
Abstract
The periosteum plays a pivotal role during bone development and repair contributing to bone vascularization and osteoprogenitor cells source. We propose a periosteal substitute engineered using a platelet-rich plasma (PRP) membrane incorporating autologous bone marrow-derived mesenchymal stem cells (PRP/BMSC gel membrane) to be wrapped around an osteoconductive scaffold for regeneration of compromised bone defects. The PRP/BMSC gel membrane was optimized using different compositions for optimal release of vascular endothelial growth factor (VEGF) and platelet derived growth factor-BB (PDGF-BB). Survival and proliferation of cells in the PRP gel membrane with time were confirmed in addition to their osteogenic capacity. Furthermore, to evaluate the possible effects of the PRP/BMSC gel membrane on surrounding progenitor cells in the injury area, we found that the PRP gel membrane products could significantly induce the migration of human endothelial cells in vitro, and increased the expression of bone morphogenetic protein 2 in cultured BMSC. These cells also secreted significant amounts of soluble proangiogenic factors, such as PDGF-BB, VEGF, and interleukin-8 (IL-8). Finally, the functionality of the PRP/BMSC gel membrane periosteal substitute for bone regeneration was tested in vivo both in an ectopic mouse model as well as in a rabbit segmental bone defect model providing evidence of its capacity to biomimic a periosteal response enhancing bone regeneration.
Introduction
To increase the vascular supply for enhancing bone healing and repair, studies have been investigating several approaches, including engineering arterioles and capillaries using synthetic and biological materials,3,4 implantation of cocultured osteogenic–angiogenic cells, 5 and local delivery of angiogenic/osteogenic growth factor (GF) combinations. 6
In addition, owing to the established part played by the periosteum during bone repair, contemporary studies have attempted to engineer periosteum substitutes to more closely mimic the endogenous repair process and overcome current problems of traditional cell/scaffold-based approaches.7–11
The periosteum, is a microvascularized connective tissue covering the outer surface of the cortical bone, with an outer fibrous layer and an inner cambium layer.10,12 Periosteal vessels deliver osteoblast precursors for new bone formation besides nutrients and oxygen supply.13,14 The current view supports that periosteum and bone marrow are the main local sources of skeletal stem/progenitor cells for bone repair with distinct, but complementary roles.10,12,15–17 During repair, the periosteum gives rise to chondrocytes, osteoblasts, and osteocytes. Consistently, damage or removal of the periosteum drastically impairs bone healing. 18 Periosteal-mediated bone repair with its intricate repair mechanisms recapitulates chondrogenic and osteogenic events occurring during development. 10 Therefore, designing a functional periosteal substitute that is capable of mimicking a natural periosteal response by both enhancing vascularization and providing essential osteogenic precursors may have substantial implications on the field of bone engineering.
Therefore, we aimed to engineer a biomimetic periosteal substitute to envelope an osteoconductive scaffold for regeneration of compromised bone defects. In our construct, bone marrow-derived mesenchymal stem cells (BMSC), as the osteoinductive components, were entrapped within a platelet-rich plasma (PRP) gel membrane. Being rich in mitogenic, angiogenic, and chemotactic factors involved in cell migration, proliferation, and differentiation, 19 and available in their natural-healing mix and proportions,20,21 we hypothesized that the gel membrane would provide the microenvironment required to initiate the healing response and enhance the overall bone regeneration effect.
Materials and Methods
Development, optimization, and characterization of the PRP/BMSC gel membrane
Preparation of the PRP gel membrane
The PRP gel was prepared by a mix of four constituents: PRP, cryoprecipitate (Cryo), which is a fibrinogen concentrate, thrombin (T) and 10 mg/mL calcium gluconate solution (Ca). The PRP, cryo, and thrombin were pooled and prepared from the blood of several healthy donors according to the procedure approved by the institutional ethics committee of the Blood Transfusion Centre of the San Martino Hospital, Genoa, Italy. The PRP had a platelet concentration of 1–2×106 platelets/μL. PRP, thrombin, and cryo were aliquoted and stored at −30°C until use.
Optimization of PRP gel membrane components by measuring PDGF-BB and VEGF contents
Different pools of PRP, cryo, and thrombin from at least three donors were prepared to reduce interdonor variability. The PRP and cryo components were mixed in different ratios by volume to identify the proportions that allowed maximum GF availability (measured by ELISA), while maintaining cell survival in the gel. Activation took place by thrombin and Ca in a 1:1 ratio. The amount of each of the components used to prepare the six tested gel compositions and the percentages of PRP present are listed in Table 1. The gels were incubated for 30 min at 37°C in a 5% CO2 environment, and centrifuged for 10 min at 4000 g. 22 Supernatants were collected and immediately stored at −80°C until analysis by ELISA kits (Human PDGF-BB ELISA kit by RayBiotech Inc. and Human VEGF ELISA kit by Invitrogen) according to the manufacturer's instructions. The obtained GF quantity for each of the three pools was plotted against the expected quantity calculated from the ratio of the PRP component in the gel.
Human bone marrow mesenchymal stem cell culture and incorporation into the PRP gel membrane
Human BMSC were obtained from iliac crest marrow aspirates of healthy bone marrow transplant donors after informed consent. The cells were cultured in a complete culture medium consisting of Coon's modified Ham's F-12 medium containing: 2 mM glutamine, 100 U/mL penicillin, 100 μg/mL streptomycin (Sigma Chemical Co.), and 10% fetal bovine serum (FBS; Life technologies, Invitrogen®) in the presence of 1 ng/mL human recombinant fibroblast growth factor 2 (FGF2) (Peprotech®). At 80% confluence, human bone marrow mesenchymal stem cells (hBMSC) were trypsinized by 0.05% trypsin–0.01% EDTA (Sigma Chemical Co.), and resuspended in a volume of PRP and cryo to yield a P8:C1 gel (PRP/Cryo ratio) at the density of 3×106 cells/mL of final gel volume. Human thrombin was added followed by Ca gluconate. After 5–10 min of jellification, complete culture medium was added to completely cover the gel.
Evaluation of cell distribution, vitality, and proliferation in the PRP gel membrane
Cell distribution within the gels was evaluated at 1, 4, 7, and 14 days. At each time point, gels were fixed with 3.7% paraformaldehyde and processed for paraffin-embedding histology. Four- μm-thick sections were obtained and stained by hematoxylin and eosin (n=3).
To assess hBMSC viability inside the PRP gels after 24 h of cell incorporation, gels were digested with 0.25 mg/mL collagenase type I (Worthington) for 1 h after which gel residues were centrifuged and replated with complete culture media. Cells leaving the gel to attach on the culture dish plastic were observed by light microscopy (n=3).
Furthermore, hBMSC vitality and proliferation within the three-dimensional (3D) gel structure were quantified using a live/dead fluorescence assay. The assay was performed at 1, 4, 7, and 14 days after gel preparation. Gels were stained with 7-aminoactinomycin D (7-AAD; Invitrogen®-excitation 488 nm, emission at 647 nm) for staining nuclei of dead cells (10 μg/mL) and Hoechst 33258 (Sigma-excitation 386 nm, emission 480 nm) for live nuclei (4 μg/mL) for 20 min in 5% CO2 at 37°C, fixed with 3.7% paraformaldehyde containing 2% sucrose for 10 min, and then washed in 2% sucrose in phosphate-buffered saline (PBS). Cell membranes were permeabilized by 0.5% Triton, 20 mM Hepes pH 7.4, 300 mM sucrose, 50 mM NaCl, 3 mM MgCl2 for 10 min at 0°C, and then the gels were rewashed. The gels were then incubated at 37°C with Alexa Fluor® 488 Phalloidin (Invitrogen®-excitation 496 nm, emission 516 nm) for actin filaments staining (5 μg/mL in PBS) for 20 min. After a final wash in PBS, gels were observed in PBS in glass-based 3-cm dishes (Iwaki Glass) using an Axiovert 200M microscope (Zeiss). The acquired images were analyzed for the blue/red (Live/Dead) ratio by ImageJ software (http://rsbweb.nih.gov/ij/download.html). The plotted percentages of Live/Dead nuclei were derived from analysis of three different areas in three different cultures (average of 9 values).
Evaluation of the osteogenic properties of the PRP gel membrane
Analysis of osteogenic induction of PRP/hBMSC gel membranes
To evaluate maintained osteogenic capacity of hBMSC cultured within the gel membrane, gel membranes incorporating hBMSC were cultured in normal complete medium or in osteogenic medium containing 50 μg/mL ascorbic acid, 10 mM ß-glycerophosphate, and 10−7 M dexamethasone (all from Sigma) for 3 weeks. The experiment was performed for a minimum of three different bone marrow donors.
Alizarin red S and Von Kossa staining of gel membranes: After 3 weeks induction, gel membranes were fixed and processed for paraffin embedding as previously mentioned. Serial sections were then stained by Alizarin red S and Von Kossa stains. Osteogenically induced gels without cells and noninduced gels with hBMSC served as negative controls. (n=3).
Gene expression analysis of cells extracted from the gel membranes by real-time polymerase chain reaction (PCR): In parallel, cells were extracted from 3-week osteogenic stimulated and from nonstimulated PRP gel membranes by digesting with plasmin 2 U/mL (fibrinolysin- Calbiotech) at 37°C for 1.5 h. The cells and gel remnants were replated with complete media for 16 h and the RNA was extracted from adherent cells by the TRIzol Reagent (Invitrogen) according to the manufacturer's instructions. Two-dimensional (2D) adherent cultures of stimulated and nonstimulated MSC served as controls. To synthesize the first-strand cDNA, 1–5 μg of total RNA were used in a 20 μL reaction with the oligo (dT) 12–18 primer and the superscript first-strand synthesis system for reverse transcriptase-PCR (Invitrogen). Relative quantification was performed with the ABI Prism 7500 Sequence Detector (Applied Biosystems) following the manufacturer's instructions. Cells were analyzed for mRNA expression of: alkaline phosphatase (ALP) (n=5), bone morphogenetic protein 2 (BMP-2) (n=3), osteocalcin (n=5), collagen I (n=5), and RUNX-2 (n=4). The housekeeping gene glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as the endogenous control for normalization. Primers and probes for each gene assayed are listed in Table 2.
Analysis of the effect of PRP gel membrane released supernatants on osteogenic properties of cultured hBMSC
The effect of PRP gel membrane-released supernatants (PRS) on hBMSC gene expression of ALP and BMP-2 in the absence of osteogenic induction was evaluated. PRS was obtained from P8:C1 gel membranes prepared as previously mentioned and left to jellify for 1 h in 5% CO2 at 37°C. Gel membranes were then centrifuged at 3222 g for 10 min at room temperature. Collected supernatants were then stored at −80°C until use. hBMSC were cultured until 80% confluence, then washed extensively with PBS, and incubated with PRS or a complete culture medium containing FGF-2 for 3 days. The cells were then thoroughly washed and further incubated for 24 h in the serum-free medium. Cells collected in TRizol for RNA extraction and conditioned media (BM-CM) were harvested, centrifuged, and stored at −80°C until use. (n=4).
Evaluation of the angiogenic properties of the PRP gel membrane
Evaluation of endothelial cell migration versus PRS (in vitro migration assays)
Human umbilical vein endothelial cells (HUVEC) were purchased from the IST- Cell Bank (www.iclc.it) and were cultured on 1% gelatin-coated culture plates in the M199 medium containing 10% FBS, 2 mM glutamine, 100 U/mL penicillin, 100 μg/mL streptomycin (Gibco), 10 ng/mL FGF-1, 10 ng/mL FGF-2, 10 ng/mL EGF (Peprotech), 1 μg/mL Hydrocortisone, and 16 U/mL heparin (Sigma) at 37°C, 5% CO2 and 95% humidity. Upon confluence, cells were detached using trypsin/EDTA and used at passage 3 or 4.
Migration of HUVEC against PRS was evaluated using 12-μm-pore gelatin-coated filters (Millipore). HUVEC were seeded at a density of 70–80×104 cells/well in the upper chamber in serum-free M199. In the lower chamber, the serum-free M199 medium or PRS was used. Chambers were incubated for 8 h at 37°C in 5% CO2. Afterward, nonmigrated cells were removed, filters were fixed with ethanol 96%, and stained with 2% Toluidine Blue. Migrated cells on the lower side of the filters were counted in five different fields at 200×magnification. (n=3).
Evaluation of the release of proangiogenic soluble factors in conditioned media of hBMSC (BM-CM) treated with PRS
The concentration of the proangiogenic soluble factors: interleukin-8 (IL-8), platelet-derived growth factor-BB (PDGF-BB), and vascular endothelial growth factor (VEGF) were evaluated in the conditioned media of hBMSC cultured for 3 days in PRS using human IL-8 (n=4) (R&D systems), human PDGF-BB (n=5) (RayBiotech, Inc.), and human VEGF (n=5) (Invitrogen) ELISA kits. The concentration of each factor was evaluated in pg/mL and normalized to the total amount of protein in μg evaluated by the Bradford assay.
Proof-of-principle: evaluation of the PRP/BMSC gel membrane in a rabbit segmental bone defect
Culture of rabbit BMSC and preparation of PRP-rabbit BMSC gel membrane/scaffold constructs
Rabbit BMSC (rBMSC) were cultured from iliac crest marrow aspirates of New Zealand male white rabbits weighing 2.5–2.7 kg as previously mentioned for hBMSC. Briefly, aspirates were washed twice with PBS and cells were counted and plated in 10-cm culture dishes at a density of 5–9×106 mononuclear cells/dish in a complete culture medium with FGF2. First passage rBMSC were used for all in vivo experiments.
For the preparation of rabbit PRP gel/rBMSC membranes, PRP and platelet-poor plasma (PPP) were prepared from a pool of whole blood obtained from a minimum of five rabbits. The blood was first centrifuged at 209 g for 16 min after which the clear supernatant phase was collected, recentrifuged at 209 g, and the plasma supernatant with the underneath buffy coat was collected. The second supernatant, including the buffy coat was then centrifuged at 1500 g for 12 min to sediment the platelets and the clear supernatant phase was collected as PPP. The platelet pellet was resuspended in a volume of PPP to obtain a PRP preparation with a final concentration of 3×106 platelets/μL. The PRP and PPP were stored at −20°C until use.
On the day of the surgery, PRP gel membranes were prepared using: PRP, PPP, bovine thrombin, and Ca gluconate in an 8:1:1:1 ratio, respectively. The gel membrane was prepared in a 3.5-cm culture dish with a total volume of 2.2 mL. Autologous rBMSC were trypsinized, counted, and resuspended in a mixture of 1.6 mL PRP and 200 μL PPP and then decanted in the culture dish. Each gel membrane contained a total of 6×106 rBMSC. Then, a mixture of 200 μL Ca gluconate and 200 μL thrombin (Multifibren U; Siemens) was added, where the final concentration of thrombin in the gel membrane was 9 IU/mL. The gel membrane was then left to jellify at 37°C in 5% CO2 for a minimum of 1 h until surgery.
A nanohydroxyapatite/poly (ester urethane) (nHA/PU) cylindrical scaffold (provided by the AO research institute) with a diameter of 4 mm and height of 15 mm was selected as the scaffold of choice. This scaffold combines the viscoelastic properties of PU with the increased scaffold stiffness and osteoconductive nature offered by nHA allowing maximum host tissue integration with minimal inflammatory response and ease of handling. 23 These scaffolds have also been shown to support ectopic bone formation in the mouse when seeded with human BMSC (data not shown).
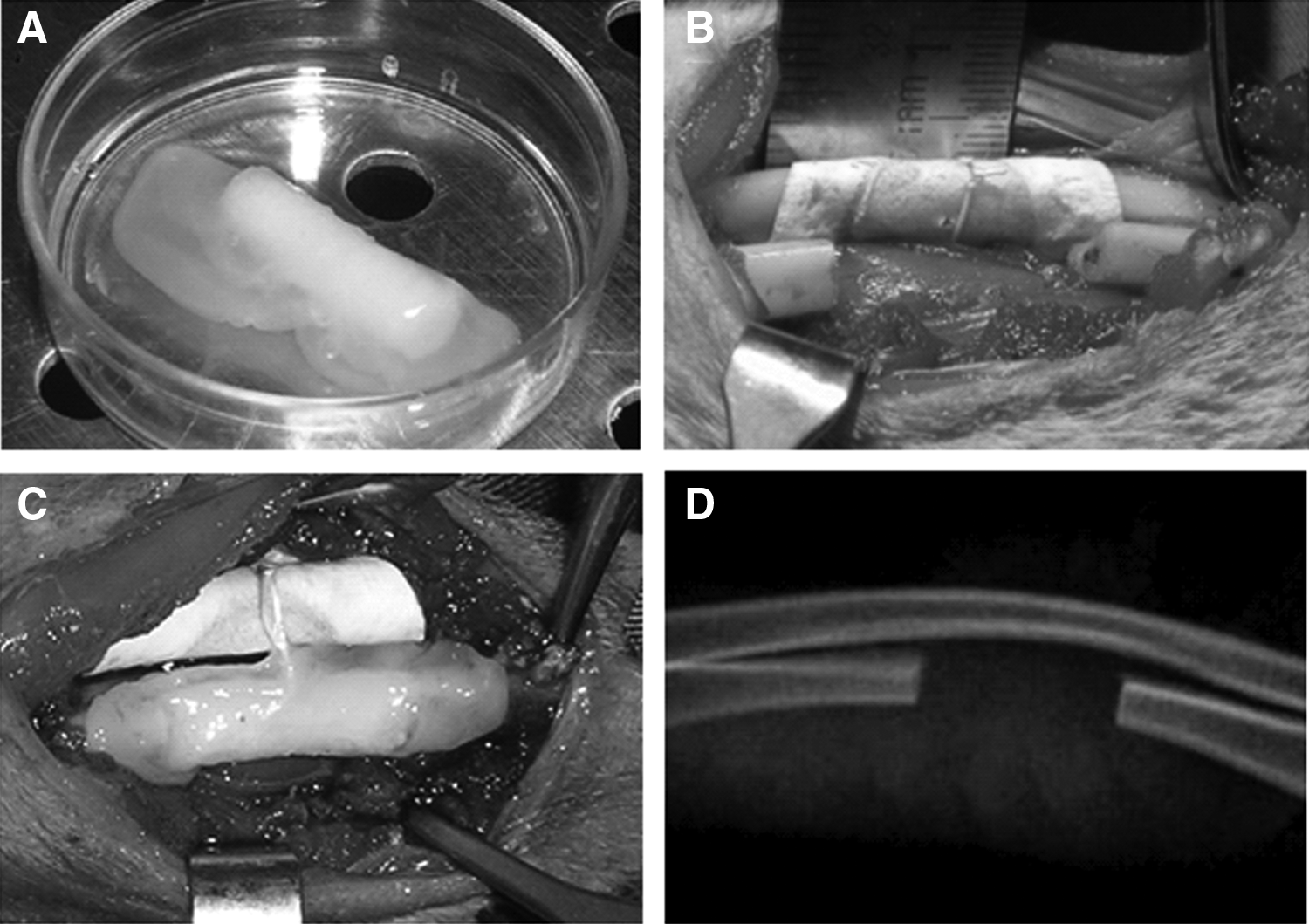
Immediately before surgery, the PRP/rBMSC gel membrane was detached from the dish and wrapped around the scaffold (Fig. 1A). The scaffold was soaked the night before in 500 μL of the same PRP used to prepare the membrane. An excess of 2 mm of the membrane was left from either end of the scaffold to overlap cut bony edges. For the groups not receiving the PRP/rBMSC gel membrane, the scaffold was soaked in PBS (control), or soaked in PRP, and then seeded statically with 6×106 rBMSC.
1.4-cm bone defect in the rabbit ulna.
Animals and surgical procedure
Ten male New Zealand white rabbits were used for the study and they were divided into three groups: Two animals, which received the scaffold with PBS (control, Group A), four animals, which received the scaffold seeded with 6×106 autologous rBMSC (Group B), and four animals, which received the scaffold wrapped with the PRP/autologous rBMSC gel membrane (Group C).
For the surgery, animals were anesthetized first using Diazepam (1 mg/kg; Hospira) followed by Ketamine HCL (35 mg/kg; Merial) and Xylazine HCL (5 mg/kg; Bio 98 Srl). Additionally, an injection of Naropin (ropivacaine HCL, 7.5 mg/mL) (2 mg/mL; AstraZeneca S.p.A.) was given locally at the surgical site to enhance local hemostasis and acute postoperative pain management. The skin was shaved and disinfected and a midline incision along the ulna/radius was done followed by creation of a 1.4-cm segmental bone defect in the ulna using an oscillating saw on a battery hand piece (Howmedica, GmbH) with copious saline irrigation. The periosteum was completely stripped from 2–3 mm of the proximal and distal ends of the cut bony stumps as well as from the adjacent radial surface to ensure maximum elimination of any periosteal tissue remnants. Furthermore, a nonresorbable expanded polytetrafluoroethylene membrane (GORE-TEX, regenerative membrane, W.L. Gore & Associates, Inc.) was interposed between the radius and the ulna at the site of the defect to avoid a possible periosteal reaction and formation of a radioulnar synostosis (Fig. 1B). The scaffold was then inserted under gentle compression and in the case of the PRP/rBMSC gel membrane constructs, the edges of the membrane were adjusted to overlap the denuded bony stumps (Fig. 1C). Subcutaneous tissue layers were then closed with vicryl 4/0 suture thread and for the overlying skin incision 3/0 silk sutures were applied. Animals were followed up daily.
Radiographic assessment and computed microtomography analysis
Postoperative radiographic assessment was performed after 1 week (Fig. 1D), and then monthly until the animals were euthanized. Nine animals were euthanized 4 months postoperatively and one animal from group C was euthanized 6 days postoperatively. Transmission X-ray computed microtomography (μCT) was performed for two representative samples per group using a microfocus X-ray source with cone beam geometry at the TOMOLAB station (www.elettra.trieste.it/Labs/TOMOLAB) according to the following parameters: tube voltage (V)=80 kV, tube current (I)=100 μA, 0.5-mm aluminum filter, exposure time=4 s, 1800 projections collected over 360° rotation, source-object distance=15 cm, source-detector distance=30 cm, resulting isotropic voxel size=12.5 μm. After tomographic acquisitions, 3D images were reconstructed from the series of 2D projections using the classical filtered back projection algorithm. Then, the commercial software VG Studio MAX (Volume Graphics GmbH) was used to produce 3D volume renderings. Bone volume (BV) regenerated in the defect area was calculated in mm3.
Histological analysis
Rabbit ulnas were harvested and fixed in 3.7% paraformaldehyde for 48–72 h at 4°C. Afterward, they were thoroughly washed and maintained in 70% ethanol till processing. The specimens were dehydrated in a graded series of ethanol (70%, 90%, 95%, and absolute ethanol) after which the specimens were infiltrated with the light-curing resin Technovit 7200 VLC (Kulzer). Samples were then polymerized by the EXAKT 520 polymerizator system (EXAKT Technologies). Longitudinal sections passing through both radius and ulna were then cut and ground using the EXAKT 310 CP cutting and EXAKT 400 CS micro grinding units to a final thickness of 30–40 μm. Sections were then stained using Stevenel's blue/Van Geison picro-fuchsin stain (SVG), air-dried, and then sealed with cover slips. Selected sections were also stained with toluidine blue. Images of the sections were acquired using an Axiovert 200M microscope (Zeiss).
Statistical analysis
All data are presented as means and standard deviations. Statistical analysis was performed online using the unpaired Student's t-test by means of the Graphpad software (www.graphpad.com).
Results
Optimization of PRP gel membrane component ratio
PDGF-BB concentration in the supernatants of gels prepared from the six different compositions, demonstrated values higher than the values expected, considering the percentage of the PRP in the gel and the concentration determined in the PRP itself before its combination with the other components (Fig. 2) in agreement with a more efficient platelet lysis during the jellification (comparable to in vivo clot formation). On the contrary, increase of VEGF concentration in the supernatants remained proportional to the percentage of the PRP component volumes. According to the highest availability of both factors and the relative enrichment of VEGF in the gel formed by PRP, cryo, thrombin, and Ca gluconate in the proportions of 8:1:1:1 respectively, we chose this gel composition (P8:C1) for all successive experiments.

PDGF-BB and VEGF contents in supernatants of gels formed starting from different PRP:Cryo proportions. Average maximum PDGF-BB in
BMSC maintained their vitality and proliferative capacity within the PRP gel membrane
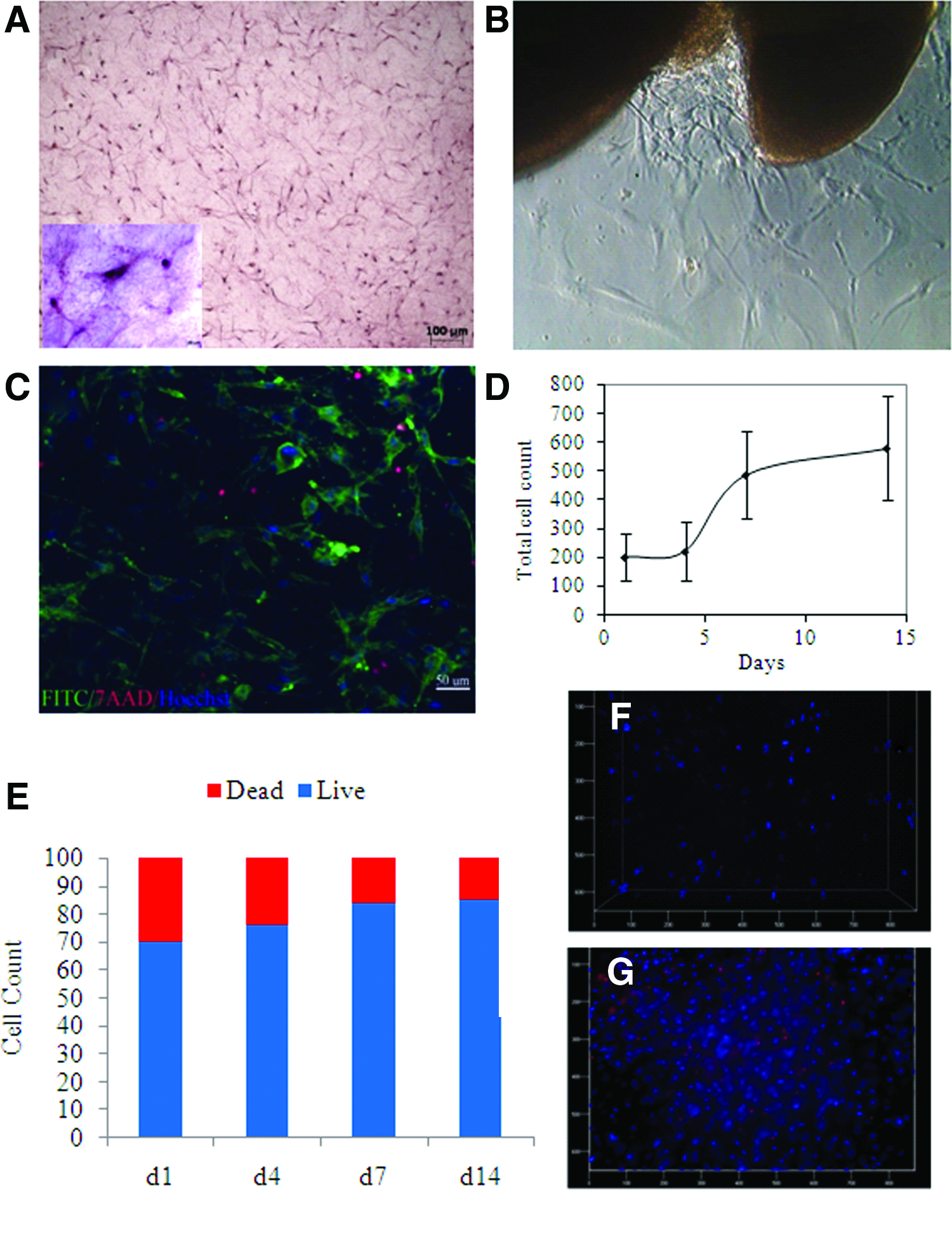
Histological sections of the fixed and stained PRP/hBMSC gel membranes after 14 days in culture showed that the cells were well distributed within the membrane (Fig. 3A). Evidence of dividing cells was also clear (Fig. 3A, insert). Viable cells were able to migrate out of gel remnants after its digestion and successfully attached to the culture dish (Fig. 3B). The number of cells within the gel membrane steadily increased from 1 day to 14 days after culture (Fig. 3C, D). Furthermore, the Live/Dead assay performed at culture day 1, 4, 7, and 14 (Fig. 3E–G) showed that at all four time points the live cells were significantly more abundant that the dead cells (p<0.01), where the percentage of live BMSC was 70% 1 day after incorporation of cells within the gel. This increased to 76% after 4 days and reached 85%–86% after 1 and 2 weeks, respectively. The live cells significantly increased from day 4 to day 7, (p<0.01).
Human BMSC distribution, viability, and proliferation in (P8:C1) PRP gel membrane.
BMSC maintained their osteogenic capacity within the PRP gel membrane
Osteogenically induced PRP/hBMSC gel membranes presented well-defined mineral deposits after 3 weeks of culture as shown by their positive staining with both Alizarin red S and Von Kossa (Fig. 4C, F). Neither stimulated gel membranes (not cell-seeded) (Fig. 4A, D) nor nonstimulated cell-seeded membranes showed any positive staining (Fig. 4B, E). Moreover, mRNA expressions of ALP, BMP-2, RUNX-2, Collagen I, and Osteocalcin from cells extracted from induced and noninduced PRP gel membranes were compared to those of 2D induced and noninduced cells (Fig. 5).
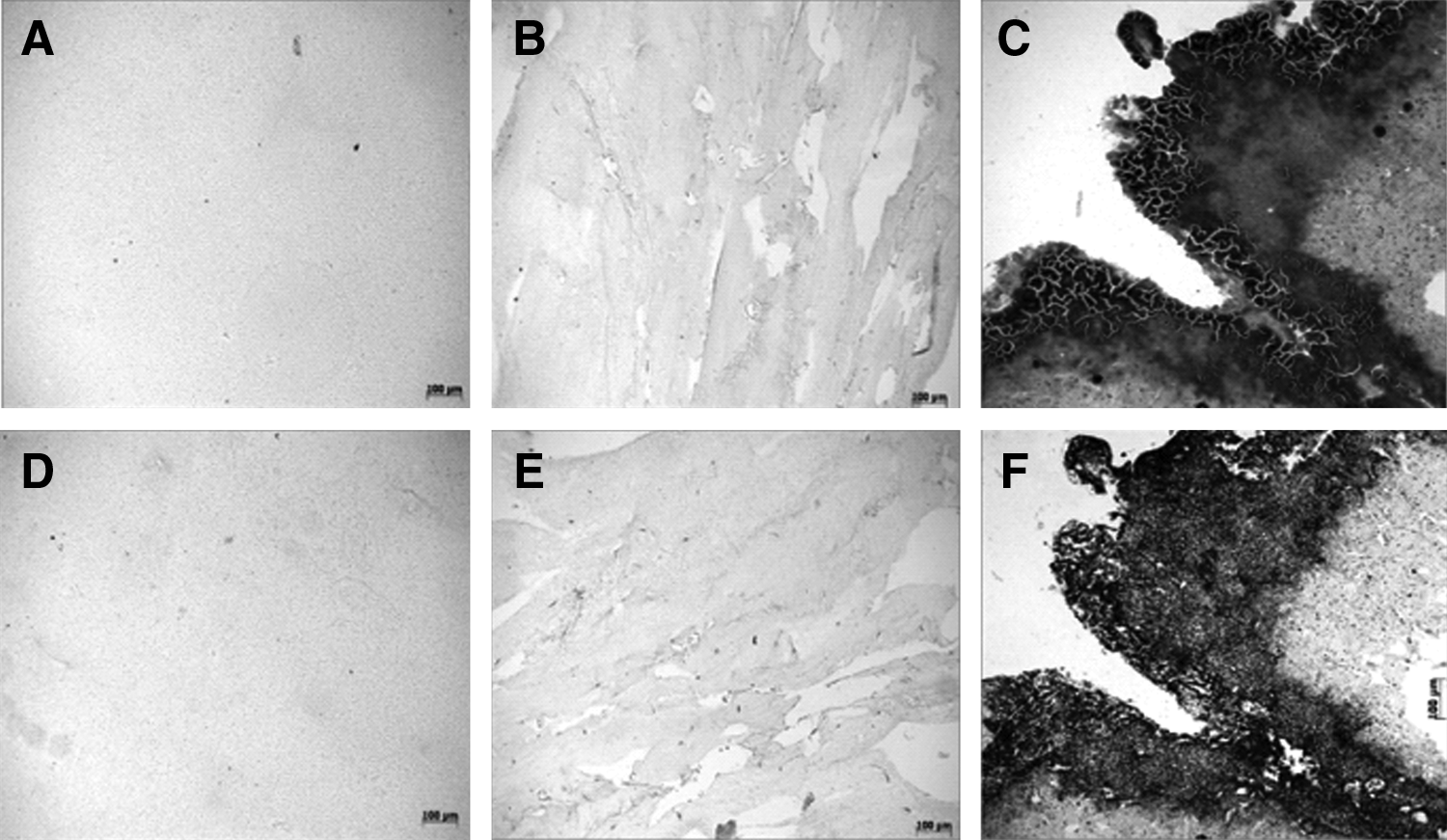
Alizarin red S and Von Kossa staining of ostegenically induced PRP/hBMSC gel membranes in vitro.

Although the levels of mRNA expression for each gene varied substantially among the different donors, the pattern remained the same for all genes analyzed. ALP expression was significantly suppressed in both induced and noninduced gel membranes as compared to the 2D noninduced cells (p<0.05) and significantly expressed in 2D induced cells as compared to 2D noninduced cells (p<0.005), (Fig. 5A). On the other hand, BMP-2 was highly expressed by cells from both induced and noninduced gel membranes, while it was minimally expressed by 2D induced cells and was absent in their controls, yet, only differences between 2D noninduced cells and cells from induced gel membranes were found to be significant (p<0.05), (Fig. 5B). RUNX-2 was significantly expressed by both 2D and gel membrane induced cells as compared to their noninduced counterparts (p<0.05). Furthermore, the levels of RUNX-2 expression were significantly higher from cells of the induced gel membranes compared to 2D induced cells (p<0.05), (Fig. 5C). The expression of osteocalcin was effectively upregulated in both induced 2D and gel membranes, compared to the control counterparts although differences were only significant for the gel membranes (p<0.05), (Fig. 5D). As for collagen I, it remained significantly expressed in the 2D noninduced cells as compared to all other conditions (p<0.05). It was also minimally expressed by 2D induced cells, yet this was significantly higher compared with cells from induced gel membranes (p<0.05), (Fig. 5E).
BMSC cultured in the presence of platelet gel membrane supernatants show distinct ALP and BMP-2 expression
Intrigued by ALP and BMP-2 expression by BMSC inside the gel, we sought to evaluate whether products released from the gel membrane would have similar effects. Indeed, when BMSC were incubated with PRS for 3 days, ALP gene expression was suppressed as compared to the control cells (p<0.05). On the other hand, the expression of BMP-2 was significantly upregulated (p<0.05), (Fig. 5F).
Platelet gel membrane released supernatant induces migration of endothelial cells and stimulates increased production of soluble proangiogenic factors from BMSC
In vitro migration assays showed that human endothelial cells (HUVEC) significantly migrated in response to PRS as compared to serum-free media (*p<0.05) (Fig. 6A). Furthermore, human BMSC incubated in PRS for 3 days significantly increased their production of proangiogenic factors in their conditioned media, such as PDGF-BB, VEGF, and IL-8, when compared to their control counterparts (*p<0.05) (Fig. 6 B–D respectively).

Proof-of-principle: The PRP/BMSC gel membrane enhanced bone repair in a rabbit segmental bone defect
Radiographic and μCT analysis
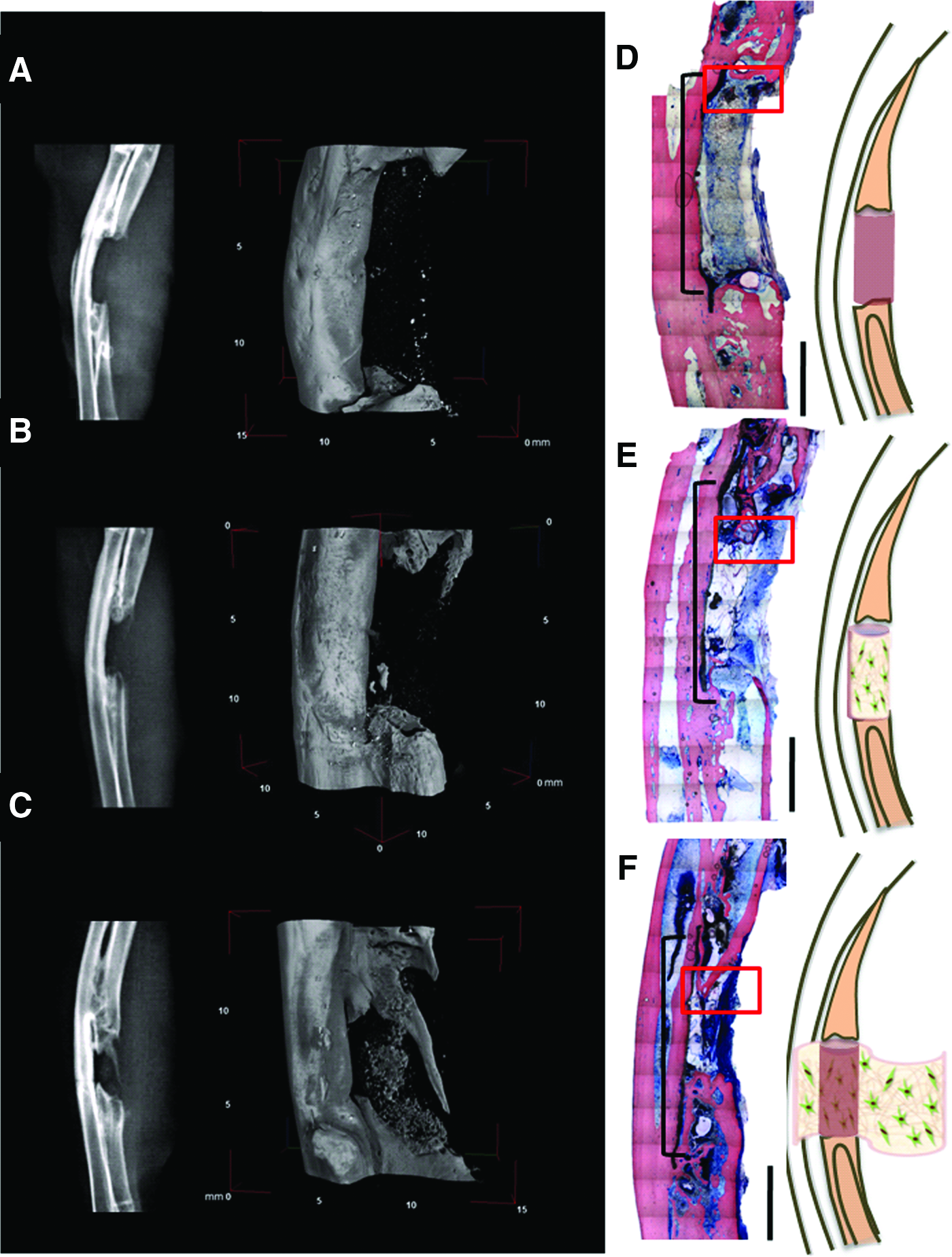
Both radiographic and μCT images revealed that group (A) defects showed no new bone formation (Fig. 7A), group (B) defects showed limited bone formation at the distal and proximal ends of the defect (Fig. 7B), while group (C) defects showed the greatest amount of bone regeneration in the defect area, with the formation of new bone attempting to bridge the defect traversing peripherally, where the PRP/BMSC gel membrane was implanted (Fig. 7C). Additionally, new bone nodules could also be seen accumulating in the central area of the scaffold. No signs of ulna/radius synostosis were evident for any of the groups. Quantification of bone regenerated in the defect area by μCT revealed that for the two samples analyzed per group, the mean BV for group (A) was 14.18 mm3, for group (B) was 19.51 mm3, and for group (C) was 44.30 mm3.
Histological analysis
The gross histological appearance of the defects from the 3 different groups was reconstructed from low-power microphotographs of a representative sample for each group (Fig. 7D–F)
Group (A): Defects implanted with scaffolds soaked in PBS—The size of the defect zone remained comparable to the original defect size with no formation of new bone (Fig. 7D). There is a lack of union between the scaffold and the old bone with dense fibrous tissue strands interposed at the scaffold–bone interface (Fig. 8A). The bone at the margins of the defect is a mature lamellar bone with no signs of remodeling. The scaffold shows minimal resorption and the adipose tissue fills the area between the gore-tex membrane and the remaining cell-infiltrated scaffold (Fig. 8D). The scaffold at the center of the defect is heavily colonized by marrow-derived cells and developing vessel-like structures (Fig. 8G).

Histological images of rabbit segmental bone defects after 4 months stained with SVG showing absence of bone formation in the defect area in group
Group (B): Defects implanted with scaffolds seeded with autologous BMSC in PRP—New bone formation was only evident at the proximal and distal ends of the defect zone with almost no bone formation in the central area (Fig. 7E). Spicules of new bone can be seen at the scaffold–bone interface, bounded by large amounts of adipose tissue and dense fibrous tissue strands mapping out new bone deposition (Fig. 8B). Peripheral areas of the scaffold are actively undergoing resorption and being replaced by a newly deposited bone matrix (Fig. 8E). The scaffold center is occupied by highly cellular fibrous tissue that is heavily infiltrated by marrow-derived cells and multinucleated giant cells (Fig. 8H).
Group (C): Defects implanted with scaffolds wrapped with PRP/BMSC gel membranes—In this group, the defect area appears filled with new bone showing definite cortical plates and a developing marrow core (Fig. 7F). There is a bony bridge traversing the defect area in a peripheral to central direction guided by the PRP/BMSC gel membrane and parallel to the gore-tex membrane (Fig. 8C). There is a well-defined bony union with a continued deposition of new bone matrix replacing the scaffold structure. Remodeling trabecular structures with osteoid seams can be seen as well as mature marrow and blood vessels (Fig. 8F). Dense mineralizing collagen bundles are clear at the edges of the newly forming bone intertwined with the scaffold (Fig. 8I). Mineralized deposits could also be seen within the remaining scaffold and the organization of vessel-like structures in the central areas of the implant with heavy accumulation of marrow-derived cells (Fig. 8I, insert).
To shed light on the possible mechanism of function and early healing events occurring in the defects implanted with the PRP/BMSC gel membrane/scaffold construct, one sample of this group was additionally processed after 6 days of implantation. This also served to understand the degradation logistics of the gel membrane in vivo after 1 week. The structure of the PRP/BMSC gel membrane was intact to a great extent on both the external and internal surfaces of the defect as well as overlapping the denuded edges of the cut bone (Fig. 9A, B). Interestingly, islands of hypertrophic cartilage (Fig. 9C, E) were seen within the implanted PRP/BMSC gel membrane. Numerous inflammatory cells could also be seen within the membrane interspersed among the seeded cells (Fig. 9D, F).

Histological images of rabbit segmental bone defect from group
Discussion
The ability of the autograft to trigger bone formation has been attributed to periosteum-initiated events.7,10 Targeting periosteum-mediated bone repair by engineering a periosteal substitute with both angiogenic and osteogenic properties offers the advantages of healing via a natural response, optimal bone integrity, appropriate vascularization, and minimal ectopic ossification. 24
Recently, studies have investigated the potential of periosteal cell cultures for tissue engineering applications,25,26 yet, they are not without significant limitations. 27 As a result, substrates of small intestinal submucosa 11 or acellular dermal matrix have been employed. 28
We herein present a strategy for improving bone engineering by designing a periosteal substitute to simultaneously support new bone deposition and implant vascularization. We hypothesized that the PRP GF-rich environment would boost the contained stem/osteoprogenitor cells' potential, while adding proangiogenic properties and modulating the early inflammatory response within the bone defect. 29
The amount of PDGF-BB and VEGF from different gel compositions tested was consistent with the literature, 22 whereby the calculated average PDGF-BB content exceeded the expected value, yet, the average VEGF content precisely coincided with the expected concentration. This could be explained by the higher affinity of fibrin, the major component of the cryo fraction and the backbone of the gel, for VEGF in respect to PDGF. 30 Compared to gels reported to be activated by 142.8 U/mL bovine thrombin, 22 our protocol rendered a higher GF content in the gel supernatants with the P8:C1 gels showing highest release of GFs. We noted that BMSC did not survive the 140 U/mL bovine thrombin concentration (data not shown). Although initial cell death was noted in the chosen P8:C1 PRP gel membranes, the percentage of live cells increased with time indicating proliferating cells that substituted those that die during gel preparation. This was also demonstrated by the increased cell count from day 1 to 14.
Positive mineral staining of induced gel membranes confirmed the entrapped BMSC's ability to undergo osteogenic differentiation. Osteogenic gene analysis showed that the PRP environment either as a gel matrix or as a culture supernatant (PRS) seemed, consistently with previously reported data 31 to spontaneously modulate BMP-2 expression from BMSC.
RUNX2 and Osteocalcin, which are known in turn to be controlled by BMPs 32 were highly expressed in the cells in the induced gel membranes. RUNX2, although an early osteogenic marker, is also expressed in high levels in differentiated osteoblasts in postnatal life. 33 This could be indicative of a more mature osteoblastic phenotype within the induced gels. This may also reflect continued osteogenic differentiation triggered by a BMP-2-dependent autocrine loop acting on different population subsets of BMSC within the gel. 31
On the other hand, Collagen I expression in the induced gels appeared to be downregulated coinciding with matrix maturation and mineralization. 34 As for ALP, its suppression upon exposure to PRS has been previously reported in the context of an osteogenic inhibitory role. 35 However, in the present study, the suppression of ALP whether in induced gels or in PRS-treated BMSC in the same culture demonstrating elevated BMP-2 levels may further support the hypothesis of a BMP-2-dependent mechanism independent of ALP. 31 While BMP-2 consistently induces ALP in rat and mouse marrow stromal cells,32,36 it fails to do so in human cells possibly pointing to nonclassical pathways, and perhaps, involving a Wnt-signaling cascade. BMP signaling may also involve several other transcriptional factors, which in turn regulate subsets of osteoblastic genes. We, hence, speculate that the cells in the gel membrane are maintained in a proliferative osteoprogenitor state, yet do not progress to a fully mature osteoblast phenotype (expressing RUNX-2 and Osteocalcin) unless they find the suitable osteogenic environment, which would in turn be mediated by the phase of bone repair.
As bone deposition is highly dependent on vascularization, the PRP gel membrane supernatant's ability to induce endothelial cell migration may reflect an enhanced angiogenic capacity. This, coupled also by the fact that PRS significantly increased PDGF-BB, VEGF, and IL-8 secretion from BMSC could confirm a tendency for creating an angiogenesis-favoring environment.37,38 BMSC have the ability to become activated and to secrete a variety of bioactive molecules in response to local injury, 39 effects which could be accentuated in the presence of the PRP gel membrane and/or its released products.
Our in vivo data, confirmed the angio-osteogenic potential of the engineered periosteal substitute both ectopically in the mouse (Supplementary Fig. S1; Supplementary Data are available online at www.liebertonline.com/tea) and orthotopically in the rabbit. Indeed, as proof-of-principle, we demonstrated that the critical-sized rabbit ulna defect receiving the nanohydroxypaptite poly (ester urethane) scaffold enveloped by the PRP/rBMSC gel membrane showed a substantially higher bone filling compared to the empty and cell-bearing scaffold controls. However, after a period of 4 months, the defects receiving the substitute were not completely bridged, possibly indicating the need for longer time periods in such a compromised model, or for increasing the number of delivered cells.
Although our PRP/BMSC gel membrane may not anatomically mimic the periosteum, we believe that it is capable of mimicking a periosteal response. Interestingly, the presence of cartilage islands in the implanted PRP/BMSC gel membrane after 6 days in vivo, hints to the possible involvement of an endochondral pathway of bone formation triggered by the membrane.
The interaction between the fracture hematoma and the periosteum during the early phases of bone repair is important for initiating a cascade of cellular events, cytokine production, and GF availability. 15 The PRP/BMSC gel membrane may create a microenvironment similar to that of the fracture hematoma directing the proliferation and differentiation of MSC as well as inducing recruitment of vessels and other multipotent stem cells to the area (see also diagram in Fig. 10). It is possible that the angiogenic and osteogenic effects of our periosteal substitute take place via a BMP-2-dependent pathway triggering an autocrine mechanism. It is known that BMP-2 expression occurs in the early periosteal callus 10 and is responsible for regulating the periosteal cell fate during bone repair. 40
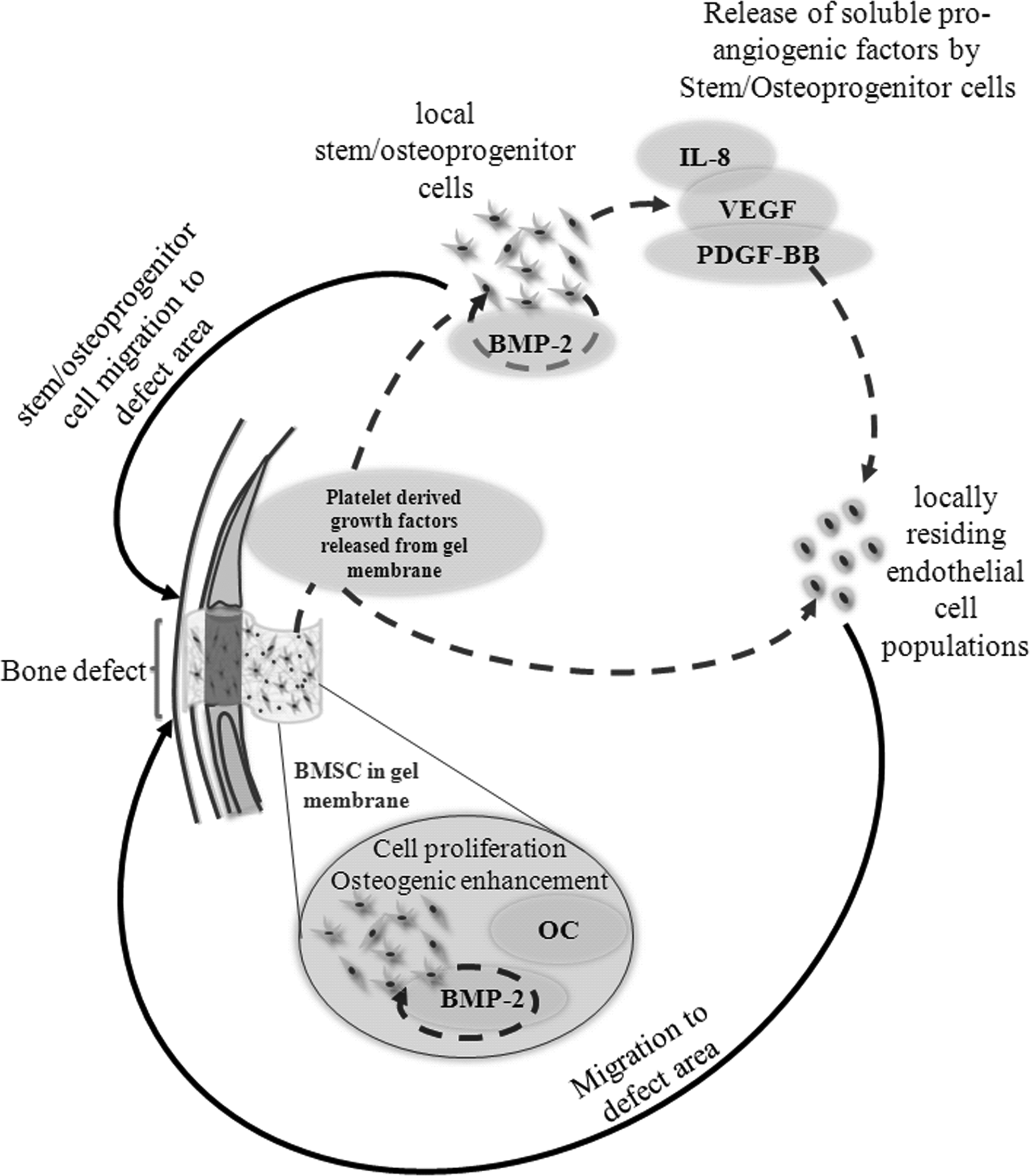
Diagram depicting the possible mechanism of function of the PRP/BMSC gel membrane as a periosteal substitute for bone engineering.
Our approach fulfills the three major requirements for engineering a functional periosteum; live osteogenic cells, osteoconductive scaffold, and osteoinductive genes or factors. 10 Engineering a periosteal substitute that can mimic a periosteal-mediated response will also provide further insight on the interactions between osteogenesis and angiogenesis during bone repair.
Conclusion
In this study, we engineered and characterized a PRP gel membrane entrapping BMSC that could mimic the natural periosteum in supporting both ectopic and orthotopic bone regeneration. The combined effect of the released GFs from the gel as well as from BMSC, both within the gel and host recruited, may contribute to the improvement of bone regeneration by creating a more favorable angiogenic and osteogenic environment. Following the notion that a 2D periosteum creates a 3D bone, the engineered periosteal substitute could represent a fourfold clinical or translational benefit: (1) it is an on-hand cell/matrix construct; (2) provides an osteogenic and angiogenic factor-rich microenvironment; (3) could be fully available from an autologous source; (4) the malleability of the membrane presents a functional potential support for irregular bone lesions, such as periodontal and head and neck bone defects.
Footnotes
Acknowledgments
This work was supported partially by funds from the European Union FP7, Regione Liguria (F.E.S.R.), and UPMC-Pittsburgh. The authors would like to thank Patrizio Castagnola, Chiara Ottonello, Giuliana Tromba, Francesco Monetti, and Paolo Strada for their experimental help and advice, and Mauro Alini for providing the poly (ester urethane) scaffold.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.