neointima and neomedia in association with the luminal surface of the ePTFE graft (Fig. 4a, longitudinal section and 4 b cross section). The luminal, blood contacting cell lining exhibited characteristics consistent with endothelium. No evidence of luminal thrombus formation was observed in the sodded grafts. The neomedial cells exhibited characteristics of myofibroblasts based on their stellate morphology and positive reactivity with antibodies to alpha smooth cell actin (data not shown). The SVF cell sodded grafts were subjected to comparative staining with H&E, Masson's trichrome, and pentachrome staining to evaluate the neo intima and neomedial maturation. Figure 5 (a. H&E; b.Trichrome, c.Pentachrome) illustrates the luminal formation of both a neointima and neomedia on the patent SVF cell sodded grafts, and cellular infiltration and extracellular matrix deposition in the interstices of the ePTFE grafts. For comparison to a native canine carotid artery, sections of normal native canine carotid arteries were stained with these three histologic stains and are compared to the SVF cell sodded grafts in Figure 6 a–f. As compared to the native vessel, the sodded grafts exhibit an antithrombogenic lining of cells and the development of a neomedia but there is no evidence of formation of organized elastic fibers and no evidence of formation of an internal elastic lamina in the sodded grafts as compared to the IEL illustrated in the native vessel.
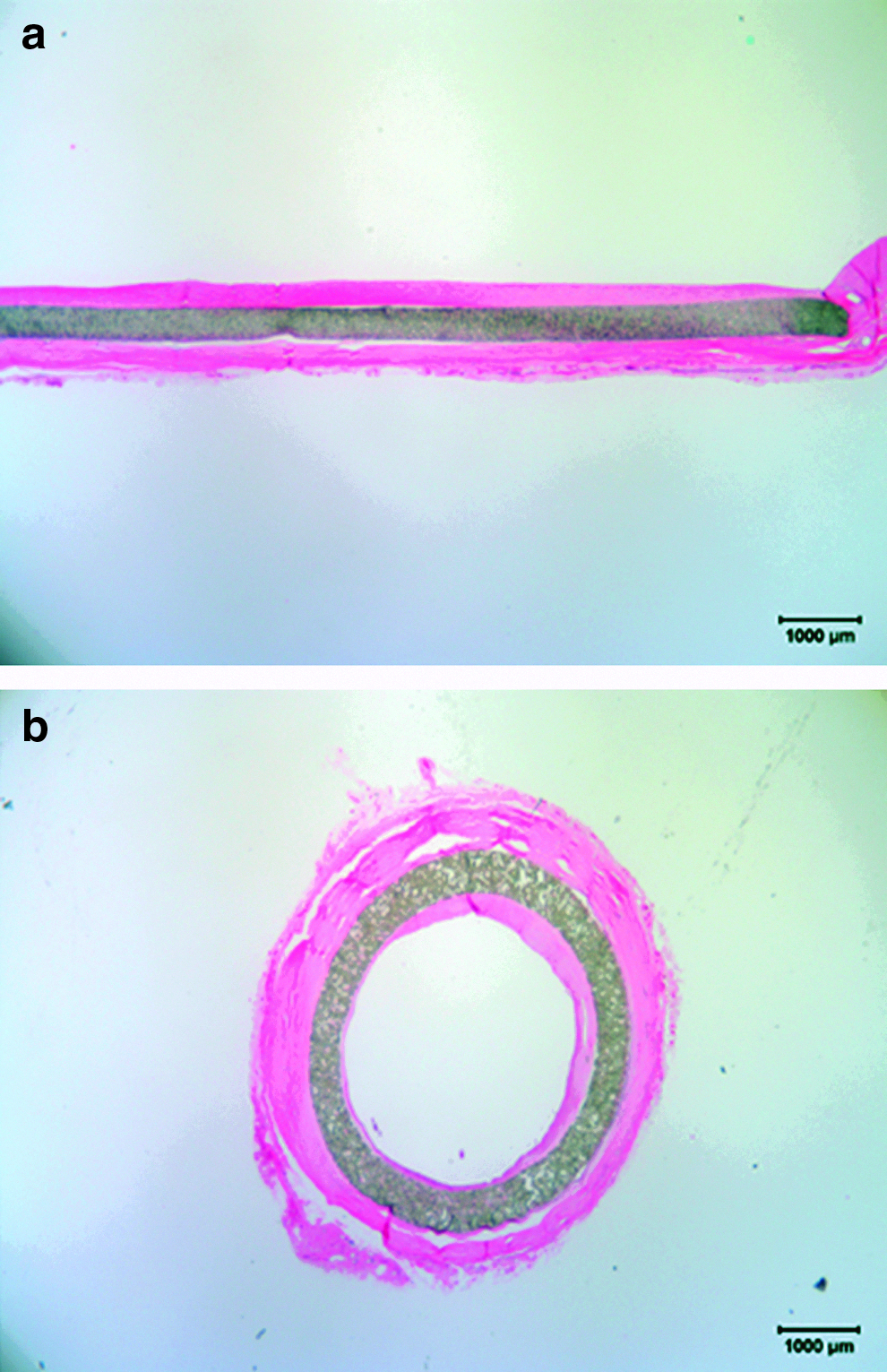
Photomicrograph of SVF sodded vascular grafts after 26 week implantation.
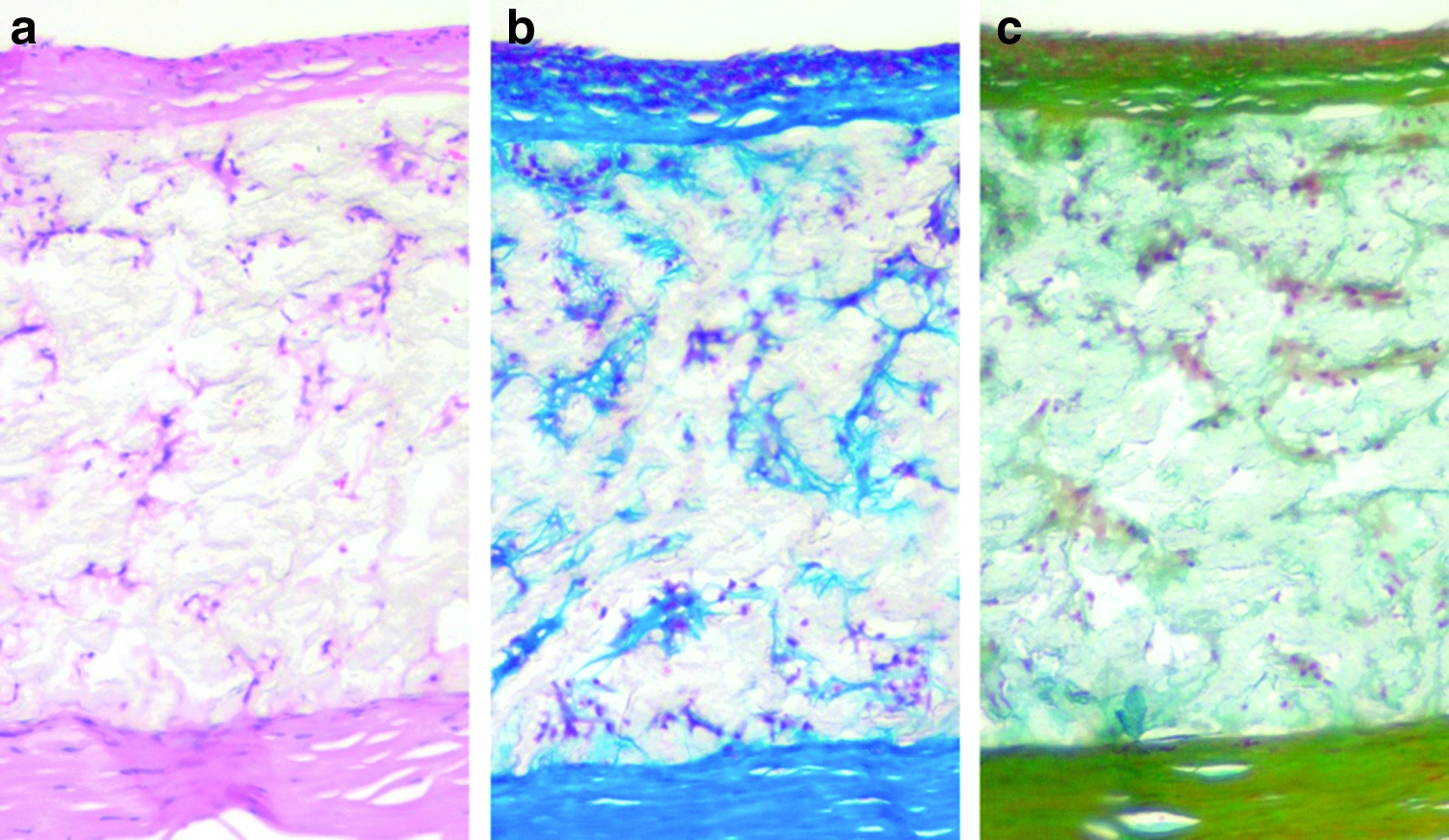
Photomicrographs of SVF sodded grafts.
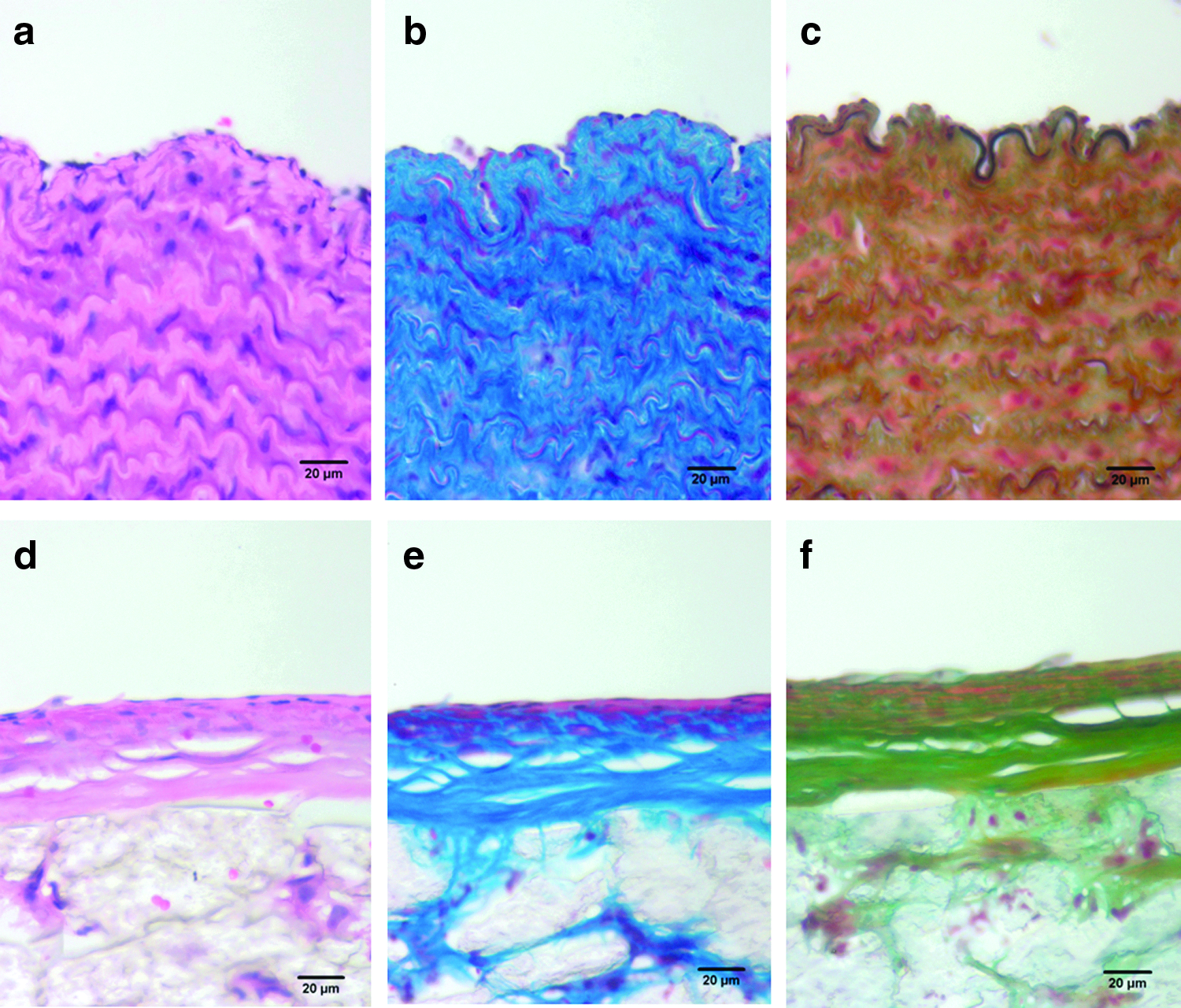
Photomicrographs of canine native carotid artery
Scanning electron microscopy
Samples of the patent grafts were prepared for SEM evaluation. The patent sodded grafts exhibited a luminal lining of cells with characteristics typical of endothelium. There was a lack of thrombus deposition consistent with the antithrombogenic nature of endothelium. The endothelial cell lining was complete on all patent SVF cell treated graft samples spanning the entire surface from proximal to distal anastomoses. The transition from native vessel to graft luminal surface was unremarkable (Fig. 7).The single patent control graft exhibited a significant deposition of thrombus, including platelets and fibrin and no evidence of spontaneous endothelialization of the luminal surface.
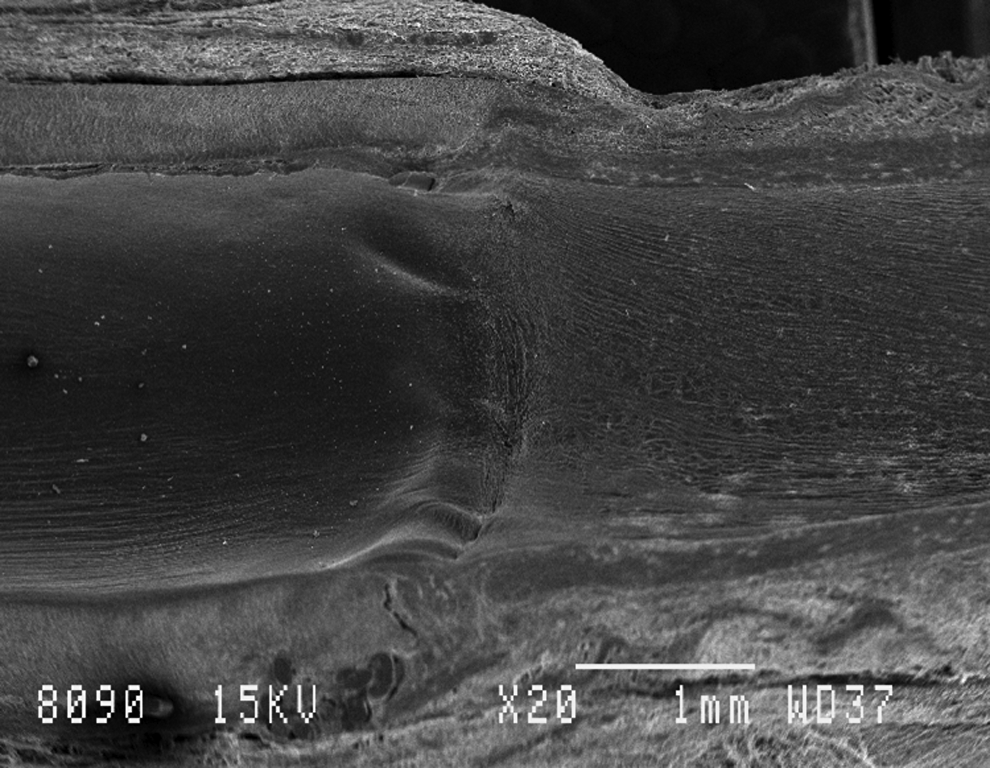
Scanning electron micrograph of SVF sodded graft illustrating anastomotic interface between ePTFE graft (left) and native vessel (right).
Patency
Immediately postimplant all grafts were patent based on hand-held Doppler ultrsonography. During subsequent analysis graft function was determined to be either patent based on a positive Doppler signal and a blood flow rate > 1 mL/min based on color-duplex ultrosongraphy, or clotted based on a lack of Doppler signal and a lack of identifiable blood flow (flow=0 mL/min) based on color-duplex ultrasonography. All animals were treated with aspirin and persantine for 5 weeks postimplant and ultrasounds were performed monthly to assess patency. Seven dogs had clotted/clotted grafts before the 6 month end point and were explanted at 4 months. The remaining five dogs proceeded out to 6 months implantation. At 6 months, 8% of the untreated/control grafts remained patent and 42% of the SVF cell treated/testgrafts remained patent (Fig. 8).
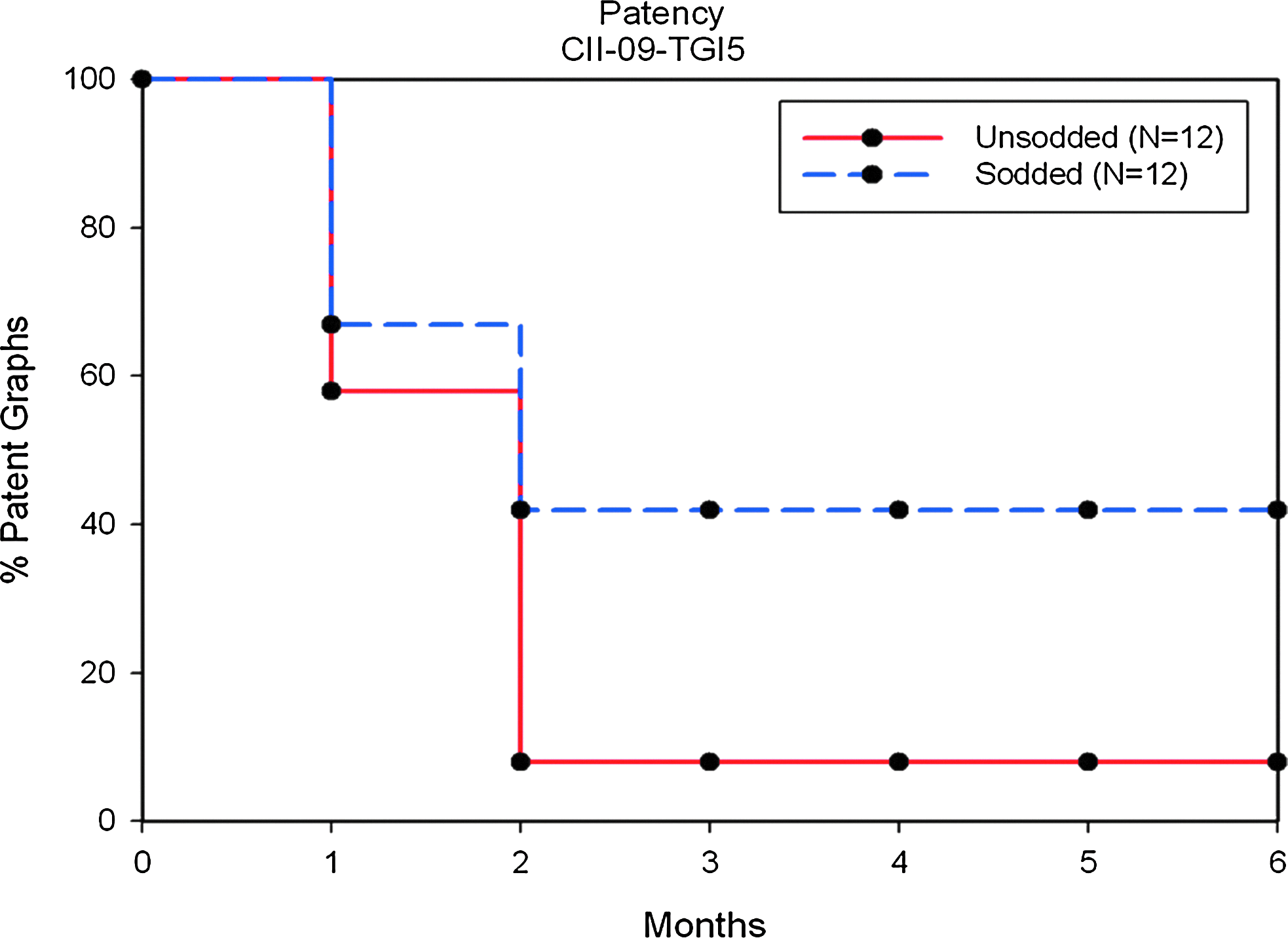
Primary patency of SVF sodded and control ePTFE grafts.
Discussion
There remains a significant unmet clinical need for a tissue-engineered vascular graft that exhibits the functional characteristics of a native blood vessel. The clinical acceptance of a blood vessel replacement therapy has several requirements, including proof that the alternate therapy exhibits improved function and the ability to have this vessel available essentially “off the shelf”, and thus, applicable to point of care environments. Previous demonstration that adipose derived SVF cells represent a point of care source of cells to improve the patency of synthetic vascular grafts preceded the current study toward development of automated systems for routine, consistent point of care isolations of adipose SVF. The instrument described and the results observed indicate the automated isolation of SVF cells was achieved and these cells can be used in an operating room compatible environment to provide a functional alternative blood vessel for bypass applications.
Formation of a functional endothelial cell lining on synthetic grafts as well as endovascular devices that maintain a blood contacting surface once implanted is generally agreed to be the primary requirement for long term device function. The accelerated formation of a functional endothelium on devices has been addressed through methods to accelerate spontaneous endothelialization and methods to transplant endothelium, or endothelial precursor cells onto the luminal surface of devices. While many successes have been reported, including the development of an alternative bypass vessel with no synthetic components, these vessel replacements often have shortcomings due to the need to culture the vessels for extended periods of time, and the need for extended anticoagulant therapy during the time a spontaneous endothelial cell lining is forming. The use of a point of care device to isolate functional endothelium from autologous adipose tissue overcomes many of these other approach shortcomings.
There are several other automated/semi automated adipose SVF cell isolation systems, Cytori, Inc.,31–33 Biosafe SA, 34 that have been reported in the literature. The basic operation of these instruments is similar with respect to the process of digesting fat using proteolytic enzymes followed by the use of centrifugation to separate buoyant adipocytes from the stromal vascular fraction cell population. However, there are significant differences in the devices and instrument used for the enzymatic digestion of fat and subsequent SVF isolation. Specifically, the Tissue Genesis automated system is entirely closed and, unlike the other systems, does not require the physical transfer of solutions between devices during processing. There is also a significant difference in the cellular endproduct of these devices, especially the yield of cells per gram of fat digested. Mean cell yield using the Cytori system is reported to be between 2.2×105 cells/g fat 31 and 3.7×105 cells/g fat, 33 and for the Biosafe SA system 2.6×105 cells/g fat has been the reported yield. 34 As reported here the Tissue Genesis automated system results in a mean cell yield of 7.10×106 cells/g fat requiring approximately 1 h for processing of the fat (calculated from the time of fat injection into the digestion chamber to the time the cells are delivered to the collection syringe and are ready for use). The cell viability was similar using all systems and was greater than 70% in all reports. We conclude that the Tissue Genesis system results in a much higher yield of cells and speculate this is due to the closed system design, the digestion chamber agitation, and the use of proteolytic enzymes optimized for fat digestion and cell release.30,35
The use of stem and regenerative cells in preclinical and clinical evaluations has undergone explosive growth. Unfortunately, the techniques and methods for the isolation of these stem and regenerative cells is highly variable with many laboratory-specific procedures evolving that make duplication by other laboratories difficult. A major hypothesis driving our current work is that automated systems, requiring minimal user interface, can be designed and constructed for tissue processing and cell isolation. This has been achieved in the currently described instrumentation. After infusion of a fat sample into the system a software controlled process regulates and records all the tissue and cell processing steps and each adipose tissue sample is processed identically.
The efficacy of the adipose derived SVF cell population toward accelerated formation of an endothelial cell lining on small diameter (<6 mm id) synthetic vascular grafts has been established in this study. This finding is not novel as the SVF cell population has previously been shown to accelerate endothelialization of grafts. The current study confirms previous results using adipose SVF cell sodding toward accelerated graft endothelialization and improved graft patency and establishes the use of automated instrumentation for tissue processing and cell isolation.
Footnotes
Acknowledgments
The authors wish to thank Robert Reed, Renia Sylvester and Josh Nelson for their technical assistance and efforts involved in the completion of this study. This work was supported by the United States Army Medical Research and Materiel Command, through Department of Defense Contract W81XWH-05-1-0620.
Disclosure Statement
The instrument described in this manuscript is manufactured by Tissue Genesis, Inc.
Stuart K. Williams is a paid consultant of Tissue Genesis, Inc.
Paul E. Kosnik is an employee of Tissue Genesis, Inc.
Erik M. Vossman is an employee of Tissue Genesis, Inc.
Kevin D. Lye, is an employee of Tissue Genesis, Inc.
Michelle H. Shine is an employee of Tissue Genesis, Inc.