
Abstract
The weak intrinsic meniscus healing response and technical challenges associated with meniscus repair contribute to a high rate of repair failures and meniscectomies. Given this limited healing response, the development of biologically active adjuncts to meniscal repair may hold the key to improving meniscal repair success rates. This study demonstrates the development of a bone marrow (BM) adhesive that binds, stabilizes, and stimulates fusion at the interface of meniscus tissues. Hydrogels containing several chondroitin sulfate (CS) adhesive levels (30, 50, and 70 mg/mL) and BM levels (30%, 50%, and 70%) were formed to investigate the effects of these components on hydrogel mechanics, bovine meniscal fibrochondrocyte viability, proliferation, matrix production, and migration ability in vitro. The BM content positively and significantly affected fibrochondrocyte viability, proliferation, and migration, while the CS content positively and significantly affected adhesive strength (ranged from 60±17 kPa to 335±88 kPa) and matrix production. Selected material formulations were translated to a subcutaneous model of meniscal fusion using adhered bovine meniscus explants implanted in athymic rats and evaluated over a 3-month time course. Fusion of adhered meniscus occurred in only the material containing the highest BM content. The technology can serve to mechanically stabilize the tissue repair interface and stimulate tissue regeneration across the injury site.
Introduction
Application of autologous intraoperative biologics (IOB) such as bone marrow (BM) aspirates or platelet-rich plasma may be an effective way to enhance the slow and inconsistent physiologic intrinsic meniscal healing response. BM has long been used to repair the musculoskeletal tissue due to its ability to facilitate fibrocartilage tissue repair, 13 and exogenous fibrin clots have been shown to enhance meniscal healing. 14 These biologics are rich in progenitor cells and platelet-derived growth factors 15 that have been shown to stimulate meniscal healing. 16 In particular, some of the known platelet-derived growth factors stimulate mesenchymal stem cell (MSC) migration,17,18 proliferation,19,20 and chondrogenic differentiation, 21 as well as fibrochondrocyte migration,22,23 proliferation,23,24 and tissue production.25,26 IOB also contain fibrinogen, fibronectin, 27 and vitronectin, 28 which can facilitate adhesion and migration 29 of MSCs and fibrochondrocytes. Together, these attributes make IOB a promising option to improve success rates of meniscal repair.
Adhesives play a vital role in immobilizing tissues in many clinical applications, 30 but none have been developed with suitable attributes to be applied to meniscal repair. In general, synthetic adhesives such as cyanoacrylates, which are very strong, are not biodegradable and do not support tissue growth or repair. 31 On the other hand, biological adhesives such as fibrin glue are highly biocompatible, but degrade quickly and are very weak. 32 To be effective, a meniscal adhesive must balance adequate binding strength and biomaterial implant residence time with the ability to support tissue repair to facilitate tissue fusion. We have developed an innovative, chemically modified chondroitin sulfate (CS) tissue adhesive suitable for use in orthopedic applications.33,34 CS is an appealing material due to its ability to promote new cartilage development by musculoskeletal progenitor cells. 35 Previously, we combined the adhesive technology with IOB to form hydrogels capable of binding soft tissues with mechanical strength exceeding that of fibrin glue and of supporting cell viability and tissue production over an extended duration. 36 Here, we combined the adhesive with BM aspirate and identified a biomaterial adhesive formulation to enable bonding and subsequent fusion of meniscus fibrocartilage with the potential to reduce meniscectomy rates.
Materials and Methods
Synthesis of chondroitin sulfate succinimidyl succinate
Chondroitin sulfate succinimidyl succinate (CS-NHS) was synthesized as reported previously. 34 Briefly, a phosphate-buffered saline (PBS) solution containing 7% (w/v) CS (25 KDA, New Zealand Pharmaceuticals Ltd., Palmerston North, New Zealand), 10% (w/v) 1-ethyl-3-(3-dimethylaminopropyl)carbodiimide (EDC), and 3.8% (w/v) n-hydroxysuccinimide (NHS) was reacted at 37°C for 10 min. The resulting CS-NHS was frozen, precipitated, and washed with −20°C ethanol and dried under argon. The product was placed under high vacuum overnight, and then stored at −20°C in argon. For use in all experiments, CS-NHS was dissolved in PBS to an application-specific concentration.
Preparation of CS-BM hydrogels
Dissolved CS-NHS and a freeze–thawed BM aspirate (Thomas D. Morris, Inc., Reisterstown, MD) were mixed at room temperature and reacted to form hydrogels. Gels containing 30, 50, or 70 mg/mL of CS-NHS and 30%, 50%, or 70% volume fractions of BM were formed. Hydrogel formulation is noted as follows: CXBY, where X is the CS-NHS loading concentration (mg/mL) and Y is the BM loading volume fraction (%).
Meniscal fibrochondrocyte encapsulation and culture
Meniscal fibrochondrocyte (MFC) cells were isolated from entire medial and lateral juvenile bovine menisci (Research 87, Inc., Boylston, MA) using a previously described collagenase digest. 37 The MFCs were suspended in bovine marrow before mixing with the CS-NHS solution resulting in 100 μL hydrogels containing 2×107 cells/mL. Material formulations investigated were C30B70, C50B50, and C70B30. Constructs were cultured in a previously described meniscus medium 38 consisting of 50:50 DMEM:F12 with 10% fetal bovine serum, 100 units/mL penicillin, 100 μg/mL streptomycin, 0.1 mM nonessential amino acids, and 25 μg/mL ascorbic acid. After 10 min, the hydrogels were transferred into the meniscus medium. The cell culture medium was changed 3 times per week. Constructs were harvested at 1 and 3 weeks for viability, biochemical, and immunohistochemical analysis. CS-poly(ethylene glycol) (PEG) was used as a control. The CS-PEG hydrogels were formed at 10% w/v with final concentrations of 50 mg/mL CS-NHS and 50 mg/mL PEG-amine (15 kDa; Sunbio, Orinda, CA). Three samples were used per material per time point for biochemical analysis.
Analysis of MFC viability
Cells were stained according to the manufacturer instructions using a LIVE/DEAD® Viability/Cytotoxicity Kit for mammalian cells (Invitrogen, Carlsbad, CA). A thin slice of hydrogel was incubated for 30 min in a medium containing 1 μm calcein-AM and 4 μm ethidium homodimer-1 at 37°C and 5% CO2. The hydrogels were imaged using a fluorescent microscope equipped with a 485±10-nm optical filter for calcein AM and a 530±12.5-nm optical filter for ethidium homodimer-1. The images were merged and percent of cell viability was quantified using ImageJ (National Institute of Health, Bethesda, MD).
Mechanical testing
The effect of CS-NHS and BM content on adhesive strength and Young's modulus was evaluated using shear testing on adhered bovine meniscus and compressive testing on CS-BM gels. A full factorial design was used to test formulations containing 30, 50, and 70 mg/mL CS, and 30%, 50%, and 70% BM. Full thickness cores from the peripheral region were obtained using a 6-mm biopsy punch, and then frozen and sectioned into 200-μm-thick sections on a cryostat. Meniscus sections were blotted dry, and 10 μL of CS-BM adhesive was applied between two sections—the top section was moved around in a circular motion to ensure the entire interface was glued, and to remove excess adhesive. Adhesive was allowed to set, and then rehydrated in PBS before testing. Samples were mounted to metal fixtures using cyanoacrylate adhesive (See Fig. 2A), and loaded at a speed of 3 mm/min in a Bose Enduratec ELF 3200 mechanical tester. Adhesive strength was calculated as the ratio of maximum load to contact area (n=10). For compressive testing, 100 μL cylindrical hydrogels were placed between plates and strained from 0% to 10% strain in 1% increments. Hydrogels were allowed to equilibrate for 20 s after each displacement, as indicated by load relaxation reaching a plateau. The Young's modulus was determined to be the slope of equilibrium stresses versus strain.
Biochemical assays
Constructs were massed, frozen, and lyophilized for 48 h before dry weights were recorded. Samples were homogenized, and then solubilized in a papain solution for 16 h at 60°C. The Hoechst 33258 dye (Sigma-Aldrich, St. Louis, MO) was used to determine the DNA content. The collagen content was determined using hydroxyproline assay as previously described. 39 Samples were hydrolyzed in 6N hydrochloric acid at 115°C for 16 h. Samples were titrated to neutral pH and reacted with p-dimethylamino benzaldehyde and chloramine-T hydrate. Absorbance was measured at 562 nm with a trans-4-hydroxy-L-proline (Sigma-Aldrich) standard.
In vitro MFC migration
Juvenile bovine meniscus was isolated aseptically and cut cross sectionally into 2-mm-thick tissue explants (See Fig. 4A). Tissue along the perimeter was excised to remove any nonmeniscus tissue and cells. A 4-mm full-thickness, circular volume defect was created and filled with CS adhesive (C30B70, C50B50, C70B30, or 10% CS-PEG) or left empty. Tissue adhesive composites were cultured in the meniscus medium, and then analyzed at 2 or 4 weeks using hematoxylin and eosin (H&E) staining and type-I immunohistochemistry to assess cell migration and matrix production.
Subcutaneous meniscus fusion model
Juvenile bovine meniscus was isolated aseptically, and full-thickness cores from the peripheral region were obtained using an 8-mm biopsy punch. The cores were cut into discs ∼1 mm in thickness. Meniscus discs were adhered with 20 μL of C30B70, C50B50, or C70B30, and then implanted subcutaneously in athymic rats. Animals were anesthetized and maintained with isoflurane. The standard sterile technique was utilized. A 1.5-cm incision was made dorsally, followed by loosening of the subcutaneous fascia to provide a pocket for implantation. The meniscal composites were placed into the pocket, and the skin was sutured closed. There were six implants per animal, two of each material formulation. Animals were euthanized and samples harvested at 4, 8, and 12 weeks postoperatively. At 4 weeks, two samples were analyzed for each material, while four samples were analyzed for each material at 8 and 12 weeks. Successful fusion was defined as meniscus disks fused with type-I collagen, as analyzed using H&E and type-I collagen immunohistochemistry. All procedures were performed with prior approval from the Institute Animal Care and Use Committee.
Histology and immunohistochemistry
Hydrogels were fixed in 10% formalin, dehydrated using a series of ethanol solutions, cleared with xylene, paraffin embedded, and sectioned. Immunohistochemical staining was performed with a sequence of treatments. The sections were exposed to rabbit polyclonal antibodies against type-I collagen, biotinylated anti-rabbit secondary antibodies (Invitrogen, Camarillo, CA), and then the streptavidin–peroxidase enzyme link. Samples were then exposed to AEC chromagen for 10 min to develop the slides. Hematoxylin was applied for visualization of cell nuclei.
Statistical analysis
Values are presented as mean and standard deviation. Statistical analysis was performed using two-way analysis of variance with SPSS software (version 20; SPSS, Chicago, IL). For experiments involving mechanical analysis, we investigated the effects of changing both the CS and BM content. For biochemical experiments, we investigated the effects of time and material formulation. Post hoc Tukey tests with an adopted significance level of p=0.05 were applied to determine the statistical significance.
Results
Hydrogel gelation and hMSC viability
BM aspirate and CS-NHS combined to form fully biologic hydrogels. Primary amines on the surface of soluble and nonsoluble proteins in BM reacted with activated carboxylic acid groups on CS to form a hydrogel mesh crosslinked by amide bonds (Fig. 1A). Compared with CS-PEG control in which no MFCs survived, CS-BM greatly improved the viability of encapsulated MFCs (Fig. 1B). Cell viability was maintained up to 3 weeks postencapsulation, although at this late time point, most viable cells were arranged in dense clumps.
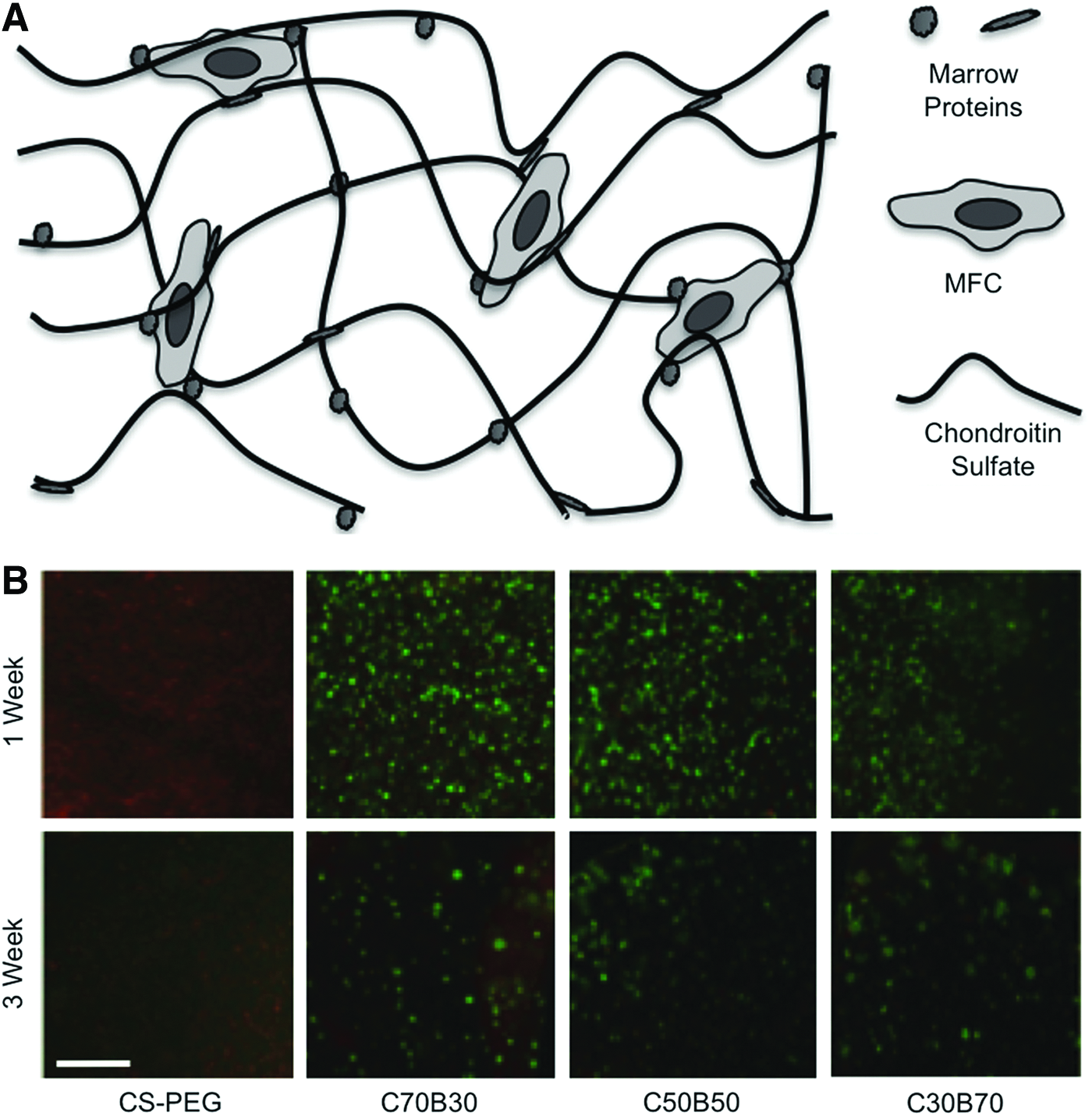
CS-bone marrow hydrogels and MFC viability.
Evaluation of hydrogel mechanics
The CS and BM content affected the tensile and compressive mechanics of the adhesive. Surface amines on the meniscus fibrocartilage reacted with the adhesive polymer, binding the tissues together (Fig. 2A). The bond strength of CS-BM to meniscus depended on the CS and BM content (Fig. 2B). With increasing CS content, adhesive strength increased steadily, whereas increasing the BM content decreased the adhesive strength, with the most dramatic decrease occurring between 50% and 70% BM levels. The adhesive strength ranged from 60±17 kPa (C30B70) to 335±88 kPa (C70B30). Compressive testing indicated that the CS and BM content also affect the elastic moduli of the bulk hydrogel. Compressive moduli varied from 3.9±0.9 kPa (C30B30) to 21.1±4.1 kPa (C50B50) (Fig. 2C).
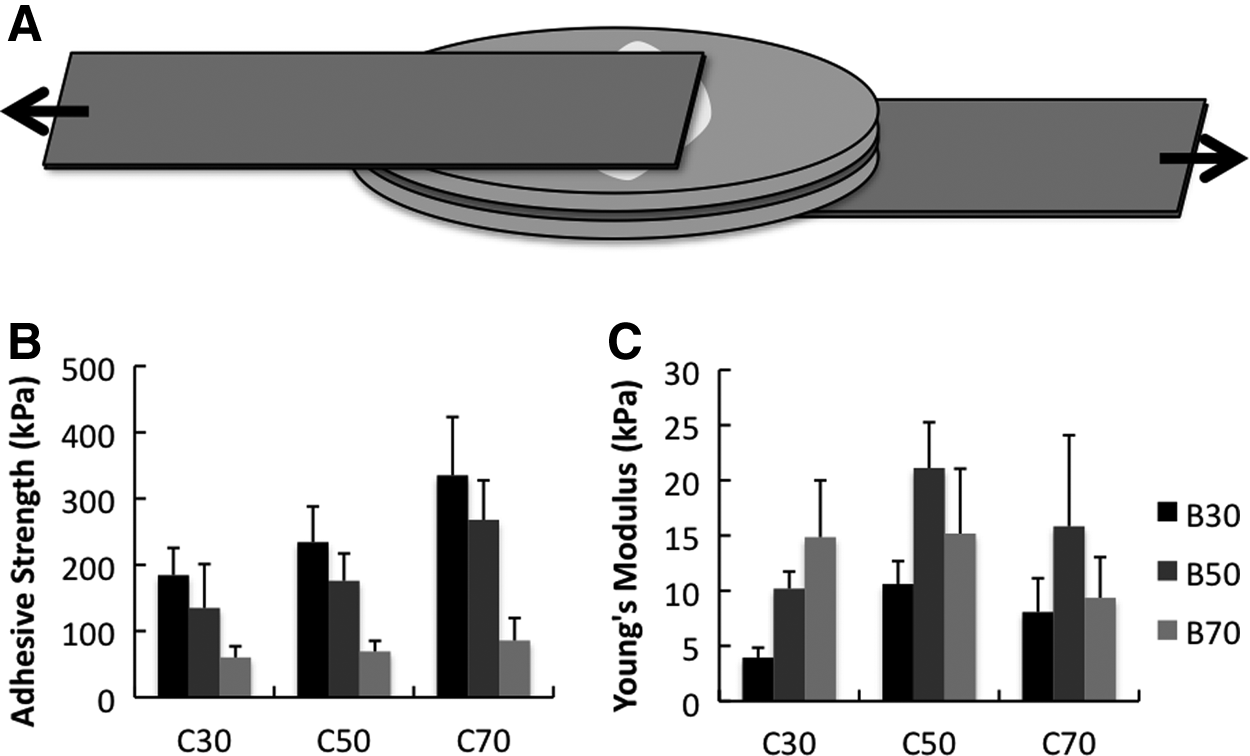
Mechanical analysis of CS-BM adhesive hydrogels.
Characterization MFC encapsulated hydrogels
MFCs remained viable in CS-BM and material formulation impacted cell proliferation and matrix production. The DNA content fell to nearly zero for the CS-PEG control between 1 and 3 weeks, whereas the DNA content increased in C70B30 and C50B50 (Fig. 3A). The DNA content also increased with increasing BM and decreasing CS. The total collagen content, normalized both to dry weight and to cell number, increased significantly between weeks 1 and 3 (Fig. 3B, C). Additionally, in contrast with the DNA content, the total collagen content increased with the increasing CS and decreasing BM content. There were no detectable accumulations of collagen at either time point from MFCs encapsulated in CS-PEG hydrogels (data not included in figure). Immunohistochemical staining for type-I collagen, the primary matrix protein in meniscus fibrocartilage, confirmed the production of the primary meniscus ECM protein by MFCs encapsulated in CS-BM hydrogels over the 3-week time course (Fig. 3D).

Biochemical assays and immunohistochemistry of encapsulated meniscal fibrochondrocytes in CSBM hydrogels.
In vitro MFC migration
MFC migration occurred in a material-dependent manner. No cells migrated from the tissue into or along the surface of CS-PEG controls and empty defects remained unfilled (not shown). By 4 weeks in culture, migration occurred in all CS-BM materials to varying degrees. Increasing the BM content increased the total number of migrating cells. In C70B30, cells migrated only across the surface of the hydrogel, and a few cells migrated into the C50B50 hydrogel. In contrast, cells migrated throughout the entire bulk of the C30B70 hydrogel materials (Fig. 4B–D). Type-I collagen immunohistochemistry confirmed that migrated MFCs maintained the ability to produce the primary matrix protein of their tissue of origin (Fig. 4E–G).

In Vitro migration of meniscal fibrochondrocytes.
Subcutaneous meniscus adhesion model
The in vivo performance of the meniscus adhesive depended on material formulation. At the 4-week time point, the menisci remained adhered together by all CS-BM formulations, and cells infiltrated the material (Fig. 5A–C). Cell migration increased with the BM content, with extremely high density in C30B70 samples. At week 8, neo-tissue bound the C30B70 samples, whereas the meniscus implants bound by other formulations failed to fuse, although some adhesive remained (not pictured). By the twelfth week, no adhesive remained and the menisci fused in only the C30B70 group (Fig. 5D–F). Cells lined the interface, where the meniscus tissue fused (Fig. 5G). Type-I collagen immunohistochemistry confirmed that migrated cells produced this matrix protein (Fig. 6A–C), and that the two meniscus pieces were fused together at a nearly indistinguishable interface by type-I collagen (Fig. 6D).
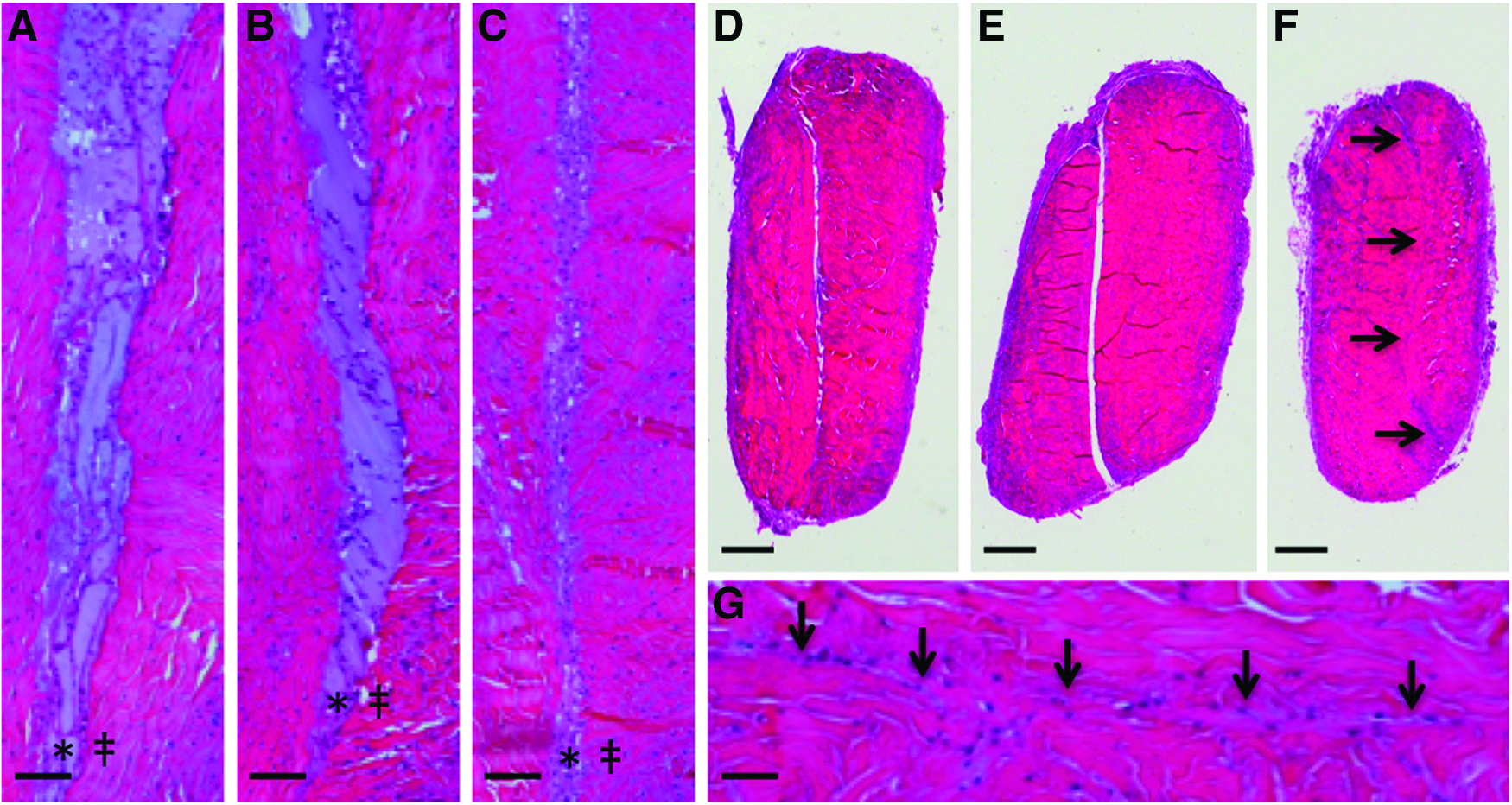
Hematoxylin and Eosin staining for subcutaneously implanted CS-BM meniscus explants. Four-week time point of subcutaneously implanted composites indicate extensive cell migration into

Immunohistochemistry for subcutaneously implanted CS-BM meniscus explants. Type-1 collagen immunohistochemistry of subcutaneously implanted composites at 4-week time point indicates new matrix formation in
Discussion
Repairing and preserving an injured meniscus is important to maintain overall homeostasis of the knee and integrity of the articular cartilage. The removal of all or a portion of the meniscus leads to joint destabilization and increased stresses in the joint environment, which can lead to the early onset of progressive joint degeneration and osteoarthritis. Surgeons will work to repair and reconstitute the meniscus whenever possible, but technically difficult repair techniques combined with the limited vascularization and marginal ability of the tissue to heal lead to meniscectomy being the most common procedure performed by orthopedic surgeons. 40 Although some damaged menisci are irreparable due to tissue degeneration and degradation, many clean tears must be removed due to either a failed repair attempt or their location in the avascular zone. Therefore, the primary aim of developing this adhesive technology is to reduce the meniscectomy rate of clean tears in two ways. First, applying this adhesive as a complement to suture repairs in the vascularized red zones of the meniscus could provide a more complete stabilization of the tissue interface and potentially reduce gap formation. Additionally, the adhesive would serve as a scaffold to fill gaps between the approximated tissue surfaces, thereby promoting tissue fusion across the entire length of the defect. Second, the delivery of a growth factor-rich IOB scaffold might extend the range of repairable meniscal tears into the avascular inner zone, where meniscectomy is currently the predominant surgical technique of choice. Extending the range of repairable injuries would reduce future costs associated with joint degeneration and osteoarthritis. The results of this work have demonstrated key attributes of the CS-BM adhesive that suggest it can be effective at stimulating meniscal healing: ability of MFCs to migrate into the material, survive, and produce the ECM, meniscus binding ability with robust mechanical properties, and extensive in vivo material residence time.
Through our investigation of hydrogel mechanics, we learned that the CS-BM has adhesive strength on the order of that necessary to withstand forces in a suture-repaired human meniscus. Studies investigating forces on sutures repairing lateral and medial meniscal tears in human cadaver models indicated that the mean distraction forces on sutures did not exceed 5 newtons in either meniscus41,42 when loaded with 300N (67 lbs) of force, which would correlate to a stress of 50 kPa for a meniscal tear measuring 1 cm2.43,44 In nonweight bearing recovery, the tensile forces on the repair would be far lower, well below the failure strength of C30B70 (60 kPa). The adhesive may, therefore, stabilize the tissue interface without failing and prevent gap formation. By doing so, the material may promote tissue fusion across the entire injury interface, preventing postsurgical tears that may occur as a result of contact healing. Although decreasing CS and increasing BM contents weaken the material adhesiveness, we prefer the biological attributes of migration, proliferation, and tissue fusion associated with the C30B70 formulation.
The biological properties of this adhesive can be manipulated to provide flexibility in optimization for specific clinical and tissue applications.33,34 For the meniscus application, we require a material that binds to meniscus and supports MFC viability and migration, and prefer a material that promotes cell proliferation and ECM production. MFCs were able to survive, proliferate, and produce meniscus ECM when encapsulated in various CS-BM formulations, whereas they were not viable when encapsulated in CS-PEG (Fig. 1B). This finding suggests that MFCs are adhesion dependent for survival and cell processes. The fibrinogen, fibronectin, and vitronectin bound in the BM hydrogel network contain cell adhesion ligands on which the MFCs can bind and spread (Fig. 1A). Additionally, the presence of growth factors present in the BM may improve MFC viability. By modulating the CS and BM content, we were able to affect MFC behavior in the material. Changing the CS and BM content had competing effects on MFC unit cell processes: cells were directed to proliferate and migrate in the presence of high BM, whereas they were stimulated to produce the ECM in the presence of high CS content. In the subcutaneous model, results of high cell density at 4 weeks followed by fusion at 12 weeks were observed for only the C30B70 material (Fig. 6C, F, G). While the ECM is produced at a higher per-cell rate in the C70B30 material, these results suggest that successful fusion of meniscus may depend more on the ability of cells to migrate and proliferate within the material to a high density. Thereafter, while the cells will secrete tissue at a lower rate, the density of cells is high enough to replace the CS-BM adhesive with meniscus tissue.
A major limitation of in vitro studies is the difficulty of recapitulating biological cues and signals that occur in vivo. Therefore, in vivo application of the adhesive is critical for evaluating any tissue repair strategy. To evaluate bovine meniscal healing, we translated the CS-BM adhesive to a subcutaneous implantation model, one with which our laboratory has extensive experience45–48 and which has been used similarly in meniscal repair studies.49–51 While not in the joint space, this small animal model allows us to simply and economically simulate more closely a natural environment for meniscus fusion so that we may more accurately evaluate biomaterial function and meniscus repair over time. This subcutaneous meniscus repair model allows us to evaluate the repair potential of meniscus tissue without a blood supply, which is relevant for comparisons to the white zone of meniscus. The key finding from the subcutaneous meniscus repair model is that only the material containing 70% volume fraction of BM was capable of fusing the glued meniscus pieces. This result suggests that the high concentration of BM delivers critical factors (growth factors and cell-adhesion ligands) that are typically not available due to poor tissue vascularization and subsequent lack of clot formation. Evidence to support this conclusion was also obtained from in vitro MFC migration results, in which substantial cell infiltration and matrix production occurred only in the C30B70 material. While it may be preferable to stabilize the defect using an adhesive with the greatest mechanical strength (C70B30), we ultimately desire tissue repair across a defect and fusion of tissue to preserve a healthy joint environment.
When designing a technology for meniscus repair, consideration of technology cost and clinical ease of use is equally important as a successful biological repair. Meniscal repairs are outpatient procedures that are relatively short and require only the material cost of degradable sutures. To be accepted as a new meniscus repair technology by clinicians and patients, a new product has to be affordable, applied in a single surgery, simple to use, and not significantly extend the duration or change the approach of surgery. Ultimately, it must also be successful in improving clinical outcomes such as the successful repair rate or reduction in rehabilitation time and cost. We have developed a single component biological adhesive, CS-NHS, which can be used in conjunction with autologous IOBs to enhance meniscal repair. With no dependence on exogenous cells or autologous cell expansion, this is an affordable technology and maintains the procedure as a single surgery. Additionally, the technology is an in situ setting, injectable polymer with polymerization on the order of minutes, allowing for the use of standard arthroscopic surgical procedures and not extensively prolonging surgical times. The combination of low cost with practicality of delivery and potential for improved clinical results makes this material promising as a new technology to enhance meniscal repair.
In sum, we have developed the first acellular bioadhesive to fuse the meniscus tissue, and the first approach involving BM.52,53 The CS-BM material leverages the stimulatory attributes of CS combined with autologous growth factors and progenitor cells to enhance the intrinsically weak healing response of meniscus repair. We have demonstrated the ability of the material to sustain meniscal cell viability and support cell migration. In a subcutaneous model to assess meniscus fusion, meniscus explants adhered by C30B70 fused together 12 weeks postimplantation. The next step for evaluating the potential of this meniscus repair technology will be to combine it with the current gold standard, vertical mattress sutures, applied in a physiologically and clinically relevant large animal model to assess the healing potential.
Footnotes
Disclosure Statement
No competing financial interests exist.