
Abstract
In a general view of anatomy, intervertebral disc is composed of three parts: annulus fibrosus (AF), nucleus pulposus (NP), and cartilage endplate (CEP). Recently, several types of stem cells were successfully isolated from these corresponding regions, but up to now, no research was performed about which kind of stem cells is the most efficient candidate for NP tissue engineering or for stem cell-based disc regeneration therapy. In this study, we compared the regenerative potentials of the above-mentioned three kinds of disc-derived stem cells with that of the classic bone marrow (BM)-mesenchymal stem cells (MSCs) in a rabbit disc degeneration model. By magnetic resonance imaging (MRI), X-ray, histology, etc. evaluations, we found that cartilage endplate-derived stem cells (CESCs) showed superior capacity compared with the annulus fibrosus-derived stem cells (AFSCs), nucleus pulposus-derived stem cells (NPSCs), and BM-MSCs (p<0.05); additionally, when comparing the CESC group with the normal control group, there existed no statistical difference in X-ray (p>0.05). Those results demonstrated that the CESC-seeded alginate construct performed the most powerful ability for NP regeneration, while AFSCs showed the most inferior potency, NPSCs and BM-MSCs had similar regenerative capacity and located in the middle. All in all, our study showed that CESCs might act as an efficient seed cell source for NP tissue engineering, which paved a new way for the biological solution of disc degeneration diseases.
Introduction
L
The intervertebral disc (IVD) is an avascular structure that is macroscopically composed of three anatomically specific tissue components: annulus fibrosus (AF), nucleus pulposus (NP), and cartilage endplate (CEP). 4 The AF consists of several annular layers of elastic fiber and fibrocartilage; the former is mainly composed of type II collagen, and the latter is mainly composed of type I collagen. 5 The layers surround the longitudinal axis of IVD at parallel state to enclose NP, a gelatinous matrix mainly comprising a random network of collagen fibril in the center of the IVD. 6 NP is rich in proteoglycan and extracellular matrix (ECM) that embrace an abundance of collagen II, which presents affinity for water to inflate the IVD against pressure from overload and plays an important load-bearing role. 7 The CEP are two thin layers of hyaline cartilages on both the superior and inferior surfaces of IVD forming a unique structure that sandwiched the AF and NP. 8
Current treatment modalities for DDD include conservative management and surgical therapy that mainly focus on symptom relief through medication or surgical removal of the degenerated disc tissue without preventing the disc from further degeneration. 9 The above two treatment methods do not aim to address the basic cause or reconstruct the biological properties of the spine, and serious side effects arise from time to time especially for the surgery therapy. Moreover, a long-term effect is not uncertain. 10 During disc degeneration, as the disc cell number decreases significantly, and the ECM, especially the proteoglycan and collagen content, drops greatly, cell implantation might be an effective approach by increasing ECM anabolism. 11 In consideration of resolving the biological changes of the degenerated IVD fundamentally, recently more biological treatments for DDD, including gene therapy, cell implantation, and tissue engineering have obtained rapid progress, among which especially, stem cell-based therapy has gained the extensive interests of researchers in this area. 12 There were already some researches showing that it might be one of the most promising treatment options.13,14
Since bone marrow (BM)-mesenchymal stem cells (MSCs) were first isolated successfully in 1999, it is believed to be a promising one in regeneration medicine as it is easy to collect and expand. 15 Recently, several types of stem cells or progenitor cells have also been isolated and identified from different anatomical regions of IVD. Risbud et al. 16 found that the degenerate NP contained populations of skeletal progenitor cells, and believed that the progenitors might be used to repair IVD. In addition, Blanco et al. 17 also isolated a type of MSC-like cells from degenerate lumbar NP and found that it fulfilled the criteria for MSCs described by the International Society for Cell Therapy (ISCT), except without the ability to differentiate into adipocytes. Feng et al. 18 successfully isolated a type of MSCs from the AF of humans that could differentiate into adipocytes, osteoblasts, chondrocytes, neurons, and endothelial cells in vitro. In our previous study, using the agarose suspension culture system, we have also isolated MSC-like stem cells with multilineage differentiation abilities from CEP of the degenerated human IVD and named it as cartilage endplate-derived stem cells (CESCs). When compared with BM-MSCs, CESCs indicated similar morphology, proliferation rate, cell cycle, immunophenotype, and stem cell gene expression. In addition, CESCs showed a significantly superior potency of chondrogenesis and osteogenesis compared with BM-MSCs.19,20
Owing to specific advantages, such as extreme low immunogenicity, powerful ability of propagation, self-renewal, and multilineage differentiation, stem cells might be suitable for DDD treatment with less side effects, 21 and several researchers have begun to try stem cell-based treatment modalities for DDD. 22 However, until now, there is still no study to compare the biological characteristics of the three types of stem cells derived from IVD (AFSCs, NPSCs, and CESCs) and BM-MSCs; which kind of stem cells has superior in vivo regenerative capability for NP tissue engineering is unknown. With these in mind, the differences among the four types of stem cells in NP regeneration and IVD restoration in vivo were investigated in our study. Using the previously reported methods, the above three types of stem cells and BM-MSCs were obtained from the same patients who had undergone posterior discectomy and fusion surgeries for lumbar degenerative disease. After culturing and expanding in vitro, cells labeled with CFDA-SE fluorescent were seeded in alginate gel and injected into the NP lacuna of rabbit IVD degenerative models made by NP aspiration. The Bradner disc index (BDI) of lateral X-radiographs and the T2-weighted signal intensity index of magnetic resonance imaging (MRI) were measured to appraise the degeneration degree of the objective IVD at 1, 3, and 6 months after operation. At the sixth month, animals were sacrificed, the operated discs were explanted for gross morphology observation, histological staining, and cell viability assessment.
Materials and Methods
Ethics statement
Approval and informed consent for sample collection were obtained from the Institutional Review Board and the patients before surgeries. All animal experiments were approved by the Xinqiao Hospital Committee on Ethics for the care and use of laboratory animals.
Case selection
The tissue samples, including AF, NP, CEP, and BM were obtained from eight patients who received posterior discectomy and fusion surgeries for the lumbar degenerative disease. The average age was 46.6 years (range: 37–61 years). Details of all samples are shown in Table 1.
BP, back pain; RP, radicular pain.
Isolation and culture of human BM-MSCs
Isolation and purification of BM-MSCs were based on the system as previously described. 23 During the surgery, 8 mL of BM was aspirated into a syringe that contained 10,000 IU of heparin from the iliac crest. Mononuclear cells were isolated by centrifugation in 1.073 g/mL of Percoll solution (Sigma-Aldrich) at 900 g for 25 min. The obtained cells were rinsed twice with phosphate-buffered saline (PBS) and resuspended with the Dulbecco's modified Eagle's medium/F12 (DMEM/F12; Hyclone) supplemented with 10% fetal calf serum (FCS; Hyclone) and 100 U/mL of penicillin–streptomycin (Hyclone). The nucleated cells were aspirated away and cultured in a 25-cm2 cell culture flask (Costar Corning) under the condition in which humidified atmosphere contained 5% CO2 at 37°C. After 72 h, the nonadherent cells were removed by replacing the medium, and the remaining cells were washed twice with PBS for culturing, with the medium changing every 3 days. When reaching 90% confluence, the cells were passaged by 0.25% trypsin and 1 mM EDTA (Trypsin/EDTA; Hyclone) until passage 3 cells were obtained.
Isolation and culture of AF-derived cells, NP-derived cells, and CEP-derived cells
The three kinds of corresponding disc tissues were, respectively, obtained by an experienced surgeon when discectomy and fusion procedures were performed.
Next, the extraneous materials were precisely excised from the objective tissue aseptically by an ophthalmic operating set using the anatomy microscope kit (4× magnification). Then, the tissue was mechanically fragmented into pieces no larger than 1 mm3 and digested with 0.15% collagenase II (Sigma-Aldrich) in the DMEM/F12 containing 2% FCS for 2 h in the shaking table at 120 rpm/min, 37°C. The mixture of digestion and cells was digested continuously for 4 h. At the end, the suspended cells were filtered through a 200-well filter, and the cell suspensions were centrifuged for 5 min at 1000 rpm/min and washed twice by PBS after the supernatant was aspirated away. The objective cell pellet was resuspended in the DMEM/F12 supplemented with 10% FCS and 100 U/mL of penicillin and streptomycin. Finally, the cells were cultured in a 25-cm2 cell culture flask at density of 3×105 cells/mL under 5% CO2, 37°C condition. When reaching 90% confluence, the cells were subcultured in agarose suspensions.
Agarose cultures to select AFSCs, NPSCs, and CESCs
The agarose suspension culture system is a mature method to screen stem cells since it was established in 2005. 24 Briefly, 1% and 2% low-melting point agarose (Invitrogen) was sterilized by autoclaving and equilibrated to 37°C in advance. Culture dishes (60 mm in diameter; Costar Corning) in advance were coated with 1% low-melting point agarose that was mixed with an equal volume of DMEM/F12 and 2% low-melting point agarose, the superfluous agarose was removed away. In this study, passage 2 cells were adopted for the stem cell colony screening. About 1.5 mL mixture of 0.75 mL DMEM/F12 and 0.75 mL of 2% low-melting point agarose were mixed with 1.5 mL of 20% FCS DMEM/F12 containing 1×105 passage 2 cells. The final mixture was incubated into the coated dishes at a circumstance of 5% CO2 at 37°C. Then, the culture medium was changed with DMEM/F12 supplemented with 10% FCS and 100 U/mL penicillin and streptomycin twice a week. Cell clusters formed after 6 weeks and were transferred into a 25-cm2 culture flask for subculturing by the Pasteur pipette. Passage 3 stem cells were adopted at last.
Cell surface antigen profile by flow cytometry
Selected cells were analyzed for the expression of cell surface antigen profile. After washing with PBS, those cells were incubated with fluorescein isothiocyanate (FITC), monoclonal antibodies: CD34-FITC, CD45-FITC, CD73-FITC, CD90-FITC, and CD105-FITC, which were purchased from eBioscience. Isotype controls were used in different cell type assays. After incubation for 20 min at 37°C, cells were washed twice with PBS and resuspended in 200 μL PBS with the total cell number no less than 104. The cells stained positively were counted as a percentage compared with the isotype staining.
Cell differentiation assays
The induction and differentiation procedures were used as described in the previous studies. 25
Briefly, for osteogenic differentiation, passage 3 cells from different types were seeded in 12-well plates at 1×105 cells/well, when reaching 80% confluence, then were incubated with the Osteogenesis Differentiation Kit (Gibco) containing 10% FCS, 10 nM β-glycerol phosphate, and 50 mg/mL ascorbic acid. The induction medium was refreshed every 3 days. Negative control cells were cultured with the DMEM/F12 supplemented with 10% FCS. After 3 weeks, the induction medium was removed; the plates were washed twice with PBS and then fixed in 70% methanol for 10 min before Alizarin red staining. For adipogenic differentiation, these cells were incubated for 24 h, then induced in the Adipogenesis Differentiation Kit (Gibco) for 21 days. Afterward, wells were fixed with 4% formaldehyde and stained by Oil Red O for 15 min; in the meantime, the cell nucleus was counterstained with hematoxylin. For chondrogenic differentiation, pellet culture was used. About 3×106 cells were transferred into a 15-mL polypropylene tube and centrifuged at 500 g for 5 min. The medium was changed with the Chondrogenesis Differentiation Kit (Gibco) after incubation for 24 h. Afterward, the induction medium was changed every 3–21 days, pellets were fixed with 4% paraformaldehyde for 20 min, and washed by PBS carefully, followed by gradual dehydration through ethanol. Finally, 5-μm-thick sections were cut. Observation and photography were performed using an Olympus microscope system.
Stem cell labeling and seeding in the alginate gel
The above four types of stem cells were labeled with CFDA-SE (Sigma-Aldrich) after expanding to passage 3. The labeling procedure was performed in accordance with the manufacturer's instructions. At confluence, those cells were trypsinized, counted, rinsed, and resuspended with the DMEM/F12 supplemented with 10% FCS and 100 U/mL penicillin and streptomycin. The cell suspension was mixed with an equivalent volume of 20 μM CFDA-SE to incubate for 30 min in an incubator with an atmosphere containing of 5% CO2 at 37°C. Then, these labeled stem cells were centrifuged at 800 rpm/min for 5 min and rinsed twice with PBS. After the supernatant was carefully sucked away, an appropriate volume of alginate (1.2% w/v) based on cell numbers was added in and blended well to form a final mixture with a cell concentration of 3×106/mL.
Surgery and implantation
Twenty-one New Zealand white rabbits, which contained both sexes randomly, each weighing 2.0–2.4 kg, aged 6 months, were used. The animals were divided into seven groups (three rabbits in each) randomly, three sequential IVDs of every rabbit (L4–L5, L5–L6, L6–L7) were operated, and in each group, only one of the following treatments was performed: (1) alginate gel containing AFSC injection group; (2) alginate gel containing NPSC injection group; (3) alginate gel containing BM-MSC injection group; (4) alginate gel containing CESC injection group; (5) only alginate gel containing no cell injection group; (6) nonimplantation control group, namely, the degenerate group, in which AF puncture and NP aspiration have been performed, but neither the stem cell nor alginate gel was injected; (7) normal control group in which animals received operation, but the discs were not manipulated. The degeneration animal model was adopted as previously described. 26 The rabbits were anesthetized with 30 mg/kg of sodium pentobarbital intravenous injection. Basing on iliac crest location, three serial IVDs (L4–L5, L5–L6, and L6–L7) were located, then these IVDs received annulus puncture at 5 mm depth by an 18G needle and NP aspiration through the retroperitoneal approach. When around 10 mg NP tissue (well weight) was basically aspirated out from each of the three IVDs, 60 μL of alginate gel containing stem cells was injected by a microinjector. Twenty seconds later, 20 μL of calcium chloride solution at a concentration of 35 g/L was injected for crosslinking with alginate in vivo, the injection port was sealed. Each group was implemented by the same procedure, only the cell type was different. Finally, the surgical incision was sutured layer by layer.
Radiographic and MRI analysis
Lateral plain radiographs (General Electric) and MRI were used to evaluate the IVD regeneration at 1, 3, and 6 months after surgery under general anesthesia with sodium pentobarbital (30 mg/kg). The measurements were all evaluated by two experienced radiologists, independently, in a blinded fashion.
The radiographic analysis was established using the protocol published by Bradner in 1972. 27 The height of the concerned disc and the upper adjacent vertebral body were measured by eFilm Workstation software (version 3.0; Merge Heathcare Co Ltd.), then the objective disc height was divided by the height of the upper adjacent vertebral body to obtain the BDI value, which was used to appraise the IVD degeneration.
MRI was taken using a 3.0-T imager manufactured by the GE Company and the protocol was performed as previously described. 28 The rabbits were checked in a supine position and the sagittal T2-weighted images of the lumbar spine were obtained. T2 values of the objective IVDs were quantized based on the 0.15-cm2 interesting oval region of the IVD center using eFilm Workstation software. The T2 signal intensity index was obtained through dividing the T2 signal intensity of the operated disc by that of the normal disc of the same rabbit. The T2 signal intensity index of the normal control group was calculated according to the same disc level of other groups.
General morphological observation and histological evaluation
Six months after surgery, all the animals were sacrificed using sodium pentobarbital overdose and the operated discs were explanted. The objective IVDs were cross cut into halves for the gross morphology observation at six postoperative months. Immediately, the harvested IVD sections were fixed in 10% neutral buffered formalin at 37°C for 24 h. Then, they were decalcified for 28 days in 0.5 M EDTA solution and embedded in paraffin. Subsequently, the paraffin blocks were sectioned at a thickness of 8 μm. Sections were stained with hematoxylin and eosin and Alcian blue for evaluation.
Viability detection of implanted stem cells
Viability of the implanted stem cells was measured qualitatively at six postoperative months based on the CFDA-SE fluorescent label. Serial frozen cross-sections, 6 μm thick, were harvested from the objective IVDs. Sections were observed by the confocal laser scanning microscope (Leica) with cell nuclei counterstained with DAPI (Sigma Chemical Co.).
Statistical analysis
The SPSS 13.0 version software was used for statistical analysis. Data are presented as mean±standard error. One-way analysis of variance (ANOVA) was applied among different groups at one specific time point, and repeated measures ANOVA was conducted to analyze the differences among these groups in general. The paired samples t-test was used to compare within groups at different time points. p-Values less than 0.05 were considered to be significant.
Results
Flow cytometric immunophenotype and multilineage differentiation
Flow cytometric analysis showed that the antigenic phenotype of the four cell types (AFSCs, NPSCs, CESCs, and BM-MSCs) had similar levels comparatively and were negative for CD34 and CD45 (<2%) (Fig. 1A). Additionally, these cell types (NPSCs, BM-MSCs) were highly positive for CD 105 (>95%), however, CD105 was modestly expressed (89.9%, 89.0%) in AFSCs and CESCs, respectively (Fig. 1A).
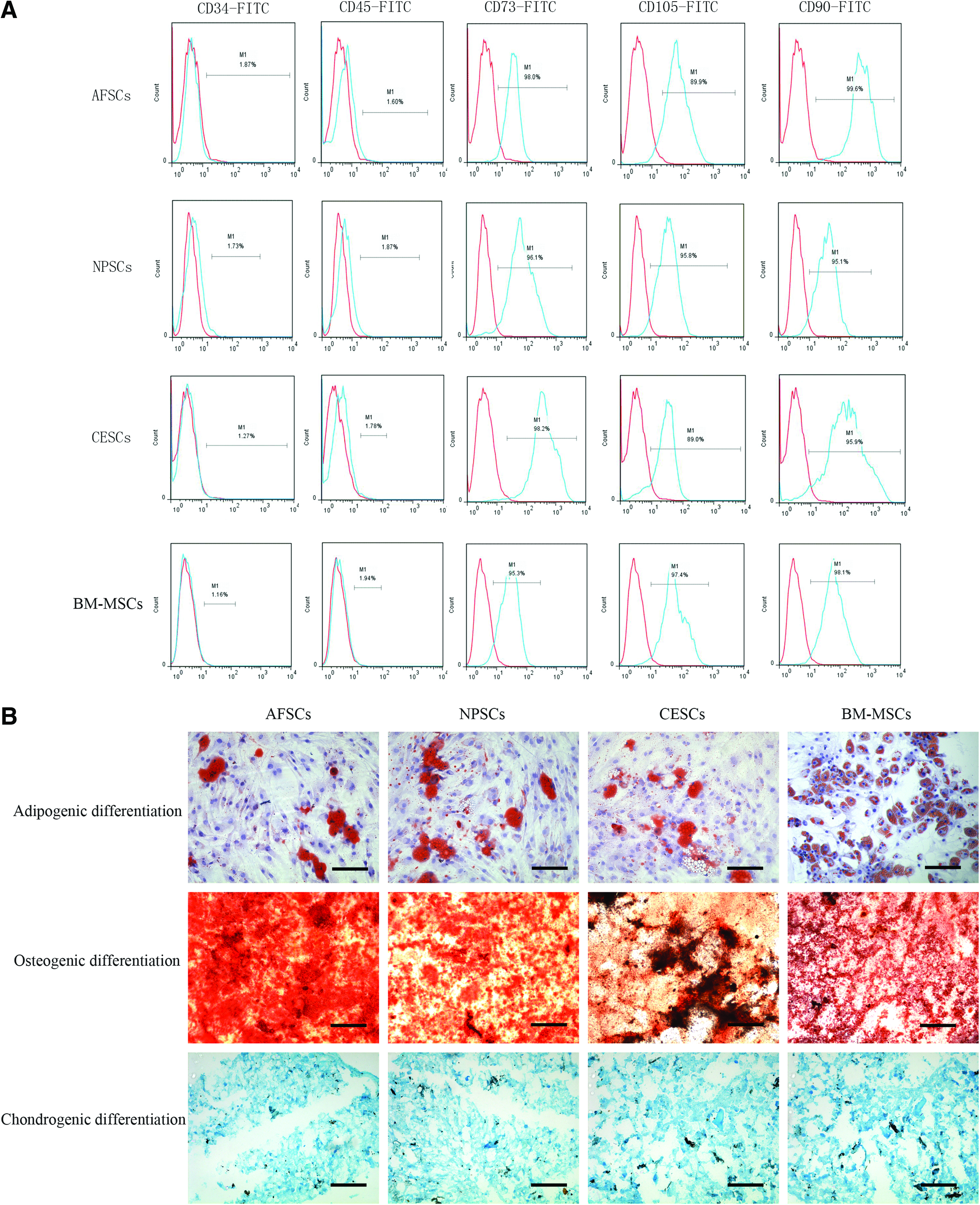
Immunophenotypic profile of annulus fibrosus-derived stem cells (AFSCs), nucleus pulposus-derived stem cells (NPSCs), cartilage endplate-derived stem cells (CESCs), and bone marrow (BM)-mesenchymal stem cells (MSCs), as analyzed by FACS
After induction, all the cell types (AFSCs, NPSCs, CESCs, and BM-MSCs) showed multilineage differentiation abilities (Fig. 1B). Additionally, the CESCs truly demonstrated a stronger osteogenic differentiation ability as coarsely shown in Figure 1B.
MRI evaluation
In the observing period, the T2 signal intensity index of the operated IVDs in all groups gradually decreased to some extent (Fig. 2).

MRI appraise of the rabbits at 6 months after surgery.
One month after surgery, the index of the CESC group (0.8475±0.0524) was the highest among all the groups except for the normal control group (1.0000±0.0320), followed by the BM-MSC group (0.6613±0.0373), the NPSC group (0.6573±0.0518), and the AFSC group (0.5488±0.0246). The index of the nonimplantation control group (0.4333±0.0230) was the lowest, followed by the only alginate gel implantation group (0.4779±0.0265). Significant differences could be observed between any two groups except for the indexes between the BM-MSC and the NPSC group (p<0.05).
Three months later after surgery, the index of CESCs decreased from 0.8475±0.0524 to 0.7754±0.0803, but was still the highest among all the groups except for the normal control group (1.0000±0.0421), followed by the BM-MSC group (0.5625±0.0391) and the NPSC group (0.5253±0.0362). The AFSC group (0.4070±0.0191) was still the lowest among the four types of stem cell containing groups. Whereas the indexes of the nonimplantation control group (0.2987±0.0230) and the only alginate gel implantation group (0.3160±0.0186) were still the lowest, in all the groups, significant differences could be observed (p<0.01) between any two groups except between the BM-MSC and NPSC group (p>0.05), and between the nonimplantation control group and only alginate gel group (p>0.05). Furthermore except for the normal control group, significant differences existed within all the groups when compared with its 1-month point counterpart, respectively (p<0.01).
At the 6-month time point, similar with the above two time points, the index of the CESC group (0.6348±0.0395) was still the highest except for the normal control group (1.0000±0.0396), the BM-MSC group (0.3837±0.0390), and the NPSC group (0.3833±0.0208) located in the middle, the AFSC group (0.3441±0.0267) still ranked at the bottom in the stem cell groups, and the indexes of the nonimplantation control group (0.1232±0.0090) and the only alginate gel implantation group (0.1254±0.0069) were still the lowest in all the groups. There still existed significant differences between any two groups (p<0.01) except for that between BM-MSC and NPSC group (p>0.05), and between the no-implantation control group and only alginate gel groups (p>0.05). Furthermore, except for the normal control group, significance could be observed within all the groups when compared with its 3-month point counterpart, respectively (p<0.01).
IVD space
In the observing period, the heights of almost all the groups decreased gradually except for the normal control group. At all the three time points, the BDI of the four stem cell containing groups were significantly higher compared with the other two groups containing no stem cells (Fig. 3).

X-ray appraise of the rabbits at 6 months after surgery.
One month after surgery, the BDI of the CESC group (0.2089±0.0078) was the highest among the four stem cell containing groups (Fig. 3), while significant differences just existed between the CESC group and the AFSC group (0.1867±0.0100) (p<0.01). At this point, when comparing the normal control group (0.2100±0.0087) with the AFSC group and NPSC group, respectively, significant differences could be observed (p<0.05), whereas there were no significant differences between the normal control group and the other two groups (BM-MSCs and CESCs).
Three months later after surgery, no significant differences existed among the four stem cell containing groups. By comparing the four stem cell containing groups to the normal control group (0.2100±0.0421), respectively, only the CESC group did not differ (0.1977±0.0530) significantly (p>0.05).
By the 6-month point, for the four stem cell containing groups and the normal control group, there were significant differences between any two groups. Furthermore, significant differences could be observed within every group except for the normal control group when comparing the 6-month point to the 1-month time point (p<0.05).
Gross morphology of IVDs
Gross morphology of the involved IVDs was observed at 6 months after surgery (Fig. 4A–G). In the AFSC group, a small quantity of regenerated NP tissue could be observed in the original aspirated NP lacuna, but the boundary between the regenerated tissue and the inherent AP was still obvious (Fig. 4A). Both the NPSC and BM-MSC group showed similar appearance. When compared with the AFSC group, more regenerated NP tissue located in the lacuna, and the boundary between the regenerated tissue and the AP was obscure (Fig. 4B, C). For the CESC group (Fig. 4D), in accordance with the results, the lacuna was almost totally filled with the hyaline cartilage-like tissue, but the general hydration extent was inferior than the normal control group (Fig. 4G). In the only alginate gel implantation group and the nonimplantation control group, nearly no residual gel or regenerated tissue could be seen in the lacuna. Clear boundary of the lacuna could be distinguished (Fig. 4E, F).

Representative images of gross observation of IVDs.
Histological assessment and viability of the heterografted stem cells
In the only alginate gel implantation group and nonimplantation control group, almost no remnants of ECM and regenerated NP tissue were seen (Fig. 5E1–F2). In the AFSC implanted group, a little excreted ECM and some scattered implanted cells could be discriminated, while the quantity of regenerated tissue was limited, and large lacuna still existed in the initial NP location (Fig. 5A1, A2). In the NPSC and BM-MSC group, more newly produced ECM surrounding the implanted cells could be indentified obviously in the NP region (Fig. 5B1–5C2). For the CESC group, dense regenerated NP tissue with clusters of cells fully filled the NP lacuna, which made the boundary between NP and AP undistinguished (Fig. 5D1, D2).
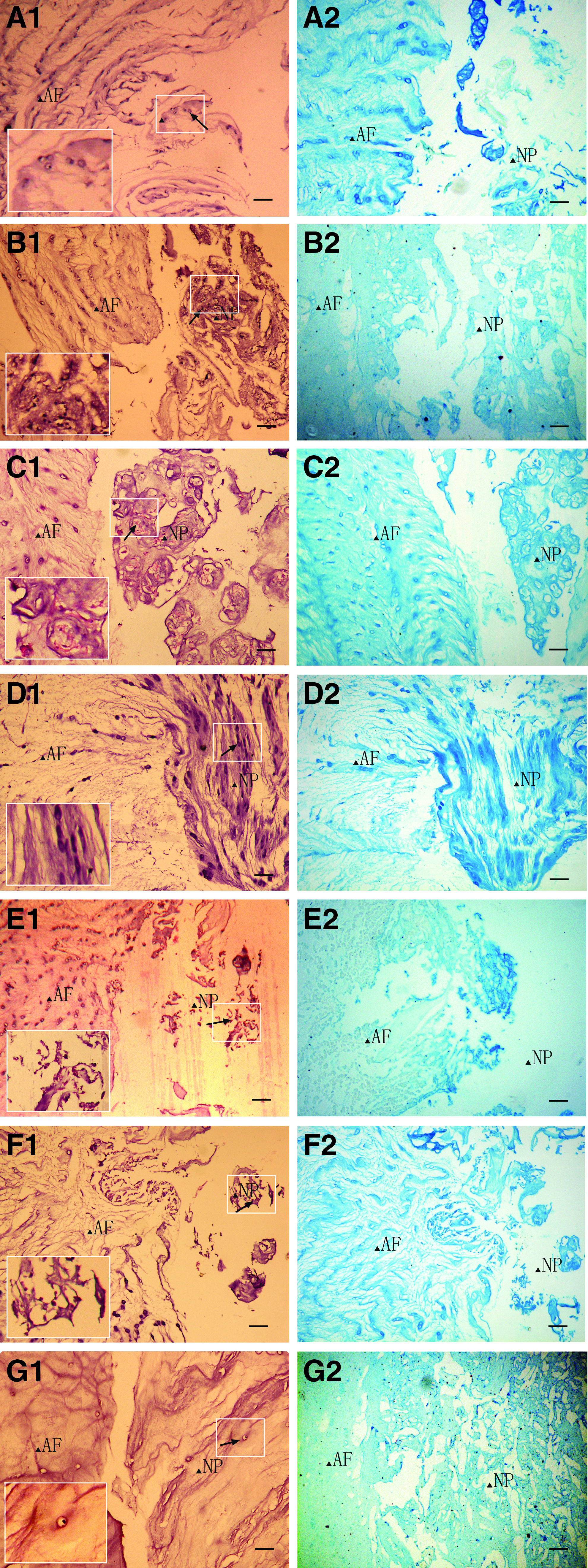
Hematoxylin and eosin and Alcian blue staining of IVDs at 6 months after surgery.
By observing through the confocal laser scanning microscope after setting a gap to counter the background effect, CFDA-SE fluorescence-labeled stem cells were easily seen in all the stem cell containing groups at 6 months (Fig. 6), which indicated that implanted cells survived well even in the xenogeneic environment. The only alginate gel implanted group served as control.
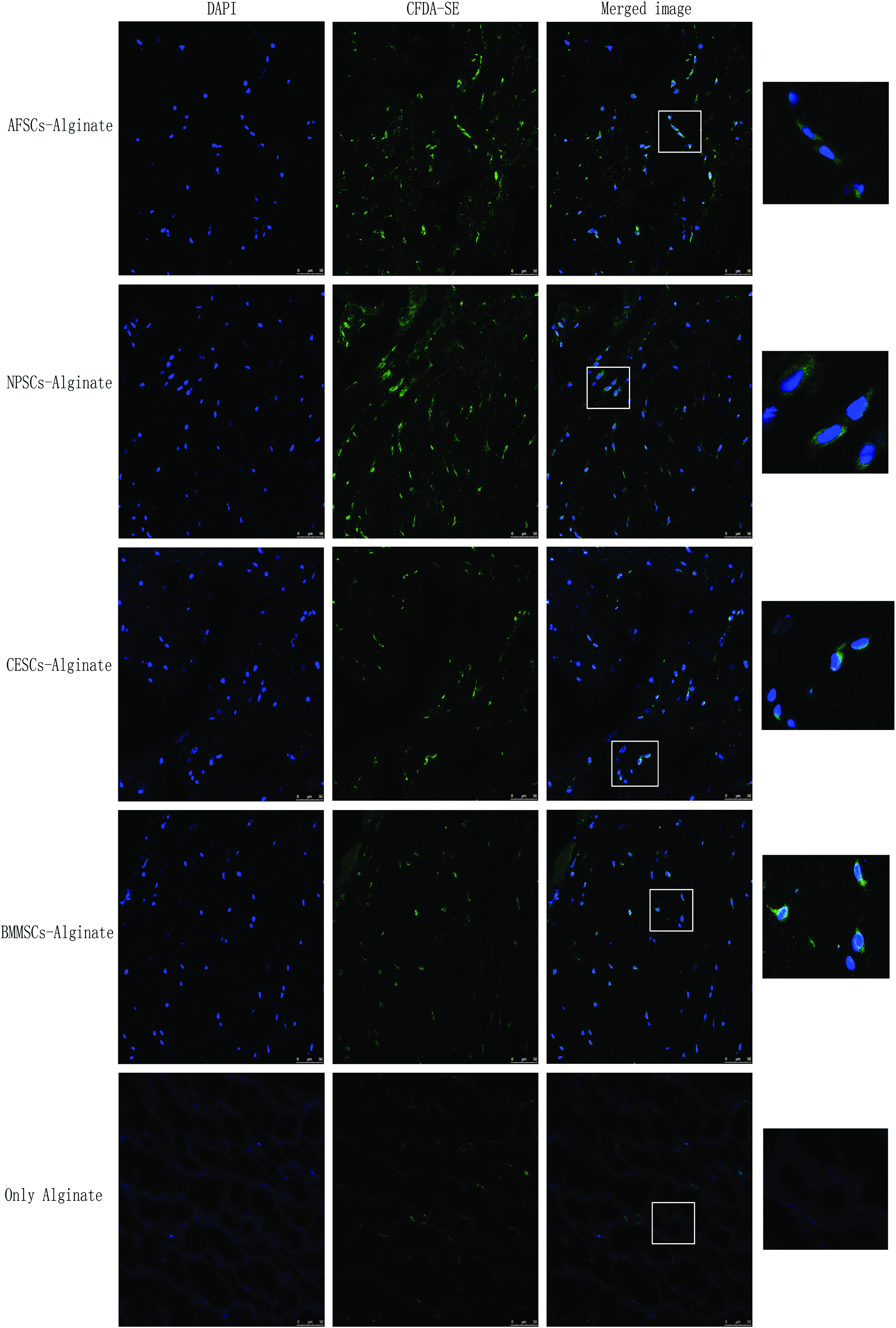
CFDA-SE labeled stem cells implanted in IVDs at 6 months after surgery were observed by the confocal laser scanning microscope. The cytoplasma was marked with green, and the cell nuclei were counterstained with DAPI (blue). Color images available online at www.liebertpub.com/tea
Discussion
BM-MSCs are now a type of widely applied stem cells in tissue engineering and possess lots of merits such as easily culturing and highly expanding potential in vitro, moreover, using of MSCs can avoid the ethical issues. 29 Lots of studies have already been performed with autograft or xenogeneic BM-MSCs in the animal disc degenerative model, all of which exhibited the ability to survive and proliferate in vivo, even could differentiate toward disc-like cells.30,31 Recently, researchers have accomplished a pilot study, in which autologous BM-MSCs were transplanted into human IVD, demonstrating rapid improvements in pain and disability with 71% of optimal efficacy and disc water content elevation, whereas the disc height was not recovered. 13 Despite the above-mentioned merits and encouraging results, there still existed some inherent shortcomings of BM-MSC application as seed cells, for example, the limited source, low cell acquisition rate, additional invasive procedure needed for cell acquisition, and aspiration site pain and infection; furthermore, BM-MSCs easily loose their differentiation potential during expansion.32,33 Therefore, exploring a novel cell source as an alternative or supplement for the traditional BM-MSCs is essential. By contrast, IVD-derived stem cells (AFSCs, NPSCs, and CESCs) could be obtained sufficiently from plenty of discarded clinical IVD samples. If these IVD-derived stem cells could be confirmed to possess excellent biological properties, it might be a potential source for regenerative medicine or tissue engineering. So, it is necessary to compare the NP regenerative potential of the IVD-derived stem cells with that of the traditional stem cells—BM-MSCs in vivo.
In our study, these IVD-derived cells (AFSCs, NPSCs, and CESCs) were negative for cell surface protein such as CD34 and CD45, and positive for CD90 and CD73, although the percentages of CD105-positive cells were slightly lower than 95% in AFSCs and CESCs (89.9%, 89.0%). Additionally, under appropriately induced conditions, all these cells (AFSCs, NPSCs, CESCs, and BM-MSCs) demonstrated the biological characteristics that could differentiate into osteocytes, adipcytes, and chondrocytes, which are the essential traits of stem cells. Furthermore, in both the previous and this study, the cells referred shared the features of adhering to a plastic culture flask when they were expanded in vitro. Totally, these data have provided the evidence that fulfill the basic criteria for MSCs defined by ISCT. 34 Therefore, in combination with previous studies, these data demonstrated that the cells used in this study possess the properties of stem cells.
MSCs have extremely low immunogenicity with low surface density of major histocompatibility complex class I molecules and negative expression of costimulatory molecules: CD80, CD86, and CD40. 35 IVDs fall into the mesoderm from the embryo development standpoint, so these stem cells derived from IVDs belong to the category of MSCs like the BM-MSCs, and might share some common characteristics with BM-MSCs such as low immunogenicity. 36 Furthermore, IVDs are considered with extremely low immunogenicity. 37 Our imaging and histological results confirmed the survival of the implanted stem cells and the exerted regeneration activity of those cells in the xenogeneic environment, which indicating that the induced immune response either was weak or had not a serious impact on the cell viability and ECM secretion potential. However, above all, if these IVD-derived stem cells served as autologous seed cells for human IVD regeneration, immunological rejection might not be an obstacle in this application.
Alginate is a kind of natural polysaccharide derived from the brown algae with a chemical constitution of copolymers composed of
To appraise the degenerative degree of the interested discs, BDI based on the radiological image and T2 signal intensity index based on the T2 value of MRI were adopted to assess the disc height and hydration and proteoglycan content, respectively. 43 At the 1-month time point, statistical difference existed in the T2 value intensity index between the noimplantation group and only alginate gel injection group, nevertheless, at the 3-month time point, there was no statistical difference between them. This result was consistent with the previous study in which an implanted alginate could also maintain the hydration status of the manipulated NP for a short time window. 42 The most probable cause is that, before the degradation, the alginate gel has a water-holding capacity, which contributed to the T2 value maintenance. 44 So, in our study, it is necessary to set up the alginate gel control group to reduce the intrinsic impact of the alginate gel itself to the T2 value maintenance among different groups. In addition, it is worth mentioning that there were always significant differences in the T2 value intensity index between the CESC group and normal group at 1-, 3-, and 6-month time points, respectively. However, until the 6-month time point, significant difference appeared in BDI between the two groups. What was the reason? The T2 value in MRI was a sensitive index and responded directly to the hydration degree of the regenerated NP, which showed positive correlation with the newly excreted ECM by implanted cells. However, besides the degree of NP hydration, several other factors determined the disc height (BDI), including the degeneration extent of AF and facet joints and hyperplasia of ligaments. 45 So, BDI was a relative indirect index reflecting NP regeneration, which was slow to keep up with the changing T2 value.
In general, at all the three time points, both BDI and T2 value intensity index showed that CESCs preserved the maximum regeneration potential among the four types of stem cells from the beginning to the end. In addition, always no significant differences were observed between the BM-MSC and NPSC group, and the only alginate gel group versus no-implantation group (p>0.05). For T2 value intensity index, the AFSC group showed the weakest regeneration potential among the four types of stem cells, but for BDI, both the AFSC and NPSC group ranked at the bottom, and no significant difference existed between them. On the other hand, the gross morphology of the excised IVDs showed that the CESCs excreted more ECM than the other three types of stem cells, BM-MSCs had similar appearance with NPSCs, the AFSCs showed the poorest performance. Moreover, histology analysis indicated that CESCs generated the maximum volume of the newly formed ECM, both BM-MSCs and NPSCs located in the middle, but AFSCs was the worst. This further data preliminarily supported the tendency proved that CESCs had the most powerful regenerative capacity to prevent the NP dehydration and disc space collapse; BM-MSCs were similar to NPSCs, and both ranked in the middle, AFSCs still were the worst ones.
The disc degeneration process could be mimicked by AF puncture or combined NP aspiration. In the former, total annular incision could induce faster disc degeneration than superficial AF stab. 43 In this study, we adopted the AF puncture and NP aspiration model, which was based on the AF puncture method, but the NP tissues were basically aspirated away after AF puncture. 31 This robust mode provided a more hostile environment for the newly implanted stem cell–alginate constructs and posed a greater challenge to test the NP regeneration ability. Whereas the four stem cell types could perform definite regeneration potentials, and CESCs showed the best, although could not meet the standard of the normal control. All of those exciting findings made us full of hope for the potentials of the disc-derived stem cells in the DDD therapy.
To our knowledge, it was the first time to compare the in vivo NP regenerative abilities of four types of stem cells, among which three types of stem cells were derived from the human IVD. Although there was lack of data to support the long-term safety and efficiency of those stem cells serving as seed cells, this study still gave some possible enlightenment for the subsequent basic research and possible clinical application in the future. Our follow-up study would immortalize CESCs to build a stem cell line, and by checking tumorigenicity, immune rejection and biological activity further explore the possibility for future clinical application.
Conclusions
In our study, we had compared the NP regenerative capability of the four types of stem cells, including AFSCs, NPSCs, CESCs, and BM-MSCs derived from the same patient in the rabbit disc aspiration model. The CESCs had the strongest regenerative ability, while AFSCs showed the weakest potency. NPSCs demonstrated the similar capability with the traditional seed cells, BM-MSCs, both of which located in the middle of the four types. These results indicated that CESCs might act as an efficient seed cell source for NP tissue engineering and pave a new way for the biological solution for DDD.
Footnotes
Acknowledgment
This work was supported by the National Natural Science Foundation of China (no. 81101364 and no. 81071498).
Authors' Contributions
Hai Wang: Performing the experiments, manuscript writing, data analysis and interpretation, collection and assembly of data; Bo Huang: Conception and design, financial support, manuscript writing, data analysis and interpretation, final approval of manuscript, provision of clinical samples; Yue Zhou: Conception and design, financial support, administrative support; Lan-Tao Liu: Data analysis and interpretation; Ming-Han Liu: Data analysis and interpretation; Jian Wang: Provision of clinical samples; Chang-Qing Li: Provision of clinical samples; Tong-Wei Chu: Provision of clinical samples; Zheng-Feng Zhang: Provision of clinical samples; Cheng-Jie Xiong: Data analysis and interpretation.
Disclosure Statement
No competing financial interests exist.