
Abstract
The biomechanical functionality of articular cartilage is derived from both its biochemical composition and the architecture of the collagen network. Failure to replicate this normal Benninghoff architecture in regenerating articular cartilage may in turn predispose the tissue to failure. In this article, the influence of the maturity (or functionality) of a tissue-engineered construct at the time of implantation into a tibial chondral defect on the likelihood of recapitulating a normal Benninghoff architecture was investigated using a computational model featuring a collagen remodeling algorithm. Such a normal tissue architecture was predicted to form in the intact tibial plateau due to the interplay between the depth-dependent extracellular matrix properties, foremost swelling pressures, and external mechanical loading. In the presence of even small empty defects in the articular surface, the collagen architecture in the surrounding cartilage was predicted to deviate significantly from the native state, indicating a possible predisposition for osteoarthritic changes. These negative alterations were alleviated by the implantation of tissue-engineered cartilage, where a mature implant was predicted to result in the formation of a more native-like collagen architecture than immature implants. The results of this study highlight the importance of cartilage graft functionality to maintain and/or re-establish joint function and suggest that engineering a tissue with a native depth-dependent composition may facilitate the establishment of a normal Benninghoff collagen architecture after implantation into load-bearing defects.
Introduction
The limits within which adaptation is possible are, however, exceeded when the cartilage is injured. The lack of spontaneous repair in chondral defects has been attributed to the lack of proliferating cells and a scaffold into which these cells can migrate. 7 Untreated defects, even focal defects of limited size, often extend to full-thickness defects over time and can eventually lead to the degeneration of the surrounding healthy cartilage tissue.8,9 None of the existing clinical treatments for chondral defects can be regarded as completely satisfactory or consistently successful (for a review see Hunziker 8 ).
Numerous tissue engineering and regenerative medicine strategies, including autologous chondrocyte implantation (ACI), 10 chondrocyte transplantation in scaffolds (e.g., matrix-assisted autologous chondrocyte implantation), 7 growth factor-guided cell therapies,11,12 and the delivery of progenitor cells13,14 are either in clinical practice or under investigation. Bioreactor culture is often used with the intention of engineering a more functional tissue in vitro.15–20 In vitro preculture of engineered implants or predifferentiation of mesenchymal stem cells have generally resulted in improved in vivo outcomes,21,22 although recapitulating the spatial organization of the native tissue has proven difficult, and the overall repair tissue quality is typically inferior to normal articular cartilage.12,21,23 After growth factor-facilitated repair in partial thickness chondral defects, tissue architecture was observed to be more isotropic than in normal articular cartilage. 12 Similar observations have been made after the use of cell-based therapies for the repair of full-thickness chondral and osteochondral defects.24,25 A partial formation of a native-like zonal collagen architecture has been observed in smaller cartilage defects treated with ACI, 26 while microfracture-based repair may be capable of producing repair tissue recapitulating certain aspects of a native-like stratified architecture. 27 In terms of tissue engineering cartilaginous grafts, it is still unclear how mechanically functional such a construct should be before implantation into a load-bearing cartilage defect,28,29 and how such properties will impact the in vivo development of the regenerating tissue.
Given that a failure to recapitulate the normal collagen architecture of articular cartilage will most likely lead to the long-term failure of the repair tissue, this study sought to develop a theoretical framework within which the role of the joint mechanical environment on the organization of the repair tissue in cartilage defects could be better understood. It has been shown that composition-based constitutive modeling in combination with collagen remodeling algorithms is capable of predicting the Benninghoff architecture in tibial plateau cartilage based on the interplay between swelling pressures and external loading. 30 We have further demonstrated that a collagen-remodeling algorithm 31 can explain aspects of altered structure–function relationships in tissue-engineered cartilage due to mechanical loading during bioreactor culture. 5 The objective of this study was first to use the same modeling framework to investigate the effect of chondral defect size and depth on remodeling of the collagen architecture in the surrounding undamaged cartilage. This model is then used to predict how the repair and undamaged surrounding tissue architecture would adapt over time after the implantation of tissue-engineered cartilage of varying biochemical composition (parameterized in terms of graft collagen content, fixed charge density, and water content). It was hypothesized that (1) in untreated defects, the degree of remodeling away from a normal Benninghoff architecture in the surrounding undamaged cartilage is a function of the defect size, and (2) successful recapitulation of a Benninghoff architecture in vivo within tissue-engineered cartilage depends on the construct composition at the time of implantation.
Materials and Methods
Computational models of collagen remodeling in response to mechanical cues have been used to demonstrate that a Benninghoff architecture develops in intact tibial plateau cartilage in response to external loading and internal swelling pressures. 30 The geometry and the mathematical relationships regarding the depth-dependent composition used in that study were adopted here and combined with a model of collagen remodeling in cartilaginous tissues5,31 to establish a numerical (undamaged or intact tissue) control against which the predictions of the defect simulations were compared (see section Study design). In this model, the collagen fiber distributions in a point were allowed to gradually change their orientation and degree of alignment depending on the deformation at that location. Generally speaking, fibers were modeled to preferentially align with respect to directions of tensile strain as illustrated in Figure 1. We briefly outline the most relevant theory here, but refer the reader to the above articles for more details. Readers uninterested in details related to the technical implementation of the model may proceed directly to the section Study design.
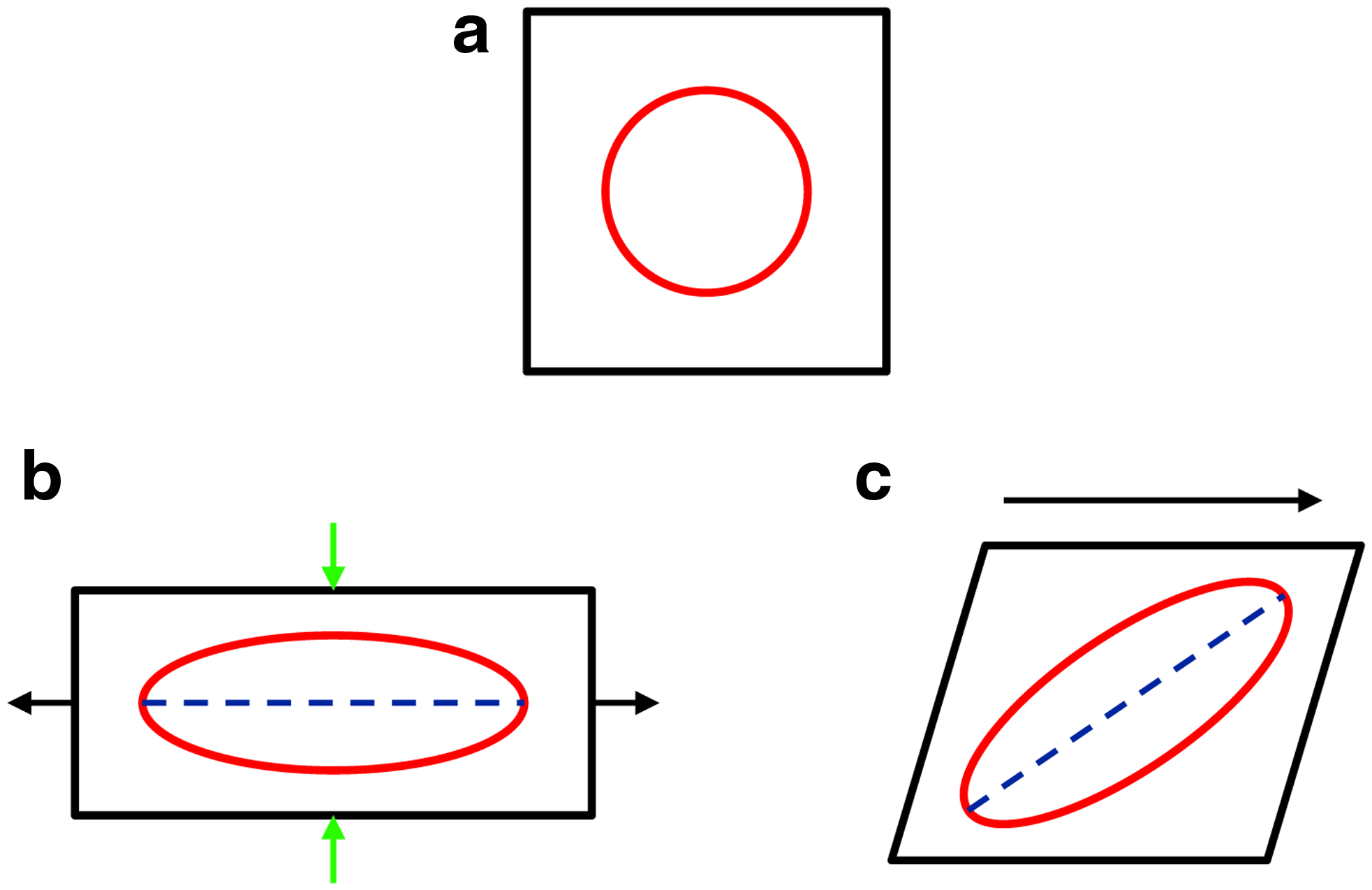
Illustration of remodeling principle. An initially isotropic fiber architecture
Depth-dependent composition of articular cartilage
With the introduction of a dimensionless coordinate
Under the assumption of equal true mass densities for all solid constituents, the total collagen mass fraction (collagen per wet weight) could be calculated using
where
Fiber remodeling
The collagen fiber distributions in a point were allowed to gradually change their orientation and degree of alignment depending on the deformation at that location. Generally speaking, fibers were modeled to preferentially align with respect to directions of tensile strain as illustrated in Figure 1.
For details on the remodeling formulation, we refer the reader to5,31 and the additional information presented in the Supplementary Material (section Fiber remodeling).
Geometry and boundary conditions
The axisymmetric geometry of the tibial plateau used in 30 was adopted here (see Figure 2). A compressive load of 800 N (estimated force per knee compartment, assuming an equal load acting on the medial and lateral compartments, for a body weight of 65 kg and an average axial force in the knee joint of 2.5 times body weight) was applied to the tibial plateau within a 0.5 s ramp to represent a step33,34 via a rigid, impermeable platen after the initial swelling deformations had converged and established the prestress in the collagen network. Free surfaces were modeled as free draining; others as sealed. All displacements were suppressed at the subchondral bone junction, and full integration between the implant and the host cartilage was assumed. Mixed formulation elements were used with biquadratic interpolation for the displacements and bilinear interpolation for the pore pressure.

Axisymmetric model of tibial plateau cartilage. The mesh was refined in regions of increased interest (center of the tibial plateau, where defects will be created). Color images available online at www.liebertpub.com/tea
At maximum load the deformations were analyzed and used to drive remodeling as described in the previous section. The iterational loop was then repeated starting with the free swelling step and based on the new material properties and structure to derive the deformations in the next iteration of the simulation.
Study design
Several simulations were performed to establish the influence of defect size and implanted engineered tissue composition on tissue architecture that was parameterized in terms of the principal fiber direction. Near-isotropic regions of the collagen network, that is, spherical distributions, were excluded from the evaluation due to ill-defined angles in this case (i.e., a sphere does not have a preferred direction. A meaningful angular measure of alignment can therefore not be assigned). The threshold chosen was a deviation in eigenvalues of <2%. All simulations were run until no change in fiber architecture was observed (steady state). The following groups were investigated.
Control group
The resulting Benninghoff collagen architecture that is predicted to form in the defect-free tissue in response to proteoglycan-induced swelling and external joint loading serves as a numerical control and defines the healthy architecture against which all other predictions will be compared. Establishment of a numerical control is necessary, as the details of the predicted fiber architecture will depend on the exact loading protocol, geometry, and material properties inherent in the model. These assumptions are common to all subsequent models that constitute perturbed versions of the healthy numerical control. Similar approaches are taken experimentally. 27
Empty defect group
Three full-thickness and three partial-thickness (extending 1.2 mm into the tissue) defects were created with diameters of 2, 4, and 6 mm. Defect surfaces were modeled as free draining. Average angular deviations with respect to the control group were calculated based on the 2D cross-sectional model representation.
Implants group
The three full-thickness defects were filled with cartilage-like engineered tissue that exhibited no depth dependency in its composition. Depending on extracellular matrix (ECM) content, these constructs were classified as (1) immature: porosity φF0=0.98, fixed charge density cF0=1.4×10−5 mEq mm3, 1.6% w/ww collagen content; (2) medium: porosity φF0=0.85, fixed charge density cF0=7.1×10−5 mEq mm3, 7.9% w/ww collagen content; or (3) mature: porosity φF0=0.77, fixed charge density cF0=1.41×10−4 mEq mm3, 15.8% w/ww collagen content.
These values for the fixed charge density (related to proteoglycan content) and collagen content were chosen to correspond to 100% (mature), 50% (medium), and 10% (immature) of the average deep-zone values (bottom 75% of the tissue thickness) in native articular cartilage. While a construct corresponding to the mature case has not yet been engineered, it was included because it represents the goal of current functional tissue engineering research. No further ECM synthesis was assumed to occur.
Results
The mechanical environment created by external joint loading and internal swelling pressures leads to the prediction of a Benninghoff-like architecture in defect-free cartilage
A Benninghoff-like collagen architecture was predicted in the defect-free (or numerical control) model (Fig. 3). The principal fiber direction, designated by the long axis of the ellipsoidal fiber distribution, was predicted to be aligned vertically in the deep zone and went through a symmetric transition via an isotropic (i.e., more random) state toward a horizontal alignment in the superficial zone. With increasing distance from the center of the tibial plateau, the transition was increasingly asymmetric; that is, fibers preferentially bent over toward the periphery and did so earlier than in the central regions. The thickness of the superficial zone as well as the distance from the center at which the fibers being to bend toward the periphery depend on both the magnitude of the applied load and the relaxation time (see Supplementary Fig. S1).
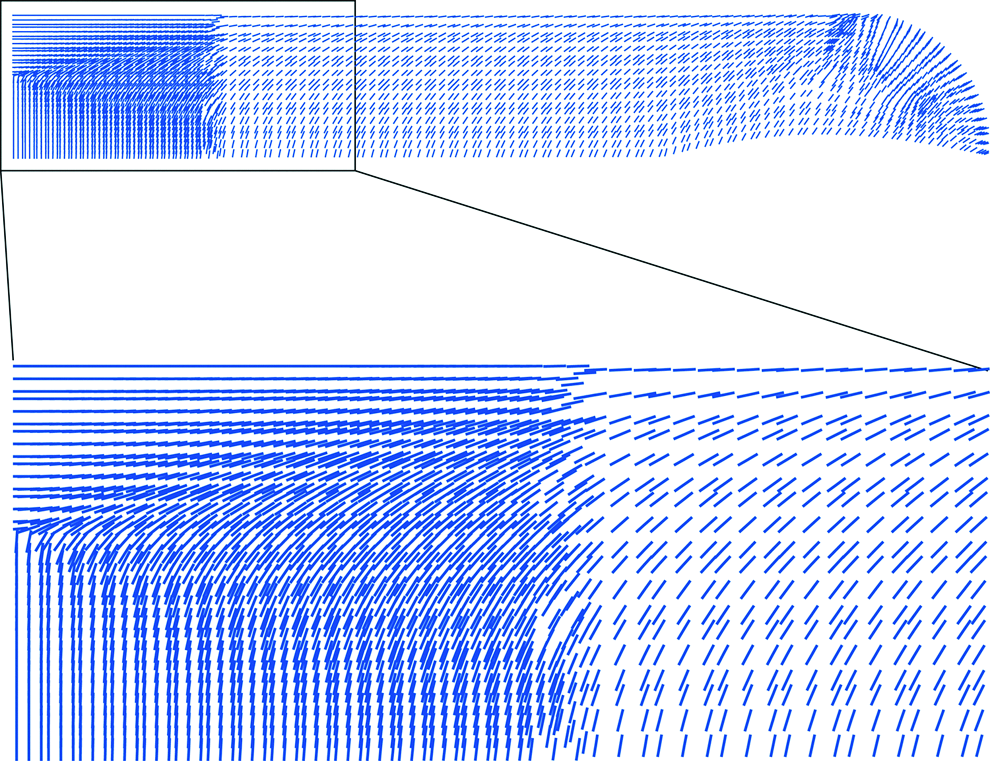
Fiber architecture in intact tibial plateau. Fibers are assumed to align with principal strain directions in response to swelling and external loading. Directions plotted designate the long axis of the ellipsoid anisotropy representation. Color images available online at www.liebertpub.com/tea
Initially undamaged articular cartilage surrounding an empty defect is predicted to become increasingly disorganized as the size of the defect increases
Creating a defect within the articular surface is predicted to alter the mechanical environment within the surrounding tissue, leading to remodeling of this initially undamaged tissue away from a normal Benninghoff-type collagen architecture. Significant deviations between the predicted predominant fiber angle (the long axis of the ellipse illustrated in Fig. 1) in the normal tissue and the damaged tissue (≥50°) were observed far into the intact tibial plateau (Fig. 4). The asymmetric fiber transition reversed from a peripheral (outward) to a central (inward) direction in the regions adjacent to the defect. The affected regions within the tissue increased with defect size (Fig. 5). For a 6-mm defect, only a small peripheral region of the articular surface had angular deviations of <5° from the normal Benninghoff architecture. The predominant collagen fiber alignment was predicted to deviate more than 50° from the Benninghoff architecture in a region extending to four times the defect radius. Similar trends were predicted in the partial-thickness simulations where the surrounding cartilage was only slightly less affected than in the full-thickness defect. Remodeling was also observed in the cartilage underlying the partial-thickness defect. When averaged over the entire tibial plateau, deviations were predicted to be between 15° and 25° (Fig. 5).
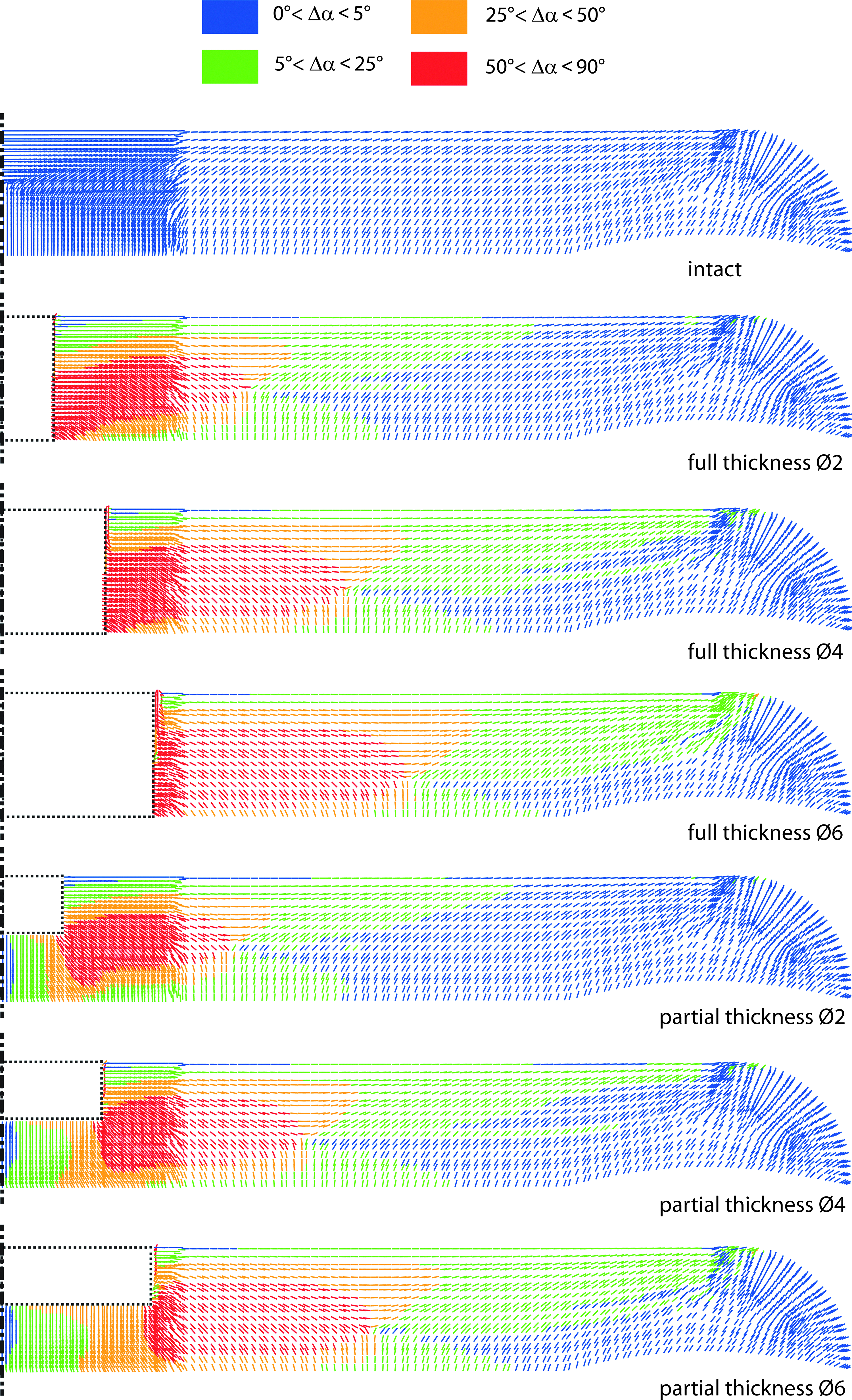
Fiber architecture in tibial plateau with defects. Blue corresponds to <5° difference compared to intact Benninghoff architecture, green to <25°, orange to <50°, and red to more than 50°. Dashed boxes represent defect areas. Color images available online at www.liebertpub.com/tea

Average angular deviation of predicted steady-state architecture from the normal Benninghoff architecture in the tibial plateau with empty defects. Color images available online at www.liebertpub.com/tea
The maturity of an engineered graft at the time of implantation is predicted to determine the likelihood of recapitulating a normal cartilage architecture in the regenerate
Independent of defect size, implanting a more mature engineered tissue was predicted to result in remodeling toward a more native-like architecture in the repair tissue (Fig. 6a–c). For engineered tissues with low or intermediate ECM content, the repair tissue failed to recapitulate a native-like collagen architecture, particularly in the superficial and middle zone. A more Benninghoff-like architecture was predicted after implantation of a mature construct (Fig. 7). The predicted fiber architecture can be explained by the composition–function relationships of the regenerating tissue. The less-mature implants have a lower compressive strength and intrinsic Poisson's ratio throughout their depth due to the low concentration of ECM constituents. The more superficial layers therefore experience lower-than-normal levels of lateral expansion during compressive loading, which does not facilitate a normal horizontal fiber arrangement in the superficial region of the repair tissue. The surrounding stiffer tissue acts to further inhibit this lateral expansion. In contrast, the mature construct is very stiff, and the tissue expands laterally due to its higher Poisson's ratio and the higher stiffness relative to the surrounding cartilage. Because the entire construct is homogeneous, much of the axial load gets transmitted into the deeper layers that become compressed more than they normally would with a native-like heterogeneous composition. Thus, deep-zone recapitulation deteriorates slightly under these conditions. In contrast to the immature constructs, the mature engineered cartilage was predicted to successfully recapitulate the collagen architecture in the superficial zone. All implants stabilized the surrounding tissue significantly during dynamic loading with more mature engineered implants predicted to result in less remodeling of the surrounding undamaged cartilage away from a normal Benninghoff architecture (Figs. 6d and 7).

Average angular deviation of predicted steady-state architecture in the superficial, middle, and deep zone of defects treated with tissue-engineered constructs
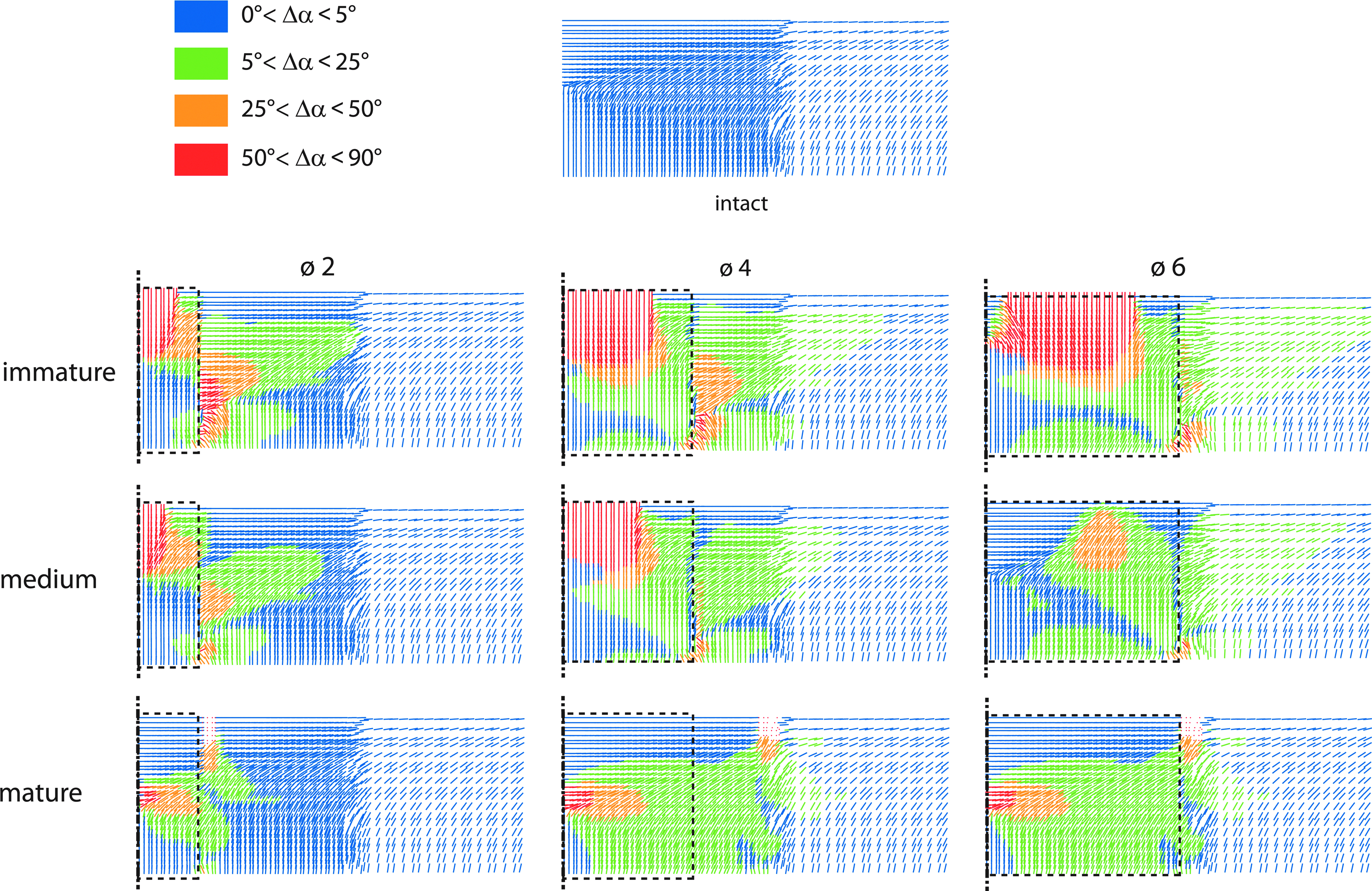
Fiber architecture in and around defects when a constant biochemical composition is maintained both spatially and temporally. Composition at implantation classified as mature, medium, or immature. Blue corresponds to <5° difference compared to intact Benninghoff architecture, green to <25°, orange to <50°, and red to more than 50°. Empty areas correspond to circumferential alignment of the preferential fiber direction. Color images available online at www.liebertpub.com/tea
Discussion
In this study, the effect of defect size and the composition of tissue-engineered cartilage implanted to treat such defects on the resulting tissue architecture were evaluated using a computational model of collagen remodeling. The model predicts that (1) even small defects (∅ 2 mm) have adverse effects on the mechanical environment in a significant portion of the surrounding healthy tissue; (2) these effects increased with defect size; (3) mature tissue-engineered cartilage is more successful at stabilizing the surrounding cartilage than immature implants; (4) mature tissue-engineered constructs create a mechanical environment in the regenerating tissue that better facilitates the re-establishment of a Benninghoff-type architecture in the repair tissue. These model predictions help to explain the results of recent in vivo studies, demonstrating that cartilage repair tissue becomes more hyaline-like as the maturity of an engineered tissue is increased preimplantation. 35
The prediction of a Benninghoff-like architecture in intact cartilage with native-like gradients in its biochemical composition (parameterized in terms of collagen content, fixed charge density, and water content) was in agreement with previous models 30 and experimental observations.36–38 The earlier transition toward horizontal alignment closer to peripheral regions has been documented in scanning electron microscopy studies.37,38 The symmetric transition of ellipsoidal fiber representations from vertical to horizontal alignment has been observed in central high-load-bearing regions, and the asymmetric transition with turning ellipsoids from vertical to horizontal alignment has been associated with peripheral joint regions 39 and was predicted by the model. These correlations between model predictions and experimental observations provide strong support for the hypothesis that collagen fiber alignment in articular cartilage is driven by mechanical cues.
Untreated chondral defects have been shown to increase in size and frequency 40 and generally lead to degeneration and osteoarthritic changes in the tissue. 9 Mechanical loading influences the synthesis of matrix metalloproteinases (MMPs), tissue inhibitors of metalloproteinases (TIMPs), and aggrecanases that are relevant for tissue maintenance, degradation, and remodeling. 41 The altered mechanical environment in the presence of defects most likely disturbs the mechanobiological homeostasis of the resident cell population. Under such conditions, the model predicts that aggravated by increasing defect size, the collagen architecture deviates from the native architecture present in healthy tissue. Assuming that mature articular cartilage is incapable of remodeling to the extent predicted by the model, this indicates that the native architecture in these regions is no longer ideally aligned to support the applied loads. The altered strain states in the collagen network of articular cartilage surrounding a defect can make it more susceptible to biochemical degradation 42 and lead to further deterioration of the structural integrity of the ECM.
To prevent or hinder the occurrence of such adverse effects, the damaged articular surface needs to be stabilized after injury. The unsatisfactory results of current clinical treatments for chondral defects present a strong motivation for tissue-engineering strategies. 8 There is debate as to the required functionality of an engineered tissue at the time of implantation, and it has been argued that due to the adaptive nature of the joint as a whole, the ideal properties of a tissue replacement vary over time and can be anywhere from below native properties to higher-than native depending on the state of the surrounding tissues. 43 The primary goal of tissue engineering in this context is to restore joint function. 44 The engineered graft should also serve to prevent further degeneration in the surrounding tissue by stabilizing the adjacent cartilage and provide a continuous smooth surface to avoid stress concentrations and excessive shear. In the simulations presented in this article, the mature implant was most successful in stabilizing the native cartilage and creating an internal mechanical environment within the regenerating tissue that provides appropriate stimuli to form (or support) a native-like Benninghoff architecture. The immature implants are very soft compared to articular cartilage, and thus carry a low proportion of the load, which limits their effectiveness for stabilizing the defect walls against bulging into the defect. This effect will become more pronounced during transient loading with loss of fluid load support.
It has been recognized that the depth-dependent organization and composition of articular cartilage are prerequisites for its function, and that tissue engineers should strive to recapitulate these gradients via different cell sources, biomaterials, gradients in scaffold mechanical properties, and signaling molecules. 45 The gradients that developed in the mature implants in vivo and resulted in a depth-dependent architecture will not develop in vitro in implants engineered under homogeneous environmental culture conditions. A re-establishment of the native depth-dependent composition via synthetic cell activities guided by location-dependent cues may create the necessary stimuli for the development of a native tissue architecture (similar to the healthy model presented above). The ideal tissue-engineered construct would thus possess a depth-dependent composition mimicking that of normal articular cartilage, as under such conditions, a Benninghoff-like architecture is predicted (Fig. 3). One way to achieve the desired composition or architecture might be using scaffolds as guiding structures,46–48 or to modulate the environment through the depth of the developing tissue to engineer constructs with native-like gradients in biochemical composition. 49
Basic parts of the presented model were based on previously published work,30,32 namely the depth-dependent composition and the geometry, with some associated limitations. The employed material model, however, was different, and the loading protocol was simplified due to high computational demands associated with the material model and the time scales considered. Despite these model differences, a Benninghoff-like architecture was recovered in accordance with the previous models, 30 with the exact organization depending on the applied loading conditions (see Supplementary Fig. S1). This confirms that the relevant model aspects for this prediction are the depth-dependent mechanical properties and composition, specifically the depth-dependent swelling pressures, as well as joint loading. External loading compresses top layers more than the deep zone, which is in line with the established cartilage biomechanics literature.50,51 While the actual joint geometry, kinematics, and contact conditions are significantly more complex than our model representation, this interplay between depth-dependent swelling and external loading is expected to be a common characteristic in the knee joint and is most likely a major driving factor in the establishment of articular cartilage architecture. Thus, the assumption that the common contact area covered by the femoral condyle and the meniscus can be lumped into one representation is not expected to influence the results qualitatively. Meniscus and tibia have been combined into one representation in other knee models, 52 and loading via rigid rather than deformable contact models has been shown to lead to a more challenging mechanical environment being predicted in the tissue. 53 The meniscus has further been shown to have a sealing function that maintains fluid load support in the tissue, 54 justifying the fluid boundary condition used in the present model. However, the interaction of deformable contact bodies becomes important for large defects where rim stresses will be elevated significantly, 55 which is why the current study was restricted to comparatively small defects. Larger defects and the investigation of the influence of defect location would also necessitate a three-dimensional knee model with a more accurate geometry.55,56 Model improvements in contact mechanics and simulations of larger defects will likely predominantly affect the predicted architecture around the defect rim. It is further expected that the importance of construct maturity and strength increases in larger defects where the joint load is distributed onto a smaller undamaged rest area. Ideal integration between the repair tissue and the native cartilage was further assumed. Integration becomes increasingly important when a mismatch in properties between the implant and the surrounding tissue occurs, and shear stresses develop as a consequence 29 as well as when loading against a deformable contact body. Since loading was simulated with a rigid contact body in this study, the influence of a potential lack of integration are expected to be confined to a boundary layer. Promising results toward the integration of cartilage replacements have been achieved12,57 and can be aided by, for example, removing proteoglycans from the defect surface. 11 Failure to achieve integration potentially disturbs the continuity of the displacement fields and may negatively influence tissue mechanics and remodeling.
In this study, the significance of remodeling was quantified in terms of the altered peak stiffness direction (i.e., alterations in the direction of the major axis of the ellipse illustrated in Fig. 1) of the collagen network with respect to the healthy reference case. As cartilage is in reality (and in our model representation) a material with a dispersed fiber network in any one point, this approach is but one simplified representation or measure of the remodeling that occurs postimplantation. An implication of this metric is that it can return high values for the change in principal fiber direction in regions of the tissue that are initially reasonably isotropic (very isotropic regions of the tissue are neglected from the analysis to minimize the impact of this). A more accurate measure of the amount of remodeling involved in the transition from one architecture to the other might be the earth mover's or Wasserstein distance (e.g., Creane et al. 58 ), which considers the shift of the entire fiber distribution rather than simply its principal direction. Such an alternative evaluation methodology may slightly alter the predicted severity with which a certain cartilage region is affected by the presence of a defect.
In conclusion, implantation of a mature engineered tissue with near-native properties was found to induce the most favorable stimuli for remodeling toward a Benninghoff-like architecture in regenerating articular cartilage. The presence of active remodeling and native compositional gradients is predicted to result in the development of a native architecture. If active remodeling cannot occur in vivo, it is suggested that the architecture should be formed before implantation. Independent of the extent to which internal remodeling occurs in native cartilage, remodeling simulations can be an important tool when evaluating varying implantation conditions in terms of the mechanical environment in the regenerate itself as well as the extent to which an adverse mechanical environment extends into the undamaged tissue.
Footnotes
Acknowledgments
We acknowledge funding by IRCSET (G30345) and a Science Foundation Ireland PIYRA award (08/YI5/B1336).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.